Is Intermittent Fasting Better for Metabolic Health
Intermittent fasting and daily calorie restriction produce nearly identical results for weight loss and long-term metabolic health in the vast majority of people. While rigorous clinical trials show that specific fasting schedules - like alternate-day fasting - can offer a slight edge in adherence and modest additional weight loss, the overall scientific consensus now views fasting primarily as an effective behavioral tool for reducing calorie intake, rather than a unique metabolic hack.
For the better part of the last decade, the debate over intermittent fasting has felt less like a scientific discourse and more like a culture war. Proponents have argued that restricting when you eat unlocks ancient biological pathways, melting visceral fat and reversing insulin resistance in ways that standard calorie counting cannot. Skeptics, meanwhile, have maintained that fasting is merely a psychological trick to force a calorie deficit, essentially putting old wine in a new bottle.
Until recently, both sides relied heavily on animal models, observational data, and small, short-term human trials to make their case. But between 2022 and 2026, the scientific landscape shifted dramatically. A wave of massive, gold-standard randomized controlled trials (RCTs) and comprehensive network meta-analyses were published in leading medical journals like The BMJ, Annals of Internal Medicine, and Science Translational Medicine 122.
By putting intermittent fasting head-to-head against traditional continuous energy restriction (CER) in long-term human populations, researchers have finally generated high-quality, actionable data. This report provides an exhaustive look at what the latest science actually proves about fasting, metabolic health, and cardiovascular risk.
Defining Metabolic Health and the CKM Framework
Before evaluating whether intermittent fasting improves metabolic health, it is necessary to define what metabolic health actually entails. In the popular consciousness, metabolic health is often conflated entirely with body weight. However, clinical researchers have long recognized that body mass index (BMI) is a deeply flawed proxy for the functional and molecular status of an individual's metabolism 3.
The Nuances of Metabolically Healthy Obesity
Although obesity is typically associated with metabolic dysfunction and an elevated risk of cardiometabolic diseases, some individuals with obesity appear protected from many of the adverse metabolic effects of excess body fat. This phenomenon is known as "metabolically healthy obesity" (MHO) 45.
For years, the definition of MHO was heavily debated, with more than 30 different definitions utilized across various studies 45. Most research defined MHO as having one or two components of metabolic syndrome - meaning many people labeled as "metabolically healthy" were not actually healthy, but simply had fewer metabolic abnormalities than their peers with metabolically unhealthy obesity (MUO) 4.
When researchers apply a strict definition of metabolic health - defined as the complete absence of any metabolic syndrome components and normal insulin sensitivity (assessed by a normal HOMA-IR score) - the prevalence of true MHO drops to approximately 5% to 7% among individuals with obesity 4. For the remaining vast majority, excess visceral adipose tissue drives systemic inflammation, oxidative stress, and insulin resistance 6.
The Cardiovascular-Kidney-Metabolic (CKM) Syndrome
To clarify these interconnected risks, the American Heart Association (AHA) issued a landmark presidential advisory in late 2023, formally defining a new medical condition: Cardiovascular-Kidney-Metabolic (CKM) syndrome 679. The AHA recognized that excess adiposity, insulin resistance, hypertriglyceridemia, high blood pressure, and declining kidney function do not exist in silos; they are deeply interconnected pathophysiological systems that drive multiorgan dysfunction 67.
The AHA proposed a novel, five-stage model to classify CKM syndrome and guide preventive care: * Stage 0: No CKM risk factors. The focus is entirely on prevention 69. * Stage 1: Excess or dysfunctional adiposity (unhealthy weight gain or abnormal fat distribution) 6. * Stage 2: The presence of specific metabolic risk factors, including hypertriglyceridemia, hypertension, metabolic syndrome, type 2 diabetes, or moderate-to-high-risk chronic kidney disease 6. * Stage 3: Subclinical cardiovascular disease presenting alongside CKM syndrome, or high predicted cardiovascular risk 6. * Stage 4: Clinical, established cardiovascular disease, which may also include kidney failure 69.
Because CKM affects nearly every major organ in the body - including the heart, brain, kidneys, and liver - identifying interventions that can halt or reverse progression through these stages is a global public health imperative 9. It is against this rigorous framework of systemic metabolic health that the true efficacy of intermittent fasting must be judged.
The Biology of the "Metabolic Switch"
To understand why intermittent fasting captured the attention of researchers in the first place, we must look at evolutionary biology. In 2018, Dr. Mark Mattson, a neuroscientist at the National Institute on Aging, formalized a highly influential concept known as "flipping the metabolic switch" 108.
According to this framework, the human body is evolutionarily adapted to function optimally in environments where food is scarce. Many animals in the wild, as well as ancient human hunter-gatherers, regularly experienced extended periods with little or no food 1213. Under a modern, continuous eating pattern - where an individual consumes meals and snacks from early morning until late at night - the body relies almost exclusively on glucose derived from carbohydrates for energy 12. Any excess glucose is stored in the liver as glycogen or converted to adipose tissue (body fat).
Transitioning from Glucose to Ketones
The "metabolic switch" represents the physiological shift that occurs when the body exhausts its liver glycogen stores and is forced to tap into fat reserves for fuel 813. This process typically begins 12 to 36 hours after the cessation of food intake, depending heavily on an individual's baseline liver glycogen content and their amount of energy expenditure or exercise during the fast 813.
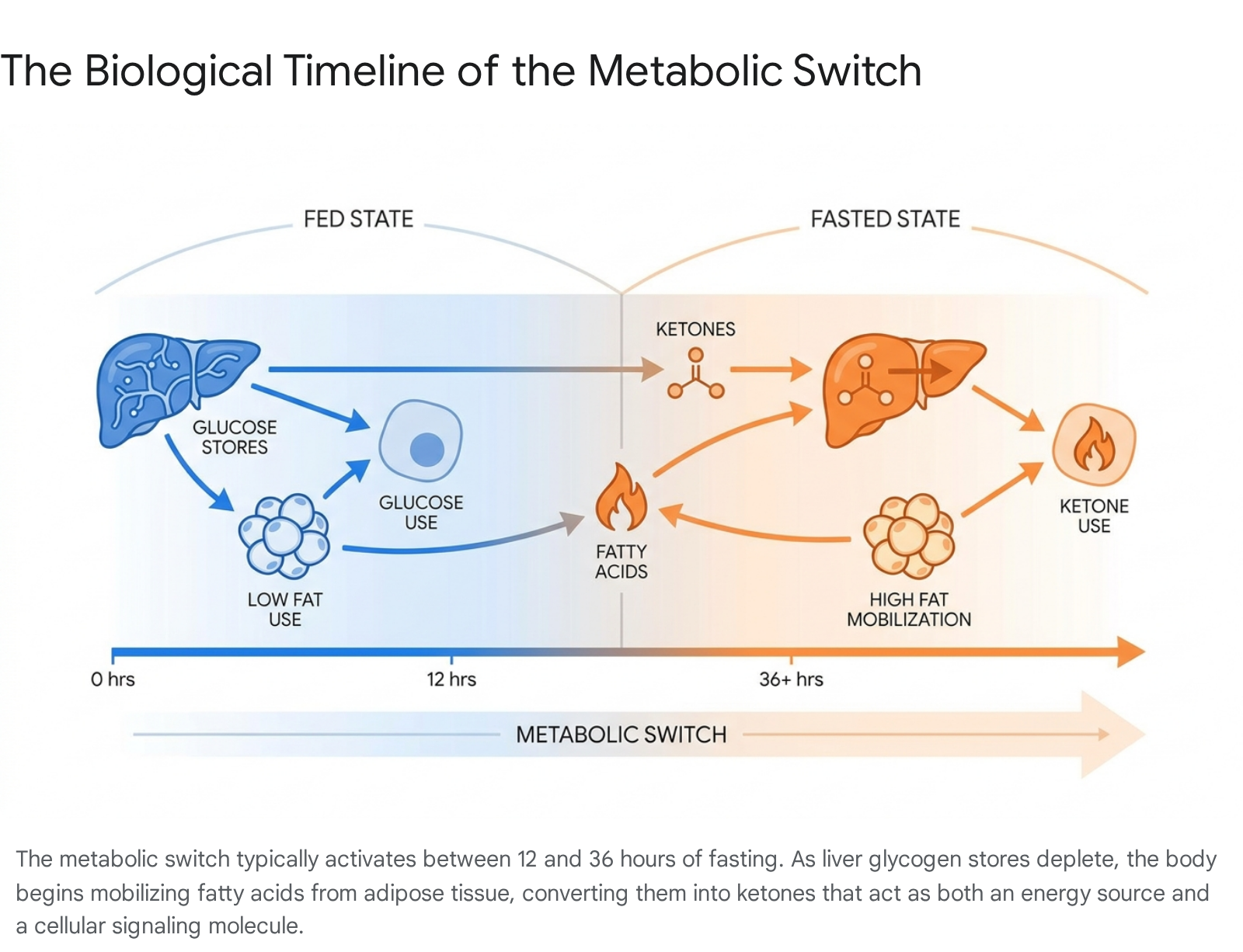
When the switch flips, accelerated adipose tissue lipolysis releases free fatty acids and glycerol into the bloodstream. These fatty acids travel to the liver, where they are converted into ketones (such as beta-hydroxybutyrate) 1213.
Triggering Cellular Survival Pathways
Ketones are not merely an alternative fuel source; they are potent signaling molecules. Mattson and other researchers theorized that these ketones trigger a cascade of cellular "survival pathways" that evolved to protect organisms during times of scarcity 812. These pathways include: * Autophagy: A cellular recycling and cleanup process where cells clear out damaged proteins and dysfunctional mitochondria 1213. * Reduced Systemic Inflammation: The suppression of inflammatory markers that are heavily linked to chronic diseases, including cardiovascular disease and metabolic syndrome 812. * Improved Insulin Sensitivity: A resensitization of cellular insulin receptors due to the prolonged absence of dietary glucose, helping to stabilize blood sugar 812.
The biological theory is elegant and well-supported by pre-clinical animal models 89. However, as researchers moved from testing rodents in controlled laboratories to testing complex humans in the real world, a critical question emerged: Do these profound cellular mechanisms translate into clinically meaningful weight loss and metabolic improvements over the long term, or does a standard daily diet with a slight calorie deficit achieve the exact same result?
Analyzing the Core Fasting Protocols
Before diving into the clinical trial results, it is necessary to distinguish between the various forms of intermittent fasting. The term itself is an umbrella phrase that encompasses several distinct behavioral dietary patterns. The clinical trials reveal that not all protocols perform equally when subjected to rigorous testing.
Comparing the Major Intermittent Fasting Methods
When assessing the literature, researchers generally divide intermittent fasting into three broad categories: time-restricted eating, alternate-day fasting, and periodic (whole-day) fasting 11011.
| Fasting Protocol | Clinical Description | Typical Application |
|---|---|---|
| Time-Restricted Eating (TRE) | Limiting daily food intake to a specific window of hours, followed by a prolonged daily fast. | The popular 16:8 method, where all calories are consumed within an 8-hour window (e.g., 10 a.m. to 6 p.m.), followed by a 16-hour fast 11012. |
| Alternate-Day Fasting (ADF) | Alternating days of normal, unrestricted eating with days where caloric intake is severely reduced or entirely eliminated. | A 24-hour complete fast every other day, or a "modified" ADF where patients consume roughly 25-30% of their daily energy expenditure (approx. 500 calories) on fasting days 11013. |
| Periodic / Whole-Day Fasting | Eating normally for the majority of the week, with severe caloric restriction on specific, non-consecutive days. | The 5:2 diet (five days of normal eating, two days of fasting) or the 4:3 diet (four days of normal eating, three days of fasting) 11415. |
Understanding these distinctions is paramount because the physiological stress - and the likelihood of triggering Mattson's "metabolic switch" - varies wildly between a 16-hour daily fast and a full 24-hour fast.
What the Latest Landmark Trials Reveal About Weight Loss
For years, the fasting debate lacked appropriately powered, long-term clinical trials. Conventional dietitians argued that weight loss from fasting was simply the result of calorie math - eating for only eight hours a day naturally leads people to consume less food. Fasting advocates argued the metabolic changes caused greater fat loss and better health outcomes than equivalent calorie reduction.
Between 2024 and 2026, the scientific community delivered a definitive, data-driven answer.
The 2025 BMJ Network Meta-Analysis
The most comprehensive evaluation of the evidence to date was published in The BMJ in June 2025 by a collaborative team of researchers from Harvard University and the University of Toronto 161723. The authors conducted a systematic review and network meta-analysis, pooling data from 99 randomized clinical trials involving a total of 6,582 adults 11819.
A network meta-analysis is a highly rigorous statistical tool that allows researchers to compare multiple interventions simultaneously, both directly against one another and indirectly across the full spectrum of the literature 1126. The participants in these trials had an average body mass index (BMI) of 31, and nearly 90% lived with existing health conditions such as type 2 diabetes, metabolic syndrome, or metabolic dysfunction-associated steatotic liver disease 161820.
The primary finding was sobering for fasting purists: all forms of intermittent fasting and continuous energy restriction resulted in similar, small reductions in body weight when compared to an unrestricted, ad-libitum diet 118.
However, the analysis uncovered one notable exception among the fasting protocols. Alternate-day fasting (ADF) was the only intermittent fasting strategy to show a statistically significant benefit in body weight reduction when directly compared to continuous daily calorie restriction 11819. On average, ADF yielded an additional weight loss of 1.29 kilograms (about 2.8 pounds) over standard calorie counting 118.
Alternate-day fasting also slightly outperformed other fasting methods in head-to-head indirect comparisons, beating 16:8 time-restricted eating by an average of 1.69 kg, and outperforming whole-day (5:2) fasting by 1.05 kg 11819.
Despite these statistical victories, the authors noted several crucial clinical caveats. First, an additional 1.29 kg of weight loss does not meet the standard medical threshold of a 2-kilogram difference required to be considered "clinically significant" for individuals managing obesity 121. Second, the distinct advantages of alternate-day fasting largely disappeared in trials that lasted longer than 24 weeks, suggesting that the body metabolically adapts to the regimen over time, or that patient adherence wanes 1118.
When looking beyond weight at secondary cardiometabolic markers, the BMJ analysis found that ADF resulted in trivial-to-moderate improvements in total cholesterol and LDL ("bad") cholesterol compared to time-restricted eating 11829. However, there were no significant differences noted between any of the intermittent fasting diets and continuous energy restriction for HbA1c (a key marker of long-term blood sugar control) or HDL ("good") cholesterol 1118.
The 2026 Cochrane Systematic Review
The findings of the BMJ network meta-analysis were heavily reinforced early the following year. In February 2026, the Cochrane Library - widely considered the absolute gold standard for evaluating evidence-based medicine - published a systematic review of 22 randomized controlled trials involving nearly 2,000 participants across North America, Europe, Australia, and Asia 2223.
The Cochrane review compared various forms of intermittent fasting (including time-restricted eating, alternate-day fasting, and the 5:2 approach) against conventional calorie-counting diets. The interventions ranged from four weeks to six months, with follow-ups extending to a year 23.
The verdict was definitive. Across the 21 studies involving 1,430 people that directly compared intermittent fasting and conventional diets, the difference in weight loss between the two approaches was a mere 0.33 percentage points of total body weight 22. Diane Rigassio Radler, clinical nutrition professor at Rutgers School of Health Professions and co-author of the review, noted that the differences between the diets were "statistically indistinguishable from zero" 22.
Furthermore, both methods resulted in nearly identical outcomes regarding patient quality of life and adverse events 22. When researchers pooled the data for participants who achieved a clinically meaningful 5% total body weight reduction, the success rates were virtually identical across both the fasting and calorie-counting groups 2223.
"From the results of this review, it doesn't look like intermittent fasting is any better than regular dietary advice," Radler concluded 23. The authors did note that the evidence base still has gaps; none of the 22 studies reported on long-term diabetes outcomes, and none lasted longer than a single year 22.
The 4:3 Anomaly: A Breakthrough in Diet Adherence
While the broad meta-analyses point strongly toward physiological equivalence, one specific, highly controlled trial from 2025 highlights the exact area where intermittent fasting may genuinely shine: behavioral adherence and psychological sustainability.
Published in the Annals of Internal Medicine, a randomized clinical trial led by researchers at the University of Colorado Anschutz Medical Campus tracked 165 adults with overweight or obesity over a 12-month period 224. The trial sought to compare a standard 34.3% daily calorie restriction against a "4:3" intermittent fasting protocol 22425.
In the 4:3 group, participants underwent a modified fast, restricting their energy intake by 80% on three non-consecutive days per week. On the remaining four days, they were allowed to eat ad libitum (without any caloric restriction), though they were encouraged to make generally healthy food choices 2425. Crucially, the researchers meticulously designed the trial so that the total weekly energy deficit was intended to be identical between both groups 224. Furthermore, both groups were provided with a high-intensity, guidelines-based behavioral weight loss program, comprehensive group support, and a free gym membership with instructions to exercise for 300 minutes per week, normalizing environmental and educational variables 141524.
At the 12-month mark, the results were highly compelling. The 4:3 intermittent fasting group lost an average of 7.6% of their body weight, compared to a 5.0% reduction in the daily calorie restriction group 22426. Even more telling was the clinical success rate: 58% of the fasters achieved the vital benchmark of at least a 5% baseline weight loss, compared to only 47% of the continuous calorie counters 22526. Furthermore, the fasting group demonstrated more favorable changes in cardiometabolic outcomes, including systolic blood pressure, fasting glucose levels, and LDL cholesterol 2526.
Why Behavioral Fatigue Matters
If the weekly prescribed calorie deficits were identical, why did the 4:3 fasting protocol work so much better?
The researchers utilized advanced isotope tracking to measure actual energy expenditure and intake via urine samples 2. They discovered that despite the intended parity, the 4:3 group unintentionally ate less overall over the course of the year 215. Because the fasting group did not have to suffer the psychological fatigue of counting, weighing, and restricting calories every single day, their adherence to the diet was significantly higher 2.
The trial data explicitly highlights this psychological advantage: the dropout rate for participants in the 4:3 fasting group was only 19%, while the daily caloric restriction group suffered a significantly higher dropout rate of 30% over the 12-month trial.
This trial underscores an emerging clinical consensus regarding intermittent fasting. It may not alter the fundamental thermodynamics of weight loss, but it operates as highly effective behavioral psychology 2. For a significant subset of patients, enduring severe restriction a few days a week is vastly easier, and more sustainable, than enduring mild, persistent hunger every single day 22526.
Does Fasting Offer Unique Metabolic Benefits Beyond Weight Loss?
While weight loss is the primary reason most people adopt a fasting regimen, researchers have intensely investigated whether the act of flipping the "metabolic switch" produces health benefits independent of shedding pounds. If a person maintains their exact body weight, does intermittent fasting still heal a broken metabolism?
The Insulin Sensitivity Argument
For a time, there was genuine hope that fasting uniquely impacted insulin dynamics. A 2024 systematic review and meta-analysis published in the journal Nutrients aggregated data from 10 randomized controlled trials encompassing 623 adults with obesity 13.
The analysis found that while fasting-based strategies and continuous caloric restriction both resulted in identical weight loss at the six-month mark (between 5.5 and 6.5 kg), the fasting groups demonstrated statistically superior improvements in insulin sensitivity 1326. Fasting insulin levels dropped by a significant 7.46 pmol/L more in the fasting cohort, and HOMA-IR scores (the standard clinical measure for insulin resistance) fell slightly further than in the continuous restriction group 1326.
Similarly, a separate 2024 meta-analysis specifically examined trials where total caloric intake was held entirely equal between the two diet groups, purposefully stripping out weight loss as a confounding variable. That study reported that intermittent fasting still produced greater long-term reductions in fasting insulin, waist circumference, and inflammatory markers like IL-6 26.
The ChronoFast Trial: Debunking the Timing Myth
Fasting enthusiasts frequently point to these isolated insulin reductions as proof that manipulating eating windows inherently heals metabolism. However, a landmark 2026 study published in Science Translational Medicine challenged this assumption with unprecedented rigor.
Led by Professor Olga Ramich at the German Institute of Human Nutrition, the "ChronoFast" trial sought to permanently decouple the variables of meal timing from calorie quantity 23527. A major flaw in previous real-world fasting research is the "unintentional calorie deficit"; when people restrict their eating to an eight-hour window, they naturally skip late-night snacks or morning pastries, thereby eating fewer calories 35.
To isolate the effect of timing alone, the ChronoFast team utilized a highly controlled, randomized crossover design with 31 women managing overweight or obesity 23527. Participants underwent a two-week period of early time-restricted eating (eTRE, eating from 8 a.m. to 4 p.m.) and a later schedule (lTRE, from 1 p.m. to 9 p.m.) 23527.
Crucially, the researchers provided the meals, perfectly matching every single calorie and nutrient across both phases, entirely removing energy intake as a variable 227. They tracked the participants using motion sensors, continuous glucose monitoring, and a specialized "BodyTime" blood assay to assess circadian clocks 2.
The results were unequivocal. When calorie intake remained absolutely identical, an eight-hour eating window provided no measurable boost to metabolism, insulin sensitivity, blood sugar control, blood fats, or inflammatory markers 928. "Our results suggest that the health benefits observed in earlier studies were likely due to unintended calorie reduction, rather than the shortened eating period itself," Professor Ramich concluded 92728.
The only physiological metric that actually changed during the ChronoFast trial was the body's circadian clock, which shifted backward by an average of 40 minutes during the late eating schedule, influencing sleep timing but failing to move the needle on metabolic health 2728.
This finding is heavily supported by other rigorous literature, including the landmark 12-month TREATY trial published in the New England Journal of Medicine in 2022, which found that time-restricted eating combined with calorie restriction produced the exact same reductions in visceral fat, body fat, liver fat, and blood pressure as calorie restriction alone 11263839.
The scientific reality is straightforward: if a patient does not reduce their overall caloric intake, an eating window provides virtually no metabolic rescue 935.
The Cardiovascular Controversy: Is Fasting Dangerous?
In March 2024, intermittent fasting dominated global headlines for a very different reason: a preliminary study suggested the practice might be lethal.
Presented at the American Heart Association's Epidemiology and Prevention Scientific Sessions in Chicago, a research poster led by Dr. Victor Wenze Zhong of the Shanghai Jiao Tong University School of Medicine analyzed data from over 20,000 U.S. adults 122930. The analysis reviewed dietary patterns from the National Health and Nutrition Examination Surveys (NHANES) collected between 2003 and 2018, and cross-referenced those patterns with the CDC's National Death Index through December 2019 2931.
The headline finding was staggering. Individuals who restricted their daily eating to less than eight hours per day (adhering to a classic 16:8 fasting schedule) had a 91% higher risk of death due to cardiovascular disease over a median follow-up of eight years, compared to those eating across a standard 12-to-16-hour window 294432.
The increased risk of cardiovascular death was especially pronounced in people already living with heart disease or cancer 2933. Furthermore, the analysis found that an eight-hour eating window did not reduce the overall risk of death from any cause whatsoever 2934.
Dr. Zhong hypothesized that the severe restriction window might lead to a loss of lean muscle mass, noting that "loss of lean body mass has been linked to a higher risk of cardiovascular mortality" 35.
Contextualizing the 91% Statistic and Methodological Flaws
While the 91% statistic sounded profoundly alarming to the general public, the broader scientific and medical community urged severe caution in interpreting the results, pointing out several glaring methodological limitations with the study 36:
- Observational, Not Causal: The study identified a correlation, not causation. It is highly possible that individuals adopting an extreme 8-hour eating window in the early 2000s and 2010s were already dealing with preexisting metabolic disorders, severe obesity, or health anxieties. They may have adopted fasting as a desperate measure to manage poor health, making them statistically more likely to suffer cardiovascular events later in life (a classic epidemiological phenomenon known as reverse causality) 30.
- Extremely Weak Dietary Tracking: Categorization into an eating window was based entirely on self-reported dietary recall from just two days of the NHANES survey 50. Relying on two days of self-reported memory to accurately represent a patient's habitual dietary lifestyle over an eight-year follow-up period is notoriously unreliable and highly susceptible to recall bias .
- Lack of Diet Quality Control: The analysis did not control for the nutritional quality of the food consumed. A participant eating ultra-processed fast food for eight hours was grouped with someone eating a pristine Mediterranean diet . Furthermore, it failed to factor in critical confounding lifestyle variables such as smoking status, alcohol consumption, shift work, baseline stress, and exercise routines 30.
- Non-Peer-Reviewed: At the time of the global media cycle, the research was presented only as an abstract poster at a conference. It had not yet passed the rigorous threshold of peer-reviewed publication in a scientific journal, meaning the underlying data had not been scrutinized by independent experts 2936.
As Dr. Kenneth Mukamal, a primary care doctor and professor at Harvard Medical School, noted regarding the AHA presentation: "At first glance, it does not suggest this is likely to be of cardiovascular benefit and indeed it was harmful. But there could be health reasons to eat in a time-restricted manner that would make this appear harmful, when it's not... If people want to eat over a shorter duration and it's easier for them to maintain their weight that way, I would not use this as a reason not to do it" 30.
The current clinical consensus remains that while the AHA data warrants further long-term study, it does not override the established safety and efficacy data generated by dozens of tightly controlled, peer-reviewed RCTs over the last several years.
The Synergistic Role of Diet Quality
Ultimately, the most sophisticated fasting schedule cannot rescue a patient from a fundamentally poor diet. Intermittent fasting modulates when you eat, but the foundation of metabolic health remains firmly rooted in what you eat.
A 2025 trial published in Nature Medicine by researchers at the NIH and the University of Granada illustrated this synergy perfectly. The study placed 197 adults with obesity on a high-quality, nutrient-dense Mediterranean diet 37. One group consumed the Mediterranean diet throughout the day, while other groups were instructed to restrict the exact same Mediterranean diet to various 8-hour windows (morning, afternoon, or self-selected) 37.
The researchers found that participants who engaged in the time-restricted eating schedules experienced excellent weight loss and significant improvements in cardiovascular and metabolic health 37. However, the most important finding was behavioral: the participants who restricted their eating windows adhered to the highly nutritious Mediterranean protocol much more faithfully than the unrestricted control group 37.
Dietary interventions targeting whole, minimally processed plant-based foods, lean proteins, omega-3 fatty acids, and fiber demonstrate immense potential for preventing or reversing metabolic abnormalities such as dyslipidemia and chronic inflammation 3. Whether a patient chooses a 16:8 time-restricted window, a 4:3 alternate schedule, or simply cuts their daily caloric intake by 20%, the non-negotiable variable is nutritional quality. A fasting protocol built on ultra-processed, energy-dense foods during the eating windows will inevitably fail to improve cardiovascular-kidney-metabolic health.
Bottom line
The highest quality clinical evidence from 2024 through 2026 confirms that intermittent fasting and continuous calorie restriction are equally effective for achieving weight loss and improving cardiometabolic health. Fasting does not appear to possess "magical" metabolic properties; rigorous trials matching exact calorie intake reveal that eating windows alone do not improve insulin resistance, blood sugar, or lipid profiles independent of a caloric deficit. However, fasting remains an incredibly powerful behavioral tool. Protocols like alternate-day fasting and 4:3 schedules have been shown to significantly reduce diet fatigue and lower trial dropout rates, helping patients successfully maintain the calorie deficit required to reverse metabolic disease over the long term.