Zone 2 Training and Longevity
The prescription of physical activity for the extension of healthspan and the prevention of all-cause mortality relies heavily on optimizing the distribution of exercise intensity over the human lifespan. In recent years, sports medicine, exercise physiology, and preventative cardiology have increasingly emphasized "Zone 2" training - a specific moderate-intensity aerobic threshold - as a foundational component for maximizing metabolic health. This report systematically examines the physiological markers that define Zone 2, evaluates its role in mitochondrial adaptation and substrate utilization, compares it against higher-intensity training modalities, and comprehensively analyzes the epidemiological evidence linking this specific training prescription to enhanced longevity.
Physiological Frameworks of Training Intensity
To evaluate the clinical and performance outcomes of physical training, sports scientists utilize specialized frameworks to categorize exercise intensity. The terminology surrounding training zones can be ambiguous because researchers, clinical practitioners, and commercial fitness platforms rely on varying models, primarily the three-zone and five-zone frameworks. Understanding the precise physiological demarcations of these models is critical for accurately prescribing exercise for longevity.
Three-Zone Versus Five-Zone Models
Exercise intensity is not a seamless continuum but is instead demarcated by specific physiological inflection points where the body's metabolic responses and primary fuel sources shift significantly. In clinical and laboratory settings, researchers universally rely on a three-zone model anchored by two measurable metabolic breakpoints: the first and second lactate thresholds (LT1 and LT2) or their ventilatory equivalents (VT1 and VT2) 123.
In this strict physiological three-zone model, the zones are defined by specific metabolic states. Zone 1 encompasses exercise performed below the first lactate threshold (LT1) or first ventilatory threshold (VT1). In this state, blood lactate remains near resting baseline levels, typically below 2.0 millimoles per liter (mmol/L), and oxygen supply meets metabolic demand effortlessly 124. Zone 2 in this model represents exercise performed between LT1/VT1 and LT2/VT2. This is often referred to as the threshold or tempo zone, where lactate begins to accumulate faster than it can be cleared, but a steady state can still be achieved, known as the Maximal Lactate Steady State (MLSS) 14. Finally, Zone 3 represents exercise performed above LT2/VT2, denoting high-intensity or maximal aerobic efforts approaching VO2 max, where lactate accumulation is rapid, exponential, and unsustainable 24.
While the three-zone model reflects objective physiological realities, practical application in commercial coaching and digital fitness platforms frequently utilizes a five-zone heart rate model popularized in the early 2000s by exercise physiologists such as Dr. Andrew Coggan 15. This division introduces a nomenclature shift that is responsible for widespread confusion in popular media and amateur athletics 13. The highly recommended "Zone 2" for longevity training corresponds strictly to the five-zone model's Zone 2, which is physiologically equivalent to the upper end of Zone 1 in the three-zone model 124.
| Physiological Marker | Three-Zone Model Equivalent | Five-Zone Model Equivalent | Metabolic Characteristics |
|---|---|---|---|
| Below LT1 / VT1 | Zone 1 | Zone 1 & Zone 2 | High fat oxidation, steady baseline lactate (< 2 mmol/L), conversational pacing. (Target of longevity Zone 2) |
| Between LT1 and LT2 | Zone 2 | Zone 3 & Zone 4 | Increasing carbohydrate oxidation, rising but stable lactate, labored breathing (Tempo/Threshold). |
| Above LT2 / VT2 | Zone 3 | Zone 5 | Predominant carbohydrate oxidation, exponential lactate accumulation, non-conversational (VO2 Max). |
Biological Markers and Lactate Thresholds
In the five-zone model, the much-discussed Zone 2 occurs strictly below LT1/VT1 3. It represents the maximum aerobic exertion an individual can sustain while maintaining a steady-state physiological response, minimal blood lactate elevation, and a primary reliance on lipid oxidation 36. An expert consensus panel in sports medicine defines the preferred intensity for Zone 2 training as being located just below LT1 or VT1 3. At this specific intensity, physiologists expect a steady-state profile with no changes or only transient, easily cleared increases in blood lactate, stable heart rate values, low values of rating of perceived exertion (RPE), and power outputs representing approximately 75% to 80% of critical power 3.
The reliance on precise biological markers is necessary because the physiological adaptations associated with Zone 2 - such as mitochondrial biogenesis and increased fat oxidation - diminish or shift in nature once the first lactate threshold is crossed 46. When an individual drifts past LT1 into the moderate-intensity domain (Zone 3 in the five-zone model), the body begins to increase its reliance on anaerobic glycolysis, initiating molecular stress signals that fundamentally alter the adaptive response and accumulate systemic fatigue without providing the maximal aerobic development characteristic of true low-intensity work 4.
Calculation Methodologies and Individual Variability
Because laboratory testing involving blood lactate sampling and indirect calorimetry is inaccessible to most individuals, proxy metrics such as heart rate tracking and subjective ratings of perceived exertion are heavily utilized to estimate the boundaries of Zone 2. The accuracy of these methodologies varies considerably, and reliance on oversimplified formulas can lead to inappropriate training prescriptions.
Age-Predicted Maximum Heart Rate Formulas
The simplest approach to defining training zones applies fixed percentages to an individual's estimated maximum heart rate. The traditional formula, calculated as 220 minus the individual's age, has been widely used since the 1970s 778. In standard commercial fitness platforms, Zone 2 is frequently prescribed as 60% to 70% of this estimated maximum heart rate 19.
However, extensive research, including the landmark HUNT Fitness Study, demonstrates that the traditional 220-minus-age formula frequently underestimates true maximum heart rate by up to 20 beats per minute, particularly in adults over the age of 40 8. This inaccuracy causes older individuals to train at intensities that are too low to elicit optimal cardiovascular adaptations. A more robust epidemiological adjustment is the Tanaka formula, calculated as 208 minus 0.7 multiplied by age, which was developed from a comprehensive meta-analysis of 351 studies and provides a much closer baseline for aging populations 778. Alternatively, the Gulati formula (206 minus 0.88 multiplied by age) has been specifically validated for female physiology to address sex-based discrepancies in maximum heart rate estimation 711.
Heart Rate Reserve and the Karvonen Method
While the Tanaka and Gulati formulas offer improvements, fixed percentage methodologies fundamentally fail to account for individual baseline cardiovascular fitness. An untrained individual and a veteran endurance athlete of the exact same age may share the same maximum heart rate but possess vastly different resting heart rates and cardiac stroke volumes. To correct this physiological oversight, exercise physiologists heavily advocate for the Karvonen formula, which utilizes the Heart Rate Reserve (HRR) by factoring in the individual's resting heart rate 7111013.
The Karvonen calculation isolates the active range of the cardiovascular system. It is calculated by subtracting the resting heart rate from the maximum heart rate to find the heart rate reserve. The target heart rate is then determined by multiplying the heart rate reserve by the desired intensity percentage and adding the resting heart rate back to the total 1314. By accounting for resting bradycardia - a common adaptation in fit individuals where the resting heart rate drops significantly - the Karvonen method provides a significantly higher and more accurate Zone 2 ceiling for well-trained athletes, ensuring they receive a sufficient aerobic stimulus 713.
Despite the mathematical superiority of the Karvonen formula over basic age-based percentages, studies tracking wide, heterogeneous populations note that standardized heart rate markers still exhibit high coefficients of variation. Research comparing various methods of determining Zone 2 demarcations revealed that the coefficients of variation range from 6% to 29% across different parameters when compared to actual metabolic responses measured in a laboratory 1116. For example, the HERITAGE Family Study, evaluating 663 subjects across various ages, sexes, and races, concluded that even the Karvonen formula could overestimate heart rates at specific percentages of maximal oxygen uptake, indicating that mathematical formulas cannot perfectly replicate individualized metabolic testing 12.
The Talk Test and Rating of Perceived Exertion
Given the inherent limitations of predictive heart rate formulas, sports medicine often recommends combining objective heart rate targets with qualitative checks, specifically the "talk test" and the Rating of Perceived Exertion (RPE). The upper limit of the five-zone model's Zone 2 corresponds precisely to the physiological threshold where an individual transitions from being able to speak in full, uninterrupted sentences to requiring periodic pauses for breath 67.
At true Zone 2 intensity, breathing becomes rhythmic and slightly effortful, but conversation remains viable 46. This aligns with an RPE of approximately 3 to 4 on a standard 10-point scale, or roughly 10 on the classic Borg 6-to-20 scale 34. If an athlete notices their heart rate drifting upward toward the end of a session (cardiac drift) and they lose the ability to speak comfortably, they have likely crossed the first ventilatory threshold and exited Zone 2, regardless of what their heart rate monitor suggests 67.
Cellular Bioenergetics and Mitochondrial Adaptations
The intense promotion of Zone 2 training within longevity medicine is fundamentally rooted in its unique impact on cellular bioenergetics. Aging, metabolic syndrome, and subsequent chronic diseases are heavily characterized by mitochondrial dysfunction, elevated oxidative stress, and impaired cellular respiration 131415. Sustained endurance training in the upper end of the low-intensity domain acts directly on these precise pathological pathways without imposing the severe systemic autonomic fatigue associated with high-intensity regimens 46.
Substrate Utilization and Fat Oxidation
At the muscular level, endurance training intensity dictates substrate utilization. Zone 2 training specifically recruits Type I (slow-twitch) muscle fibers, which possess the highest mitochondrial density, rely predominantly on oxidative phosphorylation, and are highly resistant to fatigue 6. This specific training intensity aligns closely with "FatMax," the exercise intensity at which the human body achieves its highest absolute rate of fat oxidation 11.
At Zone 2 intensities, the body meets its energy demands primarily through the oxidation of fatty acids rather than the burning of limited muscle glycogen stores 69. This metabolic pathway improves overall metabolic efficiency and decreases insulin resistance, addressing the root causes of numerous metabolic disorders 9. When the intensity increases beyond LT1/VT1 into higher zones, the recruitment of Type II (fast-twitch) muscle fibers increases, leading to a reliance on anaerobic glycolysis, a reduction in fat oxidation, and the subsequent production of higher levels of blood lactate 6.
The Lactate Shuttle and Metabolic Flexibility
Dr. Iñigo San-Millán and Dr. George Brooks have extensively researched the critical intersection of substrate utilization, lactate clearance, and metabolic flexibility - defined as the capacity of skeletal muscle to seamlessly switch between lipid and carbohydrate oxidation in response to varying energy demands 16171819. Their clinical research establishes that highly conditioned endurance athletes, such as professional cyclists, demonstrate vastly superior metabolic flexibility compared to less-fit individuals. These athletes are capable of maintaining high rates of fat oxidation at higher absolute workloads while delaying their reliance on carbohydrate oxidation 1820.
Furthermore, the work of San-Millán and Brooks has fundamentally reframed lactate from its historical characterization as an anaerobic waste product into a vital cellular fuel and signaling molecule. The "lactate shuttle" hypothesis details how lactate produced in glycolytic muscle fibers is continuously transported to highly oxidative Type I fibers, the heart, and the brain, where mitochondria clear it and efficiently convert it into adenosine triphosphate (ATP) 192127.
Zone 2 training provides a maximum aerobic stimulus while keeping the body in a steady metabolic equilibrium, thereby heavily taxing and consequently optimizing the body's lactate clearance mechanisms 27. In this state, energy production precisely matches energy demand; glycolysis supplies substrates at a rate that mitochondria can fully process, and lactate is oxidized and reused without accumulating in the blood 27. Conversely, individuals with metabolic dysfunction, such as type 2 diabetes or profound insulin resistance, exhibit impaired metabolic flexibility. Their systems prematurely shift to carbohydrate oxidation and begin accumulating lactate even at very low physical intensities, signifying mitochondrial insufficiency 172128. Regular Zone 2 training repairs these precise pathways, enhancing the expression of monocarboxylate transporters responsible for moving lactate into the mitochondria, thereby restoring systemic metabolic health 1928.
Mitochondrial Biogenesis Mechanisms
Aerobic exercise mechanically upregulates essential signaling pathways - such as the peroxisome proliferator-activated receptor-γ coactivator-1α (PGC-1α), AMP-activated protein kinase (AMPK), and brain-derived neurotrophic factor (BDNF) - that drive mitochondrial biogenesis and improve neuroplasticity 131415. The resulting morphological adaptations include increased mitochondrial volume density, enhanced mitochondrial fusion and fission dynamics, and elevated mitochondrial protein synthesis, which collectively improve bioenergetic efficiency and clear defective mitochondria via mitophagy 1314.
Continuous, moderate-intensity training has been consistently shown to stimulate significant improvements in cardiorespiratory fitness. Increases in maximum oxygen uptake (VO2 max) and mitochondrial density are readily observed following chronic low-to-moderate intensity regimens 13. Because Zone 2 training strictly limits reliance on anaerobic glycolysis, the accumulation of systemic stress and central nervous system fatigue is heavily minimized. This unique physiological ratio allows athletes and clinical patients to accumulate a massive volume of adaptive stimulus - often measured in hundreds of weekly minutes - that would be biologically impossible to sustain at higher intensities 429.
The Efficacy Debate Regarding Zone 2 Superiority
While elite endurance athletes historically build their foundational aerobic base using vast quantities of Zone 2 training, the direct extrapolation of this professional protocol to the general public has been subject to rigorous recent debate within the exercise physiology community. The specific point of contention is whether Zone 2 is physiologically superior to other intensities for mitochondrial adaptation, or whether it is merely an effective, scalable vehicle for accumulating training volume without overtraining.
Questioning the Optimal Intensity for Mitochondrial Function
Recent popular discourse, heavily amplified by digital media and wellness podcasts, frequently positions Zone 2 as the absolute optimal intensity for improving mitochondrial and fatty acid oxidative capacity 222324. However, a critical 2025 narrative review by Storoschuk, Gibala, and Gurd titled "Much Ado About Zone 2" directly and comprehensively challenged this assertion 2224.
Upon evaluating the available clinical trials comparing varying exercise intensities, the researchers concluded that current evidence does not support the claim that Zone 2 is optimal or superior to higher intensities for improving mitochondrial function 2425. To the contrary, when low-intensity and high-intensity exercise - such as High-Intensity Interval Training (HIIT) or Sprint Interval Training (SIT) - are compared directly at matched volumes, higher intensities reliably trigger more robust molecular stress signals that drive mitochondrial biogenesis 2526. Adaptations in mitochondria occur most robustly when the biological system is pushed beyond its current homeostatic ceiling, typically requiring exertion above 65% of work rate maximum, which exceeds the strict physiological bounds of Zone 2 26.
Contextualizing Volume Constraints for the General Public
The consensus among critical reviews highlights a vital contextual nuance regarding training volume. Zone 2 is highly effective and strategically necessary for elite endurance athletes who train 15 to 25 hours per week. For these athletes, it allows them to maximize cumulative aerobic volume without incurring severe muscular or neurological overtraining 425.
However, for the general public, who generally exercise closer to three to five hours per week, advising them to forgo higher exercise intensities in favor of strict Zone 2 training may inadvertently limit the health benefits of exercise 24. Prioritizing higher intensities is critical to maximizing cardiometabolic health benefits and VO2 max, which remains one of the strongest independent predictors of all-cause mortality and longevity 222425. For individuals with strict time constraints, the exercise pyramid may need to be inverted, prioritizing higher-intensity work that can still be adequately recovered from, rather than spending limited time exclusively in a low-intensity domain 26. Thus, sports medicine increasingly views Zone 2 as a comfortable, accessible foundational layer of a varied program - particularly useful for those who are overweight, diabetic, or unfit - rather than a standalone panacea that replaces the need for intense exertion 25.
Training Intensity Distribution Models
The recognition that high-intensity stimuli are ultimately required for peak longevity adaptations raises the practical question of how to balance differing exercise modalities across a weekly routine to prevent burnout while maximizing physiological gains. Sports medicine heavily evaluates two prevailing models of Training Intensity Distribution (TID): polarized training and pyramidal training.
Polarized Training Architectures
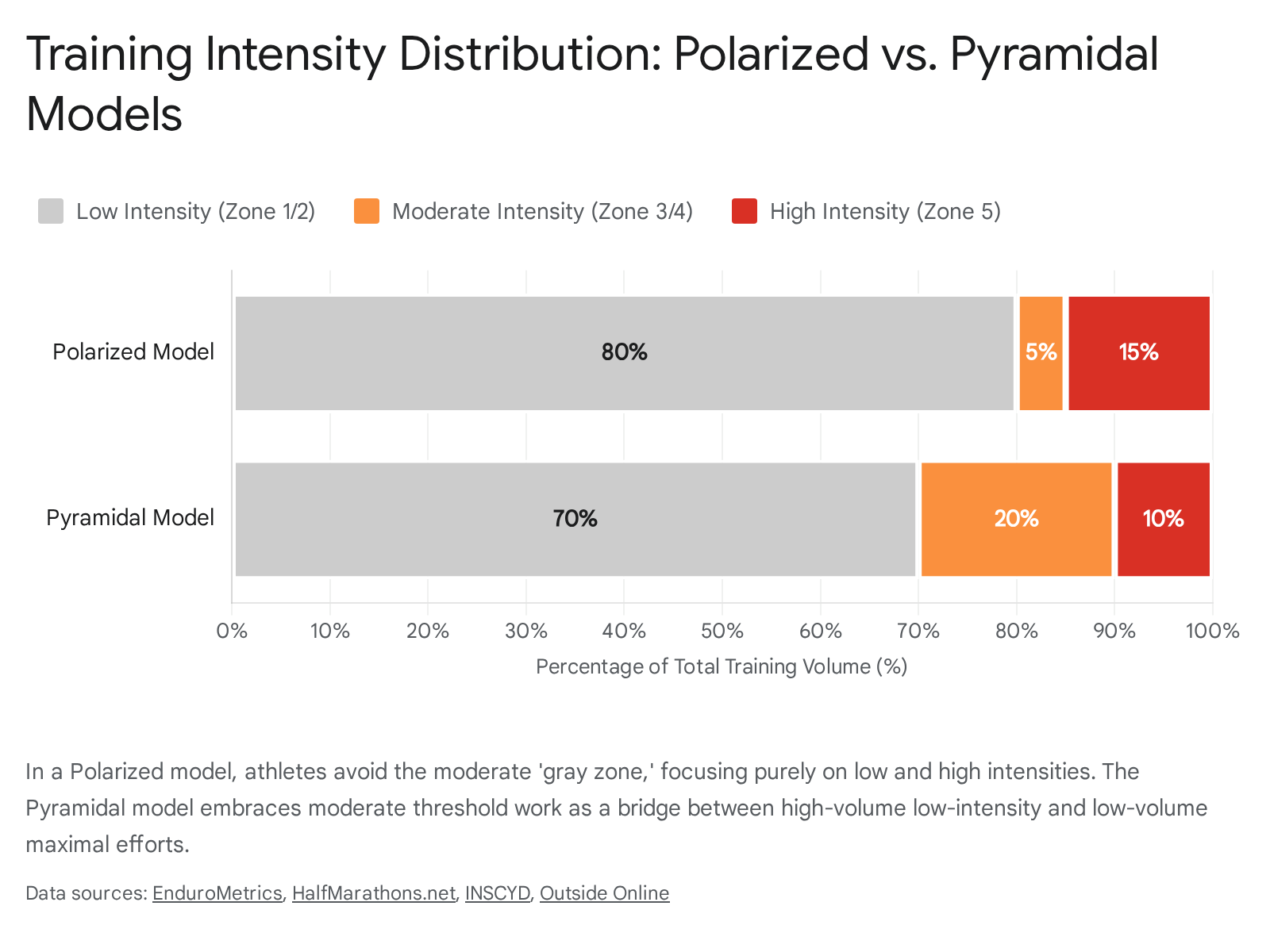
Popularized over the last two decades by researchers such as Dr. Stephen Seiler, the polarized training model is based on extensive observations of how elite endurance athletes distribute their effort. The polarized architecture dictates that approximately 80% of total training time is spent at a very low intensity (Zone 1 in a three-zone model, or Zones 1 and 2 in a five-zone model), and the remaining 20% is spent at a very high intensity (Zone 3 in a three-zone model, or Zones 4 and 5 in a five-zone model) 29272829.
In a strictly polarized model, the "murky middle" - defined as moderate threshold or tempo work - is aggressively avoided 29. The physiological rationale is that moderate threshold work creates nearly as much systemic fatigue and glycogen depletion as high-intensity interval training, but fails to yield the equivalent peak cardiovascular adaptations 429. By keeping easy days truly easy, athletes can fully recover, enabling them to execute their high-intensity interval sessions with maximum power output. Multiple studies indicate that polarized training often yields superior improvements in VO2 max, time to exhaustion, and peak velocity when compared to threshold-heavy, unpolarized regimens 292930. For example, in a study of highly trained endurance athletes over nine weeks, the polarized training group demonstrated a significant 11.7% increase in VO2 max, far outpacing groups focused on threshold or purely high-volume training 29.
Pyramidal Training Architectures
Conversely, the pyramidal training model also allocates the vast majority of volume to low-intensity training (typically 70% to 75%), but it diverges from the polarized model by allocating a moderate amount of time to threshold and tempo work (15% to 20%), and a small peak volume to maximum high-intensity work (5% to 10%) 2730313233. The pyramidal approach builds a literal base of easy endurance, stacked with a middle layer of threshold work to build lactate clearance efficiency, topped with a small amount of VO2 max work 303132.
Comparative Outcomes in Athletic and Recreational Cohorts
When comparing polarized and pyramidal training distributions in recreational and sub-elite populations, randomized controlled trials frequently show statistically identical performance and health outcomes. A 12-week study comparing polarized and pyramidal training in middle-distance triathletes found no significant overall performance differences, with average finishing times over a five-hour race varying by just two seconds between the groups 3042.
Similarly, researchers evaluating recreational runners engaged in very low-volume training have found that strict adherence to the 80/20 polarized rule may not be necessary. An eight-week study by Festa and colleagues evaluated recreational runners performing either a polarized routine or a "focused endurance" routine with a significantly higher proportion of moderate and high-intensity work 43. Because the total training volume was exceptionally low - averaging roughly 30 minutes a day - both groups improved their VO2 max and time-trial performance by roughly equal margins without significant statistical differences 43. This suggests that the polarized 80/20 rule, heavily reliant on vast amounts of Zone 2, becomes increasingly biologically necessary primarily as absolute training volume scales up, protecting athletes from the steady accumulation of neurological and metabolic fatigue 43.
Epidemiological Evidence for Physical Activity and Longevity
The mechanisms explored at the cellular level regarding mitochondrial biogenesis and metabolic flexibility translate seamlessly into robust epidemiological data regarding healthspan and lifespan. Extensive prospective cohort studies confirm that achieving high levels of metabolic health - via the adaptations secured primarily in Zone 2 and supplemented by high-intensity efforts - substantially lowers the risk of all-cause, cardiovascular, and cancer mortality.
Dose-Response Relationships in All-Cause Mortality
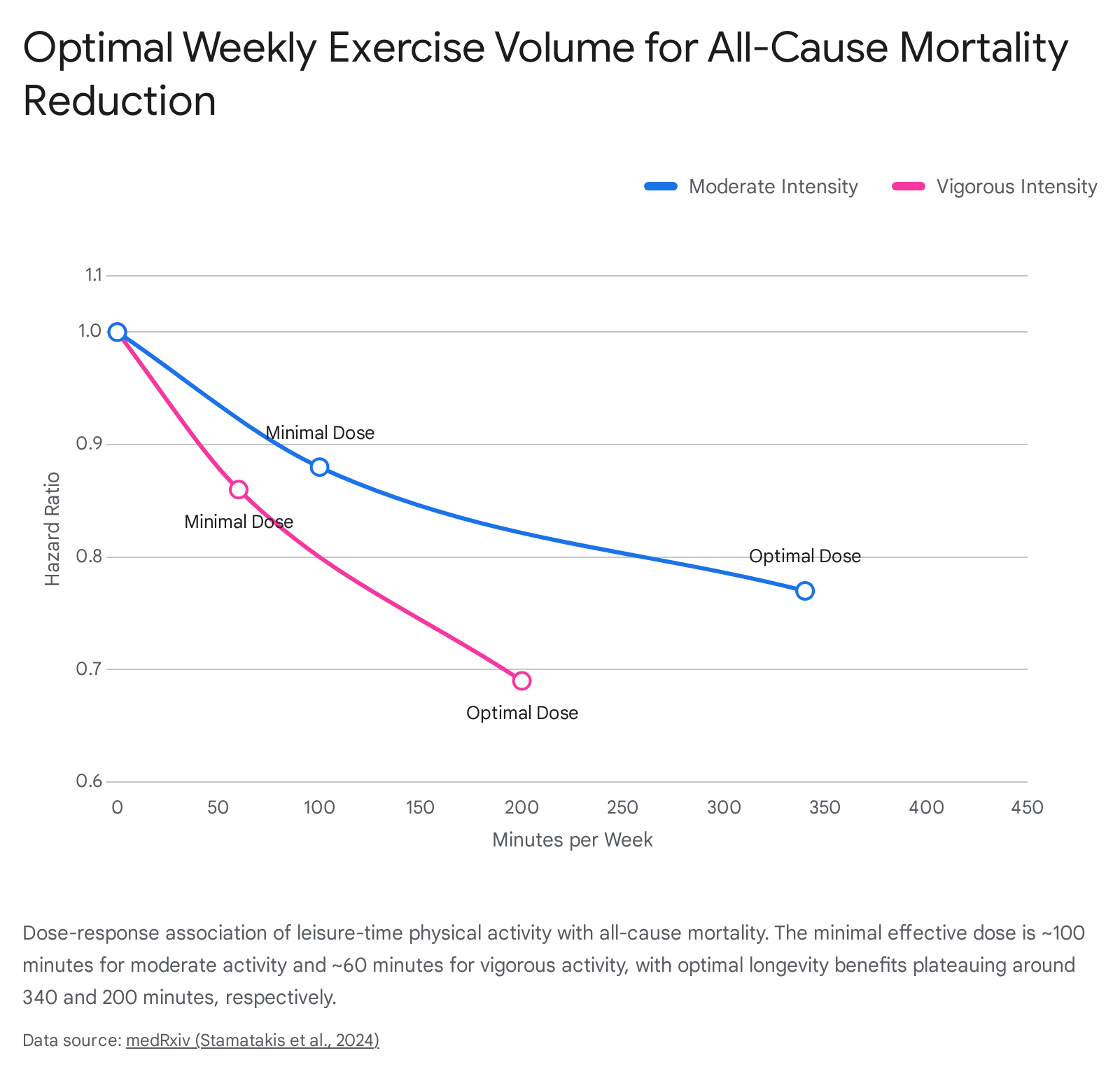
The correlation between physical activity and mortality risk follows a distinct non-linear, L-shaped or U-shaped dose-response curve. Engaging in even minimal amounts of activity yields steep, immediate reductions in mortality for previously sedentary populations, while additional volume provides diminishing but continuous returns up to a specific optimal inflection point, beyond which excessive training yields negligible additional benefits 443435.
An extensive pooled meta-analysis encompassing over 3.36 million participants tracked across 25 cohorts in 17 countries with more than 12 years of follow-up established precise optimal dosing boundaries for both moderate physical activity (analogous to Zone 2) and vigorous physical activity 34. When compared to entirely inactive baseline populations, the analysis revealed the following risk reductions: * The minimal effective dose for vigorous-intensity physical activity was 60 minutes per week, yielding a 14% reduction in all-cause mortality (Hazard Ratio [HR]: 0.86). The optimal longevity benefits maxed out at 200 minutes of vigorous activity per week, achieving a 31% risk reduction (HR: 0.69). * The minimal effective dose for moderate-intensity physical activity was 100 minutes per week, yielding a 12% reduction in mortality (HR: 0.88). The optimal benefits maxed out at roughly 340 minutes per week, delivering a 23% reduction in risk (HR: 0.77) 34.
Maintaining consistent physical activity across the lifespan acts as a powerful prophylactic against chronic disease. In comprehensive meta-analyses encompassing 85 studies, consistently active populations demonstrated approximately a 29% lower risk of all-cause mortality, a 40% reduction in cardiovascular disease mortality, and a 25% reduction in cancer mortality compared to those who remained inactive 36.
Crucially, this mortality protection holds true even for vulnerable clinical populations. For instance, engaging in any form of regular physical activity following a formal dementia diagnosis diminishes subsequent mortality risk by approximately 30%, largely independent of whether the activity is light or vigorous in intensity 37. Similarly, individuals with existing cardiovascular disease experience linear mortality benefits from increased moderate-to-vigorous leisure activity, avoiding the plateau effect generally observed in totally healthy populations 38.
Findings from Longitudinal and Asian Cohorts
Specific national registries confirm these epidemiological patterns across highly varied cultures and lifestyles. Research drawing on Scandinavian databases highlights that the context of physical activity matters just as much as the metabolic intensity. The Tromsø Study in Norway, which examined 29,605 participants over four decades, differentiated between Leisure Time Physical Activity (LTPA) and Occupational Physical Activity (OPA). The study revealed that while moderate and vigorous LTPA were universally associated with significantly lowered all-cause and cardiovascular mortality risks across both sexes, heavy manual labor (very high OPA) did not offer the same robust protection 39. This underscores that the controlled, recovery-conscious nature of structured athletic training is vital to longevity, whereas uncontrolled occupational strain may counteract physiological adaptations.
Asian longitudinal datasets, such as the Korean Longitudinal Study of Aging (KLoSA) and the JAHEAD Japanese cohort, further contextualize the immense lifespan extension available via low-risk lifestyle factors, of which physical exercise is a primary pillar 404142. Among the KLoSA cohorts, fifty-year-old women possessing four to five low-risk lifestyle attributes (including regular physical activity) boasted an impressive 34.4 years of life expectancy entirely free of diabetes, cardiovascular diseases, and cancer, compared to just 23.7 years for those adopting zero low-risk behaviors. Men exhibited similar protection, securing 31.1 years of disease-free life expectancy compared to 23.5 years for inactive cohorts 41. Related findings in Japanese aging cohorts (JAHEAD) indicate that the availability of neighborhood infrastructure promoting safe, lower-intensity Zone 2 physical activity - such as robust access to parks and walkable sidewalks - correlates positively with significantly extended healthy life expectancies 40.
Cardiorespiratory Fitness as a Modifiable Risk Factor
The objective enhancement of cardiorespiratory fitness (CRF), often driven by combinations of Zone 2 and VO2 max training, is intimately linked to long-term health outcomes. A vast study utilizing national registries in Singapore examined 148,825 healthy young men over 1.29 million person-years to understand longitudinal changes in physical fitness. The study found a highly sensitive association: a mere 1% increase in a 2.4-kilometer run time per annum was associated with a 1.13 times greater hazard of experiencing a first major adverse cardiovascular event (MACE) and a 1.06 times greater hazard of all-cause mortality up to two decades later 43.
Interestingly, while CRF is vital, high-intensity intervals are not strictly required for mortality reduction if significant moderate-intensity volume is maintained. The Norwegian Generation 100 study, a randomized controlled trial tracking 1,567 older adults over five years, separated participants into groups performing High-Intensity Interval Training (HIIT) and Moderate Intensity Continuous Training (MICT). The trial recorded an overall mortality rate of 4.6% after five years. Crucially, the overall all-cause mortality did not statistically differ between the combined training groups and the control group following national physical activity guidelines 4445. When analyzed separately, HIIT offered a modest absolute risk reduction of 1.7 percentage points, while MICT showed a slight absolute increased risk of 1.2 percentage points compared to controls, suggesting that accumulating total metabolic equivalent of task (MET) minutes via steady-state work acts as an immensely protective baseline for aging adults, even if pure longevity benefits are marginally elevated by high-intensity inclusions 4445.
Neurological and Brain Aging Metrics
The longevity benefits of endurance training extend well beyond cardiovascular metrics, heavily influencing neuroplasticity and the delay of cognitive senescence. A 2025 study utilizing the UK Biobank database evaluated 16,972 participants utilizing wrist-worn accelerometers and neuroimaging to generate a biological "Brain Age Gap" metric via an ensemble learning approach. The research found that light, moderate, and vigorous physical activities all exhibited a U-shaped relationship with brain aging. Both insufficient physical activity and excessive, unrecoverable training volumes adversely impacted brain aging. Engaging in moderate amounts of physical activity - characteristic of standard Zone 2 endurance prescriptions - was associated with the optimal slowing of biological brain age 44.
The Synergistic Role of Resistance Training
While Zone 2 is frequently heralded as the principal component of aerobic conditioning and metabolic health, modern sports medicine experts uniformly advocate a holistic training paradigm where low-intensity endurance serves as the foundation of a broader, multi-faceted protocol. Exclusive adherence to Zone 2 aerobic training ignores structural, neuromuscular, and top-end cardiovascular adaptations that are absolutely critical in the later decades of life.
The physiological limitations of aging extend beyond mitochondrial dysfunction to include sarcopenia (the age-related loss of muscle mass) and dynapenia (the loss of muscle strength and power output). Epidemiological reviews overwhelmingly confirm that the inclusion of regular resistance training provides substantial, independent longevity benefits that stack synergistically with the cardiovascular adaptations achieved through aerobic training 4647.
Non-Linear Dose-Response in Muscle Strengthening
A massive systematic review and meta-analysis of ten prospective cohort studies examining nonclinical adult populations isolated the specific, independent effects of muscle strengthening on mortality risk. The aggregated data confirmed that undertaking any amount of resistance training reduced the risk of all-cause mortality by 15%, cardiovascular disease mortality by 19%, and cancer-specific mortality by 14%, compared to cohorts performing zero resistance training 464861.
Unlike aerobic Zone 2 training, which rewards hundreds of weekly minutes of volume with continuous (albeit diminishing) returns, resistance training exhibits a starkly non-linear dose-response curve for longevity outcomes. A maximum mortality risk reduction of 27% in all-cause mortality is observed at merely 60 minutes of total resistance training per week 464861. Mortality risk reductions aggressively plateau, and may even slightly diminish due to orthopaedic or systemic stress, at higher resistance training volumes 464861. Therefore, combining approximately 60 minutes of weekly resistance training with 150 to 300 minutes of Zone 2 endurance exercise provides a comprehensive, optimized, and heavily evidence-based prescription for extending human healthspan and delaying the onset of chronic cardiometabolic decline.
Synthesis of the Longevity Prescription
The convergence of cellular biology, exercise physiology, and vast epidemiological cohort studies establishes a clear, nuanced paradigm for physical longevity. Zone 2 training, strictly defined as aerobic exertion occurring below the first physiological lactate threshold, is unparalleled in its ability to generate high volumes of metabolic stimulus without incurring detrimental systemic fatigue. By heavily taxing the lactate shuttle, maximizing fat oxidation, and upregulating the pathways responsible for mitochondrial biogenesis, Zone 2 effectively corrects the cellular dysfunctions that underpin modern chronic diseases such as type 2 diabetes and metabolic syndrome.
However, sports medicine increasingly recognizes that Zone 2 is not a standalone remedy. While it is the essential aerobic foundation utilized by elite athletes in polarized training models, the general public must balance limited training time by inverting the pyramid to include higher-intensity stimuli that maximize peak cardiorespiratory fitness (VO2 max). When Zone 2 endurance work is harmoniously paired with brief bouts of high-intensity aerobic intervals and a baseline of weekly resistance training, individuals secure the complete spectrum of physiological adaptations - cardiovascular, metabolic, and neuromuscular - required to dramatically extend disease-free life expectancy.