What Is CRISPR and How Is Gene Editing Used in Medicine
CRISPR is a revolutionary genetic technology that acts as programmable molecular scissors, allowing scientists to find, cut, and permanently alter specific sequences of DNA inside living cells. In medicine today, this technology has transitioned from a laboratory breakthrough to an approved clinical reality, successfully treating severe genetic blood disorders and advancing rapidly into human trials for cardiovascular disease, blindness, rare metabolic conditions, and chronic viral infections.
The Biological Mechanism: How CRISPR Works
To understand the profound impact of CRISPR on modern medicine, one must look at its origins in bacterial defense systems. CRISPR, which stands for Clustered Regularly Interspaced Short Palindromic Repeats, is naturally utilized by bacteria to fend off viral invaders 12. When a virus attacks a bacterium, the bacterium captures a snippet of the viral DNA and integrates it into its own genome as a CRISPR array, effectively creating a molecular memory of the attacker 2. If that same virus invades again, the bacterium produces RNA segments that match the viral sequence. These RNA segments guide an enzyme, typically Cas9, directly to the virus, where it acts as molecular scissors to slice the viral DNA apart, disabling the threat 214.
In 2012, geneticists recognized that this natural immune system could be repurposed into a programmable gene-editing tool 26. By synthesizing a custom guide RNA that matches a specific sequence of human DNA, scientists can direct the Cas9 enzyme to almost any targeted location in the human genome 47.
Once the Cas9 enzyme reaches its destination, it binds to the DNA and creates a double-strand break 48. From this point, the cell's natural repair mechanisms take over. If the goal is simply to turn off a malfunctioning gene, the cell's error-prone repair process will stitch the DNA back together, usually introducing small insertions or deletions that permanently disable the gene 4. Alternatively, if scientists provide a healthy donor DNA template alongside the CRISPR machinery, the cell can use this template to perform homology-directed repair, effectively overwriting the mutated sequence with the correct genetic code 49.
The Shift from Ex Vivo to In Vivo Editing
A critical distinction in modern CRISPR medicine is how the therapy is delivered to the patient. The field currently relies on two primary methodologies, each with distinct logistical and biological challenges.
Ex vivo therapy involves removing cells from the patient's body, modifying them in a highly controlled laboratory environment using CRISPR, and then infusing the edited cells back into the patient 1011. This is the approach used for the first approved CRISPR therapies targeting blood disorders, as blood stem cells can be reliably extracted, edited, and engrafted back into the bone marrow 212. However, this process is resource-intensive. It requires complex apheresis to collect the cells, specialized manufacturing facilities to edit them, and harsh chemotherapy conditioning regimens to prepare the patient's bone marrow for the return of the modified cells 213.
In vivo therapy delivers the CRISPR machinery directly into the patient's body, typically via an intravenous infusion or a direct tissue injection 101114. In this method, the guide RNA and Cas enzymes are often encased in tiny fat bubbles known as lipid nanoparticles, which naturally gravitate toward organs like the liver when introduced into the bloodstream 34. Alternatively, engineered viral vectors like adeno-associated viruses are used to carry the genetic instructions to specific tissues, such as the eye or inner ear 175. In vivo delivery is considered the ultimate goal of gene editing, as it transforms a complex, multi-month cellular transplant procedure into an accessible, single-visit outpatient infusion 14.
| Delivery Modality | Mechanism of Action | Clinical Advantages | Primary Challenges |
|---|---|---|---|
| Ex Vivo | Cells extracted, edited in a lab, and re-infused into the patient. | High editing precision; avoids triggering systemic immune responses to CRISPR proteins. | Extremely expensive; requires high-tech manufacturing and harsh chemotherapy conditioning. |
| In Vivo | Editing components injected directly into the patient's body. | Convenient outpatient administration; scalable; does not require cell extraction. | Hard to target specific organs outside the liver; risk of systemic off-target edits. |
The Evolution of Gene Editing: Beyond the Molecular Scissors
While traditional CRISPR-Cas9 has been highly successful, relying on the cell to randomly repair double-strand breaks introduces risks of unintended insertions, deletions, and broader off-target effects where the Cas9 enzyme might cut unintended areas of the genome 48. To circumvent these dangers, researchers have developed next-generation CRISPR tools that offer unprecedented precision.
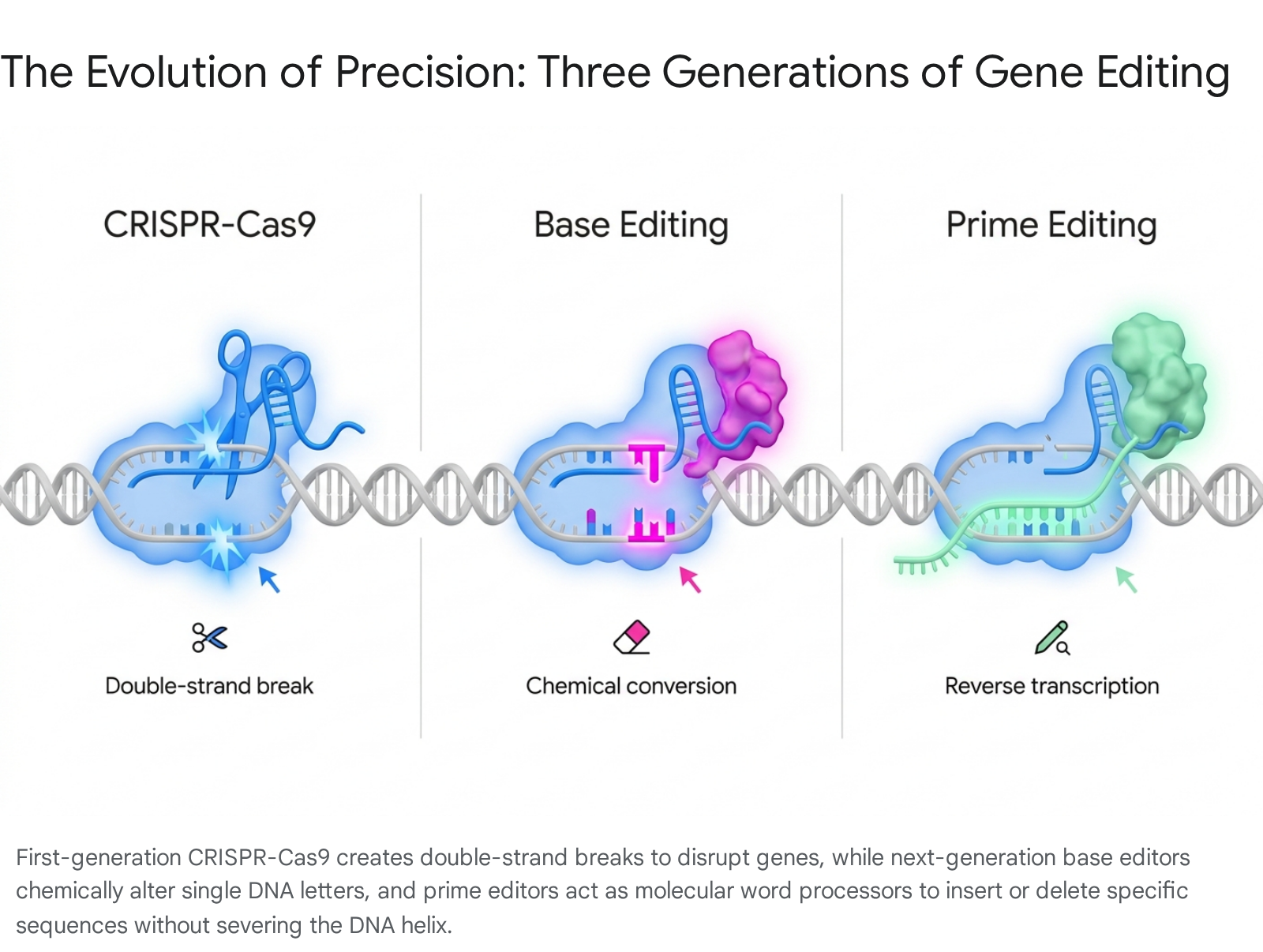
Base editing, first developed in 2016, utilizes a modified version of the Cas9 enzyme that has been disabled so it can no longer sever the DNA double helix 4819. Instead, the disabled Cas9 is tethered to a deaminase enzyme. Guided by RNA to the target site, this complex acts as a chemical eraser, directly converting one DNA letter into another without ever breaking the DNA backbone 819. Because it avoids double-strand breaks, base editing significantly lowers the risk of unintended off-target mutations, making it highly attractive for treating genetic diseases caused by single point mutations 48.
Prime editing, introduced in 2019, expands on this concept by acting as a comprehensive search-and-replace system for the genome 819. A prime editor fuses a Cas9 nickase to a reverse transcriptase enzyme. It employs a highly specialized prime editing guide RNA that not only guides the machinery to the target site but also carries the template of the new genetic code 48. The reverse transcriptase reads this template and writes the new DNA sequence directly into the genome 8. This allows prime editing to perform all twelve possible base-to-base transitions, as well as targeted insertions and deletions, theoretically allowing it to address the vast majority of all known disease-causing genetic variants 8196.
Epigenetic editing represents the newest frontier, where scientists are learning to turn genes on or off without altering the underlying DNA code at all. Recent breakthroughs have utilized modified CRISPR systems to remove chemical tags, known as methyl groups, that act as molecular anchors to silence genes 21. By demonstrating that DNA methylation directly controls gene activity, researchers have shown that genes can be safely reactivated without ever cutting the DNA strands, completely avoiding the risk of unintended genetic mutations or cancer-causing translocations associated with traditional editing 21.
| Editing Generation | Tool Used | Mechanism | Clinical Capability |
|---|---|---|---|
| First Generation | CRISPR-Cas9 | Double-strand break | Disrupts genes; can insert genes if a donor template is provided. |
| Second Generation | Base Editors | Chemical deamination | Converts single DNA letters (C→T, G→A, A→G, T→C) without breaking the helix. |
| Third Generation | Prime Editors | Reverse transcription | Search-and-replace editing; fixes point mutations, adds or deletes short sequences. |
| Fourth Generation | Epigenetic Editors | Methylation modification | Turns genes on or off by altering chemical tags without changing the DNA sequence. |
Historic Breakthroughs: The First Approved CRISPR Cures
The theoretical promise of CRISPR became a clinical reality in December 2023, when the U.S. Food and Drug Administration approved Casgevy (exagamglogene autotemcel), the world's first CRISPR-based therapy 267. Developed jointly by CRISPR Therapeutics and Vertex Pharmaceuticals, Casgevy was approved to treat Sickle Cell Disease and Transfusion-Dependent Beta Thalassemia in patients aged 12 and older 2923.
Both are severe, life-limiting inherited blood disorders caused by mutations in the beta-globin gene, resulting in flawed, sickle-shaped hemoglobin that impairs oxygen delivery and causes excruciating vaso-occlusive crises 28. Rather than attempting to fix the mutated adult hemoglobin gene directly, Casgevy employs an elegant biological workaround. Human beings possess a secondary hemoglobin gene that produces fetal hemoglobin in the womb. Shortly after birth, a regulatory gene called BCL11A turns off the production of fetal hemoglobin, and the body switches to producing adult hemoglobin, which is mutated in sickle cell patients 48. Casgevy uses CRISPR-Cas9 to target and disable the BCL11A enhancer within the patient's extracted hematopoietic stem cells 8. By breaking this genetic off-switch, the edited cells resume production of healthy fetal hemoglobin, which prevents the red blood cells from sickling 48.
The clinical results have been unprecedented. In late-stage trials, 97% of treated sickle cell patients, representing 16 out of 17 individuals with adequate follow-up, were entirely free of severe vaso-occlusive crises for at least 12 consecutive months 48. For patients with transfusion-dependent beta thalassemia, 25 out of 27 achieved transfusion independence, an outcome that dramatically alters their life trajectory and survival odds 4.
Contrast with Gene Addition Therapies
It is important to differentiate between true CRISPR gene editing and traditional gene addition therapies, which are also achieving regulatory milestones. On the exact same day Casgevy was approved, the FDA also approved Lyfgenia (lovo-cel) for Sickle Cell Disease 213. Lyfgenia uses a disabled lentivirus to insert a modified, functional gene into the patient's cells, rather than editing the patient's native DNA with CRISPR 28.
Similarly, in April 2026, the FDA granted accelerated approval to Otarmeni (lunsotogene parvec-cwha), a landmark treatment by Regeneron for a rare genetic form of profound hearing loss linked to OTOF gene mutations 52526. While frequently discussed alongside genomic medicine breakthroughs, Otarmeni is not a CRISPR therapy. It utilizes a novel dual adeno-associated virus system to deliver functional copies of the OTOF gene directly into the inner ear via surgical infusion 2627. Because the OTOF gene is too large for a single viral vector to carry, the payload is split across two vectors that reconstitute inside the cochlear cells, restoring the production of the otoferlin protein and allowing patients to gain functional hearing 2627. In pivotal trials, 80% of patients receiving Otarmeni achieved hearing thresholds that allow for natural functional hearing without cochlear implants 2526.
Treating Common Chronic Diseases: The Next Frontier
Initially, CRISPR therapies were strictly relegated to ultra-rare genetic monogenic disorders. However, by 2026, the clinical landscape expanded aggressively to target common chronic conditions affecting millions of people, marking a pivotal shift in the pharmaceutical industry's approach to genomic medicine.
Cardiovascular Disease: Editing the Liver
Perhaps the most significant leap for CRISPR is its application in cardiovascular disease, the leading cause of death globally. High levels of low-density lipoprotein cholesterol are a major risk factor for heart attacks, primarily regulated by proteins synthesized in the liver, such as PCSK9 and ANGPTL3 46.
Biotechnology companies like Verve Therapeutics, which was acquired by Eli Lilly in 2025, have pioneered in vivo base editing to permanently lower cholesterol. Administered via a single infusion of lipid nanoparticles, their candidate VERVE-102 targets and inactivates the PCSK9 gene in the liver 69. Phase 1 clinical data released in mid-2025 demonstrated that a single dose reduced PCSK9 protein levels by up to 88% and slashed bad cholesterol by up to 62%, with durability holding steady over multiple years 469. Because this is a permanent genetic alteration, it effectively replaces a lifetime of daily statin pills or biweekly injections with a single, protective genetic intervention 4.
Similarly, CRISPR Therapeutics has advanced its candidate CTX310 to target ANGPTL3, another lipid-regulating protein, achieving roughly 50% reductions in both triglycerides and bad cholesterol in Phase 1 trials 623.
Autoimmune Disorders: Engineering the Immune System
The application of CRISPR is also revolutionizing the treatment of severe autoimmune diseases. In these conditions, the body's immune system erroneously attacks healthy tissue. Researchers are now using CRISPR to edit CAR-T cells - immune cells extracted from the patient, engineered to hunt specific targets, and infused back into the body.
CRISPR Therapeutics has launched a Phase 1 clinical trial utilizing a CRISPR-edited CAR-T therapy called zugo-cel to treat systemic lupus erythematosus (SLE) 46. The therapy is designed to target CD19, effectively hunting down and depleting the rogue B-cells responsible for the autoimmune attack 4. The early results have been highly promising, with patients experiencing no severe side effects and showing immense clinical improvement. Notably, one patient suffering from severe systemic lupus achieved complete remission, recording a disease activity score of zero following the therapy 423. This represents the first successful application of a CRISPR-based therapy to drive remission in a complex autoimmune disease.
Tackling Rare and Inherited Conditions
While the expansion into common diseases is lucrative, CRISPR continues to offer unprecedented hope for patients with exceedingly rare, degenerative, and previously untreatable conditions.
Hereditary Angioedema and Amyloidosis
In vivo CRISPR is proving highly adept at targeting the liver to halt systemic disorders. Intellia Therapeutics has led this charge with two prominent candidates. The first is lonvoguran ziclumeran, known as NTLA-2002, which targets Hereditary Angioedema. This is a potentially fatal condition characterized by severe, unpredictable swelling attacks driven by elevated bradykinin levels. NTLA-2002 utilizes CRISPR-Cas9 to permanently inactivate the KLKB1 gene in the liver, choking off the production of the precursor proteins that cause the swelling 1430. In April 2026, Intellia reported stellar Phase 3 results showing a single outpatient infusion reduced swelling attack rates by 87% 1431. Intellia has initiated a rolling Biologics License Application with the FDA, expecting a commercial launch in the first half of 2027 143132.
The second candidate, nexiguran ziclumeran or NTLA-2001, targets Transthyretin Amyloidosis. This disease occurs when the liver produces misfolded proteins that build up in the heart and nerves, leading to fatal cardiomyopathy 33. Intellia's therapy targets the specific gene to halt this toxic production 634. This program highlighted the precarious safety tightrope of in vivo therapies: in late 2025, the FDA placed a clinical hold on the Phase 3 trial after a patient experienced life-threatening liver toxicity and died 3334. However, by early 2026, the FDA lifted the hold after Intellia implemented stricter safety monitoring protocols, highlighting the regulatory learning curve required for systemic genome editing 333536.
Restoring Vision and Curing Metabolic Deficiencies
CRISPR is also being utilized to treat inherited blindness. In a Phase 1/2 clinical trial called BRILLIANCE, researchers tested a CRISPR therapy named EDIT-101 on patients born with Leber Congenital Amaurosis Type 10, a rare form of blindness caused by a mutation in the CEP290 gene 717. Because the mutated gene is too large for standard viral gene addition therapies, researchers injected the CRISPR machinery directly into the patients' eyes to cut out the mutation 1737. The trial reported that 11 of the 14 participants experienced measurable improvements in visual acuity and retinal sensitivity, proving that in vivo editing of the human eye is both safe and functionally effective 717.
Furthermore, base editing and prime editing are demonstrating profound efficacy in treating rare metabolic and immune deficiencies. Beam Therapeutics utilized base editing for Alpha-1 Antitrypsin Deficiency, delivering the editors to the liver to correct a mutant protein. In their highest dose cohort, 90% of the protein in participants' blood was successfully corrected to the healthy version within 14 days 4196. Meanwhile, Prime Medicine published the first-in-human data utilizing prime editing to correct Chronic Granulomatous Disease, achieving gene correction rates of 69% to 83% in patients, marking a major milestone for the newest generation of editing tools 419.
The Quest for a Functional HIV Cure
For decades, a cure for the Human Immunodeficiency Virus (HIV) has remained elusive because the virus integrates its DNA directly into the genome of the host's immune cells, creating a dormant reservoir that standard daily medication cannot reach 3839.
In a major 2026 breakthrough, researchers at China's Wuhan University of Science and Technology published data on a novel delivery system that could offer a functional cure 3840. Recognizing that standard lipid nanoparticles struggle to effectively penetrate immune cells, the team loaded the CRISPR-Cas12a enzyme into exosomes, which are naturally occurring biological nanoscale vesicles that act as intercellular couriers 383940.
These engineered exosomes acted as stealth delivery vehicles, fusing with infected immune cells and delivering the Cas12a payload directly into the latent reservoir 39. Once inside, Cas12a recognized the integrated proviral DNA and systematically shredded the viral genetic blueprint 383910. In humanized mouse models, the treatment led to complete viral eradication and restored immune cell counts in two-thirds of the subjects, positioning the platform as a viable path toward a pill-free cure for the 39 million people living with HIV globally 384010.
The "Bespoke" Revolution: Personalized Medicine and the FDA
Traditional drug development follows a rigid model: identify a disease affecting millions, run massive clinical trials, and market the exact same chemical compound to everyone. This economic model actively punishes patients with ultra-rare, idiosyncratic genetic mutations 42.
In mid-2025, a landmark medical case forced regulators to adapt. An infant known as Baby KJ was born with severe carbamoyl phosphate synthetase 1 deficiency, an ultra-rare metabolic disorder 311. KJ's body lacked the enzyme necessary to break down dietary protein, leading to a toxic accumulation of ammonia capable of causing permanent brain damage or death within days 344.
Because the child was too small to survive a liver transplant, researchers at the Innovative Genomics Institute and the Children's Hospital of Philadelphia raced to engineer a custom-built mRNA CRISPR base-editing therapy specifically tailored to KJ's unique genetic mutation 3445. Manufactured and approved under emergency single-patient protocols in an unprecedented six months, the bespoke therapy was delivered via lipid nanoparticles into KJ's liver 44445. Following treatment, the infant regained the ability to process dietary protein, completely avoiding the need for a transplant and demonstrating the power of on-demand genomic medicine 31146.
The Plausible Mechanism Framework
Baby KJ's survival prompted a profound regulatory shift. In February 2026, the FDA formally unveiled the Plausible Mechanism Pathway for bespoke genetic medicines 464748.
This revolutionary draft guidance acknowledges that CRISPR therapies are highly modular; only the guide RNA changes from one patient to the next, while the Cas protein and lipid nanoparticle delivery vehicle remain identical 44445. Under the new framework, if a sponsor proves the underlying biological mechanism of a disease is understood and demonstrates successful target editing, they can submit a single regulatory application covering multiple targets within a single gene 424749. By treating the CRISPR system as an established platform rather than treating every new guide RNA as a brand-new drug requiring years of animal testing, the FDA has opened the door to rapid, personalized gene editing for thousands of rare inherited disorders 44447.
The Economics of Curing Disease
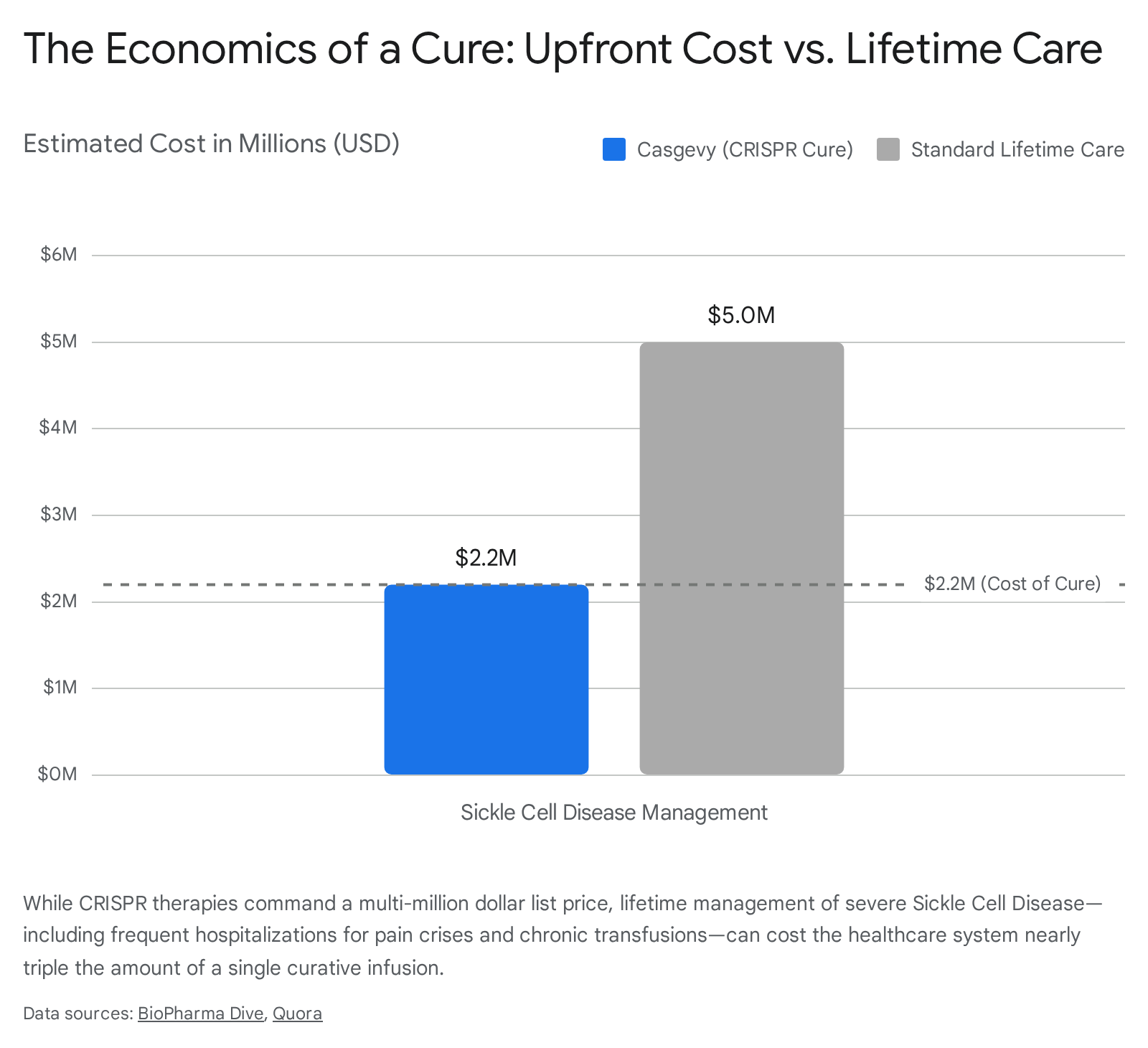
As the clinical triumphs of CRISPR multiply, the focus has increasingly shifted toward the sobering reality of commercial access. The list price of Casgevy is $2.2 million per patient, while the gene addition therapy Lyfgenia is priced at $3.1 million, placing them among the most expensive medical treatments in history 212.
However, health economists emphasize that the sticker shock of gene therapies must be weighed against the lifetime burden of chronic disease management. A patient with severe sickle cell disease requires regular blood transfusions, suffers unpredictable pain crises necessitating emergency hospitalizations, and faces high risks of organ damage 812. The lifetime healthcare cost for a severely afflicted patient averages between $4 million and $6 million 1251.
Furthermore, when accounting for the patient's regained ability to work and overall quality-of-life improvements, simulation models indicate that a multi-million dollar single-dose cure actually falls well within acceptable cost-effectiveness thresholds 5152.
Global Access: Leaving No One Behind
Despite long-term cost-effectiveness, the upfront logistical and financial hurdles create severe accessibility bottlenecks globally. Sickle cell disease predominantly impacts populations of African descent, with the highest disease burden located in sub-Saharan Africa, where approximately 1,000 children are born with the condition daily 12. Currently, the ex vivo requirement for Casgevy demands sophisticated bone marrow transplant infrastructure and stem cell mobilization capabilities, of which there are currently only three clinical centers serving all of sub-Saharan Africa 1213.
Recognizing this critical gap, international coalitions are mobilizing to ensure developing nations are not left behind. The BRICS 2025 - 2030 Innovation Action Plan explicitly prioritizes the democratization of advanced biotechnologies, with collaborative investments spanning Brazil, India, and South Africa to develop localized genomic infrastructure 13. Additionally, facilities like the KRISP laboratory in South Africa have opened to establish cutting-edge epigenetic editing capacities on the continent 2. Ultimately, the transition from complex ex vivo cellular transplant therapies to simple in vivo nanoparticle infusions will be the critical technological leap required to deliver genetic cures to resource-limited healthcare systems worldwide 128.
Myths vs. Facts: What CRISPR Cannot Do
As CRISPR embeds itself into clinical practice, it is equally important to dispel the science-fiction myths that continue to cloud public perception.
One pervasive myth is that CRISPR will be used to create customized designer babies. The fear that parents will soon order highly intelligent or hyper-athletic children misunderstands fundamental human genetics . Complex traits like intelligence, height, and athletic ability are highly polygenic, meaning they are influenced by the complex interplay of hundreds of different genes alongside powerful environmental and nutritional factors . CRISPR excels at fixing single-gene monogenic disorders, but the biological map required to engineer complex human traits simply does not exist .
Another common misconception is that CRISPR is flawlessly precise. While highly targeted, traditional CRISPR-Cas9 is not infallible. It can induce unintended off-target mutations at sites that chemically resemble the intended target, occasionally causing translocations or unintended cellular stress that could lead to malignancies 45556. This is why the regulatory review process requires intense long-term safety monitoring, and why the field is rapidly pivoting toward non-cutting alternatives like base and prime editing to mitigate these risks 41155.
Bottom line
CRISPR has unequivocally transitioned from a Nobel Prize-winning laboratory phenomenon into an approved, transformative medical therapy. With the landmark approval of Casgevy for blood disorders, the successful deployment of bespoke therapies for rare infant metabolic diseases, and late-stage clinical data proving highly effective in vivo editing for cardiovascular and autoimmune conditions, the technology is fundamentally rewriting the boundaries of modern medicine. However, significant uncertainties remain regarding long-term off-target safety risks, the durability of epigenetic edits, and the daunting challenge of manufacturing and distributing multi-million dollar therapies equitably to the populations that need them most.