Evidence-Based Ways to Improve Your VO2 Max
The most effective method for improving VO2 max is high-intensity interval training (HIIT), specifically protocols like the Norwegian 4x4 that sustain near-maximal heart rates for several minutes to maximize cardiac output. While genetics determine your absolute aerobic ceiling, combining these intense intervals with a high volume of low-intensity steady-state cardio can yield significant cardiovascular adaptations in as little as eight weeks. To safely maximize endurance without overtraining, integrating these intensities into a polarized training model is widely considered the clinical and athletic gold standard.
Understanding the Physiology of Aerobic Capacity
Maximal oxygen uptake, almost universally known as VO2 max, is the maximum rate at which your body can absorb, transport, and utilize oxygen during exhaustive exercise 12. It is recognized by exercise physiologists and medical professionals as the definitive gold-standard metric for assessing cardiovascular fitness and aerobic endurance capacity 13.
To grasp how VO2 max functions, researchers often use the engine displacement analogy. Just as a vehicle's engine size and fuel injection system determine its maximum horsepower and speed, your VO2 max determines your biological aerobic power ceiling 1. When you run, cycle, or swim at high intensities, your muscles demand massive amounts of oxygen to produce adenosine triphosphate (ATP), the cellular energy currency that powers muscle contractions 2. The measurement of this capacity is expressed in milliliters of oxygen consumed per kilogram of body weight per minute (ml/kg/min), which normalizes the data to allow for accurate comparisons across individuals of vastly different body sizes 12.
The Fick Equation and Oxygen Transport
Your VO2 max is not a single, isolated function. Instead, it represents the integrated culmination of your respiratory, cardiovascular, and muscular systems working in perfect concert. Physiologically, VO2 max is governed by a principle known as the Fick equation. This equation dictates that maximal oxygen consumption equals your maximum cardiac output multiplied by your arterio-venous oxygen difference (a-vO2 diff) 34.
To improve your VO2 max, your training must force biological adaptations in one or both of these primary variables:
- Cardiac Output: This refers to the sheer volume of oxygenated blood your heart can pump per minute, calculated as heart rate multiplied by stroke volume 13. While your maximum heart rate is largely genetically fixed and declines predictably by about one beat per minute per year after age 25, stroke volume is highly trainable 15. Elite endurance athletes achieve their massive VO2 max numbers primarily by developing enlarged, highly compliant left ventricular heart chambers 45. This adaptation, known as eccentric cardiac hypertrophy, allows the heart to relax quickly, fill with a massive volume of blood (end-diastolic volume), and forcefully eject it to the working muscles with every single beat 4.
- Arterio-venous Oxygen Difference (a-vO2 diff): This metric represents the efficiency with which your working skeletal muscles can extract oxygen from the bloodstream 4. Merely delivering oxygen to the muscle is insufficient if the muscle cells cannot process it. Training improves this extraction by increasing the density of capillary networks surrounding the muscle fibers and multiplying the size and number of mitochondria within the cells themselves 12.
Central vs. Peripheral Limitations
Exercise scientists have long debated whether VO2 max is primarily limited by central factors (the heart's ability to deliver blood) or peripheral factors (the muscles' ability to use the oxygen). The prevailing consensus is that a central component ultimately serves as the primary bottleneck for an individual's maximum capacity 5.
Research estimates that 70% to 85% of the limitation in VO2 max is directly linked to maximal cardiac output 5. During near-maximal exercise, very little oxygen is left to be extracted out of the blood; the extraction process is already operating near its limit. Therefore, the dominant mechanism for significant increases in VO2 max with training must be an increase in overall blood flow and oxygen delivery 5. This underscores why cardiovascular training that heavily stresses stroke volume is essential for moving the needle on your fitness metrics.
VO2 Max as the Ultimate Indicator of Longevity
While VO2 max has historically been the domain of elite endurance athletes, it has recently emerged as one of the most powerful predictors of human longevity, all-cause mortality, and healthspan 27.
A landmark 2018 study published in JAMA Network Open fundamentally changed how the medical community views cardiorespiratory fitness. Researchers at the Cleveland Clinic followed over 122,000 patients and found that cardiorespiratory fitness, as measured objectively by treadmill testing rather than self-reported activity, was inversely associated with all-cause mortality at every single level of fitness 7.
The Mortality Risk of Poor Fitness
The data revealed that individuals in the lowest fitness tier faced a mortality risk roughly five times higher than those in the elite group 27. More staggeringly, the risk associated with being in the lowest fitness category was comparable to, or in some cases worse than, having coronary artery disease, having diabetes, or being a current smoker 7.
The benefits of improving aerobic capacity are profound and highly responsive to even minor changes. Moving from the lowest fitness group to merely the "below average" tier yielded a larger reduction in mortality risk than quitting smoking 7.
The Metabolic Equivalent (MET) Advantage
Cardiorespiratory fitness improvements are often measured in Metabolic Equivalents (METs). One MET is the amount of oxygen your body consumes at rest, which equates to exactly 3.5 ml/kg/min of oxygen uptake 28.
Separate meta-analyses in leading sports medicine journals indicate that every 1-MET increase in aerobic capacity is associated with an 11% to 17% reduction in the relative risk of all-cause mortality 8. A 2022 meta-analysis in the British Journal of Sports Medicine further clarified these margins, showing that just a 1 ml/kg/min improvement in VO2 max corresponds to a 2% to 3% reduction in all-cause mortality risk, meaning that even granular, fractional gains in cardiovascular efficiency directly translate to an extended lifespan 7.
The Science of Trainability: Genetics vs. Effort
A pervasive and long-held misconception in physical education and exercise physiology is that your VO2 max is overwhelmingly fixed by genetics, and that if you are unhappy with your baseline numbers, you have no choice but to "blame your parents" 9. Historically, textbooks and prevailing theories claimed that the average person could only hope to improve their VO2 max by a meager 5% to 15%, regardless of how intensely or consistently they trained 910.
Modern sports science, longitudinal athletic data, and genetic sequencing paint a far more nuanced and optimistic picture. While your DNA undeniably establishes a biological baseline, your ultimate potential is remarkably fluid.
The Heritability of Aerobic Capacity
Your genetic makeup influences not only your baseline cardiorespiratory fitness but also your "trainability" - how robustly and rapidly your body adapts to an exercise stimulus 1112. Twin and family studies indicate that genetics account for roughly 47% of the inter-individual variance in VO2 max training response 1112.
Researchers have identified nearly 100 specific genes that serve as possible predictors for how well someone will respond to endurance training 12. For example, specific variants of the NRF2 gene are strongly linked to enhanced mitochondrial biogenesis, which allows these individuals to experience more rapid increases in VO2 max in response to aerobic volume 6.
Conversely, variants in the HIF1A (Hypoxia-Inducible Factor 1 Alpha) gene, which regulates cellular responses to oxygen deprivation and metabolic adaptation, can delay cardiovascular adaptations. Individuals carrying specific HIF1A variants often experience slower improvements and may require much higher intensities or more frequent high-intensity interval sessions to stimulate equivalent cardiovascular changes 6. Other significant genetic markers include the ACE gene, which helps regulate blood pressure and fluid balance, and the MTC1 gene, which affects the production and clearance of lactic acid 1011.
Typical vs. Maximum Training Improvements
The outdated rule of thumb suggesting a hard 15% ceiling for VO2 max improvement stemmed largely from short-term studies 910. Because it is notoriously difficult to keep study participants compliant in strenuous, supervised exercise regimens for longer than eight to twelve weeks, sports science historically relied on truncated datasets 914.
However, when exercise physiologists track real-world athletes engaging in consistent, well-structured endurance training over multi-year periods, the narrative shifts entirely. Improvements of approximately 25% are considered very typical for individuals transitioning from a sedentary lifestyle to a structured endurance program over several years 9.
Gains approaching 40% to 50% have been documented in highly dedicated amateurs who incrementally build their cardiovascular base 910. In one extreme and highly documented case report published in 2009, a 43-year-old male achieved an astonishing 96% improvement in his VO2 max (moving from a baseline of 27.6 ml/kg/min to 54.1 ml/kg/min) over a 24-month period of targeted, progressive training 7. This underscores that with a sufficient timeline and appropriate progressive overload, the genetic "ceiling" is much higher than previously believed.
Sex Dimorphism in VO2 Max and Adaptability
Research indicates there are distinct biological differences in both baseline aerobic capacity and the physiological adaptations that occur in men versus women following endurance training 817.
Women generally exhibit absolute VO2 max values that are 10% to 15% lower than men of equivalent training status and age 78. This gap is not a matter of effort or training methodology, but is rooted in fundamental anatomical and physiological realities. Women generally have smaller average heart sizes, which limits maximal stroke volume and peak cardiac output 8. Furthermore, women tend to have lower total blood volumes and lower hemoglobin concentrations. Because hemoglobin is the protein responsible for transporting oxygen in red blood cells, a lower concentration means the blood carries slightly less oxygen per liter pumped 1819.
Trainability Differences Between the Sexes
Beyond baseline differences, there is evidence suggesting a sexual dimorphism in how the body adapts to training. A comprehensive 2019 systematic review and meta-analysis investigated whether men and women respond differently to the exact same dose of endurance training 1920.
The pooled data from eight tightly controlled studies comprising 175 untrained men and women showed that endurance training induced substantially larger increases in absolute VO2 max in men compared with women (a mean difference of +191 ml/min) 1920. A greater effect on relative VO2 max was also observed in men (a mean difference of +1.95 ml/kg/min) 1920. These findings indicate that men may experience a slightly more pronounced cardiovascular adaptation to a standardized training stimulus.
Compensatory Mechanisms in Female Athletes
Despite lower peak VO2 max values and potentially blunted cardiovascular trainability, female endurance athletes often close the performance gap through compensatory physiological mechanisms.
Research shows that women frequently demonstrate superior running economy - meaning they utilize less oxygen at submaximal speeds compared to men 8. One study found that despite a 25% difference in VO2 max between the sexes, the maximal aerobic speed was only 18% different, indicating that enhanced biomechanical and metabolic efficiency partially offsets the sheer cardiovascular power gap 8. Additionally, some data suggests women may have slightly higher lactate thresholds relative to their VO2 max, allowing them to sustain a higher percentage of their maximum capacity for longer durations 8.
Training Modalities: The Battle of Intensities
When designing a program to improve VO2 max, the fundamental physiological debate usually centers on the relationship between intensity and duration. The primary training modalities utilized in research and athletics include:
| Training Modality | Abbreviation | Typical Intensity Level | Structure |
|---|---|---|---|
| Continuous Training | CT / MICT | 60 - 75% of Max Heart Rate | Prolonged, steady-state exercise lasting 45 to 120+ minutes. The pace is conversational. |
| High-Intensity Interval Training | HIIT | 85 - 95% of Max Heart Rate | Repeated bouts of intense work lasting 1 to 5 minutes, separated by active recovery periods. |
| Sprint Interval Training | SIT | > 100% VO2 Max (Supramaximal) | Very short, "all-out" maximal efforts lasting 15 to 30 seconds, followed by longer passive rest. |
| Repeated Sprint Training | RST | > 100% VO2 Max (Supramaximal) | Incredibly short sprints (≤ 10 seconds) separated by very brief recovery intervals (≤ 60 seconds). |
What the Data Says: Intervals vs. Continuous
To definitively settle the debate on which method is superior for improving VO2 max, researchers published a massive network meta-analysis in 2025 9. The analysis evaluated 51 eligible studies encompassing 1,261 athletes to quantify the effect sizes (using Hedges' g) and rank the probabilistic efficacy of different training methods 9.
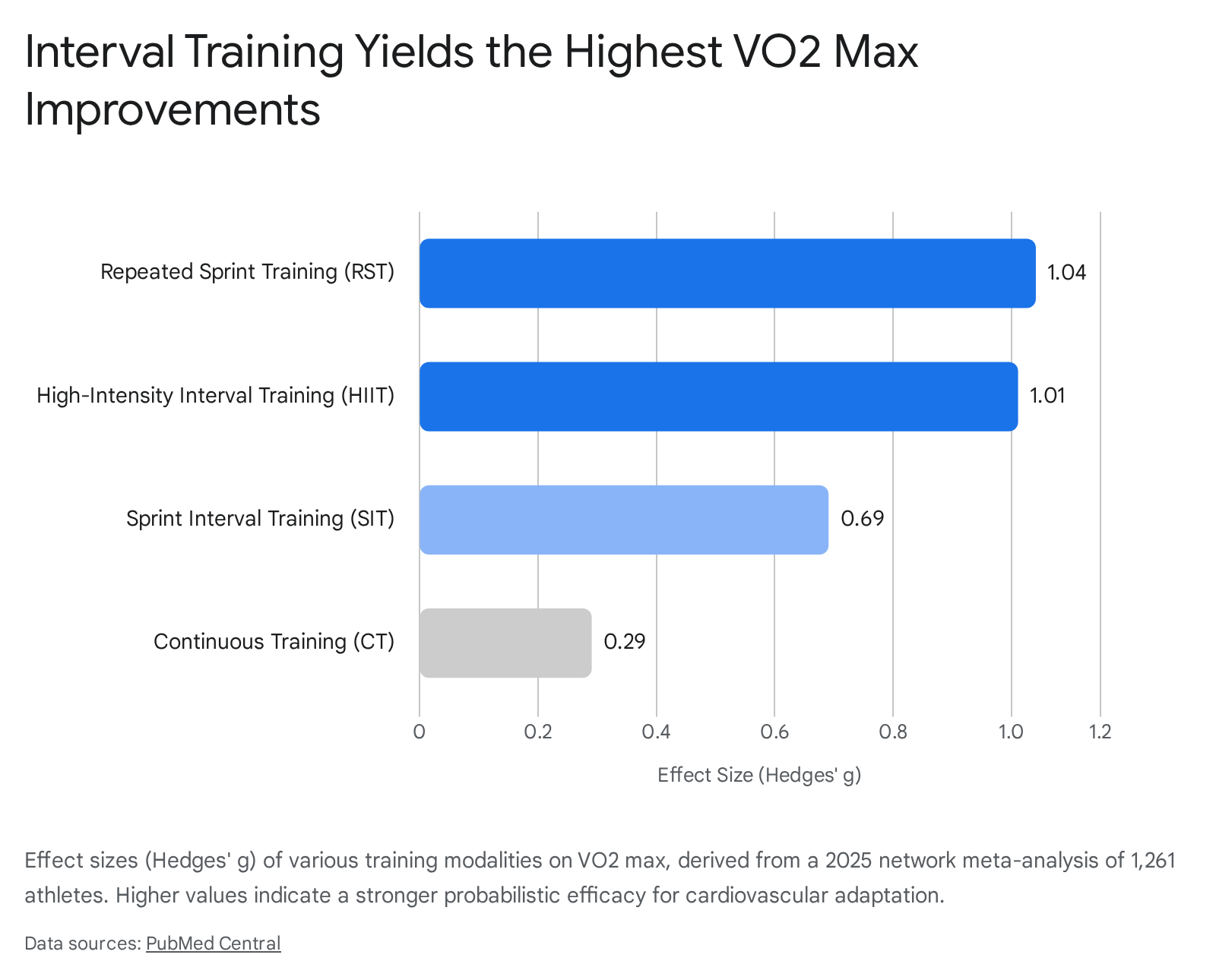
The results overwhelmingly favored high-intensity interval variations over traditional steady-state continuous training. The statistical ranking of effectiveness for increasing VO2 max was:
- Repeated Sprint Training (RST): Effect size = 1.04
- High-Intensity Interval Training (HIIT): Effect size = 1.01
- Sprint Interval Training (SIT): Effect size = 0.69
- Continuous Training (CT): Effect size = 0.29 9.
While there were no statistically significant differences in effectiveness among RST, HIIT, and SIT themselves (indicating they are all highly potent stimuli), all three interval methods were vastly superior to conventional continuous training 9. In fact, in some network comparisons, the effect size for continuous training was barely statistically significant compared to doing nothing 9.
A separate 2024 umbrella review encompassing 24 systematic reviews, 429 primary studies, and nearly 13,000 participants confirmed these findings across the general adult population. The review concluded that HIIT and SIT consistently generate significantly greater VO2 max increases than moderate-intensity continuous training (MICT), yielding an average absolute advantage of 0.52 to 3.76 ml/kg/min over steady-state cardio 822.
Dialing in the Optimal Interval Parameters
Not all interval sessions trigger the same physiological adaptations. The 2025 meta-regression models identified highly specific dose-response relationships for maximizing cardiovascular gains:
- Optimal HIIT Duration: The data revealed an inverted U-shaped relationship for High-Intensity Interval Training. The absolute peak biological benefit occurred with a work duration of 140 seconds per interval, using a work-to-recovery ratio of 0.85 (which equates to roughly 165 seconds of active recovery) 9. Interventions that were significantly shorter or longer than this sweet spot yielded diminished returns.
- The SIT Recovery Threshold: For sprint intervals (e.g., 20 to 30-second all-out maximal efforts), the recovery duration is the critical point of failure. The meta-analysis found that if the passive recovery duration between sprints exceeds 97 seconds, the improvements in VO2 max cease to be statistically significant 9. Rest intervals must be kept brief enough to prevent the cardiovascular system from fully recovering, thereby enforcing a cumulative stress load.
The Clinical Gold Standard: The Norwegian 4x4 Protocol
While meta-analyses point to an optimal 140-second interval, the most extensively researched and clinically validated specific HIIT protocol for VO2 max enhancement is the Norwegian 4x4 231025. Developed by exercise physiologists Ulrik Wisløff, Jan Hoff, and Jan Helgerud at the Norwegian University of Science and Technology (NTNU), this protocol has been successfully deployed in everyone from elite athletes to post-infarction heart disease patients 232511.
How to Execute the Protocol
The Norwegian 4x4 is a highly structured, 38- to 45-minute workout that is modality-agnostic; it can be performed while running, cycling, rowing, swimming, or cross-country skiing, provided the cardiovascular demand is sufficiently high 231012. The protocol consists of:
- Warm-up: 10 minutes of low-to-moderate intensity exercise to gradually elevate the heart rate and prepare the joints 1028.
- Interval 1: 4 minutes of high-intensity work targeting 85% to 95% of your maximum heart rate. Breathing should be extremely heavy. On a Rate of Perceived Exertion (RPE) scale, this is an 8.5 or 9 out of 10 1028.
- Active Recovery 1: 3 minutes of light, active movement (e.g., brisk walking or slow jogging). This allows your heart rate to drop to approximately 60% to 70% of its maximum, facilitating the clearance of lactic acid without allowing the cardiovascular system to return to baseline 1028.
- Repeat: Complete the 4-minute work and 3-minute recovery sequence a total of four times 1229.
- Cool-down: 5 to 10 minutes of easy movement to bring the body back to homeostasis 1028.
The Physiology of the 4-Minute Window
The specific 4-minute duration prescribed by the Norwegian researchers is not arbitrary; it is inextricably tied to human oxygen uptake kinetics. When you begin a hard cardiovascular effort, your heart and lungs do not instantly jump to their maximal capacity 2530. It takes the human body approximately 1.5 to 2 minutes of intense work for the cardiovascular system to "ramp up" and reach near-VO2 max levels 30.
If an athlete performs short 1-minute intervals, they spend virtually no time actually stressing their system at its VO2 max ceiling before the interval ends 31. By extending the interval to 4 minutes, the protocol guarantees that the heart and lungs operate at absolute maximum capacity for a solid 2 to 2.5 minutes per round. Across four intervals, the athlete accumulates roughly 8 to 10 minutes of true VO2 max stress. This sustained cardiovascular overload is the primary trigger that signals the left ventricle of the heart to expand and increase its stroke volume 3031.
In NTNU's foundational 2007 study, moderately trained male athletes who performed the 4x4 protocol three times a week for eight weeks achieved a 7.2% to 13% improvement in VO2 max 22831.
Alternative Interval Protocols
While the 4x4 is highly effective, it is also psychologically and physically grueling. Other scientifically validated interval protocols that manipulate oxygen kinetics to achieve similar ends include:
- The Billat 30/30: Developed by French exercise physiologist Veronique Billat, this protocol involves 30 seconds of hard running at VO2 max pace (roughly 5K race pace), followed immediately by 30 seconds of easy jogging, repeated continuously for 10 to 15 minutes 31. Because the recovery is incredibly short, oxygen consumption stays near its peak even during the "easy" 30 seconds. This allows athletes to accumulate almost 8 minutes of total time at VO2 max while feeling significantly less painful mentally than a continuous 4-minute unbroken interval 31.
- Jack Daniels' 5-Minute Intervals: Legendary Olympic running coach Jack Daniels advocated for 4 to 5-minute intervals with equal or slightly shorter recovery times (e.g., 5 minutes hard, 3 to 4 minutes jogging). His coaching research found that this duration hits the "sweet spot" of maximizing time spent at VO2 max without inducing catastrophic anaerobic (lactic acid) fatigue that would ruin subsequent intervals 31.
Polarized Training vs. Threshold Training
Given the overwhelming statistical superiority of HIIT and the proven track record of the Norwegian 4x4, a logical but dangerous assumption is that an athlete should abandon slow cardio entirely and perform intense intervals every day. This approach is a physiological trap.
Attempting to perform HIIT too frequently rapidly leads to overtraining, severe central nervous system fatigue, and a high risk of injury 1432. Furthermore, HIIT primarily builds the "peak" of your aerobic engine (cardiac stroke volume), but you still must build the metabolic foundation 33.
The Engine Builder: Zone 2 Cardio
Zone 2 cardio - steady-state continuous exercise performed at roughly 65% to 75% of your maximum heart rate - is the bedrock of endurance training 3233. Operating in this moderate intensity zone does not rapidly increase stroke volume, but it causes profound peripheral adaptations 3234. It stimulates the development of slow-twitch muscle fibers, increases capillary density, and massively upregulates mitochondrial size and efficiency, which enhances the body's ability to oxidize fat for fuel 2834.
If an athlete attempts high-intensity interval training without first establishing a robust Zone 2 base, they will struggle to clear lactic acid efficiently during the active recovery periods. Without this clearance, they will be too fatigued to run or cycle fast enough to actually reach their VO2 max ceiling on the third and fourth intervals, rendering the workout ineffective 32.
The 80/20 Polarized Model
To safely and optimally increase VO2 max over the long term, the scientific consensus among elite coaches and exercise physiologists points to Polarized Training 832.
This methodology distributes total weekly training volume so that approximately 80% of the time is spent at low intensity (Zone 2 or below), and 20% is spent at very high intensity (Zone 5/VO2 max intervals) 832. Crucially, it almost entirely avoids the middle ground - often referred to as the "garbage zone" or Zone 3 - which is too strenuous to allow for proper recovery but not intense enough to stimulate maximum cardiovascular adaptation 1432.
A comprehensive 2024 meta-analysis encompassing 17 studies and 437 subjects compared Polarized Training (POL) against traditional Threshold Training (THR), where athletes spend large amounts of time in those moderate, "comfortably hard" middle zones 1314. The pooled data proved that Polarized Training is definitively superior for improving VO2 max and peak aerobic power 1314.
The superiority of the 80/20 polarized split was particularly pronounced in interventions lasting less than 12 weeks, and among highly trained national-level athletes who often suffer from performance plateaus when relying on threshold models 1314.
| Training Zone Focus | Percentage of Weekly Volume | Primary Adaptation Targeted | Ideal Modality |
|---|---|---|---|
| Low Intensity (Zone 1-2) | ~80% | Mitochondrial biogenesis, fat oxidation, capillary density, durability. | Steady-state cycling, brisk walking, slow jogging. |
| High Intensity (Zone 5) | ~20% | Stroke volume, cardiac output, maximum oxygen uptake limit. | Norwegian 4x4, Billat 30/30, Hill sprints. |
In practice, an evidence-based week for a recreational athlete seeking to improve their VO2 max might involve three days of 45 to 60-minute easy Zone 2 cardio, interspersed with one or two dedicated Norwegian 4x4 interval sessions 323715.
Timelines, Plateaus, and Detraining
Cardiovascular adaptation operates on a distinct physiological timeline. While athletes often feel subjectively fitter within days of starting a new program due to an expansion of blood plasma volume, actual structural changes to the heart and muscles take weeks to materialize.
- The Upward Curve: For beginners and moderately trained individuals, significant, measurable improvements in VO2 max generally take 6 to 10 weeks of consistent training 39. The Norwegian 4x4 clinical studies routinely use an 8-week timeline to showcase their reliable 7% to 15% gains 102512.
- The Plateau Effect: After 12 to 16 weeks of executing a specific interval protocol, the rate of VO2 max improvement typically begins to slow significantly due to the law of diminishing returns 1540. Highly experienced endurance athletes may train for years with virtually no absolute change in their VO2 max, having hit their genetic ceiling 3940. However, these athletes continue to get faster in races by improving their lactate threshold and biomechanical efficiency 39.
- The Detraining Drop-off: Unfortunately, the adaptations that build VO2 max are highly transient. If an individual stops training completely, VO2 max drops rapidly. Research indicates an approximate 5% decline in VO2 max within just two weeks of total inactivity 39.
Over prolonged periods of sedentary behavior, an individual's VO2 max naturally declines by about 10% per decade of life, mostly due to the unavoidable drop in maximum heart rate and the onset of sarcopenia (age-related muscle loss) 177. However, maintaining a consistent aerobic exercise routine throughout adulthood can cut this age-related decline by half 7.
ACSM Guidelines and Cardiorespiratory Benchmarks
For general health and fitness, the American College of Sports Medicine (ACSM) is widely considered the gold standard for exercise prescription 16. According to the current physical activity guidelines (endorsed by the CDC and detailed in the ACSM's 12th edition Guidelines for Exercise Testing and Prescription):
- Aerobic Minimums: All healthy adults aged 18 to 65 should accumulate a minimum of 150 minutes of moderate-intensity aerobic physical activity per week (e.g., 30 minutes, five days a week) OR a minimum of 75 minutes of vigorous-intensity aerobic activity per week (e.g., 20 to 25 minutes, three days a week), or an equivalent combination of both 1642.
- Intensity Thresholds: To actually improve VO2 max, rather than simply maintain basic metabolic health, the ACSM notes that the minimal training intensity threshold is approximately 40% to 50% of an individual's Heart Rate Reserve (HRR) for highly deconditioned people 43. However, as fitness improves, this threshold rapidly shifts; trained individuals must operate at 60% to 85% of their HRR to force continued adaptation 4344.
Benchmarking: What Is a "Good" VO2 Max?
Because VO2 max naturally declines with age and differs by sex, the classification of what constitutes a "good" or "elite" score varies across demographics. According to ACSM fitness classifications, the benchmarks for the 50th to 75th percentile range are as follows:
| Demographic | Age Range | "Good" VO2 Max Range (ml/kg/min) | "Excellent" / Elite Threshold |
|---|---|---|---|
| Men | 20 - 29 | 37 to 41 | > 42 |
| Men | 40 - 49 | 33 to 36 | > 37 |
| Men | 60+ | 26 to 30 | > 31 |
| Women | 20 - 29 | 32 to 36 | > 37 |
| Women | 40 - 49 | 28 to 32 | > 33 |
| Women | 60+ | 21 to 25 | > 26 |
Data derived from ACSM age- and sex-stratified cardiorespiratory fitness reference data 7.
Values pushing past the "excellent" threshold for a given age group correlate strongly with maximum lifespan extension benefits and significantly lowered all-cause mortality risk 7.
Bottom line
The most effective, evidence-based strategy to improve your VO2 max is to combine a high-volume base of steady-state "Zone 2" cardio with one or two weekly sessions of High-Intensity Interval Training (HIIT). Protocols like the Norwegian 4x4 - which forces the heart to operate at 85% to 95% of its maximum capacity for prolonged four-minute stretches - consistently trigger the greatest increases in cardiac stroke volume. While genetics dictate the speed of adaptation and the ultimate biological ceiling, research confirms that implementing a polarized 80/20 training model can yield life-extending cardiovascular improvements of 7% to 15% in as little as eight weeks.