How Much Does VO2 Max Really Predict Lifespan
Exactly how strongly does VO2 max predict human lifespan? Cardiorespiratory fitness, objectively quantified as maximal oxygen uptake (VO2 max), is one of the single most powerful observational predictors of long-term survival in modern medical literature, demonstrating an impact magnitude that frequently surpasses traditional clinical risk factors such as smoking, hypertension, and type 2 diabetes 112. Epidemiological data reveals that ascending from the lowest quartile of cardiorespiratory fitness to the elite tier (the top 2.3% of the population) correlates with an approximate 80% reduction in all-cause mortality, which translates to a five-fold survival advantage over a decade 43. On a granular level, longitudinal analyses demonstrate that each single metabolic equivalent (MET) increment - roughly a 3.5 mL/kg/min increase in VO2 max - is associated with a 13% to 15% reduction in mortality risk 478. Furthermore, each unit increase in VO2 max equates to an estimated 45-day extension in absolute life expectancy, with those achieving high-normal to elite fitness levels enjoying an average of nearly three to five additional years of life compared to their sedentary counterparts 910.
Why Are Longevity Influencers Fixated on VO2 Max?
In recent years, the metric of VO2 max has transcended the confines of exercise physiology laboratories and elite sports science, cementing itself as the central pillar of the mainstream longevity optimization movement. This paradigm shift has been largely orchestrated by highly visible physicians and researchers who translate dense epidemiological hazard ratios into actionable public health directives. By tracing these popularized claims back to their academic origins, it becomes evident that the influencer consensus is deeply anchored in robust, peer-reviewed clinical science.
Dr. Peter Attia has been instrumental in mainstreaming this metric through his conceptual framework of the "Centenarian Decathlon," heavily emphasizing VO2 max as a non-negotiable prerequisite for maintaining physical independence into the final decades of life. Attia frequently cites the 2018 Cleveland Clinic data demonstrating the five-fold mortality risk reduction, advocating for an 80/20 training protocol consisting of 80% low-intensity Zone 2 training and 20% high-intensity VO2 max intervals to build an elite aerobic base 41112.
Similarly, biomedical scientist Dr. Rhonda Patrick has extensively detailed the cardioprotective mechanisms of vigorous exercise, translating specific MET increases into absolute life-years gained. She frequently highlights protocols such as the Norwegian 4x4 method (four minutes of maximum intensity followed by three minutes of recovery, repeated four times) 1314. Patrick points to clinical trials demonstrating that two years of such vigorous intervention can effectively reverse cardiac stiffness, yielding hearts that appear up to two decades younger in fifty-year-old subjects 1314. Furthermore, she emphasizes that vigorous exercise drives lactate production, which serves as a highly efficient, neuroprotective fuel source for the aging brain 15.
Neurobiologist Dr. Andrew Huberman has further synthesized these concepts into weekly behavioral protocols. Huberman advocates for accumulating 150 to 200 minutes of Zone 2 steady-state cardio per week, often utilizing joint-friendly equipment like the VersaClimber to execute maximal-effort sprints without inducing detrimental orthopedic impact 1617. Huberman frames VO2 max not as an athletic vanity metric, but as a critical survival tool, noting research which indicates that a VO2 max dropping below the threshold of 18 mL/kg/min strictly correlates with the loss of independent living and the transition into assisted care facilities 1819.
What Exactly Is VO2 Max? (The Car Engine Analogy)
To understand the longevity implications of VO2 max, it is essential to demystify what the metric actually measures. VO2 max represents the absolute peak volume of oxygen an individual's body can uptake, transport, and utilize during exhaustive, symptom-limited exercise 2021. Because achieving a high VO2 max requires the flawless, simultaneous synchronization of the pulmonary system (lungs), the cardiovascular system (heart pumping chambers and vascular network), and the cellular machinery (skeletal muscle mitochondria extracting oxygen), it serves as the ultimate holistic stress test for systemic human biology 121.
A common misconception is the conflation of VO2 max with general physical endurance. To clearly separate these concepts, sports scientists utilize a highly effective automotive analogy involving engine size, transmission gears, and fuel economy 523.
First, VO2 max represents the sheer displacement or size of a car's engine (for example, a massive V8 engine versus a small four-cylinder). It dictates the absolute maximum power the physiological system can generate when pushed to its ultimate limit 5. However, having a massive engine does not guarantee success in a long endurance race.
Second, the lactate threshold acts as the transmission or the size of the gears in that engine 5. The lactate threshold defines the highest exercise intensity an individual can sustain in a metabolic steady state before fatiguing byproducts, such as lactate, accumulate faster than they can be cleared 524. Two individuals can possess the exact same VO2 max, but the one with a higher lactate threshold can sustain a higher fraction of their maximum speed for an hour 23.
Third, running economy represents the mechanical fuel efficiency, or the "miles per gallon" of the body 2325. If an athlete has a high VO2 max but poor running economy, they waste immense amounts of oxygen on vertical oscillation or inefficient biomechanics, much like a powerful engine burning fuel poorly due to a heavy, un-aerodynamic chassis 2325.
For the specific goal of maximizing lifespan, the "engine size" (VO2 max) is the primary variable of interest. A massive engine provides an enormous functional reserve. As aging naturally diminishes physical capacity, starting with a larger engine ensures that an individual remains far above the threshold of frailty for many more years 216.
Is VO2 Max Just Another Term For General Endurance?
While the engine analogy clarifies the physiological roles, emerging endurance science from 2025 and 2026 further delineates VO2 max from actual athletic endurance through new terminology: durability, fatigability, repeatability, and resilience 24.
A traditional laboratory-measured VO2 max captures an individual's physiological ceiling under fresh, highly controlled conditions lasting roughly ten to twelve minutes 24. However, human endurance events - and the physical demands of daily life - last much longer, introducing variables such as neuromuscular fatigue, cardiac drift, thermoregulatory stress, and glycogen depletion 24. The metric of durability describes how well the body maintains its VO2 max, threshold, and economy after hours of stress 24. Therefore, while VO2 max is an essential prerequisite for endurance and an unparalleled predictor of biological aging, it is only the foundation. An individual can have a high VO2 max but poor durability, meaning their functional capacity drops precipitously under prolonged stress. Nonetheless, from a strictly epidemiological standpoint regarding mortality, the pure capacity measured by the VO2 max ceiling remains the supreme predictor of survival 11.
How Much Does VO2 Max Actually Reduce Mortality Risk?
The assertion that VO2 max dominates mortality risk assessment rests on an expansive foundation of large-cohort mega-studies, which have been continuously validated by updated 2023 and 2024 analyses.
The most frequently cited foundational dataset is the retrospective cohort study conducted by Mandsager and colleagues at the Cleveland Clinic, published in JAMA Network Open in 2018. This monumental analysis evaluated 122,007 adults who underwent symptom-limited exercise treadmill testing, tracking their outcomes over a median follow-up of 8.4 years and encompassing 1.1 million person-years of observation 43. The findings demonstrated a profound, monotonic inverse relationship between cardiorespiratory fitness and risk-adjusted all-cause mortality. Compared to patients in the lowest fitness percentile (the bottom 25%), those achieving elite performance status (the top 2.3% for their age and sex) demonstrated an adjusted hazard ratio of 0.20, representing a staggering 80% reduction in all-cause mortality risk 37. The study famously concluded that the mortality hazard imposed by low cardiorespiratory fitness equaled or exceeded traditional clinical risk factors, including coronary artery disease, smoking, and diabetes 27.
This foundational evidence was corroborated and expanded upon by Kokkinos et al. in a 2022 analysis involving a vast cohort of 750,302 United States veterans. Tracking patients with an average follow-up of nearly 16 years, the researchers established an independent, graded association where every single 1-MET increment increase in aerobic capacity was linked to a 13% to 15% reduction in mortality risk 198. The sheer scale of these mega-studies confirms that regardless of baseline comorbidities, advancing one's cardiovascular engine size offers profound life-extending benefits.
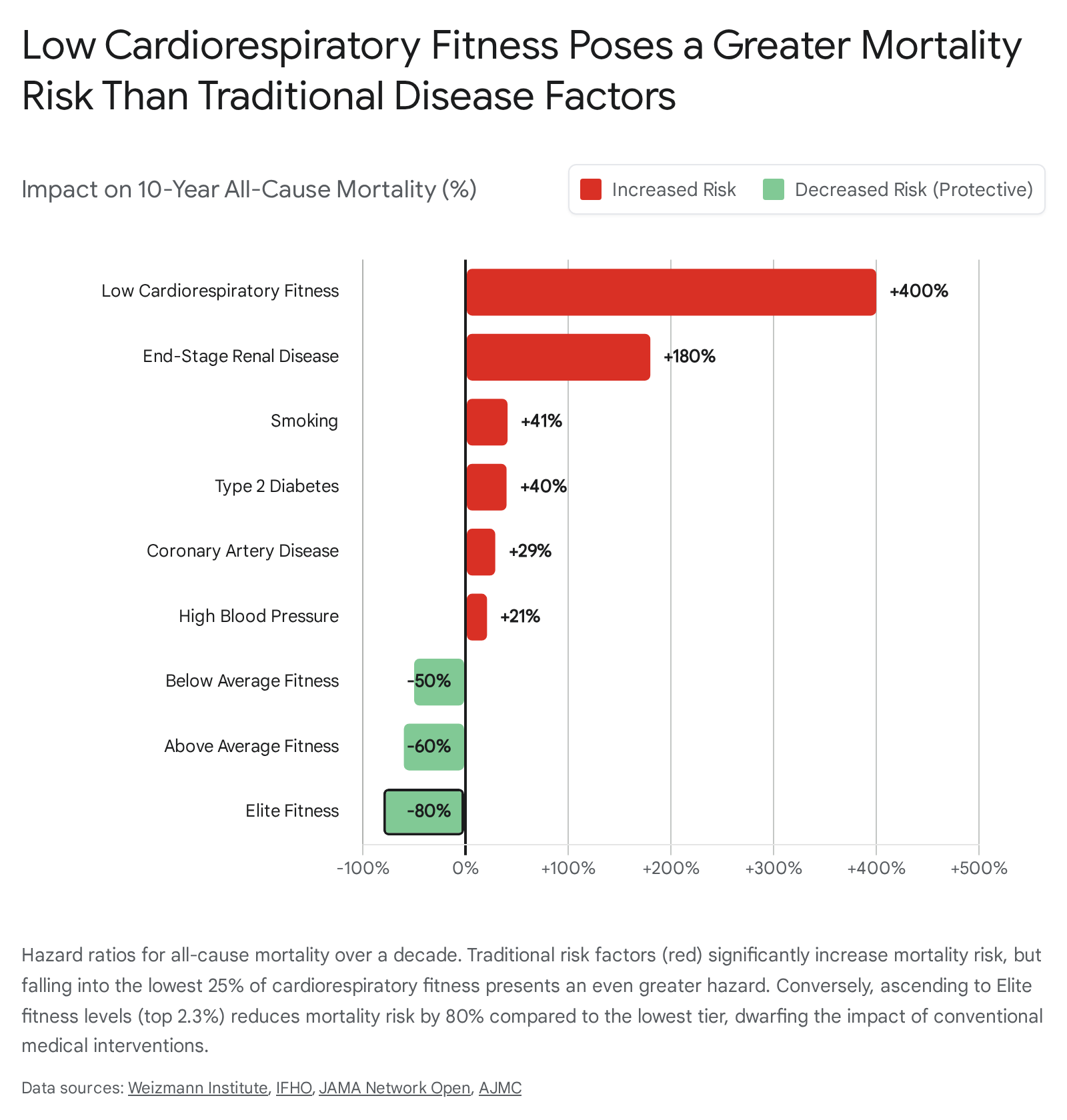
The following table contextualizes the stark difference in mortality hazard when comparing poor cardiorespiratory fitness to widely recognized, severe chronic diseases. The data vividly illustrates that remaining sedentary and allowing cardiovascular capacity to atrophy is biologically equivalent to, or worse than, acquiring a major metabolic or cardiovascular disease.
| Clinical Factor / Fitness Level | Effect on 10-Year All-Cause Mortality Risk | Physiological Implication |
|---|---|---|
| End-Stage Renal Disease | + 180% Increase | Severe, systemic organ failure requiring dialysis. 16 |
| Low VO2 Max (Bottom 25%) | + ~400% Increase (vs. Elite) | A relative mortality penalty that dwarfs individual disease risk factors. 13 |
| Smoking | + 41% Increase | A universally recognized, potent carcinogen and vascular toxin. 16 |
| Type 2 Diabetes | + 40% Increase | Drives systemic inflammation, microvascular damage, and advanced glycation. 16 |
| Coronary Artery Disease | + 29% Increase | Established blockage of the heart's primary vascular supply. 16 |
| High Blood Pressure | + 21% Increase | Chronic mechanical stress degrading the vascular endothelium. 16 |
| --- | --- | --- |
| Below Average VO2 Max | - 50% Decrease (vs. Low) | Merely escaping the bottom quartile cuts mortality risk in half over a decade. 14 |
| Above Average VO2 Max | - 60% to 70% Decrease (vs. Low) | Indicates a highly resilient cardiovascular system capable of resisting disease. 14 |
| Elite VO2 Max (Top 2.3%) | - 80% Decrease (vs. Low) | The absolute peak of physiological reserve, providing a 5-fold survival advantage. 43 |
Does Genetic VO2 Max Cause A Longer Life, Or Just Correlate With It?
While observational data linking VO2 max to lifespan is virtually irrefutable, a critical 2025 bidirectional two-sample Mendelian randomization (MR) study published in The Journal of Clinical Endocrinology & Metabolism introduced highly necessary scientific nuance regarding pure causation 9. Mendelian randomization utilizes genetic variants as instrumental variables to isolate causal effects from observational confounding, addressing the classic "correlation does not equal causation" dilemma.
The Kjaergaard et al. study yielded a fascinating insight: genetically predicted VO2 max showed no direct, independent causal association with extended longevity or the prevention of type 2 diabetes 930. In simpler terms, an individual born with a genetically large cardiovascular engine does not automatically live longer if they remain sedentary. Instead, the multi-variable analysis demonstrated that favorable body composition (specifically lower body fat percentage and higher appendicular lean mass) and lifelong, consistent physical activity were the actual causal drivers of both an elevated VO2 max and a longer lifespan 931.
This 2025 analysis provides a crucial third-order insight: VO2 max is not a magical, isolated causal lever. Rather, it is the ultimate downstream biomarker of a biologically robust, highly active lifestyle 30. The longevity benefits are derived from the strenuous process of building and maintaining capacity - the mechanical loading on joints, the metabolic flux within muscle tissue, the improvements in lipid metabolism, and the resulting adaptations in vascular flexibility 130. VO2 max flawlessly records this cumulative biological history, which is why it remains the ultimate predictor, even if the genetic capacity alone does not cause the longevity.
Do the Longevity Benefits Diminish at Elite Fitness Levels?
A long-standing debate in preventive cardiology - often encapsulated by the "Extreme Exercise Hypothesis" - suggests that chronic, extreme endurance exercise might induce a U-shaped or reverse J-shaped mortality curve. This theory posits that after a certain point, the mechanical stress of relentless aerobic training might lead to myocardial fibrosis, accelerated coronary artery calcification, and atrial fibrillation, thereby causing diminishing returns or even increased mortality at elite levels 27.
The exhaustive Mandsager cohort analysis thoroughly dismantled this misconception regarding all-cause mortality 7. The researchers explicitly and conclusively stated that there was no observed upper limit to the survival benefit of increased cardiorespiratory fitness 27. The participants categorized as "elite" (representing fitness levels equal to or greater than two standard deviations above the mean for their specific age and sex) exhibited significantly lower mortality rates than even the "high" performance group (the 75th to 97.6th percentiles) 37. While it is plausible that the extreme physical act of training twenty hours a week may present localized orthopedic or subtle electrophysiological risks for a tiny fraction of athletes, the sheer systemic physiological capacity reflected by a massive VO2 max remains unconditionally protective against all-cause mortality across the lifespan 23.
Are Women and Aging Populations Equally Protected?
Historically, exercise physiology and sports cardiology literature have heavily over-indexed on middle-aged, white, male cohorts. However, segmented data demonstrates that the survival benefits of VO2 max are equally, if not more, pronounced in diverse demographics, including women and the elderly.
In the 122,000-patient Mandsager study, nearly 41% of the cohort was female 7. When the data was stratified by sex, the inverse monotonic relationship between higher fitness and lower mortality held perfectly true 3. In fact, secondary meta-analyses suggest that women may experience a steeper relative risk reduction per unit of cardiovascular improvement. Some data indicates that for every 1 mL/kg/min increase in peak oxygen uptake, women experience an 11% lower mortality risk, showcasing robust physiological responsiveness 10.
Furthermore, the data emphatically supports the trainability and protective power of VO2 max in aging populations. Absolute VO2 max inevitably declines as a function of chronological aging - typically dropping by roughly 10% per decade after the age of 30, and accelerating to as much as 15% to 20% per decade after age 50 73311. However, this decline is heavily exacerbated by creeping sedentary behavior. Dedicated aerobic training can drastically slow this age-related decay; well-trained master endurance athletes experience an incredibly muted decline of only 5.5% per decade 7. Crucially, the Mandsager data highlighted that the survival benefit of "elite" fitness was particularly striking and statistically significant for patients aged 70 and older, proving that the cardiovascular system's cellular machinery remains highly responsive to exercise stress even in late life 27. This directly combats the onset of frailty, preserving independent living by keeping the elderly above the critical 18 mL/kg/min threshold 1819.
How Does Cardiorespiratory Fitness Impact High-Risk Global Demographics?
Expanding the lens beyond Western cohorts, aggregated data from 2024 and 2025 reveals that cardiovascular capacity is an essential, urgently needed intervention in highly vulnerable global populations.
Populations of South Asian descent (tracing ancestry to nations such as India, Pakistan, and Bangladesh) face an extreme, disproportionate burden of atherosclerotic cardiovascular disease (ASCVD) 12. A landmark 2026 analysis merging longitudinal data from the MASALA and MESA cohort studies revealed a stark reality: South Asian adults develop severe ASCVD risk factors up to a full decade earlier than other racial and ethnic groups in the United States 1213. By the age of 45, South Asian men suffer a 30.7% prevalence of prediabetes - nearly eight times higher than their non-Hispanic white peers at 3.9% 13. Similarly, South Asian women face a prediabetes prevalence of 17.6%, approximately three times higher than their peers 13. This occurs despite South Asian cohorts often reporting healthier overall behaviors, including superior diet quality and lower alcohol consumption 13. Because of this unique genetic propensity for early-onset insulin resistance, visceral adiposity, and dyslipidemia (with 78.2% of South Asian men showing elevated lipids at age 45), increasing VO2 max through rigorous physical training is not merely an athletic pursuit; it is a vital clinical necessity to counteract a biological predisposition to early cardiac mortality 13.
Similarly, the 2024 Global Burden of Disease (GBD) analysis highlights an escalating, catastrophic cardiovascular crisis in the North Africa and Middle East (MENA) region 1438. Between 1990 and 2021, the absolute incidence of cardiovascular disease surged in the region, with ischemic heart disease remaining the supreme driver of Disability-Adjusted Life Years (DALYs), followed closely by stroke 1438. The age-standardized cardiovascular mortality rate attributable specifically to high BMI and low physical activity is wildly elevated in countries like Egypt, Kuwait, and Qatar, reaching 67.5 deaths per 100,000 people - a stark contrast to the 14.4 deaths per 100,000 seen in high-income western nations 15.
Furthermore, African populations remain distressingly under-represented in clinical cardiovascular trials. A 2026 paper highlighted that fewer than 2% of global cardiovascular trials recruit from Africa, severely limiting the understanding of region-specific disease pathology 16. However, localized studies, such as the St. James Study of a low-to-middle income Trinidadian community of African and South Asian descent, reinforce the universal truth of aerobic capacity: men unable to achieve a basic level of work requiring an oxygen uptake of 1.5 L/min during ergometry faced hazard ratios of 3.49 for all-cause mortality and 5.45 for myocardial infarction 17. In these high-risk geographic contexts, public health interventions aimed at shifting massive populations from the lowest quartile of cardiorespiratory fitness to moderate levels represent an unparalleled opportunity to avert millions of premature deaths globally.
How Accurate Is the VO2 Max Estimate on My Smartwatch?
The explosion of consumer wearable technology has democratized access to personal health metrics, placing a "VO2 Max" score on the wrists of millions. However, extensive 2024 and 2025 meta-analyses and validation studies urge extreme caution regarding the clinical accuracy and diagnostic reliability of these commercial estimates.
Smartwatches from dominant brands such as Apple and Garmin do not physically measure oxygen consumption. Instead, they utilize proprietary predictive algorithms based on submaximal heart rate data, GPS-derived running pace, and demographic user inputs (age, weight, biological sex) 4243. Because these devices rely on standardized maximum heart rate formulas (which possess wide standard deviations) and often fail to accurately capture heart rate dynamics during absolute maximal intensity, their outputs are inherently flawed estimates 43.
A comprehensive 2025 validation study published in PLOS ONE specifically evaluated the accuracy of the Apple Watch against the true gold standard: laboratory-based indirect calorimetry (a Cardiopulmonary Exercise Test using a metabolic mask) 1819. The study revealed that the Apple Watch systematically underestimated true VO2 max by a substantial mean difference of 6.07 mL/kg/min 18. Furthermore, the mean absolute percentage error (MAPE) was high at 13.31%, and the Bland-Altman limits of agreement demonstrated massive, unacceptable variability ranging from -6.11 to +18.26 mL/kg/min 18. The researchers decisively concluded that while the Apple Watch provides suitable estimations for general, casual fitness monitoring, its predictions fall two to three standard deviations beyond the typical error of gold-standard measurements, making it insufficiently accurate for clinical decision-making or precise lifespan forecasting 1819.
Conversely, a separate study examining the Garmin Vivoactive 4 found the opposite problem: a large positive bias 20. The Garmin device substantially overestimated VO2 max by approximately 14 mL/kg/min compared to laboratory testing, exhibiting poor agreement when calculating the percentage of predicted VO2 max 20.
The current consensus in sports science is that while high-end wearables provide excellent relative accuracy for tracking an individual's personal trends and directional progress over time, they lack the absolute physiological precision required to establish a true baseline 4243. Individuals seeking to accurately anchor their longevity strategy should undergo direct gas-exchange analysis in a clinical setting 2142.
What Is the Practical ROI: Escaping the Bottom 25% Versus Reaching the Top 5%?
When constructing a practical, sustainable longevity strategy, it is imperative to understand the Return on Investment (ROI) of physical training. The mortality benefit curve associated with VO2 max is profoundly non-linear; the most dramatic, life-altering health gains are achieved by those making relatively modest improvements at the absolute bottom of the fitness spectrum.
For individuals languishing in the bottom 25% of the population - characterized as having "low" fitness - the risk of early mortality is severely elevated. However, this demographic possesses the highest potential for rapid transformation. Transitioning from the "low" category to simply "below average" (the 25th to 50th percentile) yields the single most profound physiological ROI available in modern medicine: an approximate 50% reduction in all-cause mortality risk over the following decade 14. This life-saving leap does not require grueling athletic regimens; it typically demands only the consistent introduction of moderate-intensity, steady-state physical activity, such as brisk daily walking, light cycling, or swimming, accumulating just 90 to 150 minutes per week 1647. Moving out of this bottom quartile translates directly into a 2.1-year absolute increase in life expectancy 9.
Transitioning further, from "low" to "above average" or "high normal" (the 50th to 75th percentile), yields a massive 60% to 70% reduction in mortality risk, granting an average of roughly three additional years of life 149. Achieving this level of resilience generally requires dedicated, structured exercise programming that deliberately stresses the cardiovascular system. This often involves a polarized training model, where the bulk of training consists of Zone 2 aerobic base work to stimulate mitochondrial density and fat oxidation, peppered with occasional, targeted high-intensity intervals to push the upper bounds of cardiac stroke volume 166.
Finally, striving to reach the elite category - the top 2.3% of the population for one's age and sex - provides the absolute maximum biological buffer against aging, delivering the lauded five-fold, 80% reduction in mortality risk and nearly five added years of life expectancy 149. However, the time and physical effort required to cross the threshold from the 75th percentile to the 98th percentile are exponential. It demands rigorous, painful protocols, such as sustained maximum-effort sprints that push the cardiovascular system to its absolute limits 1417. While reaching this elite echelon guarantees exceptional physical capability well into old age, the global public health imperative must remain sharply focused on moving sedentary, aging populations out of the lowest quartile, where the vast majority of premature, preventable deaths occur 1.
Bottom Line
Cardiorespiratory fitness, empirically measured as VO2 max, is the ultimate macroscopic indicator of systemic human health and biological resilience. While genetic predispositions and baseline body composition play foundational, causal roles in shaping physical capacity, the deliberate pursuit of a higher VO2 max through structured aerobic and high-intensity exercise provides unprecedented protection against all-cause mortality, dramatically outperforming traditional pharmacological interventions for chronic diseases. The data is unequivocal: there is no upper limit to the survival benefits of extreme fitness. However, the most urgent and mathematically impactful health intervention an individual can make is to simply escape the lowest quartile of fitness, securing an immediate, massive reduction in mortality risk and laying the mechanical groundwork for decades of functional independence.