What Chronic Stress Does to Your Body Month by Month
The long-term trajectory of chronic stress represents a profound, systemic biological remodeling of the human body. What begins as an adaptive, life-saving neuroendocrine reflex rapidly degrades into a pathological state of sustained allostatic overload when environmental pressures remain unrelenting. Under chronic psychological strain, the body shifts from acute sympathetico-adrenal arousal to a state of systemic dysregulation that fundamentally alters the hypothalamic-pituitary-adrenal (HPA) axis, suppresses adaptive immunity, induces systemic inflammation, dysregulates metabolic homeostasis, and triggers reversible structural atrophy in critical brain regions such as the hippocampus 121.
To comprehend this trajectory, one must recognize the vast biological difference between a single bad week and a grueling, three-month project. A single bad week - an acute stressor - triggers a transient surge of catecholamines and cortisol, accelerating the heart rate, sharpening cognitive focus, and temporarily boosting immune surveillance to handle immediate threats 22. Once the week concludes, the vagus nerve optimally engages the parasympathetic nervous system, effectively returning the body to baseline homeostasis 3. However, a grueling three-month project provides no such cessation. The body is deprived of the necessary biological signal to return to normal functioning 6. The resulting physiological debt transforms a psychological challenge into a verifiable, multisystem clinical syndrome 7.
The Science of Psychoneuroimmunology: The Mind-Body Axis
Recent advancements in psychoneuroimmunology (PNI) - the interdisciplinary field examining the bidirectional communication networks between the central nervous system, the endocrine system, and the immune system - have elucidated exactly how psychological strain translates into physical disease 189. PNI research from 2024 underscores that chronic stress alters integral biological pathways through complex top-down and bottom-up communication mechanisms 12.
When the brain perceives a persistent threat, it continually activates the sympathetic-adrenal-medullary (SAM) axis alongside the HPA axis 45. This chronic activation leads to the sustained release of glucocorticoids (primarily cortisol) and catecholamines. Over time, these hormones alter the composition of the gut microbiome, impeding the permeability of the blood-brain barrier and resulting in neuroinflammation 112. Consequently, individuals under chronic stress exhibit suppressed lymphocyte production, reduced efficacy of Natural Killer (NK) cells, and elevated levels of pro-inflammatory cytokines such as Interleukin-6 (IL-6) and C-reactive protein (CRP) 21314. This immune dysregulation increases susceptibility to autoimmune diseases, prolongs wound healing, and exacerbates psychiatric conditions, forming the basis of the "inflammatory hypothesis of depression" 26. The relationship is deeply bidirectional; systemic inflammation initiated by psychological stress can independently exacerbate neuronal damage, establishing a dangerous feedback loop 28.
FAQ: Month 1 vs. Month 6 - The Timeline of Systemic Breakdown
The transition from adaptive acute stress to maladaptive chronic stress is not instantaneous; rather, it follows a predictable, escalating timeline across human physiology. Physical symptoms of chronic stress operate on a specific delay trajectory. While cortisol spikes occur immediately at day zero of a stressful event, metabolic markers such as HbA1c elevate gradually over the first to second month. By the third and fourth months, structural changes such as telogen effluvium (hair shedding) actively manifest, and it is typically at the six-month mark and beyond that reductions in hippocampal volume become measurable on neuroimaging.
Early Chronic Stress: The First Month
During the first four weeks of sustained stress, the body attempts to maintain allostasis by operating at a heightened physiological baseline 16. The SAM and HPA axes remain in overdrive, resulting in disrupted sleep architecture, pervasive fatigue, and subjective feelings of being "wired but tired" 127. The gut-brain axis experiences significant turbulence during this initial phase. Heightened cortisol and adrenaline levels reduce gastrointestinal motility and alter mucosal barriers via the enteric nervous system, frequently manifesting as new-onset bloating, irritable bowel syndrome (IBS), or nausea 1218. Furthermore, metabolic shifts begin to occur rapidly. Cortisol functions to mobilize energy, increasing gluconeogenesis in the liver and promoting transient insulin resistance to keep glucose readily available in the bloodstream 1920.
The Tipping Point: Month 1 to Month 3
By the third month, the physiological debt of sustained arousal begins to manifest visibly. The most prominent physical marker during this period is telogen effluvium, a diffuse form of non-scarring hair loss 2122. When a severe stressor occurs, the body prioritizes vital organ function and diverts resources away from non-essential processes like hair growth. This neuroendocrine shock forces up to 70% of active hair follicles out of the anagen (growth) phase and into the telogen (resting) phase 2223. Because the telogen phase naturally lasts two to three months, the shedding does not become visible until month three, creating a delayed physical manifestation of the psychological burden 2324.
Concurrently, the metabolic strain becomes clinically measurable. Three months of stress-induced insulin resistance often results in elevated Hemoglobin A1c (HbA1c) levels 826. Because HbA1c reflects average blood glucose concentrations over a 90-to-120-day lifecycle of red blood cells, testing at the three-month mark accurately captures the metabolic toll of the stressor 269. Research demonstrates that sustained psychological stress independently predicts HbA1c elevation in both diabetic and healthy populations, regardless of dietary changes 198.
Late Chronic Stress: Month 6 and Beyond
At six months, the body enters a state of definitive allostatic overload, wherein the regulatory systems become exhausted and severe pathological consequences arise 16. Prolonged exposure to high levels of cortisol acts as a neurotoxin. The brain's memory center, the hippocampus, begins to undergo measurable physical changes. Sustained glucocorticoid elevations cause dendritic retraction - the shrinking of synaptic branches in hippocampal neurons - leading to volume reductions of approximately 3% to 14% 128. This structural shrinkage impairs memory consolidation, cognitive flexibility, and emotional regulation 2910. Systemically, chronic immune suppression leaves the individual highly vulnerable to recurrent infections, while sustained hypertension exponentially increases the risk of cerebrovascular diseases and metabolic syndrome 21132.
Trajectory of Stress: Acute vs. Chronic Responses
The physiological divergence between acute and chronic stress can be mapped across primary biological systems to illustrate the progressive nature of the condition.
| Biological System / Phase | Acute Stress (Hours to Days) | Early Chronic Stress (1 - 3 Months) | Late Chronic Stress (6+ Months) |
|---|---|---|---|
| Hormonal Response | Surge in adrenaline and cortisol; rapid return to baseline 511. | Sustained cortisol elevation; loss of diurnal cortisol curve 33. | Flattened or blunted cortisol curve; altered DHEA-S ratios 1235. |
| Immune Function | Temporary enhancement of innate immunity ("fight or flight" readiness) 2. | Initial suppression of lymphocytes; rising pro-inflammatory cytokines 214. | Chronic systemic inflammation (elevated IL-6, CRP); impaired NK cell efficacy 212. |
| Metabolic Function | Transient spikes in blood glucose via glycogenolysis 1920. | Sustained insulin resistance; early elevations in HbA1c 198. | High HbA1c; fat redistribution (visceral adiposity); metabolic syndrome 2632. |
| Neurological State | Heightened alertness; sharpened short-term memory 7. | Brain fog; poor concentration; disrupted sleep architecture 1236. | Hippocampal dendritic retraction; memory deficits; increased anxiety/depression risk 2829. |
| Physical Symptoms | Increased heart rate, sweating, tension headaches 7. | Digestive distress (IBS), jaw clenching (TMJ), new acne/eczema 1218. | Telogen effluvium (hair loss), chronic fatigue, severe cardiovascular strain 182122. |
FAQ: The Myth of Adrenal Fatigue and the Reality of Allostatic Load
In popular wellness discourse, the profound exhaustion experienced during late chronic stress is frequently misdiagnosed as "adrenal fatigue" - a concept suggesting that the adrenal glands simply tire out from overproduction and can no longer manufacture sufficient cortisol 33. The 2024 consensus within the endocrinology and medical communities firmly rejects this premise 537. The adrenal glands do not run out of hormones; rather, the exhaustion is a symptom of central nervous system downregulation, clinically referred to as HPA axis dysfunction and allostatic load 533.
Explaining Allostatic Load: The Car Engine Analogy
To accurately conceptualize allostatic load, medical researchers rely on the "getaway car" analogy.
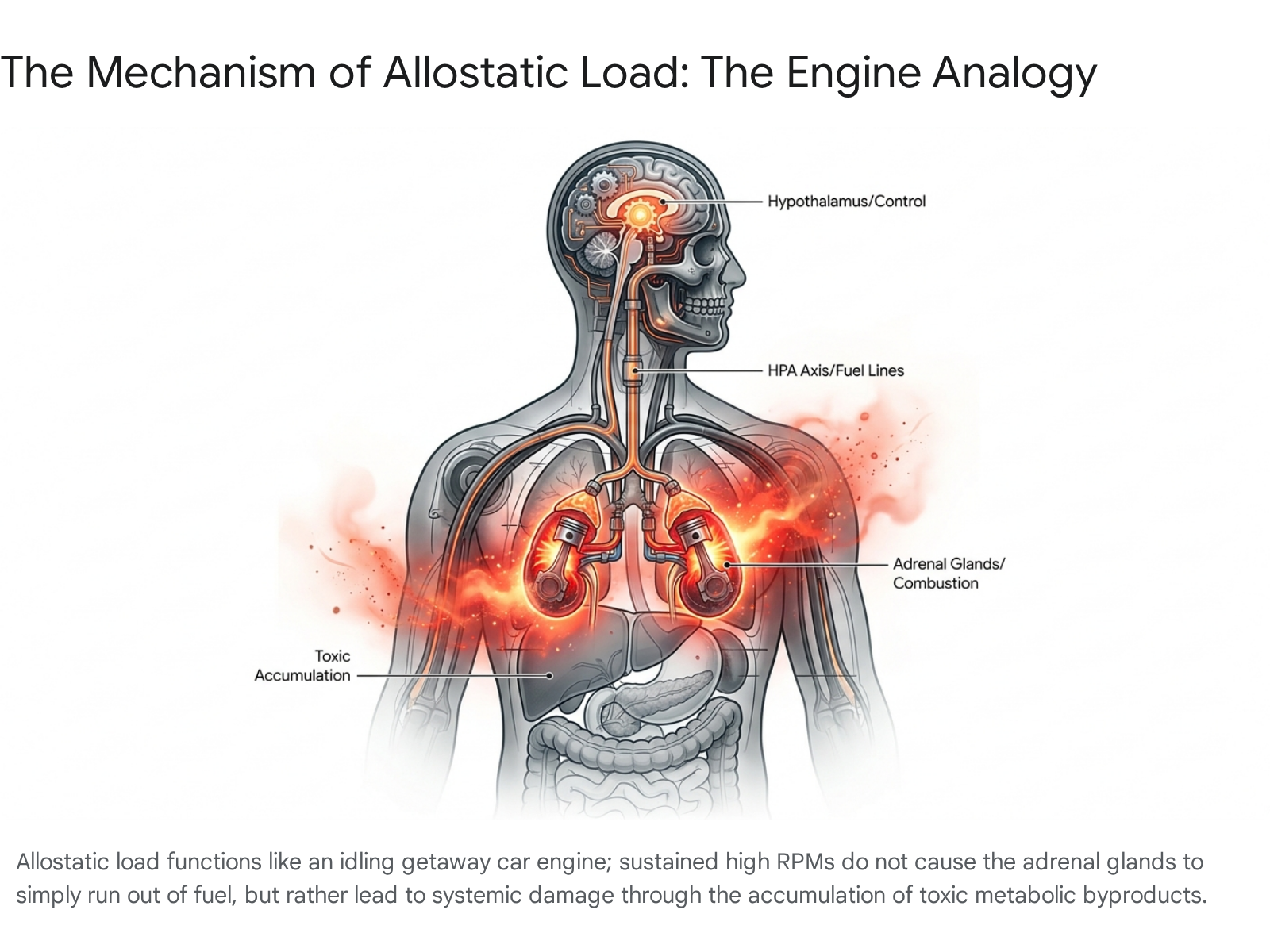
Allostasis is the body's active, adaptive process of maintaining stability through change, adjusting hormone levels and blood pressure dynamically to meet environmental demands 1613. If a getaway car is kept idling in anticipation of a high-speed chase, the revolutions per minute (RPM) of the engine can be maintained at intensely high levels. In the human body, this state of heightened readiness is allostasis 14.
However, running a car engine at high RPMs continuously comes with a severe structural cost. The engine does not stop working because it "runs out of gas" (the core flaw in the adrenal fatigue myth). Instead, the continuous combustion produces toxic byproducts and generates excessive heat. If the vehicle's catalytic converter or fuel recovery system is faulty, these byproducts build up and cause cumulative wear and tear on the engine block 1314. In the human body, this wear and tear is allostatic load 32. The physiological "toxic byproducts" are the persistent presence of cortisol and inflammatory cytokines circulating in the bloodstream, which damage the vascular endothelium, degrade hippocampal neurons, and induce systemic inflammation over time 213.
When the allostatic load exceeds a critical threshold, allostatic overload occurs 16. To protect the body from the autotoxic effects of perpetual cortisol exposure, the central nervous system (specifically the hippocampus and hypothalamus) actively downregulates its own receptors and decreases the release of the signaling hormones - such as corticotropin-releasing hormone (CRH) and adrenocorticotropic hormone (ACTH) - that command the adrenal glands to produce cortisol 533. This protective negative feedback loop results in a blunted or flattened diurnal cortisol curve, often with reversed rhythms where cortisol is inappropriately high at night, causing insomnia 35. The profound clinical exhaustion the individual feels is not because the adrenal glands are fatigued, but because the brain has deliberately suppressed the stress response to prevent further systemic biological damage 5.
Biomarkers of the Burden: Quantifying the Damage
Because chronic stress operates beneath the threshold of conscious awareness until physical symptoms become severe, researchers and clinicians rely on a diverse array of physiological biomarkers to quantify the allostatic load accurately 1340. Monitoring these markers provides a biological ledger of chronic stress over time.
While salivary and serum cortisol fluctuate wildly throughout the day, cortisol deposited in the hair shaft - known as Hair Cortisol Concentration (HCC) - provides a highly reliable, retrospective biological calendar of HPA axis activation 1412. Because hair grows at a predictable rate, sectional analysis of hair strands can map chronic stress experiences over several months, making it an invaluable diagnostic tool in psychoneuroimmunology 1312.
Furthermore, as previously noted, HbA1c serves as a critical metabolic biomarker for chronic stress. The persistent mobilization of glucose mediated by prolonged HPA axis activation fundamentally alters metabolic processing, establishing HbA1c not just as a marker of dietary habits, but as a direct proxy for chronic physiological distress 826. Beyond metabolic parameters, psychophysiological markers such as Brain-Derived Neurotrophic Factor (BDNF), Dehydroepiandrosterone sulfate (DHEA-S), and prolactin demonstrate significant relevance in reflecting multi-system dysregulation 13.
Immunological biomarkers are equally critical in mapping the trajectory. Plasma levels of IL-6, CRP, and Tumor Necrosis Factor-alpha (TNF-α) act as primary indicators of the systemic inflammation and immune dysregulation inherently linked to the chronic stress response 1315.
Calibrated Uncertainty: Genetic, Environmental, and Cross-Cultural Variations
While the overarching biological framework of the stress response is universal, it is vital to express calibrated uncertainty regarding the timeline and severity of physiological degradation. The psychoneuroimmunological response is heavily moderated by an individual's unique genetics, baseline neuroanatomy, environmental milieu, and cultural context.
Genetic and Anatomical Susceptibility
Baseline neuroanatomy dictates vulnerability. Longitudinal magnetic resonance imaging (MRI) studies using inbred C57 mice before and after chronic social defeat stress reveal that innate hippocampal volume prior to stress exposure predicts susceptibility. Individuals with naturally larger hippocampi exhibited greater resilience, whereas those with smaller baseline volumes were highly vulnerable to developing stress-induced psychopathologies 16. Furthermore, genetic polymorphisms interact intimately with perceived stress. Studies investigating late-life depression indicate that increases in perceived stress over time are associated with severe left hippocampal volume reduction strictly in individuals homozygous for the 5-HTTLPR L/L genotype, demonstrating that genetic architecture heavily moderates the neurodegenerative timeline of chronic stress 17.
Socioeconomic and Environmental Influences
Environmental and psychosocial factors act as potent catalysts for allostatic load. Objective markers of socioeconomic status (SES), such as income, certainly influence health outcomes, but recent research highlights the profound impact of Subjective Social Status (SSS). In a multi-site study utilizing the MacArthur Scale of Subjective Social Status, researchers found that lower perceived social rank independently predicted significantly higher allostatic load six months later, regardless of objective income or education levels 18. The psychological perception of lower status generates continuous psychosocial stress, accelerating wear-and-tear on multiple physiological systems 18.
The Cross-Cultural Context of Stress Manifestation
The manifestation and somatic expression of chronic stress are deeply influenced by cultural and occupational environments. In Japan, the phenomenon of karoshi (death from overwork) exemplifies the terminal endpoint of allostatic overload in a high-pressure occupational culture. Japanese health ministries define the primary risk factor for karoshi - which predominantly manifests as fatal cerebrovascular or cardiovascular events - as exceeding 80 hours of overtime per month 1920. Data compiled by Japan's Ministry of Health, Labor, and Welfare for fiscal year 2024 officially recognized a record 1,304 cases of overwork-related health disorders. Of these, 247 involved strokes or heart conditions, while an unprecedented 1,055 cases involved severe mental health disorders, largely driven by unrelenting psychological pressure, abuse of power, and insufficient recovery intervals 21. A 2024 white paper surveying the Japanese arts and entertainment sector highlighted that over 40% of technical staff worked 60 hours or more per week, while medical professionals similarly exhibited massive stress-related morbidity due to unsustainable workloads 22.
Furthermore, the expression of stress symptoms varies significantly across cultural divides. Studies comparing Chinese and United States populations reveal distinct, culturally bound patterns in symptom endorsement. Cultural norms dictate how distress is interpreted and communicated; research utilizing Hofstede's Uncertainty Avoidance Index (UAI) indicates that individuals in collectivistic cultures, such as China, often manifest and report stress through somatic (physical) symptoms - such as gastrointestinal distress, tension, or fatigue - more readily than psychological symptoms 492324. In contrast, populations in highly individualistic cultures like the United States more frequently report the emotional and psychological burdens of stress, such as depressed mood and anxiety 49. This cross-cultural variance highlights that while the biological mechanisms of HPA axis dysregulation are universal, the subjective experience, clinical presentation, and path to seeking help are heavily culturally bound 4952.
FAQ: Is Hippocampal Shrinkage Permanent? Reversing the Damage
A common and profound fear regarding late-stage chronic stress is that the neurological damage, particularly to memory centers, is permanent. Modern neuroscience firmly refutes this. The "shrinkage" of the hippocampus observed under chronic stress is largely driven by a process called dendritic retraction rather than the outright apoptosis (death) of neurons 28.
Neurobiologists liken this process to a tree dropping its leaves before a harsh winter frost to conserve energy. The neurons pull back their synaptic branches - particularly in the CA3 region and dentate gyrus of the hippocampus - to protect themselves from the neurotoxic overstimulation of prolonged circulating cortisol and glutamatergic activity 2825. Because the structural architecture merely goes dormant rather than dying, it is highly adaptable and reversible. Upon the cessation of chronic stress, robust neuroplasticity allows for the regrowth of these dendritic spines, eventually restoring hippocampal volume, improving memory consolidation, and normalizing cognitive function 282910. Early intervention, aerobic exercise, and effective stress reduction strategies have all shown measurable structural efficacy in reversing this stress-induced brain damage 2829.
Recognizing the Pivot and Interrupting the Cycle: Practical Takeaways
The biological trajectory of chronic stress is not an inevitable decline, but rather a sequence of measurable physiological shifts. The danger lies in missing the "pivot" - the critical inflection point where adaptive acute responses calcify into chronic allostatic load. By understanding the month-by-month trajectory, individuals and clinicians can recognize delayed somatic signals. When unexpected digestive issues arise in month one, or telogen effluvium manifests rapidly in month three, these must be interpreted not as isolated ailments, but as lagging indicators of systemic HPA axis overdrive 1221.
Interrupting this cycle requires aggressive prioritization of biological recovery and parasympathetic nervous system engagement.
Micro-Recovery in High-Pressure Environments
For individuals in demanding occupational roles, such as healthcare workers or C-suite executives, extended periods of rest are often structurally impossible. However, evidence-based "micro-recovery" provides substantial resilience. Micro-recovery involves brief, intentional periods of mental and physical reset interjected into demanding environments 3654. Research demonstrates that engaging in paced, slow diaphragmatic breathing (approximately 6 breaths per minute) for just 2 to 3 minutes optimizes the balance of carbon dioxide, stimulates the vagus nerve, and significantly increases Heart Rate Variability (HRV) 55. These micro-breaks - whether taking a mindful pause before charting a patient or stepping away for a brief visual reset - prevent the day-level accumulation of cortisol, effectively interrupting the progression from acute strain to chronic allostatic overload 5426. Elite performers utilize macro-recovery (protecting weekend white space) in tandem with daily micro-recovery to maintain cognitive output and prevent burnout 3657.
Novel Interventions: Vagus Nerve Stimulation
For severe clinical manifestations of chronic stress, recent 2024 literature highlights transcutaneous Vagus Nerve Stimulation (taVNS) as a revolutionary, non-invasive bioelectronic therapy. The vagus nerve acts as the information superhighway for the parasympathetic nervous system, putting the brakes on inflammation and stress 327. By delivering mild electrical pulses to the auricular branch of the vagus nerve via an ear-clip device, taVNS directly modulates the cholinergic anti-inflammatory pathway 2759.
Clinical trials demonstrate that taVNS significantly reduces pro-inflammatory cytokines, lowers sympathetic heart rate parameters, and shows profound efficacy in treating stress-induced depression, post-traumatic stress disorder (PTSD), and anxiety 2829. Double-blind randomized controlled trials indicate that varying the frequency of stimulation (e.g., 25 Hz vs 1 Hz) can produce dose-dependent reductions in neurological symptoms, offering a potent adjunctive treatment for populations resistant to traditional pharmacotherapy 5929.
Ultimately, the human body is remarkably resilient. By systematically lowering the metaphorical "RPMs" of the biological engine through intentional recovery and vagal modulation, systemic inflammation can be quelled, hormonal rhythms can be restored, and the structural integrity of the brain can be fully recovered 2814. Recognizing the pivot points of chronic stress enables the timely interruption of the cycle, preventing the devastating long-term consequences of allostatic overload.