Psychology and treatment of public speaking anxiety
Epidemiological and Demographic Prevalence
Glossophobia, commonly identified as the fear of public speaking, represents one of the most widespread manifestations of social anxiety within the global population. Epidemiological data indicates that up to 75% to 77% of individuals experience some degree of anxiety, nervousness, or physiological arousal when required to speak in front of an audience 12345. While many individuals experience only mild to moderate anticipatory nerves, approximately 5% to 10% of the population suffers from severe, debilitating glossophobia that profoundly disrupts occupational, academic, and social functioning 56. In the United States alone, an estimated 15 million individuals deal with the symptoms of public speaking anxiety on a daily basis, and over 40 million adults suffer from anxiety related to presenting 456. When evaluated through the lens of clinical diagnostics, public speaking anxiety frequently co-occurs with Social Anxiety Disorder (SAD); research demonstrates that 89.4% of patients diagnosed with SAD exhibit an intense fear of public speaking 45.
The demographic distribution of public speaking anxiety reveals distinct statistical patterns across gender, age, and socioeconomic lines. Women are consistently reported to experience higher rates of public speaking anxiety than men. National Institute of Mental Health (NIMH) data indicates that women are 1.5 times more likely to report severe glossophobia, with specific phobia prevalence reaching 12.2% in females compared to 5.8% in males 24. Age also serves as a significant modifier. A 2021 University of Sydney study found that young adults between the ages of 18 and 24 exhibit 65% higher rates of public speaking fear than individuals over the age of 50 2. Confidence in public speaking appears to increase with age and professional experience, as 69% of individuals over 45 report feeling confident during presentations, compared to only 25% of individuals aged 16 to 24 4. Furthermore, demographic tracking indicates that urban residents are 25% more prone to public speaking anxiety than rural residents, and lower-income groups report being 50% more affected by the condition 2.
The occupational and economic consequences of unaddressed public speaking anxiety are substantial. Corporate analyses reveal that glossophobia acts as a primary barrier to career advancement, hindering promotions to management positions by approximately 15% and potentially reducing overall earning potential by 10% 56. Furthermore, nearly 20% to 30% of affected individuals actively avoid careers that require presentation skills, and 7% of workers report having directly passed up promotions due to this fear 356. Despite the high economic and psychological costs - which aggregate to an estimated $42.3 billion to $46.6 billion annually for the treatment of related anxiety disorders and phobias - only 8% of individuals suffering from severe public speaking fear actively seek professional therapeutic intervention 456.
Evolutionary Origins and Psychological Maintenance
The intense fear generated by public speaking is deeply rooted in evolutionary psychology and the survival mechanisms of early human ancestors. Evolutionary psychologists posit that the autonomic arousal experienced on a stage is an archaic survival instinct triggered by perceived social vulnerability. In prehistoric human societies, survival was inextricably linked to tribal affiliation, group cohesion, and social acceptance. Rejection, ostracization, or alienation from the group effectively resulted in death by exposure, starvation, or predation 234511.
When an individual stands before an audience, they become the focal point of the group's collective attention. The primal brain interprets this sustained, unidirectional gaze as an evaluative threat, simulating the conditions of a predator's stare or the preamble to social exclusion 46. Consequently, speaking to an audience makes the individual vulnerable to rejection, triggering the exact physiological fight-or-flight mechanisms that historically protected humans from physical danger 451113. The brain's threat-processing centers cannot reliably distinguish between the psychological threat of a poorly received presentation and the physical threat of an approaching predator 5.
Fear of Negative Evaluation and Self-Focused Attention
Beyond biological determinism, public speaking anxiety is sustained through specific cognitive distortions. The primary psychological driver is the Fear of Negative Evaluation (FNE), defined as the apprehension about others' evaluations, distress over their negative evaluations, and the expectation that others will evaluate oneself negatively 51178. This fear often interacts with perfectionism and self-doubt, leading speakers to set impossibly high standards for their performance 11.
Individuals with high FNE exhibit intense self-focused attention during a presentation. Rather than monitoring the audience's actual reactions, the speaker turns their attention inward, hyper-monitoring their own physiological symptoms (e.g., trembling hands, blushing, vocal tremors) and assuming the audience perceives these symptoms as intensely as the speaker feels them 9. This creates a detrimental feedback loop: the awareness of anxiety symptoms generates further anxiety, which subsequently exacerbates the physical symptoms 410.
Post-Event Processing and Memory Consolidation
Following the presentation, the anxiety cycle is perpetuated by Post-Event Processing (PEP). PEP acts as a form of social rumination wherein the individual replays the speaking event in their mind, magnifying perceived flaws, memory lapses, or awkward interactions 11. Studies confirm that high levels of PEP are associated with increased cognitive intrusions about social interactions, poorer concentration, increased recall of past negative experiences, and lowered anticipation for success in future social situations 11. This rumination ultimately functions to reinforce the phobia, validate the initial fear, and trigger avoidance behaviors in the future 411. Over time, this learned fear solidifies the neurological association between audience attention and psychological pain, predisposing the individual to stage fright across various contexts 2412.
Neurobiological Mechanisms and Physiological Arousal
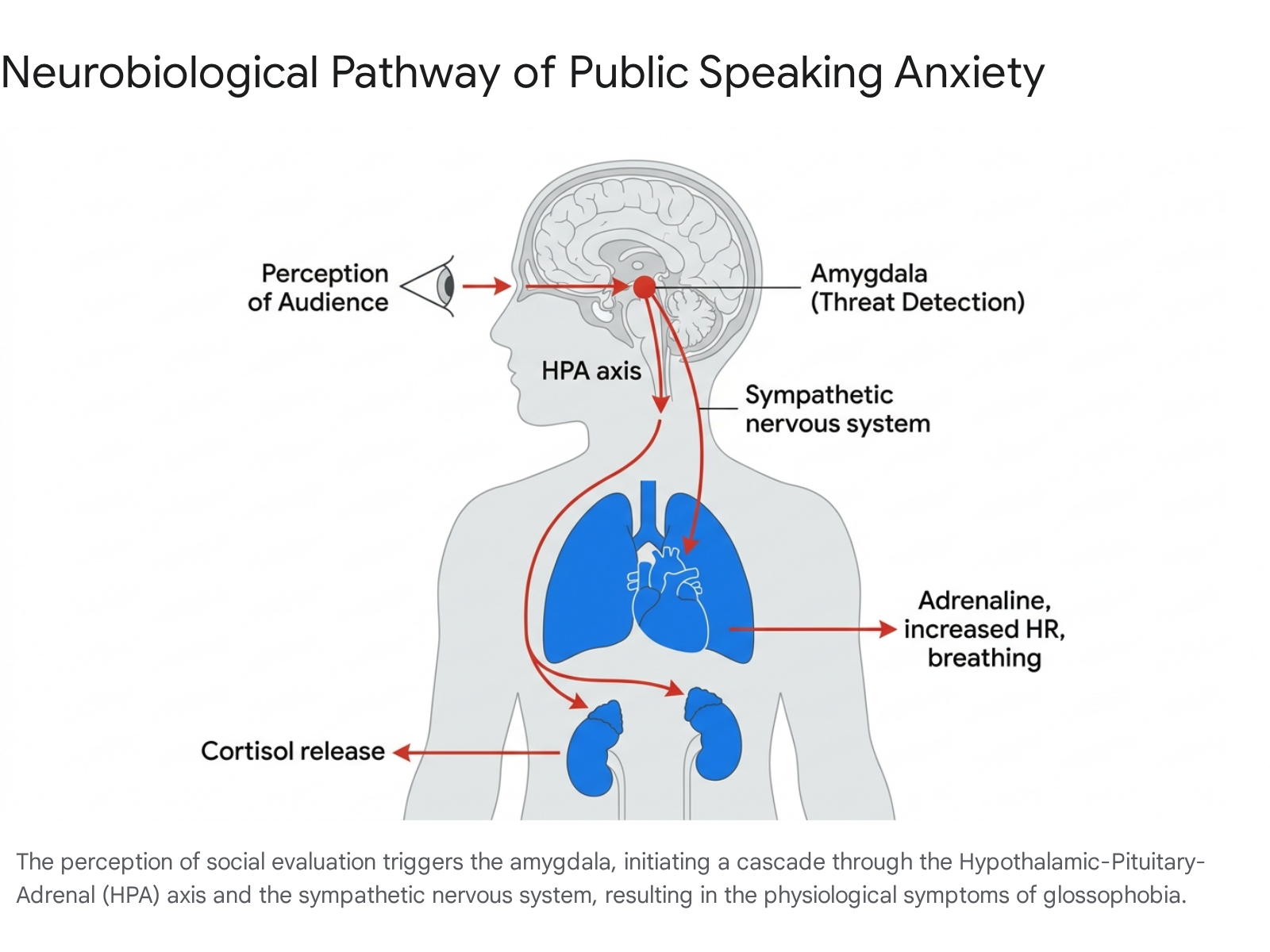
The transition from psychological apprehension to physical panic during public speaking is mediated by complex neurobiological circuits, primarily involving the amygdala, the hypothalamic-pituitary-adrenocortical (HPA) axis, and the sympathetic nervous system.
Amygdala Hyperactivity and Cortical Disconnection
The amygdala, an evolutionarily ancient almond-shaped limbic structure, acts as the brain's primary alarm system for processing emotionally salient external stimuli and initiating defensive behaviors 131314. The amygdala comprises several subnuclei, with the lateral (LA) and basal (BA) nuclei processing associative learning, and the central nucleus (CeA) serving as the primary output region initiating the fear response 14. During public speaking anxiety, the amygdala exhibits intense hyperactivity. Functional magnetic resonance imaging (fMRI) studies reveal that individuals with social anxiety show elevated subcortical, limbic, and lateral paralimbic activity when anticipating public speaking, signifying elevations in automatic emotional processing 1315.
Simultaneously, researchers observe a critical reduction in functional integration between the amygdala and cortical emotion-regulation regions, specifically the anterior cingulate cortex (ACC) and the prefrontal cortex (PFC) 1315. In a neurotypical response, the PFC acts to dampen amygdala output once a threat is deemed non-lethal or manageable. However, the severe stress of social evaluation disrupts this cortical-subcortical communication 1516. This disconnect manifests cognitively as the "brain freeze" phenomenon. As stress hormones saturate the brain, the prefrontal lobes - responsible for memory retrieval, executive function, and logical sequencing - shut down, leaving the speaker entirely unable to access their prepared material or think coherently 5. Electroencephalography (EEG) data further corroborates this state of hyper-arousal, showing an increase in high beta spectral power (20 - 30 Hz), increased gamma band power during speech anticipation, and a decreased frontal theta/beta ratio indicative of reduced cognitive control 16.
The HPA Axis and Sympathetic Autonomic System
The amygdala's distress signal rapidly activates the sympathetic nervous system and the HPA axis, resulting in the secretion of catecholamines (adrenaline and norepinephrine) and glucocorticoids (cortisol) 131316.
Adrenaline and norepinephrine are released almost instantly by the adrenal glands, causing immediate and dramatic changes designed for rapid physical action 13. This sudden influx redirects blood flow from the digestive tract to major muscle groups, dilates the pupils, and dramatically increases heart rate, respiratory rate, and systolic blood pressure 1317.
Four Phases of Physiological Response
The physiological stress response during public speaking follows a highly documented temporal sequence. Behnke established four stable characteristic events or phases in cardiac patterns during public speaking: anticipation, confrontation, adaptation, and release 18. 1. Anticipation: Anxiety and physiological markers (such as heart rate and skin conductance) begin to climb steadily in the minutes or hours preceding the speech as the individual visualizes the upcoming performance 18. 2. Confrontation: Autonomic arousal reaches its absolute peak during the first minute of the speech as the speaker absorbs the reality of the audience's gaze and the physiological cascade initiates 18. 3. Adaptation: As the speech progresses, the cardiovascular and neuroendocrine systems gradually begin to stabilize, though they remain elevated above baseline levels 18. 4. Release: Following the conclusion of the presentation, physiological metrics experience a rapid deceleration back toward resting levels 18.
Empirical measurements confirm that real-world public speaking induces significantly higher physiological distress than laboratory simulations. While procedures like the Simulated Public Speaking Test (SPST) effectively raise self-reported anxiety, authentic speaking tasks in front of an evaluative, live audience produce markedly steeper increases in salivary cortisol, heart rate, and both systolic and diastolic blood pressure 171920.
Cross-Cultural Variations in Anxiety Manifestation
While the physiological stress response to public speaking is universally human, the psychological interpretation of that stress, the specific fears harboring the anxiety, and the social acceptability of symptom expression vary significantly across cultures. Cross-cultural psychology frequently categorizes these differences along the spectrum of individualistic versus collectivistic societal values.
Individualistic Societies
In individualistic cultures - prominent in Western Europe, North America, and Australia - societal norms emphasize personal achievement, self-expression, independence, equal opportunities, and the assertion of individual desires 2129222324. Correspondingly, public speaking anxiety in these environments is generally internalized as an individual psychiatric experience stemming from a fear of personal failure. The core apprehension revolves around appearing incompetent, foolish, or inadequate, thereby damaging one's personal reputation, self-esteem, or career trajectory 2425. Because assertive communication and verbal competence are highly prized workforce competencies in individualistic cultures, individuals who exhibit socially avoidant behaviors or public speaking fear suffer significantly greater occupational and social impairment than their collectivistic counterparts 2922.
Collectivistic Societies
Conversely, collectivistic cultures - historically associated with East Asian, Middle Eastern, Sub-Saharan African, and Latin American societies - prioritize group harmony, interdependence, and strict conformity to in-group norms 2922232426. In these contexts, public speaking anxiety often manifests differently. Rather than fearing personal embarrassment, the anxiety stems from a profound fear of disrupting social harmony, burdening the audience, or bringing shame to one's family or affiliated group 24. A clinical example of this is Taijin Kyofusho, a condition found in Japan, characterized by an intense fear that one's body, appearance, or social presence will offend or displease others 24.
Global prevalence studies indicate that individuals from East Asian collectivistic countries frequently report higher baseline levels of social anxiety, Fear of Negative Evaluation, and disqualification of positive social outcomes than their Western counterparts 82122. However, this heightened self-reporting does not necessarily translate to higher clinical impairment. Because socially reticent, quiet, and avoidant behaviors are often culturally accepted or even viewed positively as signs of humility and respect in collectivistic societies, individuals may suffer less functional impairment from their anxiety than an individual in a Western workplace would 22. Some researchers propose a "response style hypothesis," suggesting that higher self-reported levels of social anxiety in these regions reflect cultural values and low independent self-construal rather than genuine pathological differences 22.
It is important to note that the binary model of individualism versus collectivism has structural limitations. Recent empirical comparisons reveal that Latin American countries, despite exhibiting strong collectivistic values, report some of the lowest social anxiety levels globally, suggesting that cultural warmth, simpatía, and other localized social norms significantly alter how anxiety develops and is expressed 2122.
Environmental Modifiers in Virtual Communication
The rapid transition to digital and remote communication environments has fundamentally altered the psychological triggers associated with public speaking. While one might intuitively assume that speaking from the physical safety of one's home reduces anxiety, the phenomenon of "Zoom fatigue" has introduced novel cognitive and visual stressors that frequently exacerbate glossophobia 62728.
Virtual public speaking environments artificially amplify several anxiety-inducing stimuli. In a standard physical conference room, audiences naturally break eye contact, take notes, or shift their gaze, providing the speaker with visual relief. On a video conferencing platform, the speaker faces a grid of faces staring directly forward. This excessive, sustained eye contact mimics the predatory threat signals recognized by the amygdala; the brain interprets the physical closeness of faces on a screen as an intense, confrontational situation, keeping the sympathetic nervous system engaged for the duration of the call 627. Furthermore, the physical immobility required to stay within the camera frame restricts the speaker's ability to utilize natural body language and pacing, which are common and necessary mechanisms for dissipating nervous energy 627.
The Mirror Effect and Self-Referential Information
Perhaps the most detrimental feature of virtual speaking is the constant consumption of Self-Referential Information (SRI), commonly referred to as the "mirror effect" 628. Keeping the self-view window active during a presentation forces the speaker into an unnatural state of hyper-self-awareness. Research indicates that staring at one's own digital reflection increases cognitive load and correlates positively with self-criticism and negative affect 2728. Users find themselves scrutinizing their own facial expressions, grooming, and micro-movements rather than focusing on content delivery, leading to rapid emotional exhaustion, visual fatigue, and lowered satisfaction with the communicative process 628.
Other situational variables interact to predict the severity of virtual public speaking anxiety. Mixed-effect models and multiple regression analyses reveal that audience size, the spatial dimensions of the virtual "room," and the audience's engagement level (e.g., supportive nodding versus disengaged silence) interact significantly to alter the speaker's anticipated distress 2930. Interestingly, physiological monitoring indicates that participants facing a supportive virtual audience with encouraging questions show an increase in skin conductance. Rather than indicating fear, researchers suggest this represents healthy physiological engagement and positive arousal during a bidirectional communicative exchange 10.
Examination of Common Remediation Myths
The universal dread surrounding glossophobia has generated a vast ecosystem of folk remedies, unverified advice, and misconceptions regarding what makes a competent speaker and how to cure stage fright. Clinical research and empirical data systematically debunk several of these deeply entrenched myths, demonstrating that many common "hacks" actually increase anxiety.
| Common Myth | Empirical Reality | Evidence Base |
|---|---|---|
| Introverts are inherently poor public speakers. | There is no correlation between introversion and public speaking anxiety. Introverts often excel at speaking due to strong listening skills, empathy, and meticulous preparation habits. | Introverts comprise 82% of individuals with high glossophobia scores, but this reflects reporting bias. Famous orators like Abraham Lincoln, Martin Luther King Jr., and Susan Cain identify as introverts 12123132. |
| Visualizing the audience in their underwear reduces anxiety. | This mental tactic actively increases the speaker's cognitive load without alleviating physical arousal. It fosters a false sense of superiority, feels dehumanizing to the audience, and breaks authentic eye contact. | In highly emotional contexts (e.g., eulogies) or virtual environments where only the chest upward is visible, the visualization technique completely breaks down and becomes a distraction 3334353637. |
| Experienced speakers do not experience physiological nervousness. | Even veteran speakers experience the autonomic "fight-or-flight" response. The distinction lies in cognitive framing; experienced speakers label the arousal as excitement or readiness rather than existential threat. | Decades of physiological tracking show that heart rate and blood pressure elevate uniformly among both novices and seasoned performers (including actors) during the confrontation phase 1181932. |
| Speakers should memorize their speeches verbatim. | Rote memorization dramatically increases the risk of "brain freeze." When a speaker forgets a single memorized word, the entire cognitive sequence breaks down, leading to panic and robotic delivery. | Experts recommend internalizing the structural outline and speaking conversationally to allow for cognitive flexibility, drastically reducing the fear of forgetting 1232. |
Efficacy of Psychotherapeutic Interventions
Because public speaking anxiety is sustained through behavioral avoidance and entrenched cognitive distortions, unstructured practice is rarely sufficient to cure severe glossophobia. Clinical interventions operate by forcing the brain to decouple the stimulus (the audience) from the catastrophic threat response.
Cognitive Behavioral Therapy and In Vivo Exposure
Cognitive Behavioral Therapy (CBT) combined with in vivo (real-life) exposure therapy has historically been the gold standard for treating public speaking anxiety and Social Anxiety Disorder 383940. The therapeutic mechanism relies on "inhibitory learning" and habituation. By systematically exposing the patient to speaking scenarios of increasing difficulty without allowing them to engage in safety behaviors or escape, the brain eventually registers that the feared catastrophic outcome does not occur 3841. Over multiple sessions, the amygdala's automatic fear response undergoes extinction 38. In Bodie's comprehensive review of treatment efficacy, meta-analytic data suggests that the most successful treatment combination sequence begins with systematic desensitization or cognitive modification, and concludes with skills training 4243.
CBT simultaneously targets cognitive maintenance factors. Therapists assist patients in identifying and restructuring their Fear of Negative Evaluation, dismantling perfectionism, and converting self-focused attention back into task-focused attention 3844. However, traditional in vivo exposure presents significant logistical hurdles. Generating a realistic, live audience for a patient to practice in front of is costly, time-consuming, and highly unpredictable. Consequently, patients frequently refuse in vivo therapy or drop out prematurely due to the sheer terror of confronting a real audience 405345. Additionally, while well-delivered CBT is effective, it is not without adverse events; approximately 10% to 17% of participants report unwanted side effects during treatment, such as transient distress, temporary worsening of symptoms, or strains in family relations due to the intense emotional work required 4647.
Virtual Reality Exposure Therapy (VRET)
To bypass the limitations of in vivo exposure, clinicians have increasingly adopted Virtual Reality Exposure Therapy (VRET). Utilizing head-mounted displays, VRET places the patient in a fully immersive, computer-generated auditorium or boardroom where they deliver speeches to virtual avatars 384041. The therapist maintains absolute control over the environmental variables, adjusting the audience size, background noise, and avatar behaviors (e.g., polite applause, yawning, looking at phones, or hostile questioning) to match the patient's exact threshold for exposure 10384145.
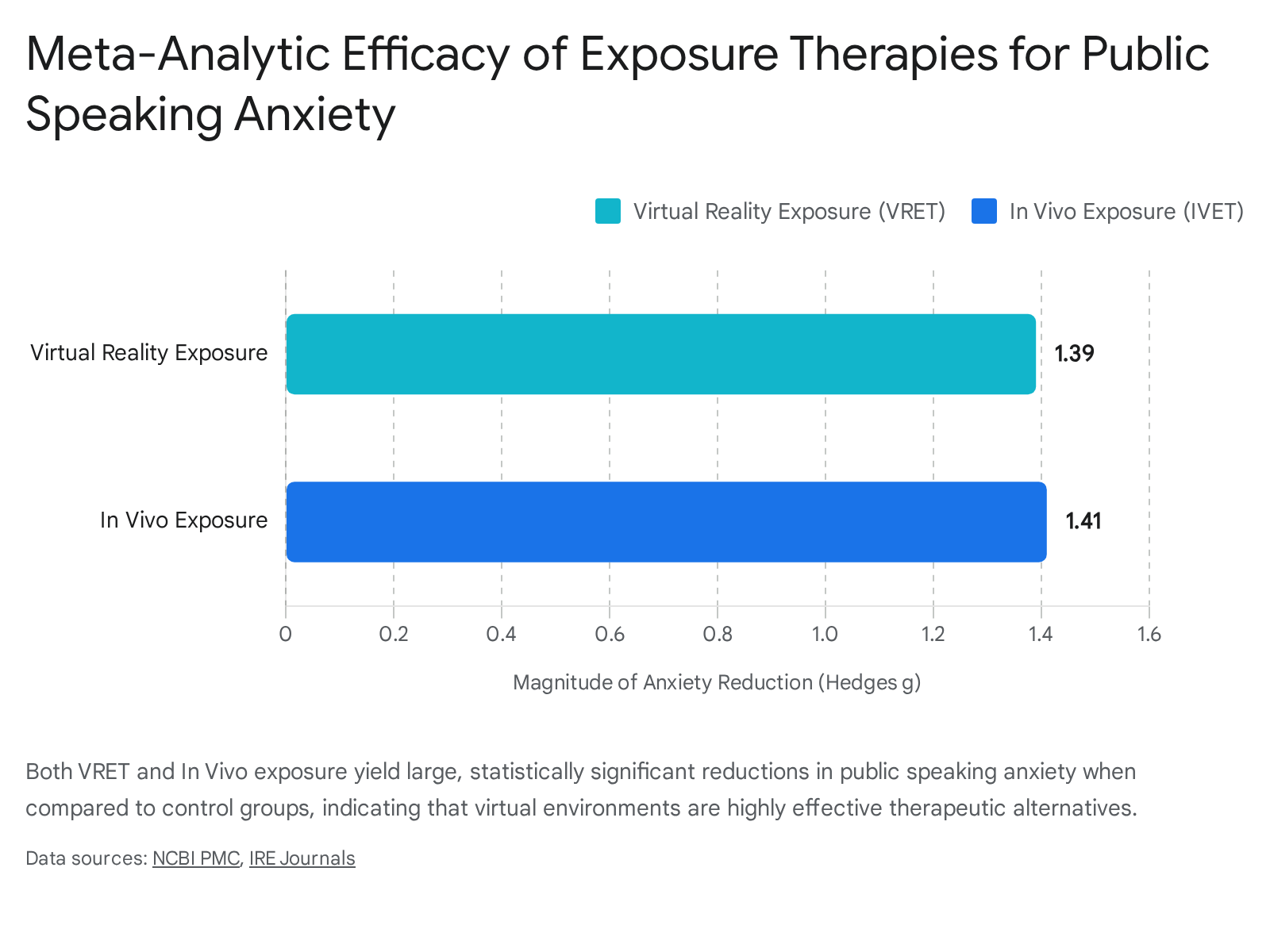
Systematic reviews and meta-analyses published between 2020 and 2025 confirm that VRET is a highly efficacious intervention, yielding large, statistically significant reductions in public speaking anxiety 39414849. Crucially, VRET demonstrates comparable efficacy to traditional in vivo exposure. In a meta-analysis comparing interventions against control conditions, VRET resulted in an effect size of -1.39, while in vivo exposure resulted in an effect size of -1.41, indicating that the virtual intervention is nearly identical in clinical power 394150. Longitudinal follow-ups indicate that the positive effects of VRET are maintained for up to six years post-treatment, though some studies suggest in vivo exposure may hold a slight superiority in long-term follow-ups at the 12-month mark 485152.
Patient acceptance is notably higher for VRET. When given a choice, approximately 76% of patients prefer VRET over in vivo exposure due to the perceived safety and confidentiality of the virtual environment 40455153. While dropout rates between the two modalities are statistically similar - averaging around 16% - the reasons for attrition differ fundamentally 45515253. Patients drop out of in vivo exposure primarily due to overwhelming fear of confronting the phobic stimuli, whereas VRET attrition is overwhelmingly driven by technological limitations, such as cybersickness, failed immersion, visual discomfort, or sensory overload 455354. VRET also faces limitations regarding the "uncanny valley" effect, where highly realistic but slightly unnatural avatars can unsettle users, and ethical concerns regarding the data privacy of physiological metrics collected by headsets 54. Nevertheless, as technology improves, VRET remains a highly scalable frontline treatment option 384055.
Pharmacological Augmentation for Performance Anxiety
For individuals whose glossophobia is restricted purely to isolated performance events - rather than a chronic, generalized social anxiety disorder - pharmacological intervention can offer immediate symptomatic relief. Beta-adrenergic blocking agents (beta-blockers), originally developed to treat cardiovascular conditions such as hypertension and angina, are frequently prescribed "off-label" to manage performance anxiety 56575859.
The most commonly prescribed agent for this indication is propranolol (a non-selective beta-blocker), though metoprolol (a beta-1 selective agent) is sometimes used as a second-line alternative for patients with mild respiratory concerns 6960. Beta-blockers exert their anxiolytic effect strictly on the peripheral nervous system. They operate by binding to beta receptors, competitively inhibiting the binding of stress hormones like adrenaline and epinephrine 57585961. By blocking these receptors, the medication successfully prevents the cascading physical symptoms of the fight-or-flight response, halting the rapid heartbeat, excessive sweating, shaking hands, and vocal tremors before they can manifest 56606162.
| Feature | Cognitive Behavioral Therapy (CBT) & Exposure | Beta-Blocker Pharmacotherapy (Propranolol) |
|---|---|---|
| Primary Mechanism | Targets cognitive distortions (FNE); uses inhibitory learning to extinguish the amygdala fear response. | Blocks peripheral adrenaline receptors; physically prevents tachycardia, sweating, and tremors. |
| Target Symptoms | Psychological terror, avoidance behaviors, cognitive rumination, and physical arousal. | Exclusively targets physical symptoms. Does not alter fearful thoughts or cognitive appraisals. |
| Onset and Duration | Requires weeks/months of sustained practice. Effects are long-lasting and potentially permanent. | Fast-acting (takes effect within 30 - 60 minutes). Short duration (lasts ~4 hours). |
| Clinical Indication | Recommended for generalized Social Anxiety Disorder and severe, pervasive glossophobia. | Recommended for infrequent, isolated performance anxiety (stage fright) in otherwise non-anxious individuals. |
| Key Limitations | High time commitment, emotional discomfort during exposure, risk of dropout, transient side effects. | Contraindicated for asthma, bradycardia, and low blood pressure. Not a cure for underlying psychological anxiety. |
Crucially, beta-blockers do not cross the blood-brain barrier in a manner that alters cognitive chemistry or emotion 596061. They do not cure the underlying psychological fear of negative evaluation, nor do they diminish cognitive dread. However, for many public speakers, the physical manifestations of anxiety are the most disturbing element; feeling their heart pound induces a secondary panic loop. By placing an artificial ceiling on the heart rate, beta-blockers prevent this secondary panic, allowing the speaker to maintain mental clarity, focus, and memory recall without the sedating effects associated with traditional anti-anxiety medications like benzodiazepines 565961.
Despite their efficacy for acute stage fright, clinical guidelines strictly warn against using beta-blockers as a daily treatment for chronic anxiety 69. Furthermore, because they alter cardiovascular and respiratory function, they carry strict contraindications. They are not recommended for individuals with asthma, chronic obstructive pulmonary disease (COPD), bradycardia, heart block, or severe hypotension, as they can exacerbate bronchospasms or mask the hemodynamic signs of hypoglycemia in diabetic patients 5758596960. Common side effects include fatigue, cold extremities, dizziness, sleep changes, and gastrointestinal distress 575862.
Conclusion
The universality of public speaking anxiety is a direct byproduct of human evolutionary wiring combined with complex neurobiological responses. Glossophobia is not an indicator of weakness, introversion, or a lack of linguistic skill; rather, it is the predictable functioning of an archaic neurological alarm system that equates the sustained gaze of an audience with existential social peril. When the amygdala detects this social evaluation, it triggers a cascade of physiological arousal through the HPA axis and sympathetic nervous system, resulting in acute physical distress that subsequently derails cognitive function.
While the biological reaction is deeply ingrained, the manifestation of this anxiety is heavily contoured by cultural context, virtual environments, and cognitive distortions like the fear of negative evaluation. Fortunately, empirical evidence demonstrates that glossophobia is highly treatable. Modern interventions - ranging from the precise, immersive habituation offered by Virtual Reality Exposure Therapy to the acute, targeted physiological dampening provided by beta-adrenergic blockers - equip individuals with the tools necessary to decouple audience attention from the threat response, ultimately transforming public speaking from a source of terror into a manageable professional competency.