Rebuilding Self-Esteem After a Toxic Relationship
The dissolution of a toxic, abusive, or coercively controlling relationship initiates a complex psychological and neurobiological transition. While immediate clinical and societal interventions often prioritize physical safety and crisis containment, the long-term prognosis for survivors hinges significantly on the reconstruction of self-esteem and identity 1. Toxic relationships - characterized by prolonged emotional abuse, intimate partner violence (IPV), gaslighting, and coercive control - do not merely diminish mood; they systematically dismantle the victim's self-concept, alter the nervous system's baseline functioning, and foster deep-seated identity diffusion 123.
Rebuilding self-esteem in this context transcends superficial exercises in positive thinking or isolated cognitive reframing. Contemporary clinical research indicates that self-esteem recovery is a profound process of neurobiological rehabilitation, trauma processing, and sociocultural reintegration 34. Survivors frequently exit these dynamics burdened by internalized shame, self-blame, and a disrupted capacity for self-trust 67. Consequently, evidence-based therapeutic frameworks and public health models increasingly prioritize targeted strategies to rebuild self-worth, recognizing that restored self-esteem acts as a central mediator in mitigating psychopathology and catalyzing post-traumatic growth 15.
Neurobiological Mechanisms of Identity Erosion
Understanding the profound loss of self-esteem requires examining the physiological and structural brain adaptations that occur during prolonged exposure to interpersonal trauma. The human nervous system interprets chronic relational threats - such as contempt, unpredictable aggression, and psychological manipulation - as acute survival threats, triggering sustained stress responses that physically alter brain architecture 367.
Structural and Functional Brain Adaptations
Research into the neurobiology of maltreatment and abuse reveals that changes in the brain resulting from toxic relationships are not necessarily arbitrary damage. Rather, they represent adaptive modifications designed to facilitate survival in a malevolent environment 68. This systemic rewiring creates an ecophenotype characterized by an enhanced threat detection system and an approach-avoidance balance skewed heavily toward avoidance 6. For self-esteem, this biological reality dictates that the survivor's brain is chronically biased toward interpreting interactions as dangerous, frequently internalizing blame as a preemptive mechanism to appease the abuser and avoid conflict.
The specific neurobiological adaptations to prolonged emotional and physical abuse involve multiple brain regions, each contributing to the behavioral and psychological profile of the trauma survivor.
| Brain Region | Morphological and Functional Changes | Adaptive Function and Psychological Impact |
|---|---|---|
| Hippocampus | Reduced volume in subfields (CA3, dentate gyrus) due to stress-induced reductions in neurogenesis and dendritic arborization 612. | Impairs memory contextualization; makes it difficult for the survivor to distinguish past abusive environments from present, safe realities, sustaining chronic anxiety 6. |
| Amygdala | Initial volume increases during early neglect, followed by hyper-reactivity to threatening stimuli (e.g., fearful or angry expressions) 61213. | Prioritizes rapid detection of danger over nuanced emotional regulation; sustains a continuous state of hypervigilance and fear 69. |
| Prefrontal Cortex (PFC) | Attenuated development and diminished activity in the anterior cingulate, dorsolateral, and orbitofrontal cortices 6129. | Reduces capacity for top-down emotional regulation, executive decision-making, and inhibitory control, making the individual vulnerable to intrusive negative self-beliefs 69. |
| Sensory Cortices | Thinning of specific sensory areas associated with the abuse (e.g., somatosensory thinning, visual-limbic pathway disruptions) 6. | Acts as a sensory shield, protecting the individual from the immediate sensory processing of an aversive experience, contributing to dissociation 6. |
| Striatum | Decreased response to anticipated rewards 6. | Tips the conflict resolution balance heavily toward avoidance rather than approach, contributing to anhedonia and diminished motivation to rebuild social connections 6. |
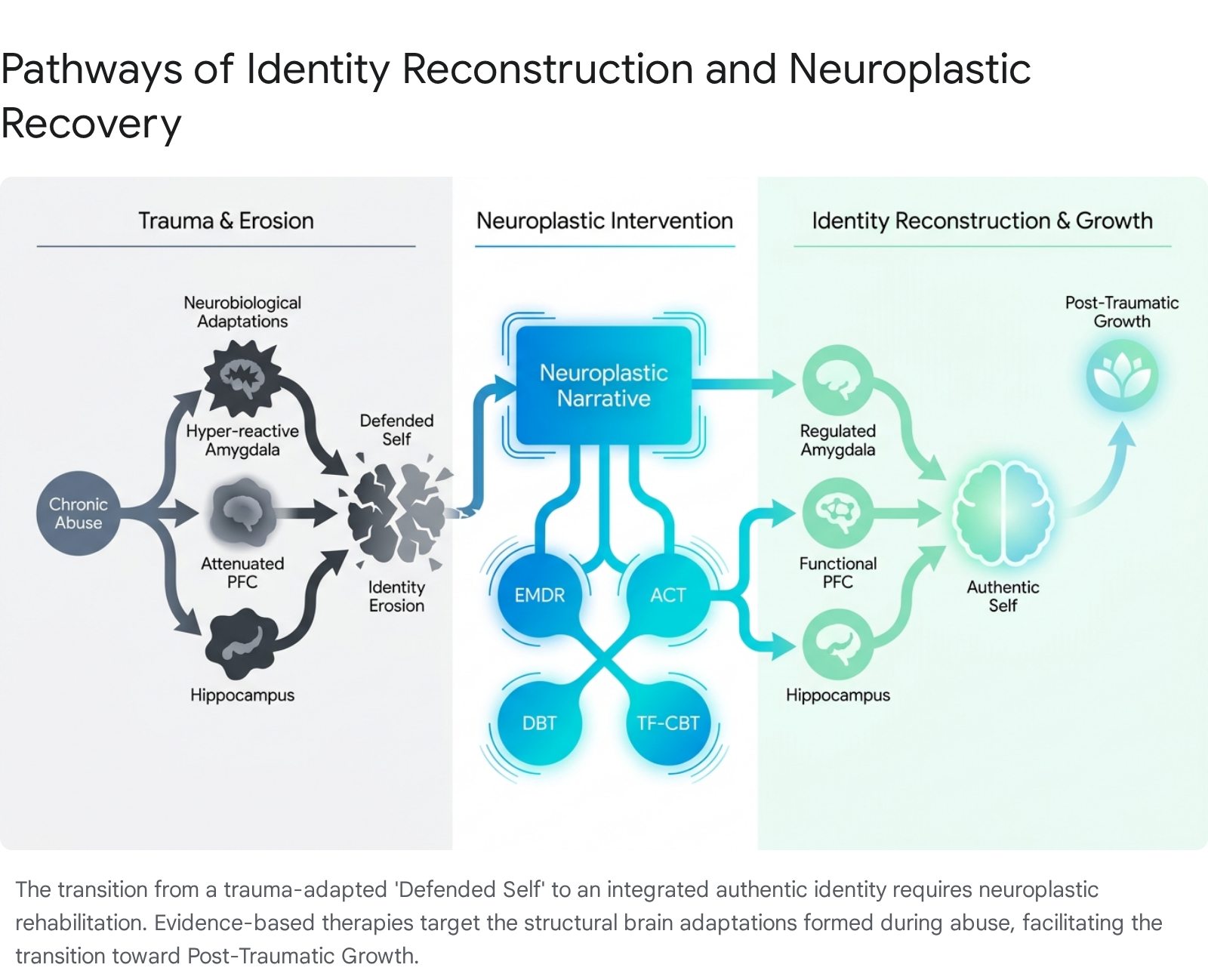
The Neuroplastic Narrative and the Defended Self
Traditional medical models have historically pathologized these neurological changes, leading to diagnoses of anxiety, depression, or complex post-traumatic stress disorder (C-PTSD) without addressing the evolutionary logic of the symptoms 8. An emerging ecological framework known as the "Neuroplastic Narrative" posits that these changes represent the brain's successful adaptation to adverse experiences 8. The brain transduces lived experiences into biological changes to better anticipate future threats 8.
When treating deficits in self-esteem, shifting from a pathological framework to the Neuroplastic Narrative is highly efficacious. It alleviates the secondary shame associated with psychiatric symptoms, allowing the survivor to understand that feelings of worthlessness, hypervigilance, and disconnection were survival strategies 18. While the toxic relationship eroded the authentic identity, it simultaneously forced the creation of a "defended self" - a protective psychological shell characterized by rigid boundaries, emotional numbness, and people-pleasing behaviors designed to monitor the abuser's mood 3.
Because the brain's baseline has been altered by trauma, rebuilding self-esteem is fundamentally tied to neuroplasticity: the brain's continuous ability to form new neural connections. Through targeted clinical interventions, environmental safety, and repetitive corrective experiences, the brain can gradually dismantle the outdated defended self, allowing the authentic self to safely re-emerge 1313.
Psychological Frameworks for Identity Reconstruction
The psychological damage inflicted by IPV, domestic violence, and emotional abuse manifests clinically as severe identity diffusion and structural dissociation. In this state, individuals struggle to maintain a coherent sense of self across different environments, leading to profound difficulties in establishing trust and regulating self-worth 2.
The Reconstruction of the Authentic Self
Identity reconstruction is not a regressive process of "finding" the person who existed prior to the abuse. Trauma permanently alters the psychological baseline, meaning the previous self cannot be fully recovered 410. Instead, recovery entails the deliberate construction of a new, integrated self. This new identity is defined by the survivor's current values, autonomous choices, and ongoing meaning-making, rather than by the parameters of the trauma 410.
The authentic self exists beneath the adaptive strategies and defensive posturing developed to survive relational contexts 10. Restoration occurs through specific, sustained practices: body-based somatic work that reconnects the individual to their physical experience, narrative work that constructs a coherent account of the abuse, and relational work that provides a safe attachment context 1011. Survivors who undertake this deep neurobiological and psychological rehabilitation frequently report arriving at a sense of self that is more grounded, authentic, and explicitly chosen than their pre-trauma identity 4.
The Illusion of Interpersonal Closure and Trauma Bonding
A significant psychological impediment to the reconstruction of self-esteem is the survivor's pursuit of "closure" directly from the abuser. Societal narratives frequently suggest that healing requires a final, honest conversation or an apology to resolve lingering questions. However, clinical consensus highlights that seeking interpersonal closure from an emotional abuser is a myth that perpetuates trauma and delays the rebuilding of self-worth 1718.
Abusive relationships operate on cycles of idealization, devaluation, and reinforcement, establishing traumatic bonds 1912. The abuser maintains power by keeping the victim in a state of cognitive dissonance and confusion; providing genuine, non-judgmental closure directly contradicts the abuser's objective of control 18.
Recent empirical research demonstrates that the "need for closure" (NFC) - a cognitive desire for definitive resolution and certainty - acts as a significant mediator in the maintenance of trauma bonding 19. Survivors exhibiting a high NFC may inadvertently prioritize the pursuit of emotional certainty over their own physical and psychological safety, increasing their susceptibility to remaining in or returning to toxic relational dynamics 19. To rebuild self-esteem, survivors must transition their understanding of closure from an interpersonal event to an internal, unilateral process. True closure involves accepting the reality of the abuse, ceasing the pursuit of the perpetrator's validation, and independently authoring a new narrative 1718.
The Trajectory of Post-Traumatic Growth
The culmination of trauma processing and identity reconstruction is often Post-Traumatic Growth (PTG). PTG is defined as the positive psychological change and advanced psychological functioning experienced as a result of struggling with highly challenging, traumatic life circumstances 131415.
The PTG journey for survivors of intimate partner violence and toxic relationships is complex, highly individualized, and non-linear. Intrapersonal recovery - possessing positive feelings toward oneself, establishing rigid self-respect, and reclaiming personal agency - forms the absolute foundation of PTG in this population 15. Studies indicate that the vast majority of IPV survivors are capable of achieving moderate to high post-traumatic growth, frequently exhibiting gains in personal strength, improved relationships with others, and the identification of new life possibilities 131416. Notably, higher levels of PTG are closely correlated with having definitively left the abusive relationship and possessing social support systems or role models who have also achieved growth 1417.
Synthesized theoretical models of trauma recovery identify eight distinct components that comprise the PTG journey for survivors of IPV.
| PTG Journey Phase | Characteristics and Psychological Manifestations |
|---|---|
| 1. Trauma before IPV | A high prevalence of survivors report previous traumatic events (e.g., childhood neglect, early abuse) that instil early vulnerabilities regarding power, control, and self-worth 18. |
| 2. Consequences of prior trauma | Prior trauma manifests in adulthood either as a "vulnerable selfhood" with porous boundaries or an overly adapted, rigid defense mechanism, both of which complicate the ability to confront later violence 18. |
| 3. The experience of IPV | The survivor is subjected to an environment resembling psychological captivity. Power is exerted through gaslighting, unpredictable aggression, and the systematic dismantling of the survivor's reality 18. |
| 4. Consequences of IPV | Severe degradation of health and well-being. Intrapersonal consequences include fear, profound shame, loss of self-esteem, and suicidal ideation. Interpersonal consequences involve deep social isolation 18. |
| 5. Facilitating factors | Constructive elements that propel PTG. These include the independent decision to seek help, accessing safe living conditions, internal resilience, and receiving trauma-informed professional support 18. |
| 6. Obstacles to growth | Destructive components that delay identity reconstruction. These include ongoing harassment from the abuser, systemic legal challenges (e.g., custody disputes), internalized self-stigma, and susceptibility to trauma triggers 18. |
| 7. Experience of PTG | The realization of positive psychological change. The survivor achieves increased inner strength, cohesive self-knowledge, a restored self-image, and an enhanced appreciation for life and personal autonomy 18. |
| 8. Lingering effects | The acknowledgment that PTG and trauma symptoms can coexist. Survivors may still experience triggers or "heavy days," but possess the psychological flexibility to manage them without losing their overarching sense of self-worth 18. |
Clinical Interventions for Self-Esteem Repair
Because the erosion of self-esteem in toxic relationships is rooted in both severe cognitive distortion and structural neurobiological dysregulation, effective treatment requires specialized psychological interventions. General supportive counseling or simple positive affirmations are insufficient to rewrite the nervous system's survival ledger 3. Meta-analyses consistently indicate that structured psychological therapies significantly outperform control conditions in reducing PTSD symptoms, depression, and low self-esteem in survivors of interpersonal trauma 19202122.
The most prominent evidence-based therapeutic modalities utilized for trauma recovery and self-worth rehabilitation include Eye Movement Desensitization and Reprocessing (EMDR), Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), Acceptance and Commitment Therapy (ACT), and Dialectical Behavior Therapy (DBT) 3132.
Eye Movement Desensitization and Reprocessing (EMDR)
EMDR is a protocol-driven psychotherapy that utilizes bilateral stimulation (typically horizontal eye movements, tapping, or auditory tones) to activate the brain's innate information processing systems 323334. The therapy operates on the Adaptive Information Processing (AIP) model, which posits that psychopathology arises from dysfunctionally stored, inadequately processed traumatic memories 3435.
Unlike traditional cognitive therapies, EMDR is a "bottom-up" somatic approach that does not require the client to extensively discuss the granular details of the trauma or complete cognitive homework outside of sessions 313637. During Phase 3 (Assessment) of the EMDR protocol, the clinician assists the survivor in identifying the specific negative core beliefs linked to the abuse. These negative cognitions generally fall into categories of defectiveness ("I am worthless"), responsibility ("It is my fault"), safety ("I am in danger"), and control ("I am powerless") 3335. As bilateral stimulation reduces the emotional and physiological intensity of the traumatic memory, the clinician facilitates the installation of preferred positive cognitions, enabling the survivor to genuinely internalize beliefs such as "I deserve respect," "I am safe now," and "I am in control of my choices" 333538.
Clinical research robustly supports EMDR's efficacy in this domain. Meta-analyses reveal large effect sizes in reducing PTSD and comorbid depressive symptoms, with improvements in self-esteem and quality of life often maintained in long-term follow-ups 23242526. Studies have explicitly shown that EMDR is highly effective in altering deeply ingrained feelings of shame, guilt, and unworthiness, systematically replacing them with a compassionate self-view 127.
However, EMDR possesses distinct clinical contraindications. Individuals with severe dissociative identity disorder (DID), active psychosis, or severe cognitive impairments may find the dual awareness required for EMDR destabilizing. Additionally, because the therapy can be physiologically activating, individuals with recent cardiac events or uncontrolled neurological conditions require careful medical assessment, and often must undergo stabilization via other modalities before EMDR can be safely administered 374445.
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
Cognitive Behavioral Therapy, particularly its trauma-focused variants, addresses the negative automatic thoughts and core schemas formed during the abusive relationship 322847. TF-CBT is a "top-down" approach that requires active cognitive engagement, relying heavily on psychoeducation, cognitive restructuring, and gradual exposure to trauma narratives 313237.
Meta-analyses continually demonstrate TF-CBT's efficacy in treating symptoms of PTSD, depression, and trauma-induced shame and mistrust, particularly among young people and adults exposed to interpersonal violence and commercial exploitation 1929. By systematically challenging cognitive distortions - such as unwarranted self-blame and internalized victim-shaming - TF-CBT helps survivors logically dismantle the abuser's narrative. While highly effective in repairing self-concept, TF-CBT requires significant homework, cognitive effort, and literacy, which may present barriers for survivors in states of acute emotional dysregulation 3637.
Acceptance and Commitment Therapy (ACT)
ACT is a mindfulness-based behavioral therapy that departs fundamentally from the traditional CBT goal of challenging or altering negative thoughts. Instead, ACT focuses on enhancing "psychological flexibility" and changing the survivor's relationship to their thoughts 493031.
For survivors plagued by an intense inner critic installed by an abusive partner, attempting to argue with thoughts like "I am unlovable" can paradoxically reinforce the trauma network by keeping the individual engaged with the abuser's narrative. ACT utilizes cognitive defusion to help individuals observe these thoughts without entanglement. A survivor learns to reframe "I am broken" to "I am noticing that my mind is generating the story that I am broken," creating immediate psychological distance 4931.
ACT mechanisms specifically tailored for self-esteem repair include: * Mindfulness and Acceptance: Acknowledging painful emotions and memories without suppressing them, thereby reducing the secondary distress caused by experiential avoidance 3031. * Values Clarification: Identifying what truly matters to the authentic self, completely separate from the abuser's demands and rules 4931. * Committed Action: Taking behavioral steps aligned with those identified values, even in the presence of severe self-doubt. This builds self-efficacy and confidence through concrete action rather than waiting for an internal feeling of confidence to appear first 4931.
Systematic reviews indicate that ACT produces moderate to large effect sizes in reducing PTSD severity, particularly for interpersonal trauma, while consistently improving emotional regulation, psychological flexibility, and social functioning 52.
Dialectical Behavior Therapy (DBT)
Originally developed to treat borderline personality disorder, DBT has proven highly effective for complex trauma, PTSD, and severe emotional dysregulation arising from chronic abuse 32445332. DBT synthesizes cognitive-behavioral techniques with mindfulness and acceptance strategies drawn from Zen philosophy, operating across four primary modules: Mindfulness, Distress Tolerance, Emotion Regulation, and Interpersonal Effectiveness 533356.
For the specific goal of rebuilding self-esteem, the Interpersonal Effectiveness module is paramount. Toxic relationships systematically destroy a person's ability to set boundaries, advocate for their needs, and manage conflict without fear of retaliation. DBT provides highly structured, actionable skills to navigate relationships while maintaining self-respect 335657. A core skill within this module is FAST, designed explicitly for Self-Respect Effectiveness during conflicts: * Fair: Being fair to oneself and others; avoiding disproportionate self-deprecation or validation of an abuser's unreasonable claims. * Apologies: Relinquishing the trauma-induced habit of over-apologizing for simply existing, having an opinion, or making a request. * Stick to Values: Maintaining personal integrity and refusing to compromise core moral beliefs to appease others. * Truthful: Avoiding exaggeration, minimizing personal pain, or lying to avoid conflict 5634.
Research confirms DBT's substantial impact; meta-analyses of trauma-focused DBT interventions report moderate to large effects in reducing PTSD symptom severity, comorbid depression, and self-harming behaviors among trauma survivors 5332. The primary limitation of DBT is the intensive commitment it requires, often necessitating both weekly individual therapy and group skills training over an extended period 313335.
Comparison of Clinical Modalities
The selection of a therapeutic intervention should be highly individualized, dependent upon the survivor's symptom severity, cognitive readiness, specific psychological deficits, and the presence of any contraindications.
| Therapeutic Modality | Primary Mechanism of Action | Processing Pathway | Impact on Self-Esteem and Identity | Clinical Contraindications and Limitations |
|---|---|---|---|---|
| EMDR | Bilateral stimulation; Adaptive Information Processing (AIP). | Bottom-Up (Sensory and Memory) | Rapidly desensitizes negative self-cognitions and installs positive self-beliefs (e.g., "I am worthy of respect") directly into memory networks 3334. | Severe dissociative disorders (DID); acute cardiac/neurological instability; lack of grounding skills 374445. |
| TF-CBT | Cognitive restructuring; psychoeducation; systematic narrative exposure. | Top-Down (Cognitive) | Logically dismantles self-blame, guilt, and cognitive distortions related to the abuse 2847. | Acute psychosis; low literacy/cognitive impairment; high initial emotional dysregulation 3237. |
| ACT | Psychological flexibility; cognitive defusion; values clarification; committed action. | Top-Down (Mindfulness and Behavioral) | Fosters self-compassion and builds self-efficacy through values-aligned behaviors, circumventing the need to argue with the inner critic 4931. | May lack the rapid physiological relief for severe intrusive flashbacks seen in processing therapies like EMDR 3052. |
| DBT | Emotion regulation; distress tolerance; structured interpersonal skills training. | Top-Down (Skills-based) | Directly builds self-respect and boundary-setting capabilities via Interpersonal Effectiveness frameworks (e.g., FAST, DEAR MAN) 5634. | Requires a high time and energy commitment; relies on an intensive program structure 3137. |
Note: In clinical practice, mental health professionals frequently utilize integrative approaches. For example, a clinician might implement DBT distress tolerance skills to stabilize a highly dysregulated survivor, subsequently transitioning to EMDR for deep memory processing once safety is established 3745.
Sociocultural Influences on Stigma and Self-Worth
The reconstruction of self-esteem does not occur in a clinical vacuum; it is heavily moderated by the survivor's sociocultural environment. The intersection of domestic abuse recovery and cultural stigma presents a profound barrier to healing, particularly in collectivist societies where identity and self-worth are inextricably linked to group cohesion rather than individual autonomy.
The Impact of Collectivist Norms on Relationship Dissolution
In many collectivist cultures - including those prevalent in South Asia, the Middle East, and Latin America - the individual ego is conceptually subservient to the greater good of the family and the broader community 603637. Consequently, self-esteem is frequently derived from maintaining group harmony, avoiding social friction, and fulfilling expected normative roles, rather than through personal achievement or self-actualization 6038.
When a survivor from a collectivist background attempts to leave a toxic or abusive relationship, they often face severe cultural backlash. Marriage is frequently viewed not merely as a partnership between two individuals, but as a binding union of families and a vital status symbol. This carries deep implications for family honor, referred to as izzat in South Asian communities 37646566. Dissolving the relationship, even to escape severe physical or psychological violence, is frequently stigmatized as a moral failure, a selfish act, or a betrayal that brings immense shame upon the extended family 36376768.
This dynamic inflicts a "second injury" on the survivor. Beyond the identity erosion deliberately caused by the abuser, the survivor must contend with public stigma, leading to intense social isolation, community rejection, and a rapid decrease in available social support 376739. Over time, this pervasive public stigma is internalized as self-stigma, leading the survivor to feel defective, responsible for the familial shame, and unworthy of a better life 3639404142.
Research underscores the devastating impact of this intersection across various regions: * East and South Asia: Among divorced, single-parent women in East Asia, self-esteem acts as a critical mediator between cultural self-stigma and severe mental health distress. Higher levels of perceived social rejection lead directly to internalized stigma, which fundamentally degrades self-esteem 542. Furthermore, the pressure to preserve family honor can result in ongoing coercion from the victim's own family to remain in the abusive dynamic, with relatives sometimes threatening self-harm or complete ostracization if the victim proceeds with a separation 3668. * The Middle East: In Middle Eastern communities, traditional patriarchal norms, strict gender roles, and the cultural imperative to conceal negative emotions often classify help-seeking as deeply shameful. In some contexts, psychological distress resulting from abuse is mischaracterized as a weakness of faith or a failure of forbearance, severely suppressing the survivor's ability to access therapy, express their reality, and rebuild self-worth 6543. * Latin America: Studies across Latin American populations regarding mental health and relationship dissolution stigma demonstrate that anticipated public stigma significantly affects individuals' self-esteem and quality of life 39. In populations of individuals lacking formal immigration status within these regions, internalized stigma has been shown to fully mediate the effect of perceived rejection on self-esteem, illustrating how compounding systemic vulnerabilities further erode identity 42.
Cultural Interventions and Social Support Systems
The presence of robust, non-judgmental social support is one of the strongest overall predictors of post-traumatic growth, the reduction of self-stigma, and the successful development of new, positive identities for survivors of IPV 1744. In collectivist contexts, restoring self-esteem requires interventions that operate simultaneously at the individual, clinical, and systemic levels.
Therapists treating survivors from marginalized or collectivist backgrounds must exercise deep cultural competence. This involves recognizing the impact of historical trauma, immigration stressors, systemic racism, and the nuanced, immense pressures of family honor 246545. Standard individualistic therapeutic models that emphasize immediate, aggressive independence and confrontation may inadvertently alienate clients whose self-worth remains partially tied to family cohesion 376576. Narrative therapy has shown particular promise in these demographics; by enabling women to rewrite their life narratives and deconstruct dominant cultural scripts, narrative approaches act as a psychosocial intervention that reframes emotional pain into coherent, empowering identity work 1119.
At the macro level, researchers strongly advocate for the implementation of comprehensive anti-stigma campaigns, community-based trauma-informed psychoeducation, and the targeted training of formal supporters (such as law enforcement, legal professionals, and religious clergy) to dismantle victim-blaming narratives at their source 414346. Facilitated peer support groups are also invaluable; they provide a substitute community that normalizes the survivor's experience, counteracting social isolation, actively dismantling cultural shame, and rapidly restoring social self-esteem 11766.
Conclusion
Rebuilding self-esteem after exiting a toxic or abusive relationship is a multifaceted endeavor that requires unwinding profound neurobiological adaptations, dismantling deeply entrenched trauma bonds, and reconstructing a fractured identity. Chronic emotional abuse and coercive control structurally alter the brain, biasing the nervous system toward threat detection, avoidance, and subjugation. Reframing these changes through a neuroplastic narrative empowers survivors to view their psychological state not as inherent defectiveness, but as a physiological survival strategy that can be intentionally rewired.
Specialized clinical therapies - most notably EMDR, ACT, DBT, and TF-CBT - provide the necessary scaffolding to process traumatic memories, neutralize the internalized inner critic, and build interpersonal self-respect and psychological flexibility. However, therapeutic success is highly contingent on mitigating the broader sociocultural environment. In collectivist communities, addressing the potent stigma surrounding relationship dissolution is essential to prevent culturally induced self-stigma from overriding clinical progress. Ultimately, self-esteem recovery is not a return to a pre-trauma baseline, but the deliberate, empowered synthesis of a new identity rooted in resilience, autonomous meaning-making, and post-traumatic growth.