How Loneliness Affects Your Physical Health
Loneliness and social isolation are not merely emotional states, but biological conditions that trigger measurable, systemic changes in the human body, increasing the risk of premature death by up to 32%. Research indicates that chronic social disconnection drives systemic inflammation, alters gene expression to suppress antiviral immunity, and dramatically elevates the risk of cardiovascular disease and cognitive decline. While targeted psychological therapies and community-level public health policies can mitigate these effects, biological markers suggest that reversing the physical damage of chronic loneliness requires sustained, multifaceted interventions that address both the individual and their environment.
The Anatomy of an Epidemic: Defining the Crisis
Historically viewed as a private emotional struggle or a natural consequence of aging, loneliness has recently been reclassified by major medical and geopolitical bodies as a severe, structural public health crisis. The impact of social disconnection extends far beyond individual distress; it compromises community resilience, reduces economic productivity, and places an enormous burden on healthcare systems globally.
In June 2025, the World Health Organization (WHO) Commission on Social Connection released a landmark flagship report revealing that one in six people worldwide - approximately 17% of the global population - experienced actionable levels of loneliness between 2014 and 2023 123. This epidemic is responsible for an estimated 871,000 deaths annually, which equates to roughly 100 deaths every hour 34. The economic fallout is similarly staggering. The U.S. Surgeon General's 2023 advisory noted that social isolation among older adults accounts for an estimated $6.7 billion in excess Medicare spending annually, driven largely by increased hospital and nursing facility utilization 5.
The Subjective vs. Objective Divide
To understand how social disconnection damages human health, epidemiologists and psychologists strictly differentiate between the subjective experience and the objective state of being alone. Treating them as identical concepts obscures their distinct biological and psychological pathways. A person can be highly socially integrated and still experience profound loneliness, just as an individual living alone may feel completely fulfilled and socially secure 267.
The scientific literature generally separates these phenomena into three distinct constructs, each carrying its own independent mortality risk:
| Construct | Clinical Definition | Biological Pathway Focus | Mortality Risk Increase |
|---|---|---|---|
| Living Alone | A binary indicator of residential status (single-person household) without regard for external social networks. | Reduced immediate physical assistance and monitoring. | 32% (OR 1.32) |
| Social Isolation | An objective deficit in social network size, infrequent social interactions, or lack of societal participation. | Reduced exposure to socially-transmitted pathogens; lower access to resources. | 29% (OR 1.29) |
| Loneliness | The subjective, distressing emotion arising from a discrepancy between a person's desired and actual social relationships. | Chronic "fight-or-flight" stress response; altered gene expression. | 26% (OR 1.26) |
Data source: Holt-Lunstad et al., 2015 meta-analytic review 89. Odds Ratios (OR) represent the increased likelihood of mortality, statistically controlling for baseline health and confounding variables.
While all three constructs elevate mortality risk, their impacts vary across different populations. For example, recent analyses utilizing the U.K. Biobank demonstrated that objective social isolation ranks higher than subjective loneliness in predicting all-cause, cancer-related, and cardiovascular mortality among individuals with clinical obesity 101112.
The Global Demographics of Disconnection
The demographic breakdown of this crisis challenges long-held stereotypes. While loneliness is frequently associated with older adults - and indeed, up to one-third of older adults experience objective social isolation - the highest rates of subjective loneliness are currently reported among adolescents and young adults 413. Globally, between 17% and 21% of individuals aged 13 to 29 report feeling lonely, with the highest rates clustered among teenagers 2413.
Furthermore, geographic and economic disparities are stark. The WHO report highlights that loneliness is twice as prevalent in low- and middle-income countries, affecting 24% of the population, compared to 11% in high-income nations 24. Regionally, Africa and the Eastern Mediterranean report the highest rates of loneliness at 24% and 21% respectively, followed by Southeast Asia at 18% 1. These figures reflect the disruptive impacts of rapid urbanization, shifting family structures, digital displacement, and inadequate social infrastructure in the Global South 21416.
Marginalized groups face compounded risks. Immigrants, refugees, ethnic minorities, and LGBTQ+ individuals living in high-income countries are particularly vulnerable to social isolation due to language barriers, discrimination, deprived neighborhood environments, and weakened cultural norms 115.
Quantifying the Mortality Risk
The foundational evidence linking social relationships to human survival crystallized over the last two decades. In a landmark 2010 meta-analysis of 148 longitudinal studies involving over 308,000 participants, researchers Julianne Holt-Lunstad and colleagues found that individuals with strong, adequate social relationships had a 50% greater likelihood of survival over an average 7.5-year follow-up period compared to those with weak social ties 16171819.
This finding remained remarkably consistent regardless of the participant's age, sex, initial health status, or cause of death, suggesting that social connection is a universal human biological imperative rather than a secondary lifestyle factor 181920.
Deconstructing the "15 Cigarettes a Day" Statistic
The most pervasive and widely quoted statistic in public health discussions regarding loneliness is that it is "as dangerous as smoking 15 cigarettes a day." This powerful analogy was utilized heavily by the U.S. Surgeon General and global media following the release of national advisories 21242223.
The statistic originates directly from the 2010 Holt-Lunstad meta-analysis, which benchmarked the effect size of lacking social connection (an odds ratio of 1.50 for survival) against other well-established mortality risk factors 1727. The data indicated that the mortality risk of severe social disconnection roughly equals the risk of smoking up to 15 cigarettes daily, and notably exceeds the independent mortality risks associated with physical inactivity, clinical obesity, and air pollution 19222327.
However, public health experts and sociologists urge caution in how this analogy is applied. A 2023 critique published in the American Journal of Epidemiology argued that while the mortality claim is mathematically sound, the cigarette metaphor risks oversimplifying the evidence 28. Smoking is ultimately an individual behavioral choice that can be targeted with clinical cessation programs, pharmaceutical interventions, and taxation. Loneliness, conversely, is a highly structural phenomenon 28. It is produced by systemic factors - such as car-dependent urban design, the transition to remote work, the erosion of "third spaces" like community centers, and socioeconomic inequality 228. Framing loneliness as a personal lifestyle failure akin to smoking obscures the societal infrastructure that generates it.
The Biological Mechanisms of Loneliness
The translation of a psychological state - the distress of feeling lonely - into severe physiological damage and early mortality operates through deeply embedded evolutionary pathways. Loneliness is not merely a feeling of sadness; it is an alarm bell signaling a threat to survival.
Evolutionary Origins: Social Safety Theory
From an evolutionary biology perspective, social isolation historically equated to physical vulnerability. For early hominids, being separated from the protective perimeter of the tribal group increased the likelihood of physical trauma, wounding by predators, and subsequent bacterial infection 2425. Simultaneously, an isolated individual was highly unlikely to encounter a socially transmitted virus, as viruses require close human-to-human contact to spread 2425.
Consequently, the human body evolved to adapt to perceived social isolation by fundamentally altering how the immune system operates. When the brain perceives a state of loneliness, it anticipates physical wounding and prepares the body accordingly. It does this by altering the transcription of genes in immune cells - a phenomenon known as the Conserved Transcriptional Response to Adversity (CTRA) 262728.
The Conserved Transcriptional Response to Adversity (CTRA)
The CTRA is the biological bridge between the social environment and cellular health.
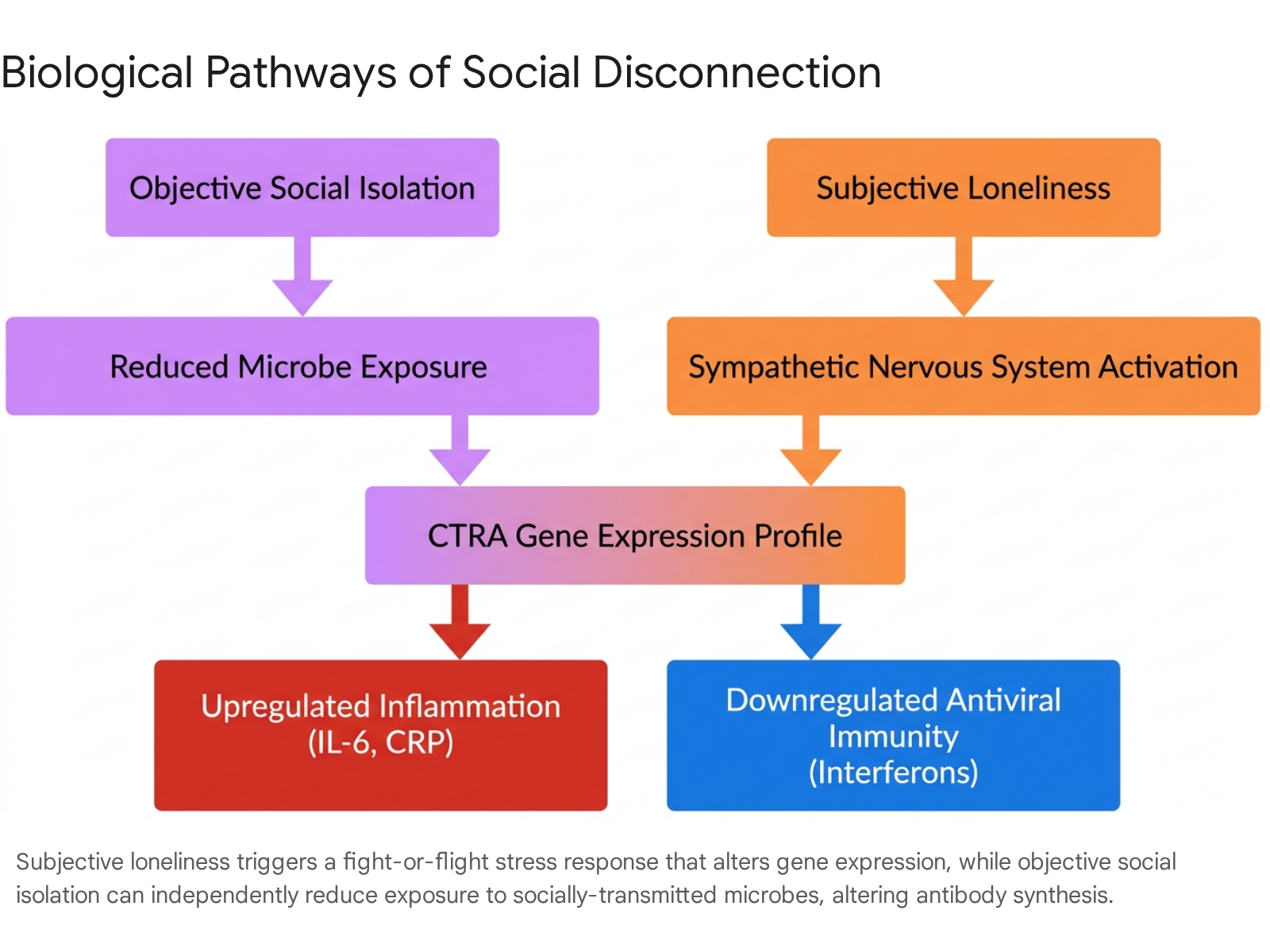
When an individual feels lonely, the brain perceives a social threat and triggers a "fight-or-flight" stress signal via the sympathetic nervous system 2829. This sympathetic activation floods the body with norepinephrine, a neurotransmitter that travels to the bone marrow and stimulates the production of immature monocytes (a type of white blood cell) 2528.
These immature immune cells are pre-programmed to express the CTRA profile, which is characterized by two simultaneous and dangerous actions: 1. Up-regulation of pro-inflammatory genes: The cells increase the expression of pro-inflammatory transcription factors (like NF-κB). The body is pre-emptively flooding the system with inflammation to heal expected physical wounds and fight off bacterial infections 242527. 2. Down-regulation of antiviral genes: The cells suppress their defense against viruses, specifically down-regulating Interferon Response Factors (IRFs) and genes related to IgG1 antibody synthesis. The evolutionary logic dictates that if you are alone, you do not need to waste biological energy fighting a socially transmitted virus you will never encounter 252829.
While this biological shift was highly adaptive in ancestral environments where physical trauma was a daily threat, it is profoundly maladaptive in the modern world. Modern social isolation rarely results in a tiger attack, but it does leave the body trapped in a persistent state of low-grade, chronic inflammation, while simultaneously rendering the individual highly vulnerable to viral infections 242527.
Chronic Inflammation: The Roles of IL-6 and CRP
The cellular activation of the CTRA profile manifests in the human bloodstream through elevated inflammatory biomarkers. Prolonged inflammation is a known precursor to autoimmune disorders, arthritis, diabetes, and heart disease 30.
A comprehensive 2020 meta-analysis examining the link between social disconnection and systemic inflammation confirmed a robust and consistent association between subjective loneliness and elevated levels of Interleukin-6 (IL-6), a primary pro-inflammatory cytokine 736.
However, findings regarding acute-phase proteins like C-reactive protein (CRP) and fibrinogen demand a more nuanced interpretation. Some longitudinal studies and ecological momentary assessments of older adults clearly demonstrate that acute loneliness is associated with higher basal levels of CRP 373139. Furthermore, multi-cohort studies have found that socially isolated individuals possess 24% higher levels of suPAR, a biomarker reflecting deeply embedded chronic systemic inflammation, with effects persisting from childhood social isolation into mid-adulthood 32.
Yet, broad systematic reviews suggest that elevated CRP and fibrinogen are often more reliably correlated with objective social isolation rather than subjective loneliness in fully adjusted models 736. Regardless of the specific marker, the biological consensus is clear: lacking social connection keeps inflammatory signals chronically activated. Over time, these proteins stop protecting the body and begin damaging blood vessels, accelerating atherosclerosis, and promoting cellular aging by shortening telomeres 39.
Downstream Health Consequences
The downstream effects of chronic inflammation and sympathetic nervous system overdrive manifest in severe clinical outcomes, drastically reducing both healthspan and lifespan.
Cardiovascular Disease and Metabolic Syndrome
The cardiovascular system bears the brunt of loneliness-induced biological stress. Chronic loneliness elevates blood pressure, increases arterial stiffness, and interferes with insulin sensitivity 39. Consequently, individuals with poor social connection face a 29% increased risk of coronary heart disease and a 32% increased risk of stroke 53334.
The intersection of loneliness and clinical obesity is particularly lethal. Obesity itself drives metabolic disorders, chronic inflammation, and cardiovascular disease 1135. However, a large-scale analysis of nearly 400,000 U.K. Biobank participants revealed that social isolation and loneliness are significantly more prevalent among obese individuals, acting as major amplifiers of mortality 1136. Crucially, the data demonstrated that obese individuals with the lowest baseline levels of loneliness and isolation had a 29% and 15% lower excess risk of obesity-related cardiovascular events, respectively, compared to their highly isolated peers 36. This indicates that mitigating loneliness can actually attenuate the cardiovascular dangers of obesity 1012.
Cognitive Decline and the Dementia Paradox
Neurologically, loneliness has long been associated with devastating outcomes. The U.S. Surgeon General's report highlights that loneliness is associated with an estimated 50% increased risk of developing dementia in older adults 52333. The chronic inflammation triggered by loneliness reduces neuroplasticity, while elevated cortisol levels damage delicate brain structures over time, accelerating cognitive decline 3945.
However, the specific neurobiological pathways linking loneliness to dementia are complex and highly contested. A rigorous 2025 study utilizing data from the Baltimore Longitudinal Study on Aging and the UK Biobank tested whether loneliness was associated with actual Alzheimer's disease neuropathology in dementia-free adults 37. The researchers examined plasma neurobiomarkers for amyloid (Aβ42/Aβ40), phosphorylated tau (pTau181), and glial fibrillary acidic protein (GFAP), as well as PET-based imaging of amyloid and tau in the brain 37.
The results were striking: loneliness was unrelated to all measures of specific Alzheimer's disease pathology, axonal damage, or astrogliosis 37. This unexpected null finding suggests a vital clinical distinction. The 50% increased dementia risk associated with loneliness may not be driven by the accumulation of Alzheimer's-specific plaques and tangles. Instead, the risk is likely driven by vascular dementia (resulting from loneliness-induced hypertension and micro-strokes), depression, or cognitive disuse stemming from a lack of enriching social stimuli 4537.
Evidence-Based Interventions: What Actually Works?
Because loneliness operates simultaneously on psychological, behavioral, and molecular levels, mitigating its effects requires highly targeted interventions. Meta-analyses of decades of intervention efficacy reveal a counterintuitive truth: simply putting lonely people in a room together (pure social facilitation) often fails to resolve chronic loneliness 3839.
When an individual has been lonely for an extended period, their brain becomes hyper-vigilant to social threat 4050. They begin to anticipate rejection, behave defensively, and interpret neutral social cues as hostile. This maladaptive social cognition creates a self-fulfilling cycle where the lonely individual subconsciously pushes others away, deepening their isolation 40.
Psychological and Cognitive Therapies
The most consistently effective interventions for reducing loneliness are psychological therapies - specifically cognitive behavioral therapy (CBT) designed to identify and rewire these maladaptive social cognitions 384041. A comprehensive 2025 rapid review of 101 interventions across all age groups found that psychological interventions yielded the largest effect size (Standardized Mean Difference = -0.79) in reducing subjective loneliness 41. By teaching individuals to critically evaluate their assumptions about social interactions, therapists can dismantle the psychological barriers preventing genuine connection.
Group-Based and Skill-Building Programs
Programs that involve structured group activities, volunteering, and skill-building (such as community gardening, continuing education, or animal-assisted activities) show strong, moderate effectiveness (SMD = -0.50) 3841. These interventions succeed because they provide a shared sense of purpose and structure. By focusing on a joint task, these programs bypass the intense pressure of direct socialization, allowing organic bonds to form while alleviating the anxiety associated with unstructured mingling 3938.
The Limitations of Digital Health Interventions
Digital health interventions (DHIs) - such as befriending apps, internet training for seniors, or social media groups - show highly mixed and modest results 4243. A 2025 systematic review of randomized controlled trials targeting older adults found that while DHIs can marginally reduce loneliness scores (SMD = -0.39) and temporarily improve mental health, the effects are often context-dependent and short-lived 43. While digital tools proved vital during the acute isolation of the COVID-19 pandemic, evidence suggests they are inadequate substitutes for in-person connection and can sometimes exacerbate feelings of exclusion if not paired with physical community integration 2443.
Novel Biological and Pharmacological Interventions
Emerging psychoneuroimmunology research is exploring whether the biological cycle of loneliness can be interrupted pharmacologically. Because loneliness drives inflammation, and inflammation induces "sickness behavior" (lethargy and social withdrawal), researchers theorized that reducing inflammation might organically improve social outcomes 44.
In a pioneering randomized controlled trial, healthy adults experiencing high loneliness were given either a placebo or Naproxen (a common non-steroidal anti-inflammatory drug) daily for two weeks 44. While the anti-inflammatory medication did not directly reduce overall loneliness scores for the general sample, it significantly reduced loneliness and increased affiliative behavior during social interactions specifically in participants who had high baseline depressive symptoms 44. Similarly, a 2026 meta-analysis found that anti-inflammatory treatments modestly reduce anhedonia and depressive severity in patients with elevated CRP levels 45.
Furthermore, research indicates that the harmful cellular changes of loneliness are reversible through specific types of social engagement. Longitudinal studies of adults demonstrate that cultivating "positive relations with others" - characterized by warmth, trust, and mutual support - significantly down-regulates the harmful CTRA inflammatory gene expression profile, above and beyond simply reducing the subjective feeling of loneliness 2646.
The Public Health and Policy Response
Recognizing that loneliness cannot be solved entirely in a therapist's office, governments are increasingly treating social infrastructure as a critical public health asset requiring structural policy changes.
At the national level, several countries have pioneered legislative approaches to combat isolation 4758. In 2018, the United Kingdom became the first nation to appoint a Minister for Loneliness, spearheading "social prescribing" initiatives where doctors can formally prescribe community activities rather than medication 47484950. Japan followed suit in 2021, driven by rising suicide rates and the phenomenon of isolated elderly deaths, eventually enacting the world's first comprehensive Act on the Advancement of Measures to Address Loneliness and Isolation in April 2024 475163.
In the United States, the Surgeon General released an exhaustive advisory in 2023 declaring a national epidemic and establishing a National Strategy to Advance Social Connection 2152. The unprecedented framework operates on six pillars: 1. Strengthening Social Infrastructure: Designing built environments (parks, libraries, public transit) that naturally facilitate human interaction 5354. 2. Enacting Pro-Connection Public Policies: Adopting a "connection-in-all-policies" approach, such as paid family leave, to ensure societal structures do not mandate isolation 5354. 3. Mobilizing the Health Sector: Integrating loneliness screening into routine primary care and expanding public health surveillance 53. 4. Reforming Digital Environments: Requiring data transparency and establishing safety standards to prevent technology from displacing real-world connection 53. 5. Deepening Knowledge: Funding continuous research on the effectiveness of interventions 33. 6. Cultivating a Culture of Connection: Promoting societal values of mutual respect and service 3367.
Globally, the WHO Commission on Social Connection is currently executing a three-year mandate (2024 - 2026) to elevate social health to the exact same priority level as physical and mental health 142355. The Commission emphasizes the urgent need for cross-border knowledge sharing, particularly to assist the Global South in developing culturally sensitive interventions that protect vulnerable populations as global demographics shift 3161549.
Bottom line
Loneliness is a profound biological stressor that elevates the risk of systemic inflammation, cardiovascular disease, and all-cause mortality to levels comparable with heavy smoking and obesity. While objective social isolation and subjective loneliness operate through slightly distinct mechanisms, both trigger measurable immune dysregulation, most notably the Conserved Transcriptional Response to Adversity (CTRA), which suppresses viral immunity while driving chronic inflammation. Reversing this damage requires a dual approach: shifting public policy to rebuild the built environment and community infrastructure, while simultaneously deploying clinical, cognitive interventions that address the maladaptive social cognitions maintaining chronic loneliness. However, uncertainties remain regarding the exact role loneliness plays in specific neurodegenerative diseases like Alzheimer's, highlighting the need for continued, long-term, biomarker-driven research to untangle the complex web of social disconnection and physiological decay.