When Therapy Speak Helps or Hurts
"Therapy speak" is the rapid mainstream adoption of psychological terminology - such as trauma, gaslighting, and boundaries - into everyday conversation. While this trend has successfully destigmatized mental healthcare and given people the vocabulary to advocate for themselves, it frequently dilutes the precise meaning of serious clinical conditions. When misapplied, these clinical buzzwords can bypass authentic communication, foster social isolation, and ultimately trivialize genuine psychological suffering.
The Cultural Evolution of Psychological Jargon
Over the past decade, the vocabulary of the clinical psychologist has migrated out of the consultation room and into the public square. Terms that were once confined to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) or peer-reviewed psychiatric literature are now the lingua franca of coffee shops, corporate boardrooms, and social media platforms 12. Individuals no longer simply disagree; they are "gaslighted." A difficult boss is not merely demanding, but a "narcissist." An uncomfortable commute is described as "traumatic," and the desire to stay home on a Friday night is framed as "setting boundaries" 134.
This phenomenon represents the imprecise and often superficial integration of psychotherapy language into everyday communication 4. According to recent industry surveys, approximately 95% of Americans report hearing mental health terms used regularly in casual conversation 4. The normalization of this language is, in many respects, a monumental public health victory. It reflects a society that is increasingly literate in emotional well-being and less burdened by the historical shame that previously forced mental illness into the shadows 15.
However, sociolinguists, anthropologists, and clinical psychologists are increasingly identifying a dark side to this linguistic democratization. The widespread appropriation of clinical terms is leading to a phenomenon known as "semantic bleaching" - a process where words lose their original intensity and meaning due to overuse 6. When highly specific diagnostic labels are stripped of their clinical nuance and applied to normative human experiences, the language intended to heal communities can instead be used to confuse, divide, and manipulate them 24.
Experts draw a sharp distinction between true "mental health literacy" and mere "therapy speak." While emotional literacy refers to the ability to recognize, express, and manage one's own emotions, mental health literacy requires possessing accurate, scientifically grounded information about psychiatric conditions 78. The current cultural moment is saturated with the latter's vocabulary but often lacks its foundational understanding, leading to a paradox where society speaks constantly about mental health without necessarily understanding it.
The Diagnostic Lexicon: Clinical Reality vs. Colloquial Use
To understand the impact of therapy speak, it is necessary to examine how specific terms have been decoupled from their clinical definitions. Psychotherapeutic concepts are not arbitrary labels; they are nuanced constructs developed through decades of empirical research, clinical observation, and rigorous peer review 29. When condensed into conversational soundbites, this underlying rigor is frequently lost.
Psychologists have long warned of the "jingle and jangle fallacies" in scientific communication. The jingle fallacy occurs when people use the same word to refer to entirely different concepts, while the jangle fallacy occurs when different words are used to describe the same phenomenon 9. Therapy speak is a massive, cultural-scale jingle fallacy: the clinical establishment and the general public are using the same words but speaking entirely different languages.
| Psychological Term | Clinical Reality (DSM-5-TR / Psychiatric Consensus) | Colloquial Misuse in "Therapy Speak" |
|---|---|---|
| Trauma | Exposure to actual or threatened death, serious injury, or sexual violence (Criterion A for PTSD) 1110. | Any highly distressing, uncomfortable, or disappointing everyday experience 3. |
| Narcissism (NPD) | A pervasive pattern of grandiosity, need for admiration, and a severe lack of empathy impairing daily functioning 1311. | Being self-centered, boastful, or acting selfishly in a specific interpersonal conflict 12. |
| Gaslighting | A systemic, intentional form of psychological manipulation designed to make a victim question their own sanity and reality 412. | Lying, having a different interpretation of a shared event, or simply disagreeing 213. |
| Trigger | A specific stimulus that provokes a severe psychiatric symptom, such as a PTSD flashback or an OCD compulsion 1112. | Anything that causes offense, annoyance, or general emotional discomfort 12. |
| Boundaries | Internal rules established to govern one's own behavior and protect personal emotional safety 1314. | Ultimatums or rules imposed to control another person's behavior to avoid personal discomfort 13. |
The Dilution of Trauma: "Big T" versus "Little t"
Perhaps no word has experienced as much semantic inflation as "trauma." In clinical psychiatry, trauma is not synonymous with distress. The DSM-5-TR criteria for Post-Traumatic Stress Disorder (PTSD) explicitly outlines a "gatekeeper" requirement known as Criterion A. For an event to qualify as clinically traumatic, an individual must be exposed to actual or threatened death, serious injury, or sexual violence. This exposure must occur through direct experience, witnessing the event in person, learning that a violent or accidental event occurred to a close family member, or experiencing repeated extreme exposure to aversive details, such as first responders handling human remains 111015.
To receive a PTSD diagnosis, a patient must also meet subsequent criteria, including persistent intrusion symptoms (nightmares, flashbacks), avoidance of trauma-related stimuli, negative alterations in cognitions and mood (exaggerated blame, feeling isolated), and marked alterations in arousal and reactivity (hypervigilance, aggressive behavior) 111016.
In contemporary culture, however, the term has been stretched to encompass a vast array of negative experiences. Individuals frequently describe ordinary life stressors - a difficult commute, a challenging workday, or a routine romantic breakup - as "traumatic" 3. Psychologists warn that this colloquial dilution minimizes the profound, neurobiological suffering of individuals living with legitimate trauma disorders. When we apply weighty terminology to commonplace matters, we downgrade the seriousness of genuine trauma and risk invalidating those who suffer from chronic hypervigilance and complex PTSD 317.
This linguistic expansion is complicated by the valid clinical recognition of "little t" traumas. While "Big T" traumas align with DSM-5 Criterion A, psychologists increasingly recognize that chronic, compounded stressors - such as childhood emotional neglect, prolonged bullying, or adverse childhood experiences (ACEs) - can profoundly alter brain development and lead to toxic stress 318. These "little t" traumas do not necessarily meet the criteria for PTSD, but they are critical for understanding attachment disorders and complex trauma responses 1822. The challenge lies in validating the impact of "little t" trauma without creating a culture where every normative disappointment is pathologized 1722.
The Misuse of Narcissism and Toxic Traits
The term "narcissist" has become the default label for any ex-partner, difficult family member, or demanding colleague. However, Narcissistic Personality Disorder (NPD) is a complex, rare, and deeply debilitating condition. Under the DSM-5-TR, a diagnosis of NPD requires a pervasive pattern of grandiosity, a constant need for admiration, and a distinct lack of empathy that begins by early adulthood and persists across various contexts 1319.
To meet the diagnostic threshold, an individual must exhibit at least five of nine specific criteria: a grandiose sense of self-importance, preoccupation with fantasies of unlimited success, a belief in being uniquely "special," a requirement for excessive admiration, a sense of entitlement, interpersonally exploitative behavior, a profound lack of empathy, chronic envy of others, and arrogant or haughty behaviors 131119. The DSM-5 Section III alternative model further requires moderate or greater impairment in identity, self-direction, empathy, or intimacy 13.
A person acting selfishly during a divorce is demonstrating a negative behavioral trait; they are not necessarily exhibiting a personality disorder. When the public conflates temporary selfishness with NPD, it not only stigmatizes the disorder but prevents individuals from examining the mutual dynamics of their interpersonal conflicts 1213.
Similarly, the word "toxic" lacks any scientific or agreed-upon clinical definition 2021. While it is a useful colloquial shorthand for individuals who regularly threaten one's psychological safety through manipulation or emotional abuse, it is frequently misused to describe anyone who causes an individual to feel normal negative emotions such as guilt, anxiety, or anger 20. The danger of labeling a person "toxic" is that it relies on moral absolutism, writing off complex human beings as irredeemable rather than addressing specific problematic behaviors 24.
Weaponizing Boundaries and Gaslighting
The concept of "boundaries" has undergone a profound distortion. In therapeutic contexts, a boundary is an internal parameter designed to protect one's own emotional energy - for instance, deciding not to answer work emails after 7:00 PM, or choosing to leave a room if a conversation becomes physically threatening 2622. However, therapy speak has transformed the concept of boundaries into a mechanism for controlling others.
This was notably highlighted in the public discourse surrounding leaked text messages between actor Jonah Hill and his former partner. In the messages, Hill used the term "boundaries" to issue a list of demands restricting his partner's behavior, friendships, and career activities 423. Experts point to this as a textbook example of weaponized therapy speak, where controlling behavior is rebranded as healthy self-care, making it difficult for the recipient to contest the demands without appearing to violate psychological health standards 423.
Similarly, "gaslighting" - a term derived from a 1938 play depicting a husband systematically driving his wife insane by manipulating her environment - has been diluted to mean any form of disagreement or invalidation 2413. When individuals use the term "gaslighting" to describe a partner who simply remembers an argument differently, they bypass the opportunity for conflict resolution. By applying a clinical label of abuse, the speaker asserts a monopoly on objective reality, framing any challenge to their perspective as a psychological attack 1329.
The Social Media Engine: Algorithms and "Mindflation"
The rapid proliferation of therapy speak cannot be untangled from the architecture of modern social media platforms. On platforms like TikTok and Instagram, mental health content has become a distinct, highly lucrative genre. Hashtags such as #TherapyTok and #MentalHealth have accumulated billions of views, driven by algorithms designed to maximize user engagement through dopamine-driven feedback loops 182930.
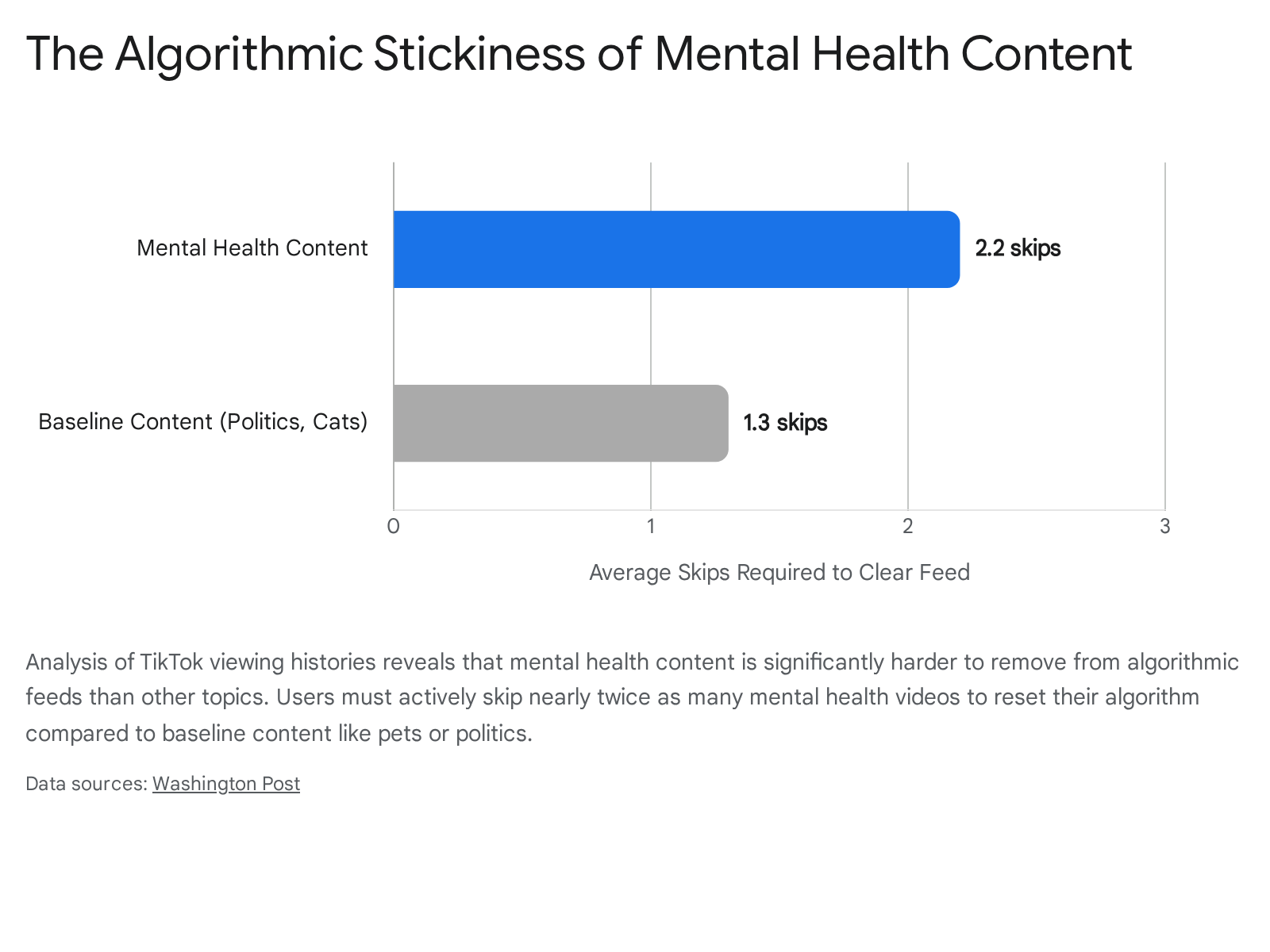
While this digital ecosystem has successfully democratized access to psychological concepts, it is governed by an algorithm that prioritizes "stickiness" over clinical accuracy. A comprehensive data analysis conducted by the Washington Post, examining the viewing histories of nearly 900 U.S. TikTok users, revealed that mental health content is significantly more aggressive in capturing and holding user attention than other content categories .
The analysis measured the stickiness of content by calculating how many times a user had to explicitly skip a type of video to remove it from their algorithmic feed. To undo the effect of watching a single full video about politics or cats, a user had to skip past an average of 1.3 subsequent videos of the same genre. To clear mental health content, the requirement jumped to 2.2 skips .
This algorithmic persistence creates rabbit holes where users are rapidly inundated with increasingly extreme psychiatric content. As users engage with this sensory rush of bite-sized videos, they receive endorphin and dopamine hits similar to behavioral conditioning mechanisms . A user who pauses on a video about generalized anxiety may quickly find their feed saturated with content regarding panic disorders, complex PTSD, and dissociative states 24.
This constant exposure fuels what sociologists have termed "mindflation" - the commodification and dilution of mental health language 14. The format of short-form video necessitates the oversimplification of complex clinical criteria 3025. Consequently, normal human behaviors - such as occasional forgetfulness, social awkwardness, or shifting moods - are frequently repackaged as symptoms of neurodivergence or clinical pathology. A recent study evaluating 1,000 TikTok videos across 16 countries found that the vast majority of mental health advice on the platform - up to 83.7% - was misleading, lacked context, or was presented by unqualified creators 1429.
This digital environment fosters a dangerous validation trap. As users relate to hyper-generalized symptoms presented online, they engage in self-diagnosis, bypassing clinical evaluation 224. This self-diagnosis provides a temporary sense of community and understanding, but it frequently leads to inappropriate medicalization. When individuals adopt psychiatric labels based on social media consumption, they risk altering how they perceive their own resilience, viewing everyday discomfort as a permanent pathological trait rather than a manageable human experience 2426.
Sociolinguistics: Epistemic Authority and Affective Injustice
To understand why therapy speak is so pervasive, one must examine the sociolinguistic power it wields. Psychotherapy language possesses what researchers term "epistemic authority" - it carries the weight, objectivity, and credibility of the medical establishment 4.
Linguistic researchers note a fascinating divide in how English speakers process emotion based on word origins. When a person communicates their emotional distress using ordinary language with Old English (Saxon) roots - such as sad, mad, or scared - they are expressing immediate, raw vulnerability 36. However, when they translate that experience into clinical, Latinate terminology - such as depressed, dysregulated, or avoidant - they invoke an objective, medicalized stance. This linguistic shift acts as an intellectual defense mechanism, allowing the speaker to place emotional distance between themselves and their feelings 3627. By using the language of science, the speaker elevates their subjective emotional experience to the status of a medical fact, making it incredibly difficult for others to question or contest their claims without appearing insensitive 427.
Academic researchers note that this dynamic frequently results in "affective injustice." This occurs when privileged individuals misappropriate the highly specific hermeneutical resources originally developed for marginalized or severely mentally ill populations 4. For example, when individuals who do not possess Obsessive-Compulsive Disorder (OCD) use the term to describe their preference for a tidy desk, they engage in semantic bleaching. This casual misappropriation deprives true OCD sufferers of the precise vocabulary needed to describe their debilitating intrusive thoughts and compulsions, ultimately causing the clinical term to lose its diagnostic power in the public sphere 412.
Furthermore, therapy speak is often utilized to evade relational responsibility. By framing an unwillingness to compromise as "protecting my peace," or ghosting a friend as a result of "attachment style," individuals can mask selfish or avoidant behavior under the unimpeachable guise of clinical self-care 427. The medicalization of the language allows the speaker to abdicate accountability for their interpersonal actions, turning moral or relational failures into inevitable psychiatric symptoms 27.
Esther Perel and the Paradox of Modern Intimacy
The relational fallout of therapy speak has been extensively documented by leading clinical psychotherapists. Esther Perel, a globally recognized relationship expert, argues that the very language intended to facilitate connection is, in practice, becoming a powerful destroyer of intimacy 28.
Perel's critique centers on the concept that labels kill curiosity 28. In healthy interpersonal dynamics, conflict requires empathy, active listening, and a willingness to explore the unknown internal world of another person. When a partner responds to a disagreement by immediately diagnosing the other person as "narcissistic" or labeling their behavior as a "trauma response," they take refuge in the false certainty of a clinical label 28. This reductionist approach strips the individual of their complexity, allowing the diagnosing partner to categorize, dismiss, and invalidate the behavior without having to engage with it 2528.
Through her systemic therapy background, Perel views relationships as living organisms composed of interdependent parts. Like ecological systems, relationships require a balance of stability and friction to survive; too much stability leads to fossilization, while too much rapid change causes chaos 2940. Therapy speak, however, is often deployed to entirely erase the natural friction of human relationships. By pathologizing normal conflict, individuals retreat into silos of self-preservation 4030.
This hyper-focus on the self and the rigid enforcement of personal boundaries contribute directly to the modern loneliness epidemic 2231. Perel notes that modern society suffers from "artificial intimacy" - we possess a vast vocabulary to analyze our feelings through our screens, yet we lack the tolerance to experience those messy feelings alongside others in three-dimensional reality 30. The casual use of phrases like "I no longer have the capacity to invest in this relationship" to end friendships prioritizes sterile emotional distance over the necessary work of human connection and repair 2229.
Gen Z and the Workplace Mental Health Reckoning
The infiltration of therapy speak has profoundly altered the modern workplace, largely driven by Generation Z. Entering the workforce during a period of global instability, remote isolation, and economic uncertainty, Gen Z employees have aggressively challenged the traditional boundaries between professional life and emotional well-being 3244.
Recent data indicates that the youngest cohort of the workforce views mental healthcare not as a personal luxury, but as a non-negotiable institutional requirement. According to human resources research, 70% of Gen Z workers state that robust mental health benefits and proactive counseling are essential when evaluating an employer, and 57% fundamentally disapprove of the 40-hour work week on mental health grounds 3244. Furthermore, corporate healthcare platforms have noted massive surges in the utilization of company-sponsored therapy. In India, for instance, Gen Z employees recorded counseling utilization growth rates exceeding 203% over the last two years, vastly outpacing older generations, with banking and financial service sectors seeing utilization surges of up to 408% 33.
However, the integration of therapeutic concepts into professional environments has generated significant intergenerational friction. While 92% of recent graduates desire the ability to discuss mental wellness at work, only 56% actually feel comfortable discussing these challenges with their managers, highlighting a gap between expectation and workplace reality 34. When younger employees utilize therapy speak to frame routine workplace stressors - such as critical performance feedback or tight deadlines - as "toxic" or "triggering," older managers often view this as a lack of professional resilience 3435.
Fascinatingly, the generation that popularized therapy speak is now the demographic most exhausted by it.

Surveys indicate that 25% of Gen Z report fatigue with therapy speak, compared to just 17% of Baby Boomers 435. Nearly one in four respondents acknowledge that therapy speak is frequently weaponized in arguments, and one in five recognize that it trivializes serious mental health conditions 35. This fatigue suggests a maturation of the mental health awareness movement. Having secured the vocabulary to discuss mental illness openly, the workforce is now grappling with the necessity for precision, recognizing that not every professional discomfort warrants a clinical diagnosis 2635.
Cross-Cultural Psychology: Is Therapy Speak a Global Export?
The current manifestation of therapy speak is deeply rooted in Eurocentric and Americentric models of psychology, which fundamentally prioritize individualism, autonomy, and self-actualization 4849. As these concepts spread globally via digital platforms, they frequently clash with the psychological frameworks of non-Western, collectivist cultures, raising concerns about cultural imperialism in mental health discourse 4950.
In Western therapy speak, concepts like "setting strict boundaries" and prioritizing "self-care" above all else are championed as the pinnacle of mental health. However, in cultures that center family, community, and interdependence, these concepts can be highly disruptive 4836. For example, in Latin American cultures, the concept of familismo (a deep dedication to extended family ties) governs social interaction 52. When Western therapy models instruct individuals to cut ties with "toxic" family members, it imposes a culturally foreign individualistic solution on a collective psychological system 4852.
Furthermore, global mental health professionals must navigate unique "idioms of distress" - ways in which different cultures experience and express psychological suffering that do not map cleanly onto the DSM-5. In Japan, while Western Social Anxiety Disorder centers on the fear of embarrassing oneself, the Japanese condition Taijin Kyofusho is the intense fear that one's body or presence is offensive and will embarrass others 36. In Latin America and the Mediterranean, the belief in the "evil eye" (Mal de Ojo) can manifest in intense paranoia regarding the safety of a child. In a Western clinical setting, this might be immediately pathologized as a delusional disorder; in its native cultural context, it is a recognized, albeit distressing, social reality 36. Emerging trends in Uganda and Ghana also show tension as Western "therapy speak" apps and platforms clash with indigenous coping mechanisms, such as turning to community counseling or Pentecostalism to explain overactivity and inattention 50.
The limitations of applying English-language therapy speak are also evident in bilingual therapy. Linguistic research demonstrates that an individual's first language is intimately connected to emotional and sensory memory 3652. First-generation immigrants often find that conducting therapy entirely in English feels overly clinical and disconnected. While they can articulate their boundaries perfectly in English, the raw emotional resonance of concepts like grief (pena) or anger (coraje) can only be fully accessed and processed in their native tongue 3652. Consequently, the global export of therapy speak risks erasing the nuanced, culturally specific ways in which human beings have historically managed distress.
Bridging the Gap: Effective Communication Without Jargon
The antidote to the misuse of therapy speak is not to abandon conversations about mental health, but to transition from superficial vocabulary toward genuine mental health literacy. Psychologists and communication experts suggest several practical frameworks to express needs effectively without relying on clinical buzzwords or diagnostic labels that shut down conversation.
Rather than relying on therapy speak to criticize what they do not want, individuals are encouraged to use the "GO" Method (Get clear), identifying what they actively want. Instead of diagnosing a partner as "avoidant," a person should clearly articulate, "I would like to spend more quality time together this week" 5354. Replacing clinical terms with descriptions of personal impact invites collaboration rather than defensiveness. Stating, "I feel overwhelmed and need help with these tasks" is highly effective; stating, "Your toxic expectations are dysregulating my nervous system" creates an adversarial dynamic 5455. Finally, when conflict arises, asking "How did you come to think this way?" forces the speaker to step out of diagnostic certainty and engage with the humanity of the other person, replacing clinical distance with actual empathy 31.
Bottom line
The widespread adoption of therapy speak has undeniably dismantled historical stigmas, empowering a generation to prioritize their psychological well-being and seek necessary care. However, the semantic dilution of terms like trauma, gaslighting, and narcissism risks trivializing the profound suffering of those with actual psychiatric disorders while replacing genuine human vulnerability with sterile, defensive labels. Moving forward, society must bridge the gap between superficial digital buzzwords and true mental health literacy, recognizing that true psychological resilience requires facing the messy realities of human connection without hiding behind the shield of a clinical diagnosis.