Scientific Definition and Neurobiology of Occupational Burnout
The phenomenon of occupational burnout occupies a contested space at the intersection of organizational psychology, clinical neuroscience, and global labor economics. For decades, both corporate wellness initiatives and individual healthcare providers have approached burnout as a personal deficit - a failure of resilience, stress management, or work-life balance. However, a rigorous examination of the latest neuroimaging data, large-scale epidemiological studies, and psychiatric nosology reveals a fundamentally different reality.
Burnout is not a transient state of fatigue, nor is it synonymous with clinical depression, though the two conditions share overlapping symptomology. The current body of scientific evidence defines burnout as a context-specific, multidimensional syndrome driven by chronic, unmanaged environmental stress that induces measurable alterations in brain network architecture and endocrine function. Consequently, the prevailing treatment paradigm - which relies heavily on individual-level interventions such as mindfulness applications, resilience coaching, and relaxation classes - is structurally misaligned with the etiology of the condition. By treating the symptoms of the individual rather than the systemic demands of the workplace, the modern corporate wellness apparatus frequently fails to generate meaningful improvements in employee well-being.
Evolution of the Clinical Definition
To understand why treatments frequently fail to address the root causes of burnout, it is necessary to trace how the scientific community defines and measures the condition. The historical reduction of burnout to mere exhaustion has fundamentally compromised organizational interventions, stripping the syndrome of its critical interpersonal and evaluative dimensions.
Maslach Burnout Inventory and Diagnostic Nuance
The foundational scientific architecture for understanding burnout was established in the 1970s and operationalized in 1981 with the publication of the Maslach Burnout Inventory (MBI) 12. Developed by Christina Maslach and Susan E. Jackson, the MBI remains the primary instrument for assessing occupational burnout and positions the condition as a continuum rather than a binary diagnostic state 344. The instrument evaluates psychological depletion across three intersecting axes, utilizing a 22-item questionnaire graded on a seven-point frequency scale ranging from "never" to "every day" 1246.
A critical error in both academic research and corporate wellness deployment has been the simplification of burnout to emotional exhaustion alone. Focusing solely on exhaustion conflates burnout with generic chronic fatigue, ignoring the critical cognitive and relational deterioration - cynicism and reduced efficacy - that uniquely define the occupational syndrome 34. To address this oversimplification, psychometric research published in 2016 introduced distinct burnout profiles to capture the multidimensional nature of the condition 23.
| Burnout Profile | Emotional Exhaustion Score | Cynicism (Depersonalization) Score | Professional Efficacy Score | Clinical Implications |
|---|---|---|---|---|
| Burnout | High (Negative) | High (Negative) | Low (Negative) | Represents the complete manifestation of the syndrome, requiring comprehensive systemic intervention 23. |
| Overextended | High (Negative) | Baseline / Neutral | Baseline / Neutral | Indicates an unsustainable workload without the presence of relational detachment or feelings of inadequacy 23. |
| Ineffective | Baseline / Neutral | Baseline / Neutral | Low (Negative) | Suggests a crisis of competence, lack of resources, or misalignment of skills, independent of extreme fatigue 23. |
| Disengaged | Baseline / Neutral | High (Negative) | Baseline / Neutral | Points to a breach of the psychological contract or values conflict, resulting in emotional withdrawal 23. |
| Engaged | Low (Positive) | Low (Positive) | High (Positive) | The target state of organizational health, marked by high energy, involvement, and professional efficacy 23. |
While the MBI is considered the gold standard, it is not without academic criticism. Some researchers, such as Wilmar Schaufeli, have argued that the instrument was developed inductively via factor analysis of arbitrary items rather than being grounded in firm clinical observation 1. Furthermore, the lack of universally established clinical cut-off scores has historically complicated the diagnosis of dysfunctional burnout levels, leading to significant heterogeneity in epidemiological data 34.
International Classification of Diseases Framework
In 2019, the World Health Organization (WHO) formally updated the definition of burnout in the 11th Revision of the International Classification of Diseases (ICD-11) under the code QD85. The WHO's classification fundamentally shifts the burden of the syndrome from the individual to the environment 569.
The ICD-11 strictly classifies burnout as an occupational phenomenon rather than a medical or psychiatric condition. It is housed in the chapter detailing factors influencing health status or contact with health services, distinct from clinical mood disorders 78. The WHO definition aligns directly with the MBI trifecta, describing it as a syndrome conceptualized as resulting from chronic workplace stress that has not been successfully managed, characterized by feelings of energy depletion, increased mental distance or negativism related to one's job, and reduced professional efficacy 78.
This distinction carries profound clinical and organizational implications. First, it explicitly limits the application of the term to the occupational context, distinguishing it from broader life stress, parental burnout, or generalized anxiety 679. Second, by emphasizing that the stress has not been successfully managed, the definition implicitly indicts the organizational environment. As noted by occupational health experts, the failure to manage chronic stressors suggests that the conditions could be structurally improved; it removes the stigma of individual mental illness and directs intervention efforts toward systemic workplace reform 510.
Neurobiological and Physiological Signatures
While the WHO explicitly excludes burnout from primary psychiatric diagnoses, the physical toll of chronic occupational stress is highly measurable. Persistent clinical burnout induces profound, and sometimes reversible, changes in neuroanatomy, neurochemistry, and network connectivity, invalidating the premise that burnout is merely a psychological attitude.
Endocrine Dysfunction and the Hypothalamic-Pituitary-Adrenal Axis
At the core of the biological burnout response is the dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, the central neuroendocrine network responsible for the body's stress response 111213. Under normal conditions, acute stress triggers the release of cortisol, which marshals physical and mental energy. However, chronic, unresolvable psychosocial stress fundamentally alters this system.
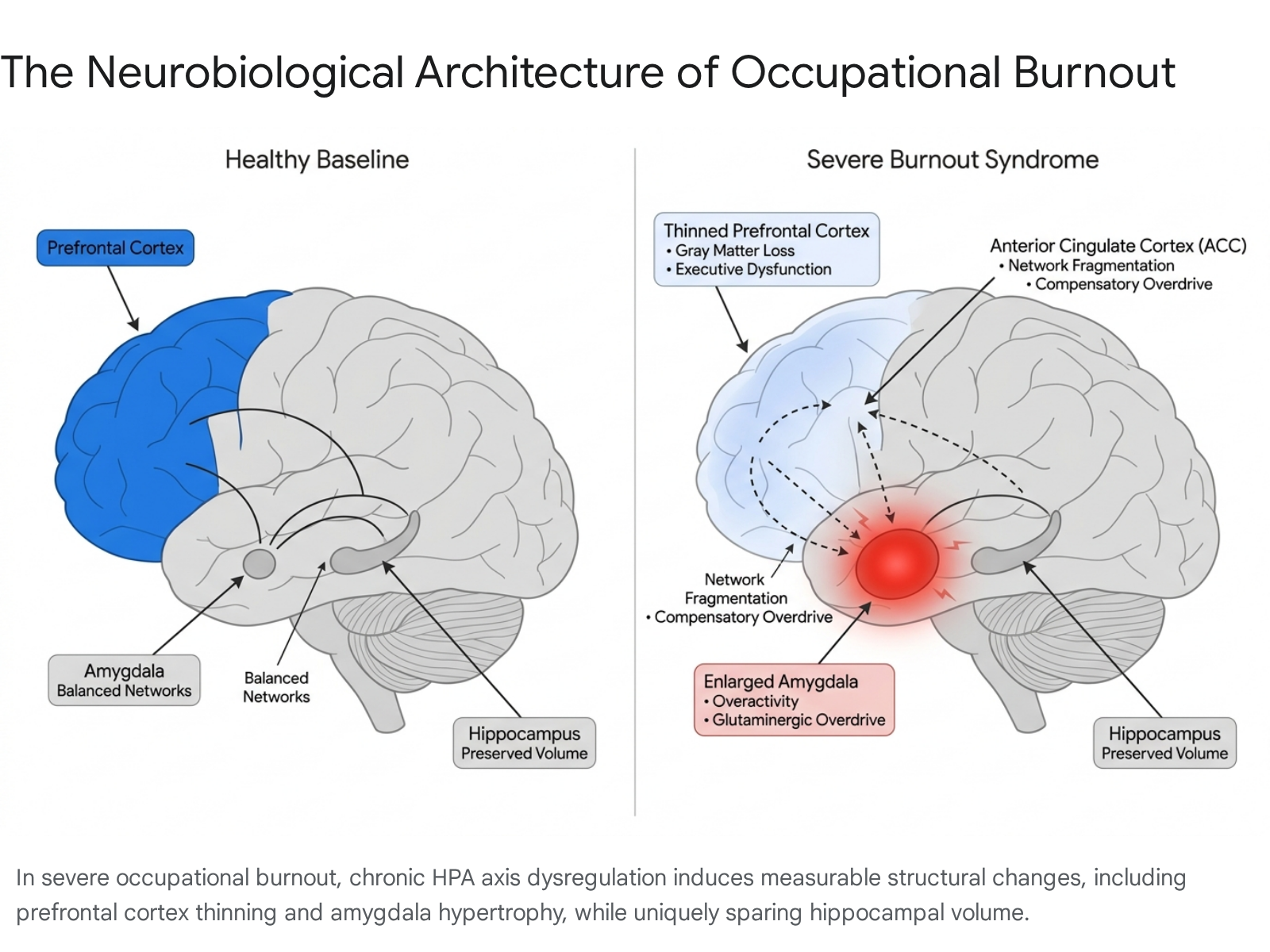
In severe burnout, persistent exposure to stress hormones triggers maladaptive neurochemical feedback loops. Glucocorticoid receptors, which are highly concentrated in the prefrontal cortex and limbic system, become overwhelmed 11. The amygdala experiences an increase in glutaminergic signaling, which upregulates its functional activity and stimulates corticotropin-releasing factor. This disrupts GABA signaling, establishing an excitatory feed-forward loop between the amygdala and the HPA axis 1114.
The clinical literature shows conflicting patterns regarding precise cortisol levels in burned-out individuals, largely depending on the severity and duration of the syndrome. While some studies observe elevated morning salivary cortisol and a hyperactive HPA axis - particularly among women or those in moderate stages of burnout - end-stage exhaustion syndrome is frequently characterized by a blunted HPA axis response. This includes a flattened diurnal cortisol curve, a blunted early-morning drop, and a reduced adrenocorticotropic hormone (ACTH) surge, resulting in a state of profound physiological under-arousal that mimics chronic fatigue 121516.
Research regarding a definitive physiological biosignature for burnout remains ongoing. Systematic reviews evaluating allostatic load biomarkers - such as heart rate variability (HRV), dehydroepiandrosterone sulfate (DHEA-S), and inflammatory cytokines - indicate that while some parameters like HbA1c and resting heart rate show correlations with burnout, current biological evidence is insufficiently uniform to establish a routine clinical diagnostic blood test 1718.
Structural Brain Alterations
Prolonged exposure to the biochemical cascades of the HPA axis eventually results in gross morphological changes to the brain. Recent systematic reviews of magnetic resonance imaging (MRI) and functional MRI (fMRI) studies involving thousands of participants have identified a reproducible neuroimaging signature for severe occupational burnout 1415.
Structural morphometry consistently reveals hypertrophy, or enlargement, of the amygdala, a finding that is predominantly observed in women and correlates with perceived stress levels 1415. Conversely, the neurotoxic effects of prolonged cortisol exposure lead to gray-matter volume loss and cortical thinning in the dorsolateral and ventromedial prefrontal cortex (PFC), as well as the striatal caudate-putamen 1415. Because the PFC governs executive control, decision-making, and emotional regulation, its atrophy perfectly mirrors the MBI dimension of reduced professional efficacy. Burned-out individuals exhibit impaired concentration and working memory, requiring substantially more mental energy to execute standard cognitive tasks 1113.
Furthermore, fMRI reveals a state of compensatory executive overdrive. The brain's rich-club networks progressively fragment, and coupling between the amygdala and the anterior cingulate cortex (ACC) weakens. The brain must hyper-activate fronto-cortical areas to maintain baseline performance, leading to rapid cognitive fatigue 1415. Empathy-related brain activity in the anterior insula (AI) and temporoparietal junction (TPJ) shows a significant negative correlation with burnout severity, providing a direct biological substrate for depersonalization and cynicism 1415.
Diagnostic Distinction from Major Depressive Disorder
A prominent debate in psychiatric literature is whether burnout is simply a context-specific manifestation of Major Depressive Disorder (MDD). The two conditions share striking phenotypic similarities, including profound fatigue, anhedonia, sleep disturbances, and impaired concentration 91920. Some large-scale meta-analyses demonstrate a remarkably high disattenuated correlation (r = 0.80) between emotional exhaustion and depressive symptoms, suggesting a shared underlying factor of general psychological distress 19.
However, bifactor modeling, specific etiology, and neuroimaging firmly establish them as related but distinct conditions. The most definitive differentiator lies in the neuroanatomy of the hippocampus.
| Clinical Feature | Occupational Burnout (ICD-11: QD85) | Major Depressive Disorder (MDD) |
|---|---|---|
| Primary Etiology | Chronic, unresolvable occupational stress and systemic workplace imbalances 92021. | Multifactorial (genetic, biochemical, psychological) with or without external stress triggers 212223. |
| Scope of Impairment | Context-specific. Symptoms frequently improve when the individual is removed from the stressful work environment 202122. | Pervasive. Affects all domains of life, including personal agency, social functioning, and baseline mood, regardless of setting 920. |
| Dominant Emotional Profile | Characterized by frustration, cynicism, emotional numbness, and reactive irritability toward tasks or colleagues 2022. | Characterized by persistent sadness, deep hopelessness, pervasive emptiness, and feelings of worthlessness 2022. |
| Response to Rest | Often improves significantly with extended time off, reduced workload, or a change in environment 202122. | Persistent fatigue and anhedonia remain despite rest, vacations, or the complete removal of external stressors 2022. |
| Neurobiological Signature | Prefrontal cortex thinning, amygdala enlargement, and notably intact hippocampal volume 1415. | Prefrontal cortex alterations, amygdala changes, and hallmark hippocampal atrophy 141516. |
Clinical literature increasingly views the relationship temporally. Chronic work stress induces burnout, which, if left entirely unaddressed, serves as a potent gateway risk factor for the development of clinical depression 192124.
Theoretical Frameworks of Occupational Stress
To understand how burnout develops and how it can be mitigated, occupational health psychology relies on validated theoretical models. The most robust and widely applied of these is the Job Demands-Resources (JD-R) model.
Job Demands-Resources Model
Introduced by Demerouti and Bakker in 2001, the JD-R model operates on a dual-pathway premise, categorizing all working conditions into two broad sets: demands and resources 25.
The health impairment pathway focuses on job demands. These are physical, psychological, social, or organizational aspects of a job that require sustained cognitive or emotional effort. Examples include heavy workloads, extreme time pressure, emotional labor, and role ambiguity. High job demands drain mental energy, leading directly to the emotional exhaustion dimension of burnout and subsequent health complaints 2627.
Conversely, the motivational pathway focuses on job resources. These are factors that help achieve work goals, reduce job demands, or stimulate personal growth and learning. Examples include autonomy, performance feedback, strong managerial support, role clarity, and psychological safety. High job resources act as a buffer against stress and drive work engagement 2627. This is heavily supported by Conservation of Resources (COR) theory, which posits that individuals strive to obtain and protect resources; when resources are depleted without replenishment, burnout ensues 27.
Burnout occurs precisely at the intersection of high job demands and low job resources. When an employee faces crushing workloads but lacks the autonomy to control their schedule or the support of management to prioritize tasks, the health impairment process accelerates 272829. When organizations increase key resources - such as granting scheduling flexibility or clarifying performance expectations - employees exhibit resilience, mitigating the toxic effects of the demands 2528.
Systemic Limitations and Contextual Variables
Recent problematization reviews of the JD-R model note that it cannot be treated as a static equation. The effectiveness of a resource is highly contextual. Furthermore, modern iterations of the theory distinguish between challenge demands and hindrance demands. Challenge demands, such as complex projects that allow for skill utilization, can actually foster engagement if matched with adequate resources. Hindrance demands, such as red tape, bureaucratic politics, or malfunctioning equipment, directly inhibit personal growth and reliably trigger burnout regardless of available resources 2729.
Despite these nuances, the JD-R model makes one empirical fact undeniably clear: mitigating burnout requires structural adjustments to the demands and resources of the job itself. It cannot be resolved solely by altering the mindset of the employee.
Corporate Wellness and Intervention Efficacy
The corporate wellness industry is projected to grow from roughly $59.6 billion in 2024 to over $108 billion by 2033, driven heavily by an increased emphasis on mental health interventions following the global pandemic 343036. Organizations invest heavily in these programs, driven by estimates that effective wellness initiatives can yield positive returns on investment (ROI). Historical claims suggest medical costs fall by $3.27 and absenteeism costs drop by $2.73 for every dollar invested in wellness programs 313239.
However, modern occupational health research highlights a profound tension. While the financial metrics of healthcare cost-containment may show improvement, the actual psychological burnout of the employees often remains entirely unchanged. This failure occurs because the vast majority of wellness programs target the individual worker while ignoring the systemic JD-R environment.
Efficacy of Individual-Level Interventions
The starkest evidence of this misalignment comes from a landmark 2024 study conducted by Dr. William Fleming at the University of Oxford's Wellbeing Research Centre. Published in the Industrial Relations Journal, the study analyzed survey data from 46,336 workers across 233 organizations in the United Kingdom, drawn from the 2017 and 2018 waves of Britain's Healthiest Workplace survey 403334.
The research evaluated the efficacy of 90 different well-being programs, grouped into broad individual-level mental health interventions. These included mindfulness classes, resilience and stress management training, relaxation sessions, sleep apps, workload management training, and online coaching 333435. The methodology rigorously compared participants against non-participants within the same organizations to control for systemic variables.
Across multiple subjective well-being indicators, employees who participated in these individual-level interventions were no better off than those who did not 4034. Furthermore, resilience and stress management programs occasionally demonstrated a small negative impact on well-being. This counterintuitive finding is attributed to selection bias: employees with lower baseline mental health actively sought out the programs but received no tangible relief from their underlying occupational stressors 3435.
The study identified only one intervention with a measurable positive effect: volunteering programs, which likely foster community and purpose outside of core work tasks 3335. Dr. Fleming interpreted these results strictly through the JD-R model, concluding that individual wellness programs fail to undo the damage of a stressful work environment because they do not provide appropriate resources in response to job demands. They frame wellness as an additive behavior - something the employee must do on top of their existing job demands - rather than reducing the demands themselves 4036.
Superiority of Organization-Directed Redesign
When leaders deploy a meditation application to an employee working excessive hours with no role clarity, they are intervening at the wrong layer of the system. Research on psychosocial working conditions consistently proves that downstream wellness perks cannot out-compete upstream stressors 2536.
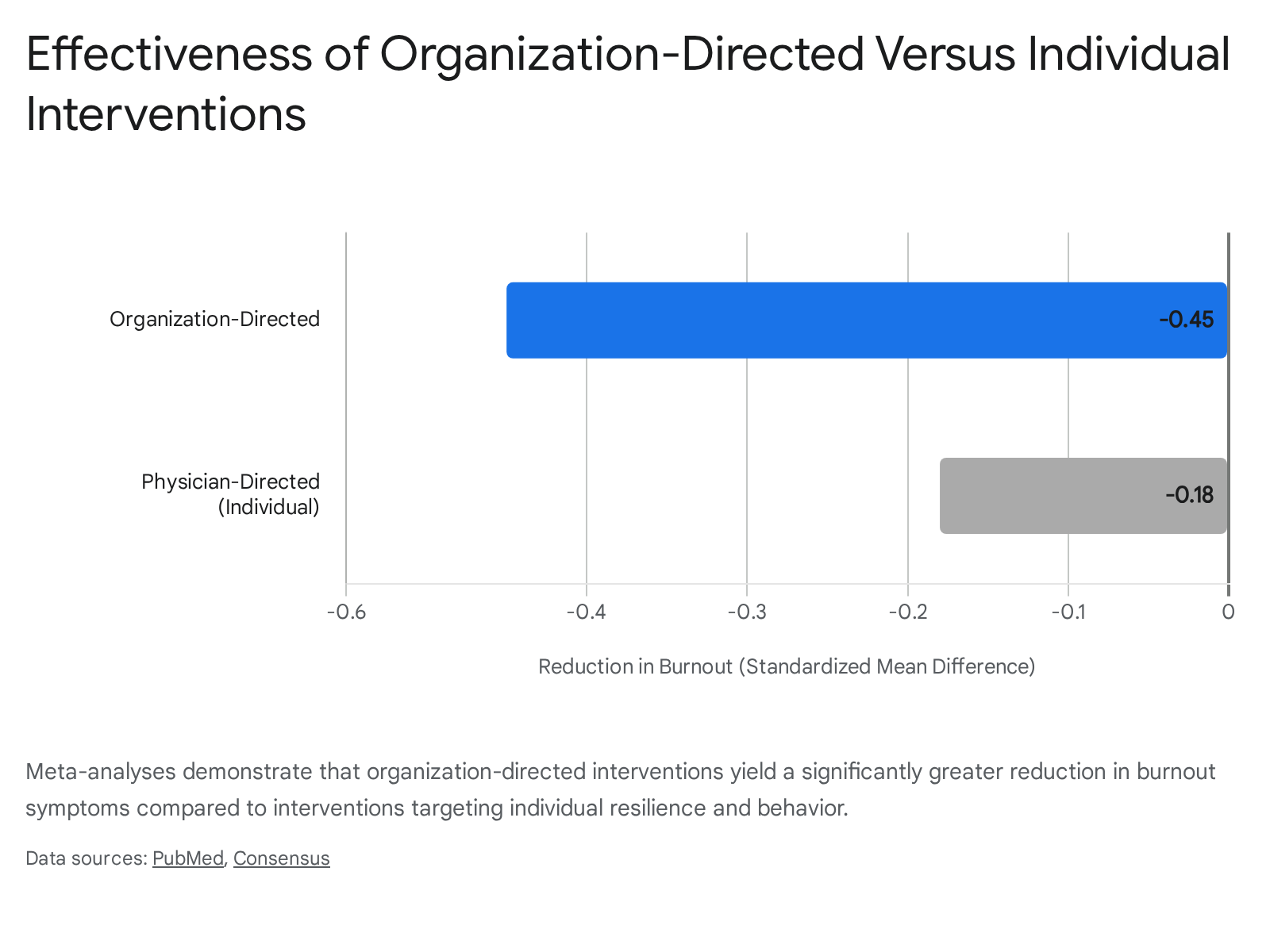
Meta-analyses confirm that organization-level interventions are more effective at combating burnout than individual-level tactics. A comprehensive analysis of interventions targeting healthcare workers found that organization-directed initiatives - such as improving practice efficiency, altering work schedules, increasing physician autonomy, and restructuring performance reviews - resulted in a moderate reduction in burnout 37.
| Intervention Target | Intervention Mechanisms | Effect Size (SMD) on Burnout Reduction |
|---|---|---|
| Organization-Directed | Workflow optimization, increased autonomy, leadership restructuring, reduction of administrative burden 37. | Moderate reduction (SMD ≈ -0.45). Notably improves emotional exhaustion and depersonalization 37. |
| Individual-Directed | Mindfulness training, resilience coaching, stress management education, digital wellness applications 37. | Small reduction (SMD ≈ -0.18). Effects are often transient and fail to address systemic stressors 37. |
It must be noted with calibrated uncertainty that not all meta-analyses yield overwhelmingly positive results for organizational change. Specific systematic reviews focusing exclusively on medical residents highlight that while individual coaching showed a small statistically significant reduction in emotional exhaustion (Cohen's d = -0.25), broad organizational interventions often showed non-significant pooled effects. This is largely attributed to data inconsistency, high risk of bias, and the extreme rigidity of the medical hierarchy, which makes genuine structural redesign difficult to achieve during a residency program 383940. However, across the broader corporate landscape, meaningful and sustainable reductions in emotional exhaustion necessitate structural redesigns of the work itself 344142.
Cross-Cultural Labor Economics and Severe Outcomes
When organizational demands are culturally entrenched and labor protections are weak, burnout progresses past psychological distress and biological atrophy into fatal consequences. The global labor market provides stark examples of how macro-level work structures dictate the severity of the burnout epidemic.
East Asian Manifestations of Extreme Overwork
In Japan, the phenomenon of karoshi - translated literally as "death from overwork" - was recognized as a sociomedical term in the 1970s. It refers to sudden fatalities or severe disabilities resulting from cardiovascular attacks, such as strokes or myocardial infarctions, explicitly aggravated by extreme workloads and chronic stress 434445. Official reports from the International Labour Organization detail cases of employees working upwards of 110 hours of overtime per month prior to fatal cardiovascular events 44. A parallel crisis exists in karojisatsu, or suicide driven by overwork, routine bullying, and impossible corporate goals 4445. Japan's 2018 Workstyle Reform Act attempted to outlaw working more than 45 hours of overtime in a single month, but systemic pressures often force employees to hide true working hours 45.
Similar phenomena have emerged across the region. In South Korea, the term gwarosa mirrors karoshi. A 2025 National Data Agency report indicated that 32.2% of South Korean youth experienced severe burnout within the past year, driven predominantly by career anxiety and work overload 46. This persists despite recent legal attempts to enforce a 52-hour workweek cap, which tech companies routinely circumvent by arguing that global competition demands extreme output 55.
In China, the technology sector has been dominated by the "996" work culture - working from 9 a.m. to 9 p.m., six days a week, totaling 72 hours 4748. While originally championed by tech executives as necessary for innovation and economic dominance, the 996 schedule has recently faced massive public backlash. The human cost is severe; a McKinsey Health Institute study found that burnout syndrome among Asian employees exceeds the global norm, approaching nearly one-third of the workforce, heavily driven by toxic workplace behavior and inescapable overwork 4858.
Western Labor Protections and At-Will Vulnerabilities
In Western economies, the manifestation of burnout is heavily mediated by employment law and the structural availability of job resources.
| Labor Market | Structural Vulnerabilities and Protective Regulations | Impact on Burnout Risk Factors |
|---|---|---|
| United States | Operates on "at-will" employment, allowing termination for non-discriminatory reasons without notice. Lacks federal mandates for paid annual vacation or parental leave 596049. | Generates high job insecurity and limits recovery periods. Contributes to the workplace ranking as the fifth leading cause of death in America due to stress-related illness 434962. |
| European Union | Enforces robust protections. Dismissals require formal processes. Laws mandate maximum working hours (e.g., 35-hour weeks in France) and minimum daily rest periods (11 consecutive hours) 4962. | Structurally mitigates job demands by enforcing rest. Lowers the risk of extreme physiological outcomes like karoshi, though psychosocial burnout still occurs 6049. |
| Germany | Features powerful Works Councils that give employees direct consultation rights over working times, redundancies, and corporate policies 604950. | Embeds "job resources" directly into the organizational framework, providing employees with autonomy and a voice to buffer against excessive demands 50. |
While European workers are certainly not immune to occupational stress, the statutory limits on extreme job demands structurally prevent the hyper-escalation seen in environments lacking such protections. In the United States, the systemic lack of guaranteed resources amplifies the health impairment pathway, making structural burnout prevention highly dependent on the goodwill of individual corporate leadership rather than mandated baselines 434950.
Synthesis and Systemic Implications
The scientific consensus on burnout is clear, multidimensional, and rigorously validated. It is an occupational phenomenon characterized by emotional exhaustion, depersonalization, and reduced professional efficacy 7. Biologically, it is a physical syndrome driven by unresolvable HPA axis dysregulation that alters the structural and functional connectivity of the brain. The resulting amygdala hypertrophy and prefrontal cortex thinning - paired with an intact hippocampus - biologically distinguish severe occupational burnout from major depressive disorder 1415.
Despite this clarity, the predominant corporate approach to mitigating burnout remains fundamentally flawed. By relying on individual-level wellness interventions like mindfulness applications and resilience training, organizations attempt to treat systemic environmental failures as personal psychological deficits. As the Oxford study and subsequent meta-analyses definitively show, these downstream interventions cannot undo the physiological and psychological damage of an upstream toxic work environment 4037.
True mitigation of burnout requires adherence to the Job Demands-Resources model. Leadership must actively reduce chronic job demands - such as excessive workloads, long hours, and toxic behavior - while structurally enhancing job resources like autonomy, role clarity, and management support 252736. Until organizations align their interventions with the scientific reality of the syndrome - treating the structural mechanics of the workplace rather than isolating the worker - burnout will remain a pervasive, escalating crisis across the global economy.