Differences Between Low Self-Esteem and Clinical Depression
Conceptual and Diagnostic Boundaries
The relationship between low self-esteem and clinical depression is a subject of extensive clinical, academic, and psychological inquiry. While the two phenomena frequently co-occur and exhibit overlapping cognitive features, they represent fundamentally distinct psychological constructs. Clinical depression is a pervasive, multi-dimensional psychiatric syndrome encompassing biological, affective, and cognitive disruptions. Conversely, self-esteem is an evaluative dimension of the self-concept - a measure of how individuals assess their own value and capabilities. Understanding the precise diagnostic boundaries between these two entities is critical for accurate clinical assessment, targeted intervention, and the mitigation of diagnostic overshadowing.
Clinical Definition of Major Depressive Disorder
Clinical depression, formally classified as Major Depressive Disorder (MDD) in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), is a severe mood disorder characterized by a constellation of affective, cognitive, and neurovegetative symptoms 12. A formal diagnosis of a major depressive episode requires the presence of at least five specific symptoms occurring nearly every day for a minimum of two consecutive weeks, representing a clear departure from previous functioning 134. At least one of these core symptoms must be a persistently depressed mood or a marked loss of interest or pleasure (anhedonia) in almost all activities 13.
The diagnostic criteria for MDD encompass severe physiological disruptions that extend far beyond cognitive self-evaluations. These include significant, unintentional weight loss or gain; persistent insomnia or hypersomnia; observable psychomotor agitation or retardation; and pervasive fatigue or loss of energy 1235. Cognitively, individuals experience a diminished ability to think or concentrate, indecisiveness, and recurrent thoughts of death or suicidal ideation, which may culminate in a specific plan or suicide attempt 13.
Crucially, the DSM-5-TR includes "feelings of worthlessness or excessive or inappropriate guilt" as Criterion A7 134. While feelings of worthlessness heavily overlap with the concept of low self-esteem, they constitute only a single diagnostic fraction of the broader depressive syndrome. The criteria stipulate that this guilt or worthlessness may reach delusional proportions and must not be merely self-reproach about being sick 134.
The International Classification of Diseases, Eleventh Revision (ICD-11), maintained by the World Health Organization, aligns closely with the DSM-5-TR to reduce international diagnostic discordance. Under the ICD-11 code 6A70 for single episode depressive disorder, the diagnosis similarly requires a two-week duration of depressed mood or diminished interest, accompanied by additional symptoms affecting cognition, sleep, appetite, and psychomotor function 6. The ICD-11 explicitly lists "feelings of worthlessness" and "low self-esteem" as typical depressive symptoms, particularly when distinguishing healthy grief reactions from prolonged depressive episodes associated with bereavement 67. To apply a bereavement exclusion effectively, the ICD-11 notes that a diagnosis of a depressive episode in connection with a grief reaction requires symptoms to last at least four weeks and include profound indicators such as low self-esteem, suicidal ideation, or psychomotor retardation 7.
Conceptual Framework of Self-Esteem
Self-esteem refers to an individual's subjective, global evaluation of their own worth as a person, existing on a continuum from high to low 89. Theoretical frameworks generally partition self-esteem into two distinct but interrelated dimensions: self-competence and self-liking 812. Self-competence describes an individual's confidence in their personal capabilities, sense of efficacy, and belief in their ability to achieve goals. Self-liking represents the affective dimension of self-evaluation, dealing with intrinsic personal acceptance and positive self-regard independent of specific achievements 812.
Unlike Major Depressive Disorder, low self-esteem is not recognized as a standalone psychiatric diagnosis in either the DSM-5-TR or the ICD-11 91310. Instead, it functions as a transdiagnostic cognitive vulnerability that frequently accompanies various emotional and psychological difficulties, including anxiety disorders, eating disorders, codependency, and substance use disorders 910. Individuals with low self-esteem characteristically engage in pervasive negative self-talk, anticipate failure, struggle to accept compliments, and exhibit a pronounced need for external validation 81011.
While these cognitive patterns can cause substantial emotional distress and foster self-defeating behaviors - often manifesting as imposter syndrome, defensive rebellion, or victimhood - they do not inherently involve the severe neurovegetative breakdowns that define clinical depression 910. An individual can experience profound feelings of inadequacy without exhibiting psychomotor retardation, complete loss of appetite, or severe anhedonia 10121314.
Differentiating Situational Declines from Depressive Episodes
A critical clinical distinction lies between chronic clinical depression and situational drops in self-esteem. Adverse life events - such as unemployment, relationship dissolution, financial hardship, or academic failure - can trigger acute periods of self-doubt and diminished self-worth 1516. If these cognitive evaluations manifest alongside transient sadness and difficulty adjusting, clinicians may classify the presentation as an "adjustment disorder with depressed mood," commonly referred to as situational depression 1516.
Situational depression and acute low self-esteem are typically self-limiting, resolving as the individual processes the stressor, develops new coping mechanisms, or as environmental circumstances improve, typically within a six-month window 1516. The symptoms, while distressing, usually lack the profound severity and functional paralysis of MDD. In contrast, clinical depression is a persistent, chronic condition that can arise without an identifiable environmental trigger (endogenous depression) or persist long after a triggering event has passed. MDD causes profound functional impairment across occupational and social domains and typically requires pharmacological or specialized psychotherapeutic interventions, whereas situational self-esteem drops may resolve organically or with basic supportive counseling 1516.
| Feature | Low Self-Esteem | Clinical Depression (Major Depressive Disorder) |
|---|---|---|
| Diagnostic Status | Non-diagnostic; a transdiagnostic cognitive vulnerability 1310. | Formal psychiatric disorder (DSM-5-TR: MDD; ICD-11: 6A70) 16. |
| Core Characteristics | Negative global evaluation of self-worth, self-criticism, fear of failure 811. | Pervasive low mood and/or severe anhedonia (loss of pleasure) 12. |
| Somatic Symptoms | Generally absent, unless co-occurring with an affective or anxiety disorder 811. | Prominent: weight changes, insomnia/hypersomnia, severe fatigue, psychomotor alterations 15. |
| Duration and Course | Can be a lifelong stable trait or fluctuate rapidly based on social feedback 812. | Episodic or chronic; requires a minimum of two continuous weeks of severe, persistent symptoms 12. |
| Suicidality | Not a primary defining feature, though can co-occur in severe psychological distress 810. | Recurrent thoughts of death or suicidal ideation are a core diagnostic criterion (Criterion A9) 14. |
Psychometric Assessment Profiles
The phenomenological differences between self-esteem and clinical depression are distinctly captured by the psychometric instruments utilized in clinical and research settings. These validated questionnaires highlight how self-esteem assessments isolate cognitive evaluations of worth, whereas depression scales cast a wider net to capture systemic physiological and behavioral deterioration.
The Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale (RSES), developed by Morris Rosenberg in 1965, remains the preeminent psychological instrument for measuring global self-worth 171819. The RSES is a concise, 10-item self-report questionnaire that assesses an individual's overall attitude toward the self as a totality. Items are strictly cognitive and evaluative, asking respondents to rate their agreement on a four-point Likert scale (from "Strongly Agree" to "Strongly Disagree") with statements such as "On the whole, I am satisfied with myself," "I feel that I have a number of good qualities," and "I certainly feel useless at times" 81819.
The scale yields a total score ranging from 0 to 30, with scores between 15 and 25 generally considered within the normal range 20. Subscale analyses further divide the RSES into the self-competence dimension (items 3, 4, 5, 7, 9) and the self-liking dimension (items 1, 2, 6, 8, 10) 8. Notably, the RSES does not inquire about physical health, energy levels, sleep architecture, or the capacity to experience pleasure 818. It is purely an appraisal of how an individual conceptualizes their own value. Research applying item response theory to the RSES confirms its robust internal consistency (reproducibility coefficients reaching .92) and test-retest reliability (.85 to .88 over a two-week period) 171819.
Depression Inventories: PHQ-9 and BDI-II
In contrast to the focused cognitive scope of the RSES, clinical depression is measured using broad-spectrum instruments such as the Patient Health Questionnaire-9 (PHQ-9) and the Beck Depression Inventory-II (BDI-II), which capture both the affective and neurovegetative criteria of the disorder 202126.
The PHQ-9 is a 9-item tool directly mapped to the DSM-IV and DSM-5 criteria for a major depressive episode 2223. It asks patients to report the frequency of symptoms over the past two weeks on a scale from 0 ("not at all") to 3 ("nearly every day"). While item 6 explicitly touches upon self-worth ("Feeling bad about yourself - or that you are a failure or have let yourself or your family down"), the remaining eight questions focus on physiological and systemic disruptions: poor appetite or overeating, trouble falling or staying asleep, feeling tired or having little energy, psychomotor retardation or agitation, anhedonia, and suicidal ideation 2324. The PHQ-9 demonstrates excellent internal reliability (Cronbach's alpha of 0.86 to 0.89) and criteria validity; a score of 10 or greater yields an 88% sensitivity and 88% specificity for diagnosing major depression 2223.
Similarly, the BDI-II is a 21-item inventory providing granular detail on depression severity. While it measures cognitive distortions through items like pessimism, past failure, self-dislike (item 7), and worthlessness (item 14), it dedicates substantial bandwidth to somatic indicators 252632. The BDI-II asks patients to rate their loss of energy, changes in sleeping patterns, changes in appetite, crying frequency, agitation, and loss of interest in sex 252627. Scores ranging from 29 to 63 indicate severe depression 32.
The heavy weighting of somatic items in both the PHQ-9 and BDI-II mathematically and clinically distinguishes depression screening from the purely evaluative nature of the RSES 202728. Studies comparing these instruments reveal that an individual can score highly on the RSES (indicating low self-esteem) without crossing the clinical thresholds for depression on the PHQ-9 or BDI-II if their physical functioning, sleep, and hedonic capacity remain intact. Conversely, studies have shown that self-reported changes on the PHQ-9 and BDI-II during treatment do not always align perfectly with a patient's internal perception of emotional recovery, illustrating the complex, multidimensional nature of clinical depression relative to singular cognitive measures 28.
Theoretical Models of Longitudinal Interaction
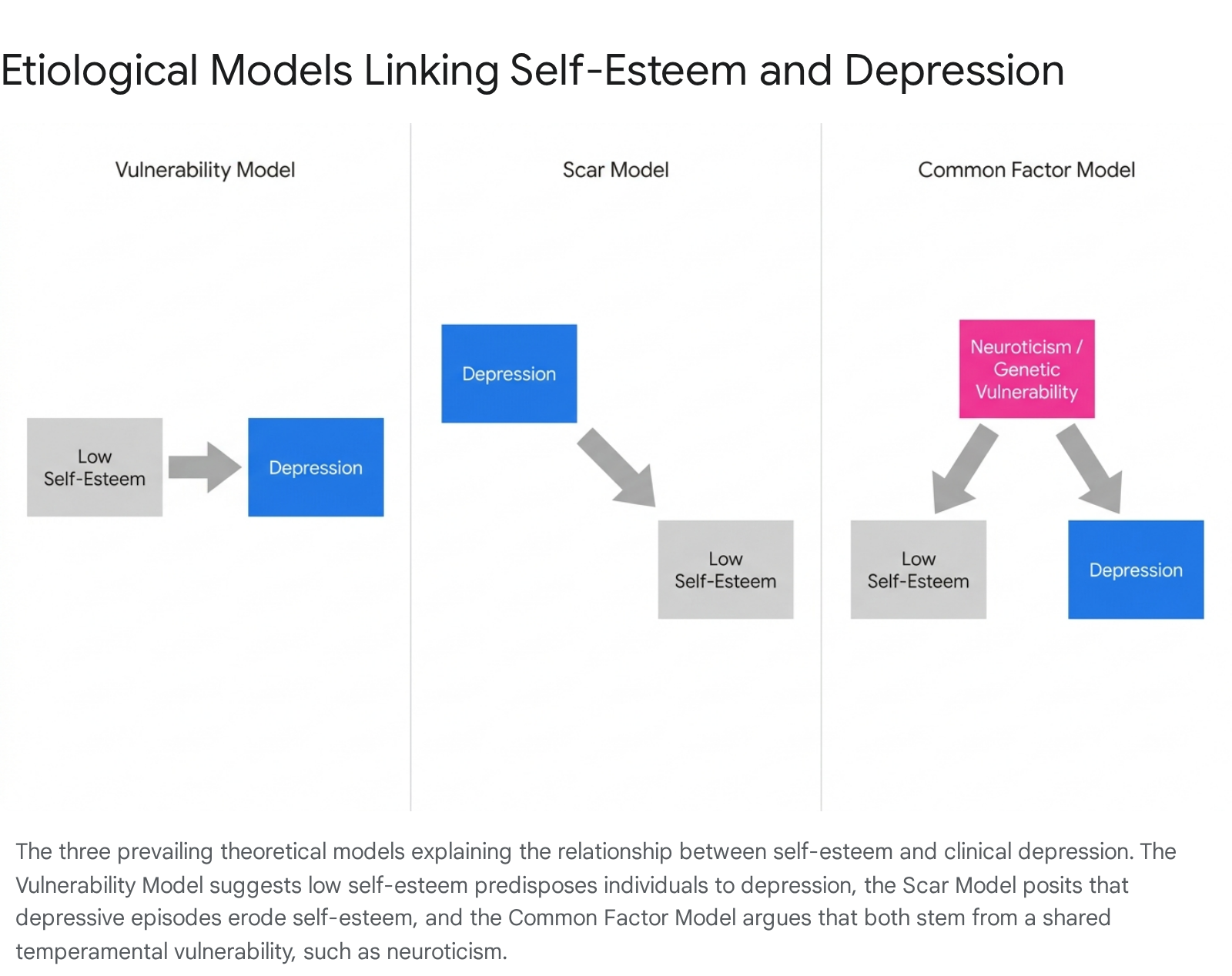
Although conceptually and psychometrically distinct, self-esteem and depression are deeply intertwined phenomenologically. Longitudinal and behavior genetic studies consistently demonstrate that low self-esteem and depressive symptoms co-occur and prospectively predict one another over time 2930. To explain the temporal and etiological relationship between the two constructs, psychological research relies on three primary theoretical models: the Vulnerability Model, the Scar Model, and the Common Factor Model 29313233.
The Vulnerability and Scar Models
The Vulnerability Model posits that low self-esteem operates as a stable, long-term risk factor that actively predisposes individuals to the development of clinical depression, particularly when confronted with stressful life events 29313233. According to this framework, individuals harboring persistent negative self-evaluations possess a profound cognitive vulnerability; they frequently catastrophize failures, expect the worst outcomes, and lack the internal psychological resilience required to buffer against distress 4041. When adversity strikes, this cognitive distortion acts as a catalyst, precipitating a full, syndromal depressive episode.
Extensive longitudinal research provides robust empirical support for the vulnerability model. A major study tracking 1,359 individuals from adolescence into middle adulthood over three decades confirmed that adolescent self-esteem prospectively predicts adult depressive symptoms 3133. Similarly, cross-lagged panel models from large datasets indicate that low self-esteem consistently predicts subsequent levels of depression independently of prior mood states 832.
Conversely, the Scar Model suggests the inverse pathway: clinical depression serves as the primary pathology, and low self-esteem is its residual consequence 29313233. In this view, experiencing a severe depressive episode - characterized by intense emotional pain, loss of occupational and social functioning, and interpersonal withdrawal - leaves permanent psychological "scars" on an individual's self-concept 33. The negative feelings and cognitive biases inherent in depression fundamentally alter how individuals process and encode self-relevant information, resulting in lowered global self-esteem that persists long after the acute affective and somatic symptoms have remitted 2933.
Meta-analyses of longitudinal data evaluating both pathways suggest that while both models possess validity, the effects of the vulnerability model are consistently more robust than those of the scar model. A meta-analysis encompassing 77 longitudinal samples found that the predictive pathway from self-esteem to future symptoms of depression was approximately twice as large (β = -.16) as the pathway from depressive symptoms to future self-esteem (β = -.08) 293233. Acknowledging this mutual influence, many researchers advocate for a Reciprocal Risk Model, which recognizes a bidirectional, reinforcing cycle where low self-esteem and depression continuously amplify one another across an individual's lifespan 2942. For example, a 25-year study assessing 978 high school seniors from age 18 to 43 found that autoregressive cross-lagged modeling supported bidirectional prospective prediction at every measurement occasion 29.
The Common Factor Model and Genetic Covariation
An alternative to direct causal pathways is the Common Factor Model. This paradigm argues that self-esteem and clinical depression do not necessarily cause one another directly; rather, their co-occurrence is the phenotypic expression of a shared underlying genetic or temperamental vulnerability 30323435.
Behavior genetic studies, utilizing trivariate twin modeling, have illuminated a substantial genetic overlap among self-esteem, depression, and neuroticism 34353637. Neuroticism - a fundamental personality trait characterized by a persistent tendency to experience negative emotions, physiological reactivity to stress, and generalized psychological distress - appears to function as the "core negative affect" variable connecting the two constructs 303537.
Large-scale structural equation modeling on population-based adult twin samples - such as the Virginia registry (n = 4672) and two Australian samples (n = 3598; n = 1878) - reveals that the covariation of self-esteem, neuroticism, and major depression is driven largely by shared genetic factors 3436. When studies control for the influence of neuroticism, the seemingly direct causal links between self-esteem and depression often diminish significantly 3236.
However, genetic research also confirms the distinctiveness of MDD as a complex clinical syndrome. In the aforementioned twin samples, the proportion of genetic risk unique to lifetime MDD (not shared with the broad neuroticism/self-esteem common factor) was estimated at 77%, 61%, and 65% across the respective cohorts 34. This indicates that while baseline self-worth and vulnerability to emotional distress are genetically linked via neuroticism, the onset of clinical depression involves substantial, disorder-specific genetic and neurobiological processes likely underlying the episodic nature of its motor, cognitive, and neurovegetative manifestations 34.
Sociocultural Modulators of Presentation
The phenomenology, expression, and conceptualization of both self-esteem and depression are not uniform across human populations; they are profoundly modulated by cultural frameworks.
Individualistic Versus Collectivistic Variations
Cross-cultural psychology demonstrates that an individual's cultural orientation dictates how self-concept is constructed and, subsequently, how depressive pathology is expressed 12383940. In highly individualistic cultures, predominantly observed in Western societies (e.g., North America, Western Europe), the self-concept is defined by independence, personal achievement, self-actualization, and autonomy 384050. Consequently, self-esteem in these cultures relies heavily on personal success and superiority relative to peers 12. When an individual from a highly individualistic culture experiences clinical depression, the disorder frequently manifests through profound cognitive distortions involving personal failure, pervasive guilt, and severe drops in self-worth 12404142.
In contrast, collectivistic cultures - predominantly found in Asian, African, and Latin American societies - emphasize group cohesion, interdependence, social harmony, and loyalty 383940. The "Cultural Trade-Off Hypothesis" suggests that individuals in collectivist societies inherently exhibit lower global self-competence but higher self-liking relative to their in-group, experiencing self-esteem as a fluid trait highly contingent upon social feedback and group standing 1243.
Crucially, the clinical presentation of depression in collectivistic societies often diverges from the cognitive-heavy DSM-5-TR standard. Rather than presenting primarily with cognitive complaints of low self-esteem, worthlessness, or guilt, individuals in collectivist cultures frequently express depression through somatic symptoms (e.g., chronic fatigue, headaches, dizziness) and anhedonia 12414244. This phenomenon of somatization allows emotional distress to be communicated through a culturally acceptable physical framework, avoiding the heavy social stigma associated with mental illness, "weak faith," or personal moral failure that can be prevalent in some Eastern societies 12404244. Thus, the direct diagnostic link between low self-esteem and clinical depression is significantly less pronounced in collectivist clinical settings compared to Western contexts.
| Cultural Orientation | Dominant Self-Esteem Source | Typical Depressive Presentation | Somatization Level |
|---|---|---|---|
| Individualistic (Western) | Personal achievement, autonomy, self-actualization 123850. | Cognitive focus: Guilt, feelings of worthlessness, self-reproach 124142. | Lower; emphasis on emotional and psychological pain 4142. |
| Collectivistic (Eastern/Global South) | Group harmony, interdependence, social role fulfillment 3840. | Somatic focus: Fatigue, dizziness, sleep disruption, anhedonia 124142. | Higher; distress communicated via physical ailments 4244. |
Modern Environmental Catalysts
In recent years, the psychological landscape has been rapidly altered by novel environmental stressors that directly impact both self-esteem stability and depression incidence, specifically the proliferation of digital media and post-pandemic socioeconomic precarity.
Digital Media Exposure and Social Comparison
The ubiquitous adoption of social media has introduced pervasive environmental mechanisms that systematically degrade self-esteem and increase the risk of depressive episodes, particularly among adolescents and young adults. Algorithms on platforms such as Instagram and TikTok expose users to highly curated, idealized portrayals of peers and influencers 454647.
This continuous exposure fosters "upward social comparison," establishing unattainable lifestyle, aesthetic, and achievement standards that actively dismantle baseline self-esteem 4546. Survey data reveals that 62% of users feel their own achievements are lacking when comparing themselves to others online, and high social media use is linked to a 60% higher risk of developing low self-esteem 47. The erosion of self-esteem via social media acts as a direct vulnerability catalyst for depressive symptoms. Studies conducted between 2024 and 2026 indicate that prolonged social media use displaces protective real-world social interactions, blunts emotional reciprocity, and severely disrupts sleep hygiene, directly compounding the risk for clinical depression 45464748. Interventions involving structured one-week abstinences from social media have demonstrated rapid, significant reductions in anxiety, insomnia, and depressive symptoms, highlighting the acute, environment-driven nature of modern self-esteem degradation 46.
Post-Pandemic Socioeconomic Chronicity
The long-term psychological sequelae of the COVID-19 pandemic have further complicated the interplay between self-worth and mood disorders. While acute generalized pandemic anxiety has begun to stabilize in high-income nations, longitudinal data spanning 2024 - 2026 reveals a persistent chronicity of psychological distress among vulnerable populations, particularly young adults facing socioeconomic precarity 4950516252.
For individuals grappling with persistent job instability, financial insecurity, and isolation, the lack of occupational achievement directly undermines self-competence 5051. The Paris Mission Locale study, which tracked socioeconomically disadvantaged young adults across two waves (T1 in 2020, n=960; T2 in 2024 - 2025, n=380), demonstrated progressive deterioration in mental health rather than recovery 5162. Mean scores on the PHQ-9 increased significantly from 9.43 to 11.35 over the four-year period, while rates of suicidal ideation nearly doubled 62.
Network analyses of these symptom clusters revealed an evolving psychopathological structure where anxiety and socioeconomic defeat became increasingly central and tightly linked to suicidal ideation and deep depressive episodes 5162. In these contexts, feelings of worthlessness transcend internal cognitive distortions; they are anchored to tangible economic and social marginalization, thereby transforming situational low self-esteem into entrenched clinical depression 495051.
Clinical and Therapeutic Implications
Recognizing the technical, etiological, and psychometric distinctions between low self-esteem and major depressive disorder is vital for optimizing psychiatric diagnosis and psychotherapeutic intervention.
Diagnostic Precision and Treatment Paradigms
Because low self-esteem is so pervasive within the general population, its role as an independent variable or a primary vulnerability factor is frequently mismanaged in clinical settings 4041. Diagnostic overshadowing occurs when practitioners fail to decouple the two constructs. For instance, a patient exhibiting severe self-criticism, chronic procrastination, and an intense fear of failure may be inappropriately diagnosed with generalized anxiety or Attention-Deficit/Hyperactivity Disorder (ADHD) when the foundational pathology is profound low self-worth 13. Conversely, focusing exclusively on a patient's cognitive self-criticism might cause a clinician to overlook the systemic neurovegetative indicators of MDD, such as early-morning awakening or marked psychomotor retardation, leading to delayed or inadequate treatment 10.
Therapeutic interventions must be tailored with precision. Pharmacological treatments - such as Selective Serotonin Reuptake Inhibitors (SSRIs) or Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs) - are highly effective at alleviating the neurovegetative and somatic symptoms of MDD 5354. They can restore sleep architecture, energy levels, and appetite. However, antidepressants do not inherently rewrite an individual's deep-seated cognitive self-concept 13. To build structural self-esteem and prevent future depressive relapse (as predicted by the vulnerability model), patients require targeted psychotherapeutic interventions. Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT) are necessary to actively dismantle negative self-schemas, challenge cognitive distortions (e.g., catastrophizing), and cultivate sustainable self-compassion 8131040.
The Mediating Role of Self-Stigma
The phenomenon of self-stigma illustrates a final, critical dynamic where clinical depression continuously suppresses self-esteem, creating barriers to recovery. When individuals are diagnosed with a psychiatric condition like MDD, they frequently internalize prevalent societal prejudices regarding mental illness, viewing their disorder as a personal failing or character weakness 55. This internalized stigma generates intense shame and guilt, further degrading the patient's global self-worth.
Research indicates that elevated self-stigma in clinical depression significantly reduces patient empowerment and self-efficacy 55. A 2025 study in the Journal of Affective Disorders found that 42% of participants with MDD reported elevated self-stigma, which had a significant negative effect on treatment engagement 55. The resulting dynamic is a vicious cycle: the diagnosis of clinical depression erodes self-esteem through stigma, and the resulting low self-esteem strips the patient of the motivation and self-efficacy required to adhere to treatment protocols and recover from the depression 5556. Addressing this complex interplay requires holistic, culturally competent care models that not only treat the physiological symptoms of MDD but actively engage in psychoeducation to restore the individual's sense of personal agency, resilience, and intrinsic worth 525556.