Psychological Effects of Psychedelic-Induced Mystical Experiences
Research into classic serotonergic psychedelics has demonstrated that these pharmacological agents can reliably induce profound altered states of consciousness, frequently characterized within clinical literature as "mystical experiences." These transient states are phenomenologically defined by an overwhelming sense of unity, sacredness, transcendence of ordinary time and space, and ineffability. Extensive clinical trial data accumulated over the past two decades indicates a robust correlation between the acute intensity of these subjective experiences and sustained psychological benefits, including statistically significant reductions in symptoms of major depressive disorder, generalized anxiety, and substance use disorders 1234.
However, the study of psychedelic-induced mysticism is exceptionally complex, situated at the intersection of molecular pharmacology, systems neuroscience, environmental psychology, and cultural epistemology. Ongoing scientific inquiry seeks to clarify whether the phenomenological mystical experience is a strict causal mechanism driving therapeutic outcomes, or whether it acts as a correlative epiphenomenon accompanying underlying neuroplastic alterations.
Conceptualization and Measurement of Mystical States
The systematic quantification of subjective psychedelic states is foundational to establishing their therapeutic validity. This effort relies primarily on validated psychometric instruments designed to capture the qualitative intensity of the altered state of consciousness across demographically diverse cohorts.
The Development of the Mystical Experience Questionnaire
The most widely utilized instrument in contemporary psychedelic research is the 30-item Revised Mystical Experience Questionnaire (MEQ-30) 56. This assessment tool was derived from earlier, more expansive versions - such as the MEQ-43 and the States of Consciousness Questionnaire (SOCQ) - that were fundamentally based on the philosopher Walter Stace's conceptual model of mysticism 767. Stace originally proposed nine universal characteristics underlying a mystical experience: internal unity, external unity, inner subjectivity, sacredness, noetic quality, positive mood, transcendence of time and space, paradoxicality, and ineffability 7.
Subsequent psychometric validation, including exploratory and confirmatory factor analyses applied to data from controlled psilocybin administrations in laboratory settings, condensed Stace's nine characteristics into a statistically robust four-factor structure 68.
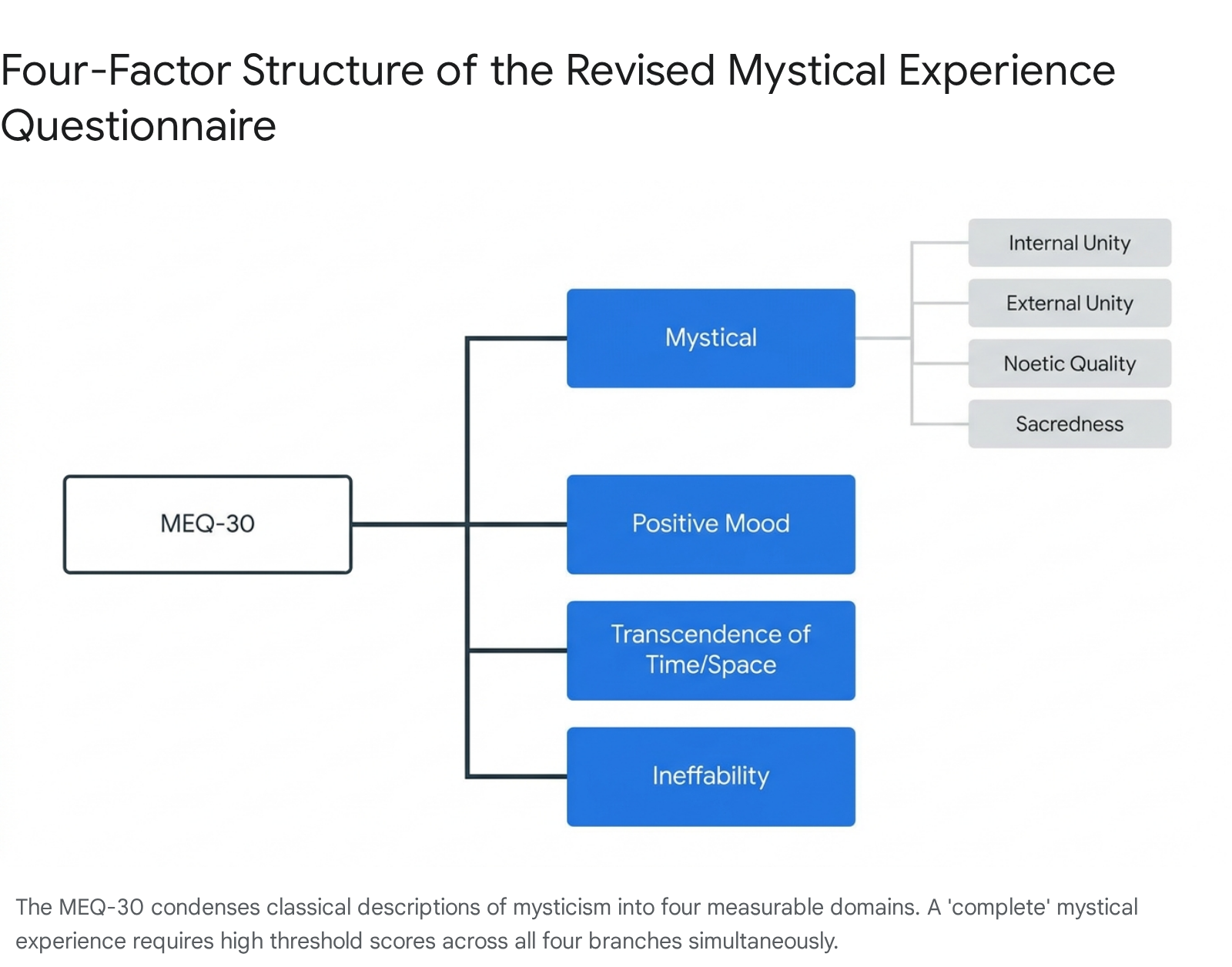
The MEQ-30 is scored on a six-point Likert scale ranging from 0 ("none; not at all") to 5 ("extreme; more than any other time in my life") 579. In modern clinical protocols, a "complete" mystical experience is conventionally defined as achieving a score of at least 60% of the maximum possible score across all four sub-dimensions simultaneously 610.
| MEQ-30 Dimension | Core Characteristics and Measurement Focus | Phenomenological Examples |
|---|---|---|
| Mystical (Unity, Noetic Quality, Sacredness) | Captures feelings of deep interconnectedness, the sense that the experience conveyed profound objective insight, and the perception of ultimate reality. Combines internal and external unity. | Freedom from personal self limitations; the psychological insight that "all is One"; awareness of a living presence in all things 69. |
| Positive Mood | Reflects the presence of intense, overwhelming positive emotional states experienced during the acute peak of the drug's effects. | Feelings of profound peace, joy, amazement, tenderness, and ecstasy 69. |
| Transcendence of Time and Space | Refers to profound alterations in the subjective perception of temporal boundaries and physical spatial orientation. | The sensation that time has slowed, stopped entirely, or that consciousness has entered a realm of infinity 69. |
| Ineffability | Measures the subjective difficulty or total impossibility of describing the experience adequately using conventional language. | The explicit cognitive sense that words are inherently insufficient to convey the reality of the phenomena encountered 69. |
Alternative Psychometric Instruments
While the MEQ-30 remains the standard, recent psychometric advancements have sought to expand this framework to capture nuances that a condensed scale might obscure. The Psychedelic Experience Scale (PES48), which was validated initially in German and subsequently in English across multiple placebo-controlled psilocybin studies, incorporates the four MEQ-30 factors but adds additional dimensions 11. The PES48 isolates "paradoxicality" and "connectedness" into distinct mystical factors - forming an expanded MEQ40 subset - while also quantifying non-mystical parameters such as "visual experience" and "distressing experience" 11.
Other frequently utilized instruments include the 5-Dimensional Altered States of Consciousness (5D-ASC) scale, which assesses "oceanic boundlessness" and "dread of ego dissolution," and the Ego Dissolution Inventory (EDI), which specifically tracks the disintegration of the narrative self 31213. To measure therapeutic utility beyond pure mysticism, researchers employ the Emotional Breakthrough Inventory (EBI) and the Psychological Insight Questionnaire (PIQ), which evaluate acute emotional catharsis and cognitive restructuring during the dosing session 1417.
Cultural Biases and Indigenous Perspectives
Despite the widespread clinical adoption of the MEQ-30, significant academic critiques highlight inherent epistemological and cultural biases embedded within the instrument. The operationalization of mysticism in contemporary psychedelic science relies heavily on a "perennialist" philosophy, a framework assuming that a discrete, universal, unmediated spiritual experience exists across all human cultures and historical epochs 15. Critics argue that this perspective, largely derived from Western European colonial observations, historically placed Christian theological concepts at the apex of religious classification while dismissing Indigenous cosmological practices as "primitive" 15.
The conceptual templates underpinning the MEQ-30 align closely with 18th-century charismatic Protestant traditions, which prioritized a highly individualized, internal, and sudden emotional awakening - such as being "sensuously overtaken" by a divine presence 15. Consequently, the scientific measurement of mysticism often operates with Christianity as the paradigmatic model. This introduces a structural bias wherein the questionnaire explicitly links theological "God-talk" (e.g., encountering "ultimate reality" or feeling a unity with the "Ground of Being") to the highest tiers of the mystical experience, inherently alienating secular or non-theistic phenomenological interpretations 1115.
Furthermore, the MEQ-30 exhibits a stringent positive bias. By defining mystical and spiritual phenomena as inherently unitive, peaceful, and blissful, the instrument fails to capture profound, highly impactful spiritual experiences that are challenging or nihilistic, such as encounters with perceived malevolent entities, "hell" realms, or physical sensations of being violently consumed by the universe 15.
Indigenous scientific frameworks and Traditional Ecological Knowledge (TEK) offer contrasting paradigms. In many Indigenous cultures, particularly those utilizing traditional plant medicines like ayahuasca or peyote, nature and spirituality are not abstract concepts encountered by a subjective, isolated individual; rather, the environment is an active, animate participant in a continuous, interconnected reality 1617. Western assessments focusing on distinct "unitive experiences" may therefore fail to capture the baseline phenomenology of individuals from cultures where the world is already perceived as fundamentally united and animate 15. Western biomedical science typically views health as the absence of illness, whereas Indigenous practices view it as a composite measure of thriving spiritual, mental, emotional, and physical health interwoven with the community 16.
Pharmacological Agents and Experiential Profiles
Classic psychedelics - primarily psilocybin, lysergic acid diethylamide (LSD), and N,N-dimethyltryptamine (DMT) - share a primary mechanism of action as agonists or partial agonists at the serotonin 2A (5-HT2A) receptor 121819. However, variations in receptor affinity, secondary receptor profiles, pharmacokinetics, and routes of administration produce distinct experiential profiles and highly variable rates of mystical experience induction.
Psilocybin and Lysergic Acid Diethylamide
Psilocybin (the prodrug of psilocin, the primary psychoactive compound in various species of fungi) and LSD are the most extensively studied compounds in modern clinical trials. Both are typically administered orally in controlled settings, possessing distinct durations of action: 4 to 8 hours for psilocybin, and 8 to 12 hours for LSD 121823.
Dose-response studies indicate that moderately high doses of psilocybin (typically 20 to 30 mg per 70 kg of body weight) reliably induce mystical-type experiences in a majority of healthy volunteers and treatment-resistant psychiatric populations 1810. LSD, administered at clinical doses of 100 to 200 μg, produces similarly profound alterations in consciousness. Direct phenomenological comparisons utilizing the 5D-ASC scale reveal that medium to high doses of LSD yield significantly higher ratings of "visionary restructuralisation" compared to equivalent doses of psilocybin 12. Pharmacologically, while both substances bind avidly to the 5-HT2A receptor, LSD induces significantly higher levels of inositol phosphate (IP) formation at this receptor site than both DMT and psilocin, suggesting a distinct intracellular signaling cascade 12.
Recent Phase 2b clinical data investigating a proprietary formulation of LSD (MM120) for generalized anxiety disorder demonstrated potent efficacy. In a double-blind, placebo-controlled trial of 198 adults, a 100 μg oral dose produced rapid, significant, and durable anxiolytic effects that persisted for at least 12 weeks without concurrent psychotherapeutic integration 2021. Notably, 65% of participants maintained a clinical response, and 48% achieved complete disease remission by week 12 2122. The 100 μg dose was highly psychoactive, inducing hallucinations in 93% of participants 20.
Dimethyltryptamine and 5-Methoxy-Dimethyltryptamine
N,N-Dimethyltryptamine (DMT) and its structural analog 5-Methoxy-N,N-Dimethyltryptamine (5-MeO-DMT) are tryptamine alkaloids characterized by extremely rapid onsets and short durations of action when administered parenterally or via inhalation. Exogenous DMT is rapidly metabolized by peripheral monoamine oxidase (MAO) enzymes in the gut and liver, rendering it entirely inactive when ingested orally as a standalone compound 232723.
Intravenous administration of DMT fumarate bypasses this metabolic barrier, inducing profound psychological effects almost immediately. Effects peak between 90 and 120 seconds and resolve almost completely within 30 minutes 2425. Clinical dose-finding studies delineate a precise response curve for IV DMT: doses of 0.05 to 0.1 mg/kg are primarily somatic and affective, lacking intense hallucinations; 0.2 mg/kg represents the hallucinogenic threshold; and 0.3 to 0.4 mg/kg doses trigger full ego-dissolution alongside an immersive, rapidly moving, brightly colored visual display 2531. Vaporized free-base DMT operates on a similar timeline, with typical "breakthrough" doses reported between 40 and 50 mg 2724.
Clinical trials evaluating BPL-003, a novel synthetic intranasal benzoate salt formulation of 5-MeO-DMT, have demonstrated a highly reliable induction of mystical experiences. At single doses of 10 mg and 12 mg, 60% of psychedelic-naïve participants achieved a "complete mystical experience" based on the MEQ-30 criteria 2326. Systemic exposure and subjective intensity increased dose-proportionally, with a remarkably rapid onset and acute effects resolving completely in under two hours 26. Comparative psychometric data suggests that inhaled 5-MeO-DMT occasions mystical effects at an intensity significantly higher than moderate doses (20 mg/70 kg) of psilocybin, and is statistically equivalent to the intensity of high doses (30 mg/70 kg) of psilocybin 10.
Ayahuasca and Ceremonial Contexts
Ayahuasca is a traditional Amazonian decoction typically brewed from the Banisteriopsis caapi vine and the leaves of the Psychotria viridis shrub 2335. The pharmacological synergy of the brew relies on harmala alkaloids (such as harmine, harmaline, and tetrahydroharmine) within B. caapi, which act as reversible inhibitors of monoamine oxidase-A (RIMAs) 232427. This enzymatic inhibition prevents the rapid gastrointestinal breakdown of the DMT contained in P. viridis, allowing the compound to enter systemic circulation, cross the blood-brain barrier, and activate central 5-HT2A receptors 2327.
The resulting pharmacokinetic profile differs starkly from inhaled or intravenous DMT. Ayahuasca induces a gradual onset of psychoactive effects that persist for 4 to 6 hours, occasionally extending up to 12 hours depending on the specific alkaloid ratios of the brew 142335. Phenomenologically, the experience is described as less immediately overwhelming than freebase DMT, allowing for prolonged introspective, narrative, and emotional processing 2335.
Clinical evaluations of standardized ayahuasca analogs (e.g., formulations combining 100 mg of oral harmine with incremental intranasal DMT dosing) demonstrate robust induction of psychological insights and emotional breakthroughs with high personal and spiritual significance 14. In contrast to the highly controlled, sterile environments of modern Western clinical trials, botanical ayahuasca is traditionally consumed in communal, ritualistic settings guided by experienced practitioners (shamans or curanderos). The ceremonial context explicitly emphasizes spiritual healing and physiological purging (emesis), heavily influencing the overarching psychological outcome and therapeutic integration 3527.
| Pharmacological Agent | Primary Receptor Target | Standard Route of Administration | Typical Duration of Action | Acute Phenomenological Profile |
|---|---|---|---|---|
| Psilocybin | 5-HT2A Agonist | Oral (Capsule/Fungi) | 4 to 8 hours | High rates of mystical experience, deep emotional processing, manageable visual alterations 11012. |
| LSD | 5-HT2A / Dopamine D2 Agonist | Oral (Sublingual) | 8 to 12 hours | Intense visionary restructuralization, extended temporal distortion, high cognitive stimulation 121828. |
| DMT (Base/Fumarate) | 5-HT2A / Sigma-1 Agonist | Inhalation / Intravenous | 15 to 30 minutes | Rapid onset, total environmental displacement, dense and rapidly moving geometric visual displays 242531. |
| 5-MeO-DMT | 5-HT1A / 5-HT2A Agonist | Inhalation / Intranasal | 30 to 90 minutes | High rates of ego dissolution and "void" states, potent somatic effects, lower visual geometry than DMT 102326. |
| Ayahuasca | 5-HT2A Agonist + MAOI | Oral (Botanical Decoction) | 4 to 6 hours | Gradual onset, sustained emotional and autobiographical processing, frequent physiological purging 142335. |
Neurobiological Mechanisms of the Psychedelic State
Advancements in advanced neuroimaging techniques, particularly functional magnetic resonance imaging (fMRI) and electroencephalography (EEG), provide a sophisticated mechanistic understanding of how psychedelics disrupt ordinary waking consciousness to facilitate mystical states. The subjective phenomena of ego dissolution and universal unity are increasingly mapped to specific, measurable alterations in functional connectivity (FC) across distinct brain networks.
Disruption of the Default Mode Network
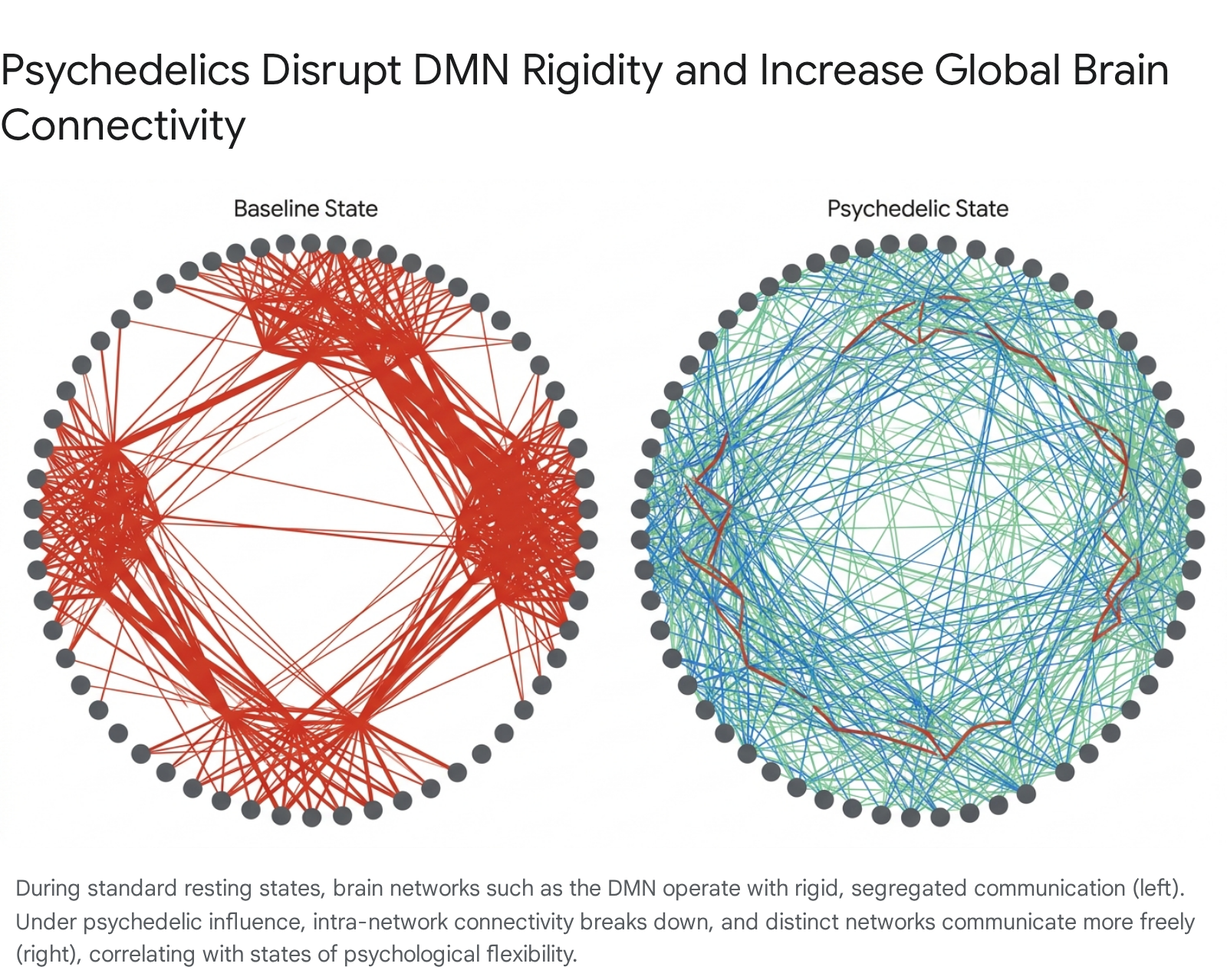
A primary and highly consistent neurobiological signature of classic psychedelics is the acute disruption of resting-state connectivity within the Default Mode Network (DMN) 28293031. The DMN is a widespread network of interacting cortical regions - principally the medial prefrontal cortex (mPFC), the posterior cingulate cortex (PCC), the angular gyrus, and the precuneus 282932. In standard waking states, the DMN is highly active and highly synchronized, supporting self-referential processing, autobiographical memory retrieval, social cognition, and the maintenance of a continuous narrative identity (the psychological "ego") 3233.
Hyperconnectivity and structural rigidity within the DMN are strongly implicated in the pathophysiology of depressive disorders, generalized anxiety, and substance addiction, manifesting behaviorally as repetitive negative rumination and maladaptive self-focus 293033. Under the acute influence of psilocybin, LSD, and DMT, functional connectivity within the DMN is significantly decreased, decoupling core integrative hubs like the mPFC and PCC 282932. This dissolution of hierarchical network integrity tightly correlates with subjective clinical reports of ego dissolution and the transcendence of personal identity boundaries - the core psychometric features of the mystical experience 283233.
Animal models have successfully validated these human neuroimaging findings. High-resolution MRI in rat models administered psilocybin reveals significant decreases in connectivity strength across widespread cortical clusters, including the prefrontal cortex, insula, and hippocampus 43. Furthermore, psilocybin administration effectively blunts disease-specific DMN hypoconnectivity in alcohol use disorder phenotypes, offering a neural correlate for the drug's anti-addictive properties 43.
Thalamocortical Gating and Global Brain Connectivity
While psychedelics disintegrate the internal cohesion of the DMN, they simultaneously increase global brain connectivity and integration between distinct functional networks that rarely communicate during baseline states 282932.
Functional connectivity increases between the DMN and task-positive, visual, sensorimotor, and salience networks, fostering a state of neural entropy and heightened signal complexity 293234.
The thalamus acts as a central neurobiological gating mechanism, filtering sensory and cognitive information ascending to the cortex. Psychedelics broadly increase connectivity between the thalamus and various cortical regions (thalamocortical connectivity), effectively overwhelming the cortex with uninhibited sensory and limbic data 2832. Specifically, LSD has been shown to increase functional connectivity between the thalamus and the lingual gyrus, striatum, and insula 2834.
Subcortical regions heavily involved in associative memory and emotional regulation - such as the amygdala and hippocampus - also demonstrate significant alterations. Psilocybin has been shown to reduce excessive amygdala reactivity and decrease functional connections to and from the right amygdala, a mechanism likely underlying its high efficacy in resolving trauma and intractable anxiety 34. Conversely, under the influence of DMT, the brain reorganizes into a hyperconnected state where subcortical structures gain unusual prominence, loosening the hierarchical organizing control typically maintained by the prefrontal cortex and exposing the user to intense emotional catharsis 32.
Extra-Pharmacological Variables and Trial Methodology
Not all psychedelic administrations result in mystical experiences; therapeutic and phenomenological outcomes are highly variable and subject to numerous psychological and environmental modulators. Identifying and controlling these extra-pharmacological variables is a critical focus for optimizing trial methodology.
Participant Personality and Expectancy Effects
Baseline personality traits significantly influence the trajectory of a psychedelic session. Data derived from large longitudinal and clinical cohorts indicates that the Big Five personality trait of "openness to experience" consistently relates to enhanced mystical states, visual phenomena, and overall positive experiences 353647. Trait openness acts as both a predictor of therapeutic success and a consequence of it, establishing a positive feedback loop 36. Conversely, higher baseline neuroticism correlates with a higher probability of enduring challenging, anxious, or dysphoric experiences during the acute drug phase 3537.
Furthermore, expectancy bias - the conscious or subconscious anticipation of positive outcomes influenced by media hype, preparatory psychotherapy, and cultural narratives - is a profound confounding variable in modern psychedelic trials 383940. Individuals with high positive outcome expectations are vastly more willing to participate in trials, potentially skewing enrollment toward highly motivated, risk-tolerant demographics 47. The overt, unmistakable psychoactive effects of classic psychedelics result in pervasive "functional unblinding," meaning participants and clinicians quickly realize whether the active drug or a placebo was administered 2241. If participants recognize they are in the active arm, high outcome expectations can synergize with pharmacological effects, inflating the perceived therapeutic efficacy and complicating direct comparisons with conventional psychopharmacology 3842.
Standardization of Set and Setting
The contextual environment - summarized in the psychedelic literature as "set and setting" - plays a determinative role in whether a psychedelic experience manifests as a deeply therapeutic mystical state or a severe psychological crisis. Psychedelics rapidly amplify environmental stimuli, meaning identical neurochemical dosages can trigger profound spiritual unity in a supportive clinical environment or severe paranoia in a sterile, unsupported hospital ward 4143.
To address the historical lack of methodological rigor in documenting these environmental variables, an international Delphi consensus study produced the ReSPCT (Reporting of Setting in Psychedelic Clinical Trials) guidelines in 2025 434445. Synthesizing input across four iterative rounds from 89 researchers and clinicians across 17 countries, the guidelines established 30 critical extra-pharmacological variables requiring standardized reporting 4345.
| ReSPCT Guideline Domain | Key Variables Monitored and Reported | Methodological Rationale |
|---|---|---|
| Physical Environment | Room aesthetics, lighting, comfort, proximity to medical equipment, and clinical versus non-clinical ambiance. | Prevents environmental stressors from inducing acute anxiety or paranoia during the vulnerable psychedelic state 4357. |
| Dosing Session Procedure | Use of specific music/soundscapes, presence of guiding personnel, and rigorous management of external interruptions. | Ensures the auditory and social environment is curated to support internal focus and emotional breakthrough 4345. |
| Therapeutic Framework | Theoretical orientation of the psychotherapists, duration of preparation protocols, and structured integration practices. | Standardizes the psychological scaffolding that helps patients interpret and integrate mystical phenomena 4357. |
| Subjective Experiences | Degree of participant autonomy, physical interactions, and methods for obtaining ongoing consent during the session. | Protects patient agency and tracks interpersonal dynamics that influence the sense of safety and surrender 4345. |
Drug Interactions with Serotonergic Antidepressants
A major clinical barrier to the widespread adoption of psychedelic therapy has been the theoretical risk and presumed efficacy blunting associated with the concomitant use of conventional antidepressants, specifically Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) 46. Because SSRIs operate by increasing synaptic serotonin, chronic use reliably downregulates cortical 5-HT2A receptors, the primary target required for psychedelic activation 46.
Retrospective and prospective survey data confirms that concurrent use of SSRIs/SNRIs - and even recent discontinuation within one to three months prior to dosing - frequently blunts the acute subjective intensity of psilocybin 474849. Individuals actively taking serotonergic antidepressants report significantly lower aggregate scores on the MEQ-30, experiencing 18% weaker mystical states, 50% fewer challenging experiences, and 31% fewer emotional breakthroughs compared to medication-naïve participants 4748.
However, secondary analyses of clinical trial data present a nuanced paradox: while the subjective intensity and mystical features of the experience are statistically attenuated by SSRIs, the therapeutic clinical outcomes (i.e., reductions in depressive severity) remain largely intact and statistically similar to non-medicated cohorts 4648. Furthermore, requiring patients with severe, chronic depression to undergo a rapid tapering and washout period from their SSRIs prior to a psychedelic trial frequently destabilizes their mood, leading to severe withdrawal symptoms and increased baseline depression, which can ultimately hinder the therapeutic process 46. Consequently, modern clinical protocols are increasingly exploring the simultaneous administration of psychedelics and standard antidepressants to maximize safety 46.
Clinical Efficacy and the Role of the Mystical Experience
The ultimate clinical utility of psychedelic-induced altered states rests in their capacity to catalyze enduring changes in psychological health. The clinical data surrounding classic psychedelics indicates rapid, highly durable efficacy across several intractable psychiatric indications.
Durability of Psychiatric Interventions
Psilocybin-assisted psychotherapy (PAP) has demonstrated unprecedented durability in the treatment of Major Depressive Disorder (MDD) and Treatment-Resistant Depression (TRD). In landmark randomized, wait-list controlled trials, participants receiving moderate to high doses of psilocybin (e.g., 20 mg and 30 mg sessions) alongside supportive psychotherapy exhibited rapid and massive reductions in depression severity 1.
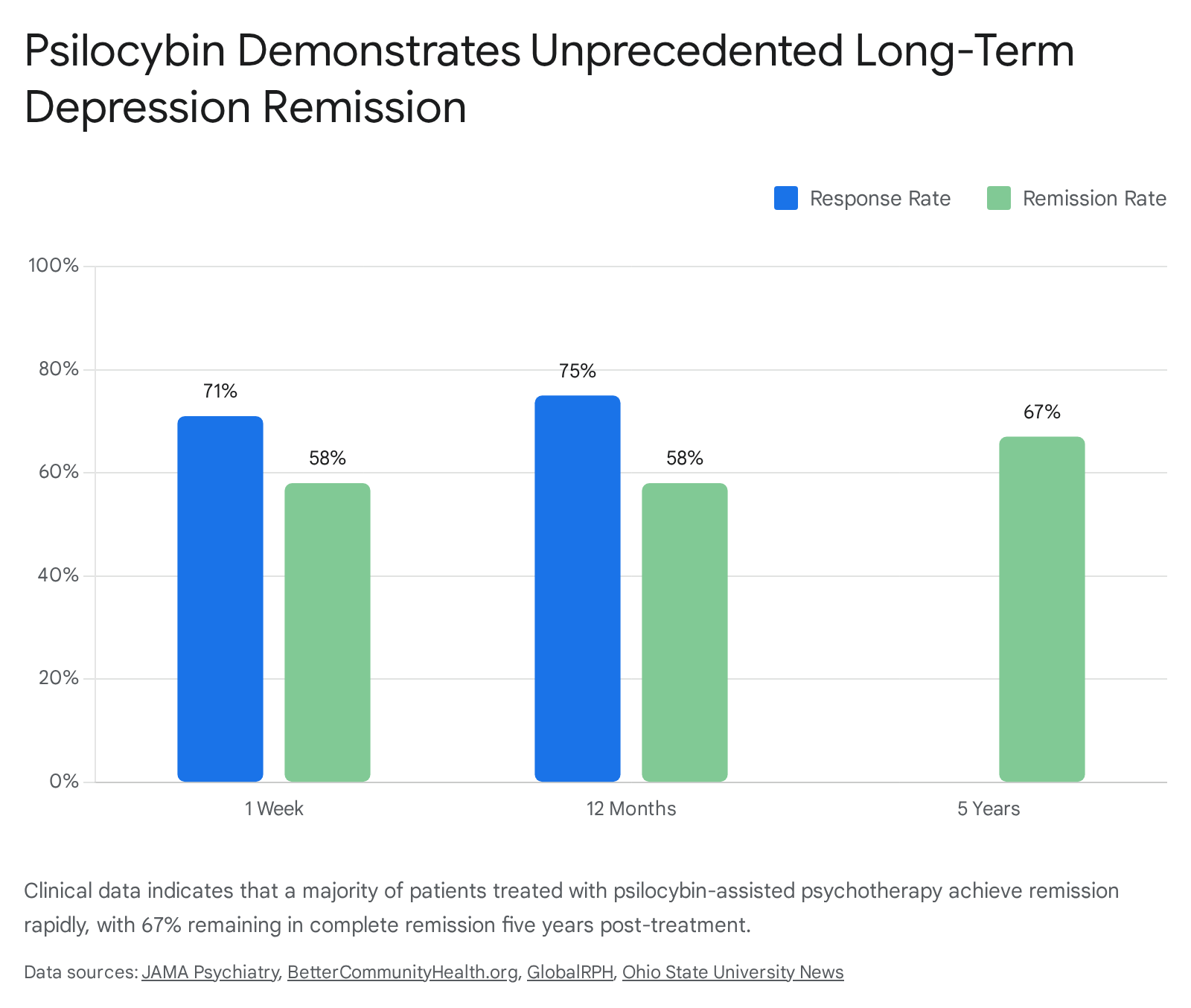
Long-term follow-up data underscores the remarkable sustainability of these interventions. In one cohort of 27 participants, depression severity scores (GRID-HAMD) plummeted from a baseline of 22.8 to 8.5 within four weeks 1. Participants maintained clinically significant improvements up to 12 months post-treatment, yielding a 75% response rate and a 58% complete remission rate 462. Unprecedentedly, five-year follow-up data from the same trial revealed that 67% of participants remained in complete remission from MDD, reporting sustained improvements in baseline anxiety, global occupational functioning, and overall life satisfaction 50.
These long-term outcomes contrast sharply with standard selective serotonin reuptake inhibitors, which generally require chronic daily administration and frequently suffer from high relapse rates upon cessation 4.
Beyond depression, psychedelic therapies display broad efficacy in treating severe anxiety disorders and existential distress. In double-blind randomized trials involving patients with life-threatening cancer diagnoses, psilocybin induced massive reductions in end-of-life anxiety and depression, with sustained clinical responses extending well beyond six months 36251.
Is the Mystical Experience a Necessary Catalyst?
A central, highly contested debate in psychopharmacological research revolves around whether the subjective mystical experience is causally necessary for therapeutic success, or if it is merely a psychological marker of the neurobiological neuroplasticity occurring at the cellular level.
A substantial body of meta-analytic data supports the premise that the intensity of the subjective psychedelic experience is reliably and positively correlated with clinical improvements, particularly in mood disorders 265. A meta-analysis of 34 independent studies confirmed a globally significant positive association (R=0.33) between subjective intensity and clinical outcome, with the correlation peaking robustly for mood disorders (R=0.41) 265. Studies utilizing the MEQ-30 frequently identify high total mystical scores, alongside high levels of "oceanic boundlessness" and low levels of "dread of ego dissolution," as the primary predictors of long-term symptom reduction 31951. Furthermore, machine learning algorithms utilizing Natural Language Processing (NLP) to analyze post-session integration transcripts have accurately predicted long-term responder status (with 88% accuracy) based solely on the emotional valence and breakthrough metrics articulated by the patient, tightly linking subjective processing to clinical outcomes 17.
Conversely, emerging clinical data challenges the absolute necessity of the mystical threshold. Certain trials investigating psilocybin for TRD have found that while mystical experiences strongly correlated with response following an initial dose, the effect disappeared entirely upon subsequent dosing, suggesting diminishing predictive returns 19. Other rigorous placebo-controlled and wait-list controlled trials have failed to find any significant correlation between MEQ-30 scores and long-term depressive improvements 19.
A highly novel 2024 study of psychedelic-assisted therapy in Switzerland indicated that patients who achieved a state of deep physiological and psychological relaxation during their session experienced the most pronounced antidepressant effects, statistically outperforming mystical insight or ego dissolution as a predictor of success 52. In fact, compared to healthy participants, the clinical patients undergoing therapy reported overall lower levels of ego dissolution, yet still achieved remission 52.
Additionally, the observation that SSRIs significantly blunt the mystical intensity of psilocybin while perfectly preserving its antidepressant efficacy suggests that structural neuroplastic mechanisms - such as the promotion of neural stem cell growth, dendritic arborization, and the reopening of critical learning periods for social reward circuitry - may drive psychiatric recovery independently of the subjective trip 234248. This has spurred pharmaceutical interest in "psychoplastogens" - novel compounds engineered to trigger neuroplasticity at the 5-HT2A receptor without inducing hallucinogenic or mystical effects 65.
In summary, classic psychedelics can reliably induce profound, unitive altered states of consciousness when administered at sufficient dosages within highly curated, supportive clinical contexts. These mystical-type experiences are tightly correlated with rapid, dramatic, and enduring improvements in intractable psychiatric conditions. As the field continues to mature, standardizing the measurement of extra-pharmacological variables, diversifying the cultural frameworks of measurement beyond Western templates, and successfully decoupling the raw neurobiological mechanisms of action from the subjective experience will be vital for fully integrating these powerful compounds into mainstream psychiatry.