Understanding and Explaining High-Functioning Depression
Clinical Classification and Diagnostic Criteria
The term "high-functioning depression" has increasingly permeated clinical commentary, occupational health discussions, and popular psychology to describe individuals who experience persistent depressive symptoms while maintaining outward social, academic, and occupational success 12. Despite its widespread usage, which accelerated notably around 2016, high-functioning depression is not recognized as a formal diagnostic category in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) or the World Health Organization's International Classification of Diseases (ICD-11) 12342.
Instead, the phenomenon described by this term most accurately aligns with the clinical diagnosis of Persistent Depressive Disorder (PDD), a classification that consolidated the previously distinct diagnoses of chronic major depressive disorder and dysthymic disorder 3467341011.
Persistent Depressive Disorder
According to the DSM-5-TR, a formal diagnosis of PDD requires the presence of a depressed mood for most of the day, for more days than not, spanning a minimum duration of two years in adults or one year in children and adolescents 3423101112. During this extended timeframe, the individual must exhibit at least two of the following six diagnostic symptoms: 1. Poor appetite or overeating 2. Insomnia or hypersomnia 3. Low energy or fatigue 4. Low self-esteem 5. Poor concentration or difficulty making decisions 6. Feelings of hopelessness 3634101112.
To satisfy the criteria for PDD, the patient cannot experience a symptom-free interval lasting longer than two consecutive months during the established diagnostic period 61011. Furthermore, the presentation must not be attributable to the physiological effects of a substance, medication, or another underlying medical condition, and there must be no history of manic or hypomanic episodes 3410.
Unlike Major Depressive Disorder (MDD), which is characterized by acute, highly debilitating episodic crashes that often severely impair an individual's ability to perform Instrumental Activities of Daily Living (ADLs), PDD functions as a chronic, continuous emotional baseline 267131415. Because acute functional impairment is not strictly mandated across every symptom domain concurrently, many individuals with PDD successfully mask their condition by continuing to execute their professional and familial responsibilities mechanically 126.
Comorbidity and Subthreshold Presentations
The diagnostic boundaries between depressive disorders are highly fluid. Epidemiological data suggests that approximately 75% of individuals diagnosed with PDD eventually experience worsening symptoms that culminate in a major depressive episode 74. When MDD and PDD co-occur, the clinical presentation is referred to as "double depression" 274. In these cases, once the acute major depressive episode resolves, the individual typically returns to their chronic PDD baseline rather than achieving full remission, resulting in cumulatively higher levels of hopelessness and dissatisfaction than either disorder produces in isolation 7.
In addition to DSM-5-TR frameworks, international health organizations provide specific guidance for depressive presentations that fail to meet the full symptom count or duration requirements for formal MDD or PDD diagnoses. The National Institute for Health and Care Excellence (NICE) guidelines classify such presentations as "subthreshold depressive symptoms" or "mild depression" 1656. NICE guidelines emphasize that symptom severity is a composite of symptom intensity, duration, and the resulting impact on personal functioning 6. For individuals exhibiting persistent subthreshold symptoms, clinicians are advised to pursue active monitoring, recommend structured physical activity or sleep hygiene programs, and consider early-stage psychotherapeutic interventions 165.
| Diagnostic Feature | Major Depressive Disorder (MDD) | Persistent Depressive Disorder (PDD) / "High-Functioning" | Subthreshold Depressive Symptoms |
|---|---|---|---|
| Duration Requirement | At least 2 weeks per episode 613141519 | At least 2 years (1 year for pediatric populations) 3263 | Variable; often evaluated if persisting after initial active monitoring 165 |
| Symptom Threshold | Minimum of 5 symptoms, including depressed mood or anhedonia 61315 | Depressed mood plus a minimum of 2 additional symptoms 36312 | Fewer than 5 symptoms, failing to meet full MDD or PDD criteria 125 |
| Course and Pattern | Episodic; distinct onset, peaks, and periods of remission 26714 | Chronic, continuous baseline; smoldering presentation 267 | Fluctuating or persistent low-level mood without severe escalation 125 |
| Functional Impairment | Severe, often visibly debilitating; interrupts daily activities 613141519 | Hidden or moderate; mechanical performance of duties maintained 1326 | Mild to minimal external impairment; persistent internal distress 12165 |
| Primary Symptom Emphasis | Neurovegetative symptoms (acute anhedonia, severe psychomotor changes) 6 | Cognitive and emotional symptoms (low self-esteem, chronic apathy, pessimism) 46 | Varies; often mood dysregulation or mild somatic complaints 567 |
Pathophysiology and Biomarkers
The biological underpinnings of chronic depressive states provide critical insight into the physiological reality of conditions perceived outwardly as mere emotional fluctuations. Research into the pathophysiology of depression has identified robust alterations in several biological markers that correlate with disease presence and severity 8.
Enhanced systemic inflammation is a hallmark of depressive disorders, reflected by increased serum concentrations of inflammatory markers such as C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and the soluble interleukin-2 receptor 8. This pro-inflammatory state frequently manifests in "sickness behavior," a biological mechanism characterized by anhedonia, fatigue, anorexia, and social withdrawal - all core symptoms of clinical depression 8. Furthermore, neurotrophic factors are heavily implicated; individuals with depression consistently demonstrate a significant decrease in brain-derived neurotrophic factor (BDNF) alongside increases in fibroblast growth factor-2 and insulin-like growth factor-1 8.
Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis, indicated by elevated or chronically disrupted cortisol rhythms, is another primary biological signature 89. Oxidative and nitrosative stress pathways are also elevated, with lipid peroxidation markers serving as characteristic indicators of depressive pathology 8.
Motivational Dysfunction and Decision-Making
A central feature of high-functioning depression is the immense discrepancy between an individual's external output and their internal energy reserves. Computational psychiatry research investigating effort-based decision-making sheds light on the cognitive mechanisms underlying this specific motivational dysfunction 2310.
In experimental paradigms such as the Apple Gathering Task - where participants must decide whether to exert physical grip force to obtain varying levels of reward - individuals with depression demonstrate distinct computational mechanisms driving their decisions 23. Model-agnostic analyses indicate that depressed individuals are fundamentally less willing to exert effort 2310. However, computational analysis reveals that this is primarily driven by a lower "effort acceptance bias" rather than an altered sensitivity to the reward itself 23. Consequently, the internal calculation of required cognitive and physical effort is skewed; routine daily tasks are perceived as exacting a much higher metabolic and psychological cost 2310.
For the high-functioning individual, continually overriding this depleted motivational baseline to meet external expectations requires severe psychological friction. This continuous overriding exacerbates long-term fatigue, rendering the sustained performance of occupational and social duties physically and neurologically exhausting, despite the lack of visible impairment 1223.
The Paradox of Preserved Functionality and Masking
High-functioning depression exposes a significant limitation in traditional psychiatric frameworks that equate mental health strictly with observable functionality 1. Individuals experiencing this condition often embody behavioral traits that modern society explicitly rewards and incentivizes: intense ambition, high resilience, self-control, and perfectionism 124. This outward compliance and objective success create a profound diagnostic blind spot. Because the individual successfully meets deadlines, maintains personal hygiene, and fulfills caregiving obligations, lay observers, employers, and even primary care providers frequently fail to recognize the underlying psychopathology 2426.
The characterization of an individual as "functioning" privileges external appearance over internal suffering 26. Patients in this category frequently report a pervasive sense of emptiness, chronic apathy, and a mechanical participation in their own lives 4614. They experience anhedonia not as an inability to execute tasks, but as a total inability to derive joy or satisfaction from their completion; achievements are met with emotional numbness rather than pride 46. This paradox places high-achieving professionals, academics, and caregivers at a distinct disadvantage. Their outward success is often weaponized against their internal reality, leading to a dangerous delay in clinical diagnosis and intervention 1226.
Emotional Labor and Expressive Suppression
Maintaining a composed, productive exterior while enduring chronic depressive symptoms demands significant, continuous cognitive effort. This process is closely aligned with the psychological concept of "emotional labor," which involves the active management of emotional expression to conform with occupational, social, or familial display rules 11121314.
Within the emotional labor framework, individuals primarily utilize two regulatory strategies: "surface acting" and "deep acting." Surface acting corresponds directly with the emotion regulation strategy of "expressive suppression," defined as the conscious effort to conceal outward behavioral expressions of emotion to minimize negative social reactions and maintain a facade of normalcy 111415. Conversely, deep acting aligns with "cognitive reappraisal," a generally more adaptive strategy involving modifying one's internal feelings to match the required outward expression 11.
Empirical research consistently links the habitual use of expressive suppression and surface acting with detrimental psychological and physiological outcomes 9111416311718. The act of suppressing emotion leaves the subjective experience of the negative emotion entirely intact while simultaneously diminishing the capacity to experience positive emotions, thereby increasing feelings of inauthenticity and social isolation 14.
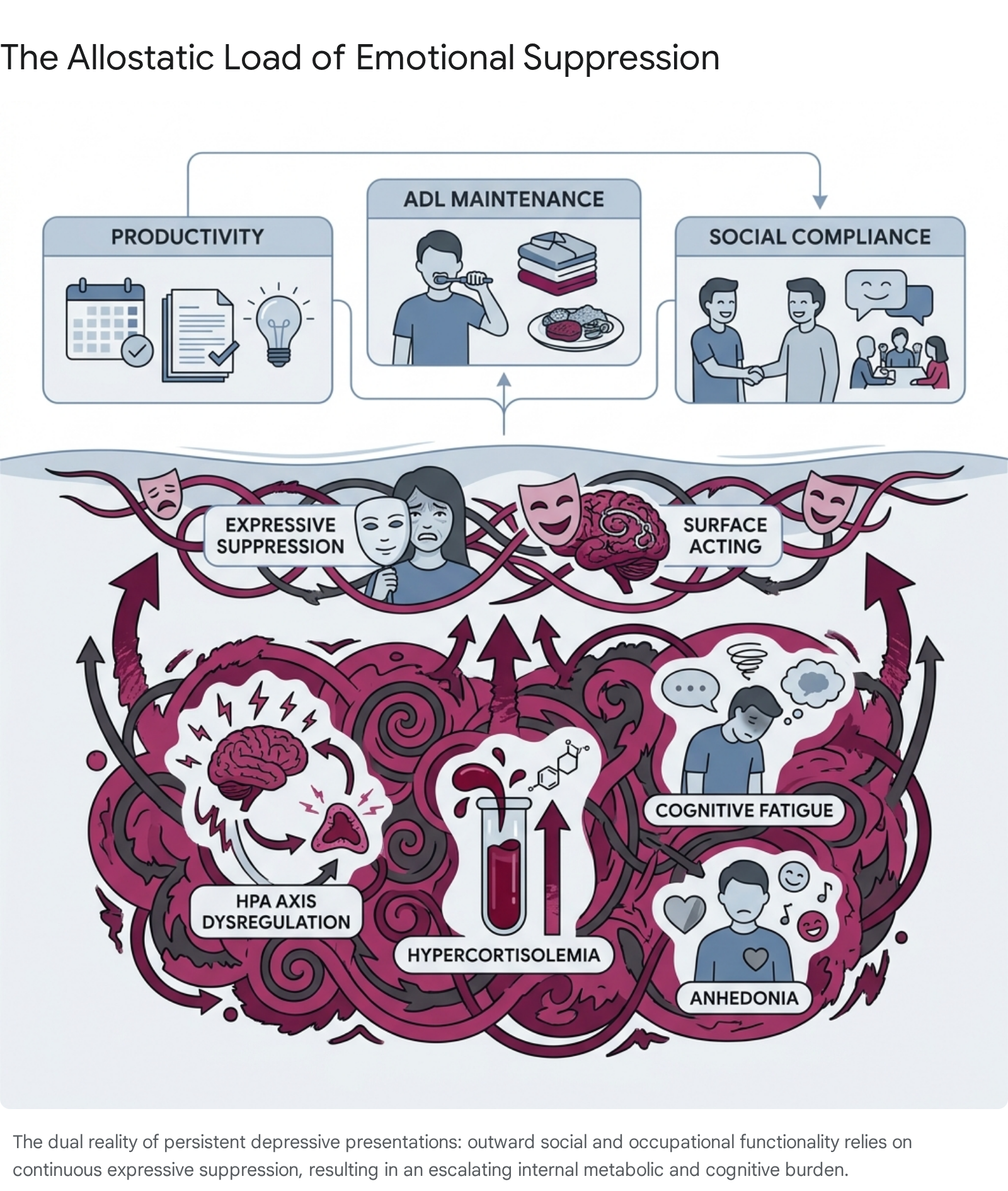
The physiological toll of this continuous expressive suppression is profound. Suppression operates as a chronic stressor that amplifies stress-induced physiological arousal 9161819. Meta-analyses of experimental and correlational data reveal that individuals who habitually mask their depression exhibit heightened sympathetic nervous system activation during acute stressors, even when outward behavioral expressions are successfully minimized 1819. Over the life course, structural equation models indicate that habitual suppression significantly predicts flatter diurnal cortisol slopes - indicating severe HPA axis dysregulation - and elevated inflammatory burdens, independent of standard health behaviors 9. This continuous requirement to exert executive control over emotional reality depletes prefrontal brain activation, manifesting as severe cognitive fatigue and diminished self-control capacity 18.
Somatization and Clinical Misattribution
Because the psychological and emotional vocabulary of depression is actively suppressed by the high-functioning individual, the accumulated allostatic load frequently manifests in physical symptoms, a phenomenon traditionally termed "masked depression" 720. Instead of reporting persistent low mood or anhedonia, these individuals present to primary care providers with medically unexplained physical complaints 7.
Surveys analyzing the diagnostic perspectives of psychiatrists versus general practitioners highlight a significant gap in the recognition of masked depression 720. Non-psychiatric physicians report that chronic pain is present in up to 44% of their patients with masked depression, while psychiatrists are more likely to identify cognitive symptoms such as a lack of concentration (31%) 720. Other common physical manifestations include unexplained gastrointestinal distress, extreme fatigue, severe insomnia, and sexual dysfunction - particularly in younger cohorts 720. General practitioners often misinterpret these somatic presentations as primary physical ailments, leading to an over-reliance on laboratory and radiological investigations, the prescription of ineffective somatic treatments, and a complete failure to address the underlying depressive psychopathology 720.
Sociocultural and Demographic Dimensions
The impulse to suppress depressive symptoms and maintain a facade of functionality is not merely an individual psychological phenomenon; it is heavily dictated by sociocultural norms, gender socialization, and community expectations.
Cross-Cultural Stigma and "Saving Face"
In many Asian American Pacific Islander (AAPI) communities, as well as broader minority and collectivist cultures globally, the sociological concept of "saving face" - an effort to protect reputation, honor, and dignity in social settings - creates an overwhelming barrier to acknowledging mental health struggles 362122. Within these cultural frameworks, mental illness is frequently stigmatized not merely as a personal health issue, but as a moral failing or weakness that has the potential to tarnish an entire family lineage 2122.
Consequently, high-achieving individuals within these populations may experience intense shame if they fail to uphold the "model minority" myth, which enforces positive but restrictive stereotypes regarding academic and professional success 21. Driven by the fear of ostracization and the pressure to meet familial expectations, individuals choose silence, relying on discipline rather than clinical treatment to overcome their distress 21.
These cultural differences also directly impact linguistic expression and clinical presentation. Computerized text analysis using the Linguistic Inquiry Word Count (LIWC) tool has demonstrated significant cross-cultural variations in how depressed individuals speak 23. For example, individuals from Eastern European and Asian cultures, which often exhibit more collectivistic tendencies and prioritize emotional restraint, may utilize higher degrees of self-censorship and display less explicit emotional language than individuals from Western populations 23. This cultural variability reinforces the necessity for clinicians to understand that an absence of explicit emotional disclosure does not equate to an absence of depressive pathology 232425.
Gendered Expectations and Role Strain
Gender socialization further complicates the presentation of high-functioning depression. For men, adherence to traditional masculine norms - which prioritize stoicism, self-reliance, and emotional control - forces the habitual suppression of vulnerable emotions 917. Research on men navigating major life stressors, such as a prostate cancer diagnosis, reveals that anger and externalizing behaviors often mask underlying clinical depression 17. In these models, expressive suppression acts as a direct mediator between anger and depression symptoms, highlighting how the socialization to bottle up emotions physiologically embodies itself as depressive illness 917.
Similarly, the concept of "role strain" disproportionately affects neurodivergent individuals and women of color operating in high-pressure academic or corporate environments 12. Role strain refers to the deliberate, exhausting adjustments individuals make to mitigate the conflict between their authentic selves and the neuronormative or gendered expectations of their workplace 1213. The continuous requirement to mask neurodivergent traits or engage in code-switching generates immense cognitive and emotional labor, exacerbating burnout and internal distress while outward professional compliance is flawlessly maintained 1213.
The Occupational Environment and Remote Work
The structural transformation of the modern workforce, particularly the widespread adoption of remote and hybrid work arrangements between 2024 and 2026, has introduced new complexities to the identification and management of high-functioning depression 424344452647.
While remote work theoretically offers greater autonomy and eliminates commute-related stress, it creates a digital buffer that effectively conceals the behavioral, somatic, and social signs of mental illness from colleagues and managers 424426. In a traditional office, withdrawal, changes in physical appearance, or persistent lethargy are observable metrics of distress. In a remote environment, an individual can attend a virtual meeting, present an engaged and composed facade, and immediately return to a state of emotional exhaustion off-camera 26.
Furthermore, remote arrangements frequently precipitate severe boundary erosion. Without the physical demarcation between the workplace and personal living space, remote workers often overcompensate to prove their productivity. Data analysis covering thousands of employees indicates that fully remote workers average 47.8 hours per week, compared to 41.6 hours for fully onsite employees - effectively performing an extra full workday every two weeks 44. This relentless overwork is a common manifestation of high-functioning depression, wherein continuous labor is utilized as an avoidant coping mechanism to drown out intrusive negative affect 24448.
As a result of this boundary erosion and the lack of spontaneous social interaction, recent workforce surveys identify a significant paradox: the flexibility of remote work correlates with the highest rates of psychological strain.
| Work Arrangement | Reported Stress/Burnout Levels | Isolation and Loneliness Metrics | Mental Health Symptom Prevalence |
|---|---|---|---|
| Fully Remote | Highest. 38% report severe exhaustion; elevated digital burnout 424347. | High. Up to 40% feel more isolated than tenured peers 42452649. | 40% associated with increased likelihood of anxiety/depression symptoms 444727. |
| Hybrid (1-4 days remote) | Lowest overall stress; best reported work-life balance 4428. | Moderate. Access to both social dynamics and focused autonomy 434428. | Healthiest outcomes; slightly lower odds of depression risk compared to full-time remote or onsite 4428. |
| Fully Onsite | Moderate to High, primarily driven by commute stress and lack of autonomy 4244. | Lowest. Regular face-to-face interaction and organic sensemaking 4249. | 35% likelihood of anxiety/depression; baseline metric 47. |
The phenomenon of "digital burnout" is further driven by information overload, the fear of missing out on work-related communications, and the pressure of an "always-on" culture, leading to functional decline across emotional, cognitive, and physical dimensions 454929.
Clinical Risks and Morbidity
The most severe danger associated with high-functioning depression is the latency of diagnosis. Because individuals with persistent depressive symptoms often project an image of competence, the primary barrier to receiving life-saving care is non-disclosure. Internalized stigma convinces the individual that because they can still work, their suffering is invalid or "not sick enough" to warrant clinical intervention 1453.
This delay creates a highly volatile clinical scenario. Epidemiological data and large-scale meta-analyses demonstrate that Major Depressive Disorder accounts for approximately 87% of completed suicides globally 30. Individuals living with depression face a nearly 10-fold increased risk of suicide and a doubled overall mortality rate compared to non-depressed populations 3056. The mortality risk is particularly acute within the first 180 days following a formal diagnosis, underscoring the critical importance of early intervention .
Furthermore, demographic vulnerabilities are pronounced. The suicide rate among individuals under 25 with depression is significantly elevated, and males account for roughly 80% of all completed suicides, despite women being diagnosed with depression at higher rates 30. Because PDD acts as a chronic condition without the acute physical collapse that typically prompts emergency psychiatric care, interventions for high-functioning individuals are often delayed until an irreversible crisis point is reached or until severe comorbid physical diseases - such as cardiovascular or neurological disorders driven by chronic inflammation - manifest 146.
Interpersonal Communication and Disclosure
When an individual with high-functioning depression ultimately decides to disclose their condition, they frequently encounter variations of the phrase, "But you seem fine," or "You have nothing to be depressed about." While generally born of ignorance rather than malice, these responses are deeply invalidating and demonstrate a fundamental misunderstanding of psychiatric illness 193132. The observer experiences cognitive dissonance because the individual's external productivity contradicts their stereotypical archetype of severe depression.
Addressing this dissonance requires understanding how depression fundamentally alters communication. Depression acts as a neurological filter, causing well-meaning advice or platitudes to land as criticism or accusations of inadequacy 3233. Explaining high-functioning depression successfully requires bridging the gap between internal reality and external presentation without becoming defensive. Mental health communication experts advise against trying to convince dismissive individuals by reciting diagnostic criteria; instead, the focus should shift to translating the subjective experience and asserting specific relational boundaries 19313234.
Effective communication of an invisible illness requires shifting from behavioral vocabulary (e.g., "I am still going to work every day") to emotional and metabolic vocabulary (e.g., "Going to work consumes all of my available energy, leaving me entirely depleted"). Narrative therapy techniques advocate using concrete physical metaphors to help laypersons grasp the concept. For example, comparing the condition to a physical ailment that allows for outward functioning but causes continuous pain - such as walking on a fractured ankle - can effectively bypass a listener's immediate skepticism 19313536.
The Dialectical Behavior Therapy (DBT) Framework
To navigate complex disclosures and request necessary support without capitulating to guilt, Dialectical Behavior Therapy (DBT) provides highly structured communication frameworks within its Interpersonal Effectiveness module 636437. The most prominent of these is the DEAR MAN technique, designed to help individuals assert their needs clearly, maintain self-respect, and manage defensive or dismissive reactions from family members or employers 633766676838.
When facing a loved one or supervisor who struggles to comprehend the invisible nature of the condition, the DEAR MAN framework can be applied to maintain objective effectiveness:
| DBT Step | Action Description | Clinical Application for Disclosing Hidden Depression |
|---|---|---|
| Describe | State the objective, indisputable facts of the current situation without judgment. | "I know I have been meeting all my deadlines and attending family events recently." 633767 |
| Express | Share emotional reality using "I" statements, avoiding assumptions or accusations. | "However, I have been experiencing chronic depression. Internally, I feel completely exhausted and overwhelmed." 633767 |
| Assert | Clearly and directly ask for what is needed, or set a definitive boundary. | "I need to step back from organizing the holiday gathering this year to focus on my clinical treatment." 633767 |
| Reinforce | Explain the positive outcome of respecting the request for both parties. | "Taking this time will help me recover my energy so I can be more genuinely present with the family later on." 633767 |
| Mindful | Stay rigidly focused on the primary objective; ignore distractions or attacks. | If told "But you seem fine," calmly repeat: "I understand I look fine, but my doctors and I are taking this seriously, and I need a break." (Broken Record technique) 66673870 |
| Appear Confident | Maintain steady eye contact, an even physical posture, and a firm tone. | Do not apologize for being ill, whisper the request, or stare at the floor. Present the boundary as a firm medical necessity 63676838. |
| Negotiate | Offer alternative solutions or compromises if the absolute request is impossible. | "If I cannot step back completely, I can handle the catering order, but I cannot host the event at my house." 63376738 |
Complementary DBT skills include the GIVE protocol (maintaining a Gentle, Interested, Validating, and Easy manner to preserve the relationship during conflict) and the FAST protocol (remaining Fair, offering no unnecessary Apologies, Sticking to core values, and remaining Truthful to preserve self-respect) 6438. By integrating these frameworks, the individual removes emotional volatility from the disclosure, treating their depression as an objective physiological reality that requires logistical accommodation rather than a character flaw requiring defense 3839.
Evidence-Based Communication Scripts
Despite clear, assertive communication, ingrained societal stigma and complex family dynamics - particularly generational gaps - can generate dismissive pushback. Evidence-based communication scripts emphasize the importance of brief validation followed by an immediate pivot to firm boundaries 323539.
- When met with "But you seem fine" or "You have so much to be grateful for":
- Script: "I am glad that I am still able to function externally, but clinical depression is a medical condition affecting how my brain regulates mood and energy, not a problem of ingratitude. It takes an enormous amount of effort for me to look fine right now." 193135
- When met with unsolicited lifestyle advice (e.g., "Just try yoga," "Eat better," or "Snap out of it"):
- Script: "I appreciate that you want to help, and those habits are good for general wellness. However, I am dealing with a neurobiological issue and I am working with a professional. What would help me most from you right now is just your patience, not immediate solutions." 333540
- When addressing parents or older relatives who may experience generational guilt:
- Script: "I want to share this with you because you are important to me. This is a health issue, and it is not about anything you did or did not do as a parent. I am getting help, and I just need you to understand why my availability and energy levels are shifting." 3435
- When the listener refuses to accept the reality (the invalidation pivot):
- Script: "I understand this is hard to see from the outside because my symptoms are largely invisible. However, my medical team has confirmed this is a real condition. I am not going to debate my health status, but I wanted to keep you informed of my limitations." 3941
If pushback continues, the individual must pivot strictly to behavioral boundaries. Over-explaining can inadvertently transform a boundary into a negotiation. Asserting that one does not need to continuously justify their invisible illness to access rest or medical accommodation is a vital component of long-term therapeutic recovery 5339.
Conclusion
High-functioning depression exposes a critical flaw in both societal assumptions and standard clinical assessments of mental health: the over-reliance on external productivity as the ultimate metric of psychological well-being. By mapping clinically to Persistent Depressive Disorder, this phenomenon demands recognition as a chronic, biologically taxing condition that carries severe morbidity risks, including progression to major depressive episodes and significantly heightened suicidality. The physiological toll of masking - fueled by emotional labor, cultural pressures to "save face," and the boundary-blurring isolation of remote work - silently exacerbates the underlying distress, destroying the individual's metabolic and cognitive reserves.
Addressing this hidden burden requires a systemic paradigm shift. Clinicians must refine screening protocols to look past occupational success and proactively identify internalized distress and somatic symptoms. Concurrently, individuals suffering in silence must be equipped with structured, evidence-based communication tools, such as DBT frameworks, to safely dismantle the "you seem fine" narrative. By replacing the stigma of invisible illness with objective, boundary-driven disclosure, those experiencing high-functioning depression can bridge the gap between their flawless external performance and their exhausting internal reality, securing the clinical interventions and social accommodations they desperately require.