Clinical applications and limitations of digital twins in medicine
Baseline Definitions and Taxonomic Classification
The integration of high-dimensional clinical data, predictive algorithms, and continuous physiological telemetry has facilitated the rapid development of human digital twins in medicine. A medical digital twin is strictly defined as a highly personalized, dynamically updated virtual replica of a patient's anatomical, physiological, or metabolic state, designed to execute predictive simulations that directly inform clinical decision-making 12. As of 2026, the technology has transcended theoretical modeling and is actively deployed across multiple biological scales, ranging from single-organ mechanistic models in cardiovascular surgery to synthetic patient cohorts utilized in oncology clinical trials.
Despite the widespread commercial adoption of the terminology, a rigorous taxonomic distinction is necessary to evaluate the current clinical landscape accurately. According to the foundational criteria established by the National Academies of Sciences, Engineering, and Medicine (NASEM), a true medical digital twin requires bidirectional data exchange, high-fidelity personalization, predictive forecasting capabilities, and explicit uncertainty quantification 2. A comprehensive 2025 scoping review published in npj Digital Medicine analyzed 149 active healthcare applications claiming digital twin capabilities and found that only 12% fully met the strict NASEM criteria 2.
The vast majority of currently deployed systems function either as "digital shadows" - where clinical data flows unidirectionally from the physical patient to update the digital model without automated, closed-loop therapeutic feedback - or as virtual patient cohorts based on statistical population averages rather than individualized pathophysiology 12. Furthermore, the review noted that critical mechanisms for verification, validation, and uncertainty quantification (VVUQ) were explicitly detailed in only a small fraction of studies, highlighting a gap between commercial marketing and validated clinical simulation 2.
System Architectures and Multi-Omics Integration
The architectural framework of a medical digital twin generally comprises three distinct strata: the physical entity (the patient and their localized environment), the virtual entity (the computational models simulating biological function), and the information processing layer (the data pipelines, sensors, and artificial intelligence algorithms mediating the connection) 1. The methodology employed within the modeling block varies fundamentally depending on the clinical domain. In fields governed by well-established physical laws, such as cardiology and orthopedics, systems primarily rely on mechanistic models including computational fluid dynamics (CFD) and finite element modeling (FEM) to represent blood flow and tissue mechanics 34.
Conversely, in systemic disciplines such as oncology and metabolic medicine, the underlying mechanisms are highly complex and less deterministic. In these domains, digital twins rely heavily on data-driven approaches, utilizing deep learning (DL) and machine learning (ML) architectures to map input variables - ranging from electronic health records to continuous wearable telemetry and multi-omics sequencing - to clinical outcomes 56.
Transformer-Based Neural Architectures
As digital twin applications expand into precision oncology and systemic disease management, the ability to effectively integrate heterogeneous multi-omics data (genomics, transcriptomics, proteomics, metabolomics, and radiomics) has emerged as a central architectural challenge. Traditional data integration methods often rely on simple concatenation strategies, which frequently fail to capture the complex, non-linear interactions across different biological regulatory layers 7. This approach obscures crucial cross-talk mechanisms and introduces the "curse of dimensionality," where the sheer volume of variables degrades algorithmic performance 78.
By 2026, the prevailing solution to this integration bottleneck relies on advanced Transformer-based neural network architectures. Originally designed for natural language processing, Transformers utilize self-attention mechanisms to weigh the relative importance of millions of biological features simultaneously, identifying latent relationships and regulatory dependencies without explicitly programmed rules 910.
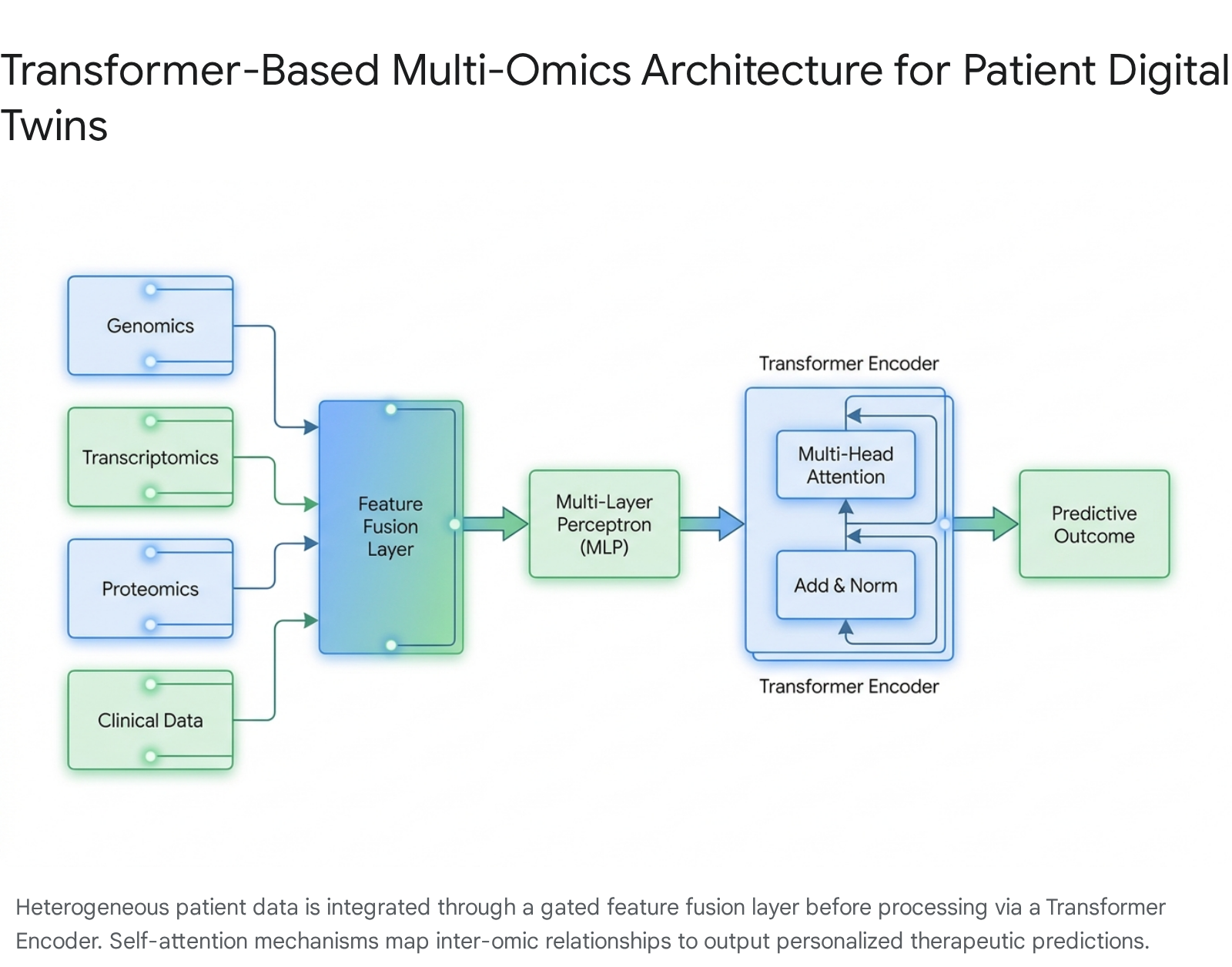
Frameworks such as DeePathNet integrate specific cancer pathway knowledge with multi-omics data. By mapping the interdependency among biological pathways via a Transformer module, the system predicts drug responses and classifies cancer subtypes while preserving a degree of biological interpretability that is typically absent from black-box deep learning models 8. Evaluations of specific architectural variations, such as the MultiOmicsTransformerFusion model, demonstrate that gated fusion - which processes and normalizes the distinct characteristics of each biological modality independently before combining them - yields superior predictive accuracy compared to models that attempt complex cross-modal interactions too early in the network hierarchy 9.
The clinical superiority of this multi-omics integration is quantifiable in recent deployments. In predictive models developed for assessing preterm birth risk, algorithms trained exclusively on single modalities like cell-free DNA (cfDNA) or cell-free RNA (cfRNA) achieved area under the receiver operating characteristic curve (AUC) metrics of 0.822 and 0.851, respectively 8. However, when integrated within a unified Transformer-based framework, the combined multi-omics model achieved an AUC of 0.890, demonstrating a statistically significant improvement in risk assessment fidelity 8. These multilayer network scaffolds now provide the necessary mathematical foundation for oncology digital twins capable of simulating disease progression across both spatial and temporal biological scales 7.
Global Regulatory Frameworks and Engineering Standards
The regulatory landscape for medical digital twins, in silico clinical trials, and artificial intelligence as a medical device (AIaMD) has matured significantly by 2026. Regulatory bodies across major global jurisdictions have moved from issuing conceptual guidance documents to actively enforcing strict evaluation frameworks and continuous post-market surveillance.
United States Food and Drug Administration Authorization
The United States Food and Drug Administration (FDA) has recognized the limitations and escalating costs of traditional human and animal testing, actively encouraging the use of computational modeling and simulation (CM&S) as valid scientific evidence in regulatory submissions 12. Through the end of 2025, the FDA authorized a cumulative total of 1,451 AI/ML-enabled medical devices 13. Radiology constitutes the overwhelming majority of these authorizations, representing approximately 76% of all cleared devices, followed by cardiology at roughly 9% 1314. The vast majority of these devices have entered the market via the 510(k) pathway, reflecting a regulatory reliance on proving substantial equivalence to existing predicate devices rather than pursuing the more costly and time-intensive premarket approval (PMA) process 13.
The historical data demonstrates a consistent and exponential upward trend in regulatory clearances over the past decade, underscoring the rapid transition of AI-driven healthcare tools from academic research into commercial deployment.
| Year | Annual FDA Authorizations for AI/ML-Enabled Medical Devices |
|---|---|
| 2015 | 6 |
| 2022 | 91 |
| 2023 | 221 |
| 2024 | 253 |
| 2025 | 295 |
Data representing the acceleration of FDA clearances for algorithmic and AI-based medical devices 13.
To establish the credibility of digital twins for regulatory submissions, the FDA relies heavily on established engineering frameworks, specifically the American Society of Mechanical Engineers (ASME) V&V 40 standard, titled "Assessing Credibility of Computational Modeling through Verification and Validation: Application to Medical Devices" 129. The V&V 40 standard mandates that developers define a specific "Question of Interest" (the exact problem the simulation addresses) and a "Context of Use" (the degree of reliance placed on the model for regulatory decision-making) 12. If a digital twin is intended to replace a critical safety test in a high-risk human trial, the evidentiary burden requires rigorous and transparent validation against real-world biological data, extensive sensitivity analysis across parameter ranges, and robust version control mechanisms 1216.
United Kingdom Medicines and Healthcare products Regulatory Agency
The UK Medicines and Healthcare products Regulatory Agency (MHRA) has implemented a comprehensive reform program for Software as a Medical Device throughout 2025 and 2026 17. The regulatory transition is anchored by three core principles co-developed through international collaboration with the FDA and Health Canada: Good Machine Learning Practices (GMLP), Predetermined Change Control Plans (PCCPs), and specific Transparency Guidelines 17.
In June 2025, stringent new Post-Market Surveillance (PMS) regulations came into force, establishing rigorous monitoring and reporting requirements for deployed AI algorithms to ensure their performance does not degrade over time 1710. Furthermore, pre-market statutory instruments expected to take full effect in 2026 will mandate updated conformity assessment procedures and revised in vitro diagnostic classification rules, which directly impact predictive multi-omics software platforms operating in the UK market 17. The MHRA has explicitly clarified that AI models used for a "medical purpose" - such as predicting patient deterioration or recommending targeted therapies - are highly likely to fall within the definition of a general medical device, subjecting them to the UK Medical Device Regulations (MDR) and potential up-classification to higher risk tiers 10.
Japan Pharmaceuticals and Medical Devices Agency
Japan's Pharmaceuticals and Medical Devices Agency (PMDA) has accelerated its regulatory modernization to support the deployment of medical digital twins. The 2019 amendment to the Pharmaceutical and Medical Devices Act established a robust Unique Device Identification (UDI) system that became fully mandatory and integrated by 2025 19. This system provides the essential traceability infrastructure necessary for the post-market surveillance of digital health tools and enables seamless electronic labeling (e-IFU) integration 19.
For software and algorithm developers, the PMDA operates a dedicated SaMD One-Stop Consultation Desk to expedite reviews and provide early guidance on clinical data requirements 11. Additionally, the PMDA mandated eCTD v4.0 electronic submissions starting in April 2026, positioning Japan as the first major regulatory authority to require this modernized format for pharmaceutical and device approvals 21. To overcome historically slow approval times and mitigate the "drug lag," Japan extensively utilizes the SAKIGAKE expedited pathway. This program targets a highly accelerated six-month review timeline for novel therapies and diagnostic tools addressing serious unmet medical needs, provided the technology is submitted for review in Japan first 21.
Virtualization of Clinical Trials and Synthetic Control Arms
One of the most consequential operational deployments of digital twin technology in 2026 is the virtualization of clinical trials. This application explicitly addresses the profound inefficiencies, escalating costs, and ethical dilemmas associated with traditional randomized controlled trials (RCTs). In conventional Phase III clinical trials, thousands of patients are recruited and randomized, with a substantial cohort receiving a standard-of-care or placebo treatment to establish a comparative baseline 12. By generating patient-specific digital twins utilizing deep learning models trained on vast repositories of historical clinical data, biopharmaceutical companies can construct "synthetic control arms" or "computational control arms" 1213. These models effectively predict how an individual patient would respond physiologically if they were assigned to the control group, based on their specific baseline characteristics 1324.
Commercial Platforms and Predictive Accuracy
Unlearn.AI has established substantial regulatory validation and commercial traction in the clinical trial sector with its TwinRCT platform 1426. The platform generates digital twins that accurately simulate patient outcomes under control conditions, enabling trial sponsors to reduce physical control arm sizes by up to 35% to 50% 272829. This reduction significantly cuts trial timelines and operational costs while allowing a higher proportion of enrolled patients to access the experimental therapy 2729. Unlearn.AI secured a formal Qualification Opinion from the European Medicines Agency (EMA) for its PROCOVA procedure, marking the first time a major regulatory body formally supported a machine-learning-based method for reducing pivotal Phase II and Phase III trial sample sizes 2627. Following a $50 million Series C funding round in 2024, the company has expanded its deployments from neurology into immunology and metabolic disease trials, partnering with leading global pharmaceutical corporations 262728.
Altis Labs has pioneered computational imaging digital twins specifically within the oncology sector through its proprietary Nota platform. Altis trains deep learning models on an expansive repository of over 182 million real-world medical images, matched with diagnostic records and longitudinal outcomes 2430. Instead of relying on the traditional RECIST (Response Evaluation Criteria in Solid Tumors) standard - which depends on relatively simplistic, unidimensional tumor measurements - the Altis IPRO (Imaging-Based Prognostication) AI model analyzes millions of complex imaging features early in the clinical study to predict overall survival (OS) and patient progression 3132.
In a high-profile demonstration of clinical utility, Altis Labs partnered with AstraZeneca to reanalyze historical data from the 2017 MYSTIC lung cancer trial, which had originally failed to meet its primary endpoints 24. The AI model successfully predicted overall survival outcomes with significantly greater prognostic discrimination than conventional staging metrics 2433. By accurately differentiating between true treatment responders and stable patients with unfavorable long-term prognoses, the digital twin approach enables sophisticated patient stratification, facilitating adaptive trial designs where treatment regimens can be adjusted mid-trial based on evolving patient risk profiles 31.
Oncology Simulations and Survival Predictions
Similarly, the FarrSight-Twin technology utilizes computational frameworks originally designed for astrophysics algorithms to model individual therapeutic responses to chemotherapy and immunotherapy across multiple cancer types 15. Integrating deep clinical and genetic data, researchers utilized the platform to simulate patient outcomes across eight distinct clinical trials. The digital twin model accurately predicted the log odds ratio for overall response rates (ORR) in each treatment arm, demonstrating remarkably strong alignment with the actual clinical outcomes reported in the physical trials 1535.
Furthermore, a retrospective analysis applying the FarrSight-Twin model to the The Cancer Genome Atlas Program cohort revealed significant findings: patients who received the specific standard-of-care treatments recommended by the digital twin model exhibited noticeably better therapeutic responses and significantly improved survival outcomes compared to patients receiving alternative standard therapies 1516. This approach enhances single-arm clinical trials by enabling individual patients to serve as their own synthetic controls, drastically improving trial interpretation for rare cancers where large patient cohorts are impossible to recruit 3516.
Cardiovascular Anatomical Modeling and Interventional Planning
Cardiology represents the most mature and widely deployed clinical domain for anatomical digital twins. Because the human heart functions as a complex electro-mechanical pump governed by the fundamental physical laws of fluid dynamics, tissue elasticity, and electrical signal propagation, it is uniquely suited to physics-based mechanistic modeling 34.
Non-Invasive Diagnostics and Hemodynamic Simulation
A prominent example of FDA-cleared, commercially deployed digital twin technology is the HeartFlow FFRCT Analysis. Utilizing standard, non-invasive coronary computed tomography angiography (CCTA), the software generates a personalized, three-dimensional digital replica of a patient's coronary arteries. It then applies complex computational fluid dynamics to simulate blood flow through the vessels, calculating the fractional flow reserve (FFR) to diagnose ischemia accurately without subjecting the patient to an invasive cardiac catheterization procedure 1718.
In September 2025, HeartFlow received subsequent FDA 510(k) clearance for its Next Generation Plaque Analysis algorithm 19. Trained on a massive dataset of approximately 273,000 patients, the updated AI model provides highly detailed, color-coded, 3D visualizations that quantify coronary plaque volume, specific plaque type, and overall distribution 18. The algorithm demonstrated a 21% improvement in plaque detection accuracy over previous iterations and established a 95% agreement rate with the invasive gold standard of intravascular ultrasound (IVUS) 1819. The clinical utility and economic viability of this non-invasive technology are evidenced by its widespread payer adoption; major national insurers in the United States, including UnitedHealthcare and Cigna, mandated coverage for the platform across commercial and Medicare Advantage plans in late 2025 20.
Electrophysiology and Surgical Navigation
In the highly specialized realm of electrophysiology, the France-based firm inHEART provides an AI-driven digital twin tailored specifically for planning complex cardiac ablation procedures, targeting critical arrhythmias such as ventricular tachycardia (VT) 4221. The software module, which received FDA 510(k) clearance in March 2024, employs fully automated segmentation of preoperative CT and MRI scans to create an interactive, high-fidelity 3D model of the patient's unique cardiac anatomy 4222.
Crucially, the inHEART digital twin visualizes microscopic myocardial tissue characteristics - such as ventricular wall thinning and the precise location of arrhythmogenic scar tissue corridors - that are often impossible to discern during conventional intraoperative mapping 42. By pre-planning the ablation targets digitally on the virtual twin, clinicians have been able to reduce procedural durations in the operating room by 60% (dropping from an average of five hours to under two hours) 2122. Furthermore, clinical evaluations demonstrated that these image-guided ablations decreased VT recurrence rates by 38% compared to conventional, non-digitally planned ablation strategies 21. The system is engineered for direct integration with existing electroanatomic mapping (EAM) systems in the catheterization laboratory, seamlessly bridging the gap between preoperative digital simulation and physical intraoperative execution 4221.
In Silico Device Testing and Medical Engineering
Beyond procedural planning, digital twins are aggressively replacing traditional animal models in the research, development, and regulatory approval of novel medical devices. Virtonomy's v-Patients platform enables medical device manufacturers to test cardiovascular implants virtually across an extensive database of real clinical anatomies encompassing diverse demographic and pathological variations 45.
For example, Scandinavian Realheart utilized the v-Patients platform to conduct in silico fatigue simulations and virtual implantations of their developmental Total Artificial Heart (TAH) 4623. The platform allowed the company to identify precise anatomical fit parameters and long-term durability metrics under varying physiological loads prior to initiating First-in-Human trials 4623. Utilizing advanced GPU-accelerated computing infrastructure, Virtonomy compressed complex fluid dynamics and tissue interaction simulation workflows that would traditionally require months of physical bench testing into a matter of weeks, providing the exact computational evidence required by regulators under the ASME V&V 40 framework 1248.
| Clinical Domain | Specific Application | Key Digital Twin Technology / Vendor | Primary Outcome Metric |
|---|---|---|---|
| Cardiology | Coronary Ischemia Detection | HeartFlow FFRCT | Fractional Flow Reserve (FFR) diagnostic agreement with invasive IVUS. |
| Cardiology | Ventricular Tachycardia Ablation | inHEART Models | Procedure duration reduction; Long-term arrhythmia recurrence rate. |
| Medical Device R&D | Implant Simulation & Fatigue Testing | Virtonomy v-Patients | Verification of anatomical fit and mechanical durability prior to human trials. |
| Oncology / Pharmacology | Synthetic Control Arms for Trials | Unlearn.AI TwinRCT | Reduction in required physical trial sample sizes and acceleration of trial timelines. |
The MEDITWIN Consortium and National Initiatives
Recognizing the strategic importance of virtual healthcare modeling, national governments are heavily subsidizing the industrialization of digital twins. In France, Dassault Systèmes has significantly expanded its pioneering Living Heart Project into the national MEDITWIN consortium. Announced in late 2023 and generously funded by the French government's "France 2030" investment plan, the five-year MEDITWIN initiative unites 14 public and private partners 4950. The alliance includes Inria (the French national research institute for digital science and technology) and seven leading University Hospital Institutes (IHUs) 50.
The primary objective of the consortium is to industrialize, clinically validate, and standardize digital twin technologies to ensure equitable healthcare deployment. The project explicitly targets the development and commercialization of seven distinct "virtual healthcare products" spanning medical practices in cardiology, neurology, and oncology, all deployed on a sovereign, secure industrial cloud platform 50. In early 2025, Dassault Systèmes launched a beta test of a fully parametric, next-generation Living Heart model 51. This advanced iteration allows clinicians and engineers to adjust tissue properties, structural anomalies, and hemodynamic variables instantly at the touch of a button 51. Because it is built upon years of data from real patients, it serves as a robust training engine for generative AI, accelerating medical device testing under extreme physiological parameters without requiring animal subjects 51.
Metabolic Digital Twins and Precision Nutrition
While anatomical digital twins excel in mechanical disciplines like procedural cardiology, metabolic digital twins are scaling rapidly in the realm of chronic disease management, particularly for obesity, prediabetes, and Type 2 diabetes. The biological complexity of human metabolism dictates that generalized dietary guidelines frequently fail to address immense inter-individual variability; identically composed meals can provoke vastly different glycemic and insulinemic responses across different patients, even among identical twins sharing the same DNA 52.
Twin Health represents a vanguard deployment in this sector, having secured $53 million in a 2025 funding round that valued the company at nearly $1 billion 53. The platform generates a "Whole Body Digital Twin" - a hyper-personalized digital replica of a patient's metabolism 5455. This model is constructed using continuous, real-time data streams ingested from continuous glucose monitors (CGMs), wearable fitness trackers measuring sleep and activity, blood laboratory results, and self-reported meal logs 5355. By continuously simulating a patient's metabolic state and utilizing machine learning to identify specific nutritional triggers, the AI engine prescribes highly granular, individualized behavioral interventions 5255.
The clinical outcomes reported by Twin Health surpass those of traditional first-generation digital health lifestyle interventions. A gold-standard randomized controlled trial published in the New England Journal of Medicine Catalyst rigorously validated the platform's efficacy 55. According to the published results, 71% of participating members reversed their type 2 diabetes diagnosis 53. Furthermore, 95% of participants engaged in the full digital twin program achieved an HbA1c level below 6.5% - the established threshold for clinical remission - without the use of medication 52. Crucially for the healthcare economics landscape, 81% of patients enrolled in the program successfully eliminated their reliance on high-cost GLP-1 receptor agonists, demonstrating substantial economic viability for health plans and employers seeking to curb escalating pharmaceutical expenditures 5355.
However, regulatory nuance is required when analyzing the deployment of metabolic digital twins. While the hardware inputs - such as the Dexcom and Signos CGMs - are fully FDA-cleared medical devices, comprehensive "Whole Body Digital Twin" platforms frequently operate legally as clinical decision support software or general wellness tools, rather than Class II or Class III Software as a Medical Device (SaMD) subject to strict pre-market approval regarding their underlying predictive algorithms 1453.
Algorithmic Bias and Health Equity Limitations
As the deployment of medical digital twins accelerates across health systems, the systemic infusion of algorithmic bias remains a critical and unresolved limitation. Artificial intelligence models, regardless of their architectural sophistication, are acutely susceptible to replicating and amplifying historical inequities embedded within their training datasets 5657.
The introduction of bias occurs through multiple entry points across the development lifecycle. The primary vector is historical underrepresentation and skewed training data. Populations bearing the heaviest burden of specific diseases - such as cardiovascular disease among Black populations in the United States, the UK, and sub-Saharan Africa - are frequently the least represented in the clinical data cohorts used to train predictive algorithms 5657. Consequently, an algorithm may misclassify disease presentation, predict risk inaccurately, and recommend inappropriate treatment regimens for marginalized demographics simply because it has not learned to recognize their specific physiological baselines or disease markers (e.g., dermatological models failing on dark skin, or cardiovascular models failing on female presentations of ischemia) 5657.
A secondary vector involves the unintentional use of proxy variables. For instance, due to historical structural barriers and healthcare system inequities, Black patients have historically received less frequent care and fewer expensive diagnostic interventions 57. Consequently, their electronic health records often display lower overall healthcare utilization and expenditure. If an AI algorithm is trained to equate lower utilization with better underlying health (using cost as a proxy for disease severity), it actively penalizes vulnerable patients by under-predicting their health risks 57. In documented retrospective academic reviews, when developers replaced cost-based variables with direct health-needs variables, racial bias in the algorithmic outcomes decreased by an astonishing 84% 57. This indicates that the bias was highly correctable but had remained embedded within a deployed algorithm used on millions of patients for years because post-market surveillance had not specifically tested for it 57.
The current regulatory framework exhibits persistent vulnerabilities regarding bias prevention. In 2026, the FDA recommends - but does not strictly require - that manufacturers test AI medical devices for racial and ethnic bias prior to market authorization 57. A comprehensive scoping review of 692 FDA-approved AI medical devices published in npj Digital Medicine in 2024 revealed that only 3.6% of approvals reported the race or ethnicity of their validation cohorts 57. Addressing these deficiencies requires the mandatory implementation of adversarial debiasing processes during model training, the use of explainable AI architectures, and ongoing fairness audits as a strict prerequisite for clinical software deployment 56.
Clinical Implementation and Infrastructure Barriers
Despite extensive commercial progress in specific niches, multiple technical, infrastructural, and practical barriers prevent the ubiquitous, hospital-wide adoption of medical digital twins in 2026.
First, establishing and maintaining a true digital twin demands immense computational resources. Continuous, real-time data fusion using high-fidelity CFD simulations and large-scale multi-omics transformer networks requires advanced edge-computing infrastructure and dedicated cloud capabilities that far exceed the budgets, hardware, and technical expertise of many standard regional healthcare facilities 358.
Second, model generalization outside of controlled clinical environments remains highly challenging. Many digital twin systems are built upon strong theoretical assumptions and mathematical simplifications of human biology that may not hold true under extreme pathological stress or in patients with complex, interacting comorbidities 3. As noted in recent cardiovascular scoping reviews, while diagnostic accuracy is exceptionally high, evidence demonstrating that digital twin interventions lead to long-term downstream improvements in patient mortality outside of specific procedural trials remains limited 3. Furthermore, the "black-box" nature of advanced deep learning algorithms creates significant friction in clinical environments, where physicians ethically and legally require interpretable mechanistic reasoning before altering a standard treatment plan based on a machine's recommendation 1316.
Third, data interoperability and patient privacy severely restrict scalability. Integrating fragmented electronic health records, proprietary wearable telemetry, and highly sensitive decentralized genomic data into a single, cohesive predictive pipeline requires strict adherence to rigid data standards (such as ISO/IEEE 11073) and advanced cybersecurity protocols to prevent data breaches 224. The ethical tension regarding data ownership is profound. Moreover, the dual-use nature of digital twins - particularly in infectious disease scenarios within hospitals, where a single patient's digital twin must simultaneously model their individual risk while mapping contamination risks to the broader ward population - complicates existing legal and governance frameworks designed solely for single-patient privacy 25.
Conclusion
In 2026, medical digital twins have successfully transitioned from theoretical computational concepts to validated commercial tools that are actively altering the landscape of medical device engineering, cardiovascular diagnostics, and clinical trial execution. Companies such as HeartFlow, inHEART, Unlearn.AI, and Twin Health have definitively proven that computational simulation, when rigorously validated against engineering standards like ASME V&V 40, can provide clinically actionable insights. These platforms are reducing surgical procedure times, optimizing operational efficiency, lowering pharmaceutical costs, and fundamentally challenging the absolute necessity of extensive animal testing and massive placebo-controlled human trials.
However, the medical digital twin industry currently faces a critical inflection point. To move beyond specialized procedural applications and achieve broad clinical deployment across complex systemic diseases like oncology and neurodegeneration, the field must resolve the profound mathematical hurdles of multi-omics integration while simultaneously addressing the socioeconomic imperative of algorithmic fairness. Future trajectories point toward standardizing predictive transformer architectures to handle biological complexity and enforcing strict, post-market demographic validation to ensure health equity. If these technical interoperability and ethical governance frameworks are successfully aligned, digital twins stand to fundamentally transform medicine from a science of reactionary treatment into a discipline of precise, predictive, and personalized simulation.