Is Intermittent Fasting Better Than Calorie Restriction
For weight loss and overall cardiometabolic health, both intermittent fasting and continuous calorie restriction are highly effective, producing nearly identical long-term results for the average person. While certain fasting schedules like alternate-day fasting may provide a slight short-term edge in fat loss and insulin sensitivity, the primary driver of success in both diets is a sustained caloric deficit. Ultimately, the superior approach is whichever eating pattern fits your lifestyle, minimizes your hunger, and allows you to adhere to a lower energy intake over time.
The Global Obesity Challenge and the Diet Debate
According to the World Health Organization's 2022 data, approximately 2.5 billion adults - 43% of the global adult population - were classified as overweight, and about 890 million lived with clinical obesity 12. This epidemic carries a staggering economic and physiological burden, dramatically increasing the risk of type 2 diabetes, cardiovascular disease, hypertension, and metabolic dysfunction-associated steatotic liver disease (MASLD) 134. The traditional medical response to this crisis has been continuous energy restriction (CER), commonly known as daily calorie counting. While mathematically sound, daily restriction requires constant vigilance, leading to "diet fatigue," metabolic adaptation, and notoriously poor long-term adherence 456.
In response, intermittent fasting (IF) or intermittent energy restriction (IER) has surged in popularity. Fasting shifts the focus from what or how much you eat to when you eat. Proponents of fasting have long argued that abstaining from food for extended periods triggers unique biological mechanisms - such as cellular repair and metabolic switching from glucose to fat - that make it inherently superior to traditional dieting 79. Conventional nutritionists counter that fasting is merely a behavioral trick to achieve the same caloric deficit.
Thanks to a wave of gold-standard randomized controlled trials (RCTs) and extensive network meta-analyses published between 2022 and 2026, the scientific community finally has the data to settle the debate. The evidence reveals a nuanced reality: fasting is a highly effective tool with some unique metabolic advantages, but it is not a biological magic trick that overrides the laws of energy balance.
Defining the Dietary Approaches
To understand the research, it is crucial to recognize that "intermittent fasting" is a broad umbrella term encompassing several vastly different protocols 178. The metabolic and psychological impacts vary heavily depending on the specific method utilized.
Time-Restricted Eating (TRE)
Time-restricted eating confines daily caloric intake to a specific window, typically ranging from four to ten hours, with the remainder of the day spent fasting 8910. The most popular iteration is the 16:8 method, which involves fasting for 16 hours and consuming all meals within an 8-hour window 2713. Unlike other methods, TRE does not explicitly mandate a reduction in calories, though a deficit naturally occurs for most people simply because they have less time to eat.
Alternate-Day Fasting (ADF)
Alternate-day fasting involves alternating between "feast days" of normal, unrestricted eating and "fast days" where caloric intake is severely restricted or eliminated entirely 7910. In modified alternate-day fasting (MADF), participants consume roughly 20% to 30% of their baseline energy needs (usually around 500 calories) on fasting days 8.
Periodic or Whole-Day Fasting (5:2 and 4:3)
Periodic fasting schedules structure the week into distinct blocks. The 5:2 diet involves five days of unrestricted eating and two non-consecutive days of severe calorie restriction (typically 500 to 600 calories) 1014. The 4:3 approach escalates this to three non-consecutive fasting days per week 711.
Continuous Energy Restriction (CER)
The traditional benchmark, continuous energy restriction (also referred to as daily caloric restriction or DCR), requires a consistent, moderate reduction in daily caloric intake - typically a deficit of 500 to 750 calories per day, or roughly 20% to 30% of total daily energy expenditure 616.
The Weight Loss Showdown: What the Data Shows
For years, human trials comparing IF to CER were small, short-term, or poorly controlled. Between 2022 and 2025, researchers executed massive, rigorously controlled trials designed to isolate the variables of meal timing and total calories.
The 2025 BMJ Network Meta-Analysis
In June 2025, researchers from Harvard University and the University of Toronto published one of the most comprehensive evaluations of fasting to date in The BMJ 713. The network meta-analysis pooled data from 99 randomized clinical trials involving 6,582 adults 21312. This advanced statistical method allowed researchers to compare different fasting strategies both directly against continuous energy restriction and indirectly against each other.
The headline finding challenged popular assumptions: time-restricted eating (like 16:8) and whole-day fasting (like 5:2) did not produce significantly greater weight loss than standard daily calorie counting 2713. Both IF and CER successfully reduced body weight compared to an unrestricted diet, with participants losing an average of 1.7 to 2.5 kg more than control groups 13.
However, alternate-day fasting (ADF) stood out as the sole fasting strategy to show a statistically significant advantage over continuous energy restriction 212. ADF resulted in a mean difference of an additional 1.29 kg of weight loss compared to CER 212. ADF also outperformed time-restricted eating by 1.69 kg and whole-day fasting by 1.05 kg 2. While statistically significant, the researchers noted that an additional 1.29 kg is a modest clinical benefit, falling short of the 2.0 kg threshold defined as a "minimally important clinical difference" for obesity management 12.
Crucially, the timing of the trials mattered. The slight edge observed in fasting interventions was primarily seen in short-term studies lasting less than six months. When researchers looked strictly at long-term trials spanning 24 weeks or more, the weight-loss benefits between fasting strategies and continuous restriction entirely equalized 21213. Over the long run, metabolic adaptation and adherence fatigue level the playing field.
Isocaloric Testing: When Calories Are Equal
To determine if meal timing possesses intrinsic weight-loss properties independent of calorie math, researchers utilize "isocaloric" trials. In these studies, participants in both the fasting group and the daily restriction group are forced to consume the exact same number of calories.
The landmark TREATY trial, published in the New England Journal of Medicine in April 2022, applied this methodology to time-restricted eating. Researchers randomized 139 adults with obesity to a 25% caloric deficit for 12 months. One group ate exclusively between 8:00 a.m. and 4:00 p.m., while the control group spread the same 25% deficit throughout the day. At the end of the year, the TRE group lost 8.0 kg and the daily restriction group lost 6.3 kg 7. While the fasting group lost slightly more, the difference was not statistically significant. The trial demonstrated that when calories are matched, compressing the eating window does not magically accelerate fat loss 7.
This was reinforced by the 2026 ChronoFast study out of Germany. Researchers tested a time-restricted eating window without asking participants to cut calories at all. The results were definitive: without an energy deficit, an eight-hour eating window failed to improve insulin sensitivity, cardiovascular markers, or body weight 14. The meal timing did successfully shift the participants' internal circadian clocks, but calorie reduction remained the essential driver of metabolic health 14.
The 4:3 Fasting Trial and Behavioral Adherence
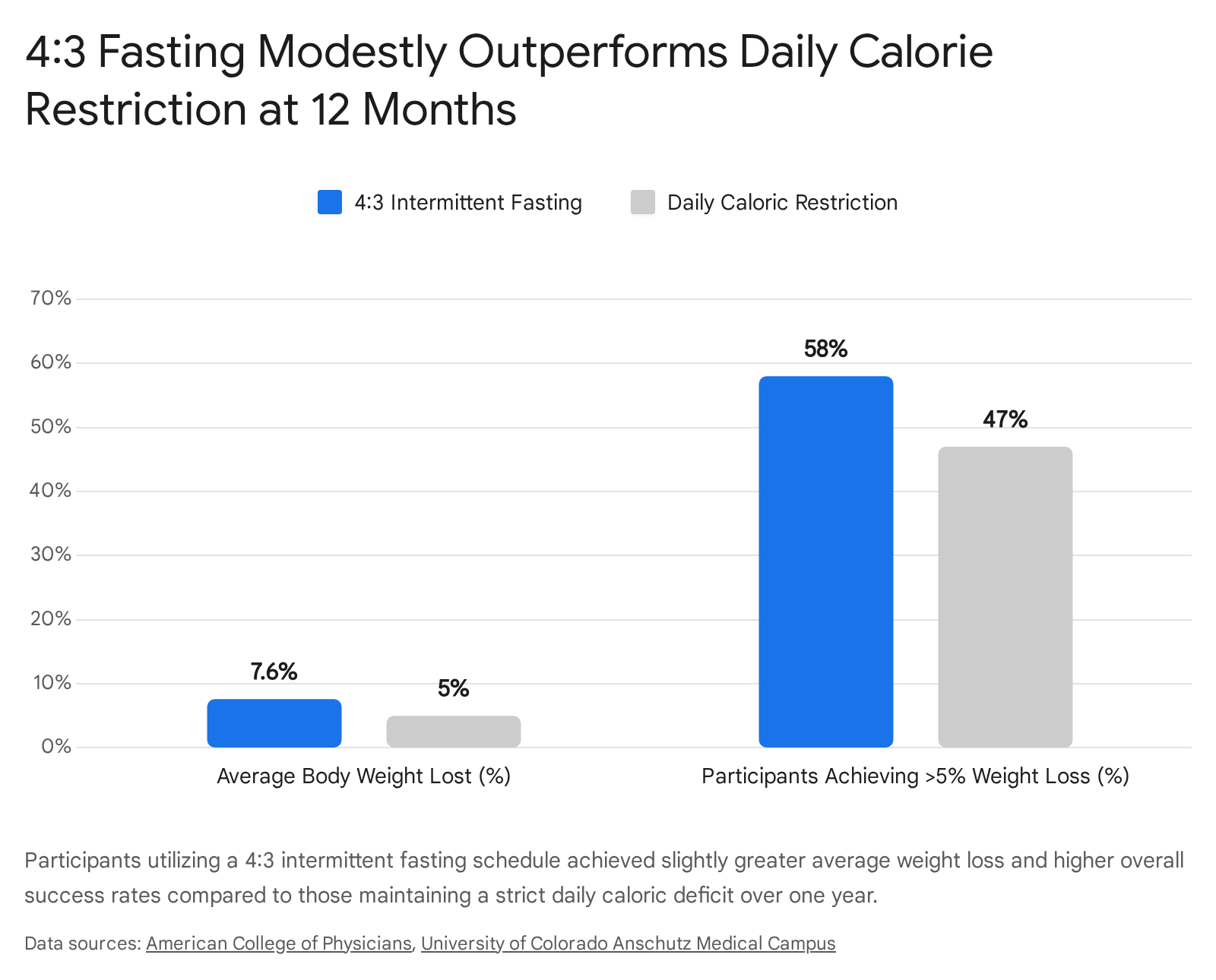
While time-restricted eating appears to be primarily a vehicle for calorie reduction, periodic fasting protocols like the 4:3 diet may offer distinct behavioral advantages. A highly cited 2025 randomized clinical trial published in the Annals of Internal Medicine evaluated 165 adults with overweight or obesity over a 12-month period 71120.
Researchers engineered the interventions so that both groups achieved the same 34% weekly energy deficit. The daily restriction group cut calories by 34% every single day. The intermittent fasting group followed a 4:3 protocol, severely restricting intake to just 20% of baseline calories (roughly 400 to 700 calories) on three non-consecutive days per week, and eating without restrictions on the remaining four days 711. Both groups received comprehensive behavioral support and a prescription for 300 minutes of weekly aerobic activity 112015.
The results demonstrated a statistically significant advantage for the 4:3 group. At 12 months, participants in the fasting group recorded an average body weight loss of 7.6%, compared to 5.0% in the daily restriction group 1120. Furthermore, 58% of the fasting cohort achieved a clinically meaningful weight loss of at least 5%, compared to 47% of the daily restriction cohort 20.
When examining why the fasting group succeeded, researchers turned to psychological surveys. Over the course of the year, binge eating and uncontrolled eating scores decreased significantly in the 4:3 fasting group but actually increased in the continuous restriction group 15. Improvements in cognitive restraint and emotional eating were strongly correlated with greater weight loss in the fasting group 15. For many individuals, the psychological reprieve of eating normally four days a week makes a severe deficit on the remaining three days much easier to tolerate than the unending vigilance required by daily calorie counting 14.
Does Fasting Improve Insulin Resistance?
While the weight loss differences between IF and CER are generally modest, intermittent fasting appears to possess a genuine, defensible advantage when it comes to glucose metabolism and insulin sensitivity.
Insulin is a hormone produced by the pancreas that acts as a key, unlocking cells so that glucose from the bloodstream can enter and be used for energy 2223. In individuals with obesity or type 2 diabetes, cells become resistant to this process. Using a common medical analogy, the cellular "lock" becomes rusty and jammed; the key is present, but it struggles to turn 23. When an individual eats continuously throughout the day, the pancreas must constantly secrete insulin to deal with incoming glucose, keeping the body in a state of high insulin circulation.
Intermittent fasting provides the body with a prolonged physiological break from insulin secretion. This fasting window appears to allow cellular receptors to resensitize to the hormone more effectively than simply eating smaller meals around the clock.
Multiple 2024 meta-analyses confirm this metabolic edge. A systematic review of 10 randomized trials published in Nutrients found that while short-term weight loss was similar between IF and CER, fasting groups exhibited distinct, statistically significant improvements in insulin sensitivity 79. Fasting insulin dropped by 7.46 pmol/L more in the fasting groups, and HOMA-IR (Homeostatic Model Assessment for Insulin Resistance, the standard clinical metric) fell significantly further compared to continuous restriction 79.
A second 2024 meta-analysis published in Nutrition, Metabolism and Cardiovascular Diseases isolated trials where calories were held exactly equal between the groups, purposefully stripping out weight loss as a confounding variable. Even with identical caloric intake, intermittent fasting produced greater long-term reductions in fasting insulin and HOMA-IR 716.
Cardiovascular and Metabolic Biomarkers
Beyond insulin, both intermittent fasting and daily caloric restriction are remarkably effective at improving broader cardiovascular risk factors. The following table synthesizes findings from recent network meta-analyses regarding their impact on specific health markers.
| Cardiometabolic Marker | Efficacy of Intermittent Fasting (IF) | Efficacy of Daily Caloric Restriction (CR) | Comparative Advantage |
|---|---|---|---|
| Systolic Blood Pressure (SBP) | High. Network meta-analysis shows ADF reduces SBP by up to 7.24 mmHg 26. | High. Consistently lowers BP across populations 727. | Tie. Both drive improvements largely tied to weight loss, though specific IF trials show slight superiority 1317. |
| Triglycerides | Moderate to High. ADF and 5:2 protocols show significant reductions 2729. | High. Isocaloric analysis indicates CR groups often report better long-term triglyceride outcomes 716. | CR. Slight edge in long-term isocaloric environments 716. |
| LDL "Bad" Cholesterol | Moderate. ADF linked to lower total and LDL cholesterol 2. | Moderate. Reliable reductions alongside fat mass loss 729. | Tie. Neither strategy shows overwhelming superiority for lipid panels 1729. |
| Visceral / Fat Mass | High. Modest advantages in fat-free mass preservation in some short-term studies 426. | High. Strong, predictable reductions tied to energy deficit 16. | IF. Slight isocaloric advantage for waist circumference and fat mass percentage 716. |
| Systemic Inflammation | High. Shows specific reductions in markers like Interleukin-6 (IL-6) 716. | Moderate. Reduces inflammation as adiposity decreases 18. | IF. Accelerated reduction in oxidative stress and inflammatory cytokines 1618. |
Liver Health: Reversing Fatty Liver Disease
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease, is a major complication of obesity 19. Caloric restriction is a first-line treatment, but adherence is notoriously poor.
Recent clinical trials suggest intermittent fasting is a highly viable alternative. A 12-week randomized trial comparing intermittent calorie restriction (a 5:2 diet utilizing 500 calories on fast days) against continuous restriction in 60 adults with MASLD found striking improvements in both groups. The fasting group saw a mean reduction in liver fat content (LFC) of 20.5%, compared to 15.5% in the continuous restriction group 19. While the 5% difference was not statistically significant between the groups, it demonstrated that IF is equally potent for liver de-fatting 19.
Another 2024 trial evaluating the 5:2 diet specifically noted that fasting significantly decreased the proportion of patients with moderate-to-severe hepatic steatosis and fibrosis compared to daily restriction, suggesting that fasting may improve liver stiffness and fibrosis independently of pure weight regulation 5.
Hormonal Impacts: Hunger, Satiety, and Stress
While fasting scores well on insulin and liver health, it is not without physiological drawbacks. When comparing the two diets, one of the most critical factors for long-term success is how the body manages hunger hormones like ghrelin (which signals hunger) and leptin (which signals satiety) 1520.
In the 12-month 4:3 fasting trial, researchers measured fasting levels of leptin, ghrelin, and brain-derived neurotrophic factor (BDNF). They found absolutely no between-group differences in fasting appetite-related hormones at any time point during the year 15. Both groups experienced the expected hormonal adaptations to weight loss - leptin dropped as fat mass decreased - but fasting did not uniquely "hack" the hunger hormones 15.
In fact, continuous caloric restriction frequently wins when measuring subjective well-being. The 2025 isocaloric meta-analysis published in Nutrition, Metabolism and Cardiovascular Diseases revealed that participants in continuous restriction groups reported significantly lower levels of hunger and fatigue compared to those in fasting groups 716.
For individuals with physically demanding jobs, active athletic training schedules, or those prone to severe blood sugar crashes, the sustained energy provided by daily caloric restriction is a major advantage. Extended fasting spikes cortisol and can trigger dizziness or lethargy, making standard dieting a more comfortable baseline for many 71620.
Autophagy: The Cellular Recycling Program
If you dive into the literature surrounding intermittent fasting, you will inevitably encounter the concept of autophagy. The word translates from Greek as "self-eating," and it represents one of the body's most critical self-preservation mechanisms 2122.
To understand autophagy without a biology degree, medical educators frequently use a bakery analogy 2336. Imagine running a bustling bakery that possesses no trash cans. At the end of the day, you have a massive pile of leftover ingredients, stale pastries, and damaged goods. You have two options. You could grind all the waste up and attempt to flush it down the plumbing, which is inefficient and places immense stress on the building's infrastructure. Or, you could get creative and recycle. You take the old bananas meant for yesterday's dessert and mash them into today's banana bread. You take the stale sourdough loaves and bake them into croutons 2336.
Autophagy is the cellular equivalent of getting creative. Over time, human cells accumulate damaged proteins, dysfunctional mitochondria, and cellular junk 2122. When the body is deprived of external nutrients - such as during a fast - it senses a state of energetic stress. To survive, cells act like the resourceful baker. They gather up the internal debris, wrap it in a microscopic garbage bag called an autophagosome, and fuse it with a lysosome, which acts as a cellular recycling center. The junk is broken down into its constituent amino acids and repurposed to build fresh, healthy cellular structures 2223.
Spermidine, Gut Health, and Aging
Autophagy is heavily implicated in anti-aging, longevity, and defense against neurodegenerative diseases like Alzheimer's and Parkinson's 212237. Animal research demonstrates that intermittent fasting significantly elevates cellular levels of spermidine, a compound that acts as a valiant defender against cellular aging and vigorously promotes autophagic activity 38.
Furthermore, aging naturally degrades the intestinal barrier, leading to a "leaky gut" that allows harmful substances into the bloodstream, triggering systemic, low-grade inflammation (often termed "inflammaging") 39. A 2025 study published in Aging Cell demonstrated that short-term, alternate-day fasting successfully reversed leaky gut in aged mice by restoring the mitochondrial function and regenerative capacity of intestinal stem cells (ISCs) 39. Fasting provides the digestive tract with a crucial period of rest, allowing the intestinal lining to repair itself from the constant barrage of digestive enzymes 39.
Is Autophagy Unique to Fasting?
Many fasting proponents argue that autophagy is the magic bullet that proves fasting is biologically superior to standard dieting. However, human clinical reality is more complex.
While fasting for 12 to 16 hours is a highly reliable way to force the body to switch from glucose metabolism to fat metabolism - thereby triggering protein synthesis regulation and autophagy - it is not the only way 840. The scientific consensus in 2024 and 2025 confirms that caloric restriction also stimulates autophagy 1824.
Any state of sustained energy deficit places stress on the cells, forcing them to increase autophagic flux to conserve resources. Whether that deficit is achieved by skipping breakfast (time-restricted eating) or simply eating 25% less at every meal (continuous restriction), the body will engage its cellular recycling program 18. While prolonged, multi-day fasts may induce deeper states of autophagy, excessive autophagic response can actually become harmful, potentially stimulating autophagic cell death 24. For general health and weight loss, both IF and CR leverage this biological pathway effectively.
Preserving Muscle Mass and Exercise Performance
A common fear regarding weight loss - and fasting in particular - is the loss of metabolically active muscle tissue (sarcopenia). When the body lacks calories, it can break down muscle protein alongside body fat to meet energy demands.
However, recent data indicates that both IF and CR can be safely paired with exercise without disastrous impacts on performance. A 2025 meta-analysis of 35 randomized trials involving 1,266 participants investigated the effects of combining intermittent fasting or calorie restriction with exercise 42. The researchers found that neither dietary strategy significantly impaired VO2 max (aerobic capacity), bench press strength, leg press strength, vertical jump, or sprint speeds when compared to an exercise-only control group 42. In fact, the combination of IF or CR with exercise actually resulted in slight increases in handgrip strength 42.
Despite these reassurances, clinical guidelines emphasize caution. The American Diabetes Association (ADA) specifically updated its 2025 Standards of Care with a new mandate: clinicians must counsel any patient actively losing weight to incorporate muscle-strengthening exercises into their routine to aggressively prevent sarcopenia 2544.
The AHA Controversy: Navigating Nutritional Risk
In March 2024, intermittent fasting was thrust into the center of a media firestorm. The American Heart Association (AHA) released a press briefing covering a poster presentation from its Epidemiology and Prevention conference. The abstract claimed that adults following an 8-hour time-restricted eating schedule faced a startling 91% higher risk of death from cardiovascular disease compared to those eating across a standard 12-16 hour window 262747.
The scientific and medical communities quickly pushed back against the alarming headlines, criticizing the AHA for releasing premature, non-peer-reviewed data 4828.
The study was an epidemiological survey, a retrospective analysis of observational data drawn from the National Health and Nutrition Examination Surveys (NHANES) between 2003 and 2018 4828. The methodology had severe limitations. First, participants were categorized based on just two 24-hour dietary recall questionnaires submitted over a 15-year period 4748. Second, and most importantly, observational data cannot prove causation. The survey failed to account for why individuals were restricting their eating to an 8-hour window 4748.
In the real world, heavily compressed eating windows are frequently correlated with poverty, lack of food access, severe underlying illness (which suppresses appetite), or chaotic shift-work schedules 48. All of these factors independently and dramatically increase cardiovascular mortality risk. The study did not prove that time-restricted eating damages the heart; rather, it likely highlighted a population facing intense socioeconomic or health stressors. Rigorous, controlled clinical trials consistently show that intermittent fasting improves, rather than harms, cardiovascular biomarkers like blood pressure and lipid profiles 92626.
Clinical Guidelines: What the Experts Say in 2025
Moving beyond observational controversies, the highest authorities in clinical medicine now recognize intermittent fasting as a valid, evidence-based therapeutic tool.
The American Diabetes Association (ADA) 2025 Standards of Care updated its dietary guidelines to explicitly include intermittent energy restriction alongside the Mediterranean and DASH diets for weight management and pre-diabetes care 1625. The ADA recommends an initial goal of 5% to 10% total body weight reduction over six months, noting that this degree of loss produces clinically meaningful improvements in glycemia, lipids, and blood pressure 425.
However, the ADA stresses that the overall quality of the food matters most. The guidelines emphasize nutrient-dense, high-fiber, non-processed foods and healthy fats, regardless of whether a patient restricts their eating window 25. Furthermore, the 2025 updates heavily promote the integration of GLP-1 receptor agonists (like semaglutide) alongside lifestyle interventions for individuals suffering from obesity and MASLD, recognizing that dietary restriction alone is often insufficient for chronic disease management 254429.
The World Health Organization (WHO) also provides guidance on fasting, particularly concerning religious practices like Ramadan. The WHO acknowledges that fasting can be an excellent mechanism for obesity prevention, provided individuals practice safe re-feeding 3. The organization recommends hydrating heavily before meals, breaking fasts with soups to replenish electrolytes, and prioritizing lean proteins and complex carbohydrates (like whole-grain bread and brown rice) over refined sugars and fried foods 3.
Bottom line
The choice between intermittent fasting and daily caloric restriction should be driven entirely by personal preference and psychological sustainability. Both methods reliably produce meaningful weight loss, stimulate cellular autophagy, and improve cardiovascular health when a caloric deficit is achieved. While fasting protocols like the 4:3 diet or alternate-day fasting provide a modest metabolic edge regarding insulin sensitivity and liver fat reduction, daily restriction remains superior for minimizing subjective hunger and fatigue. There is no biological magic trick; the most effective diet is simply the one you can stick to in the long run.