How Extreme Heat Increases Hospital Risk
Extreme heat acts as a systemic stressor that triggers a cascade of organ failures, flooding emergency departments with metabolic, renal, and psychiatric crises far beyond simple heatstroke. Epidemiological data demonstrates that this surge systematically overwhelms hospital capacity, leading to a massive spike in excess mortality when critical care limits are breached.
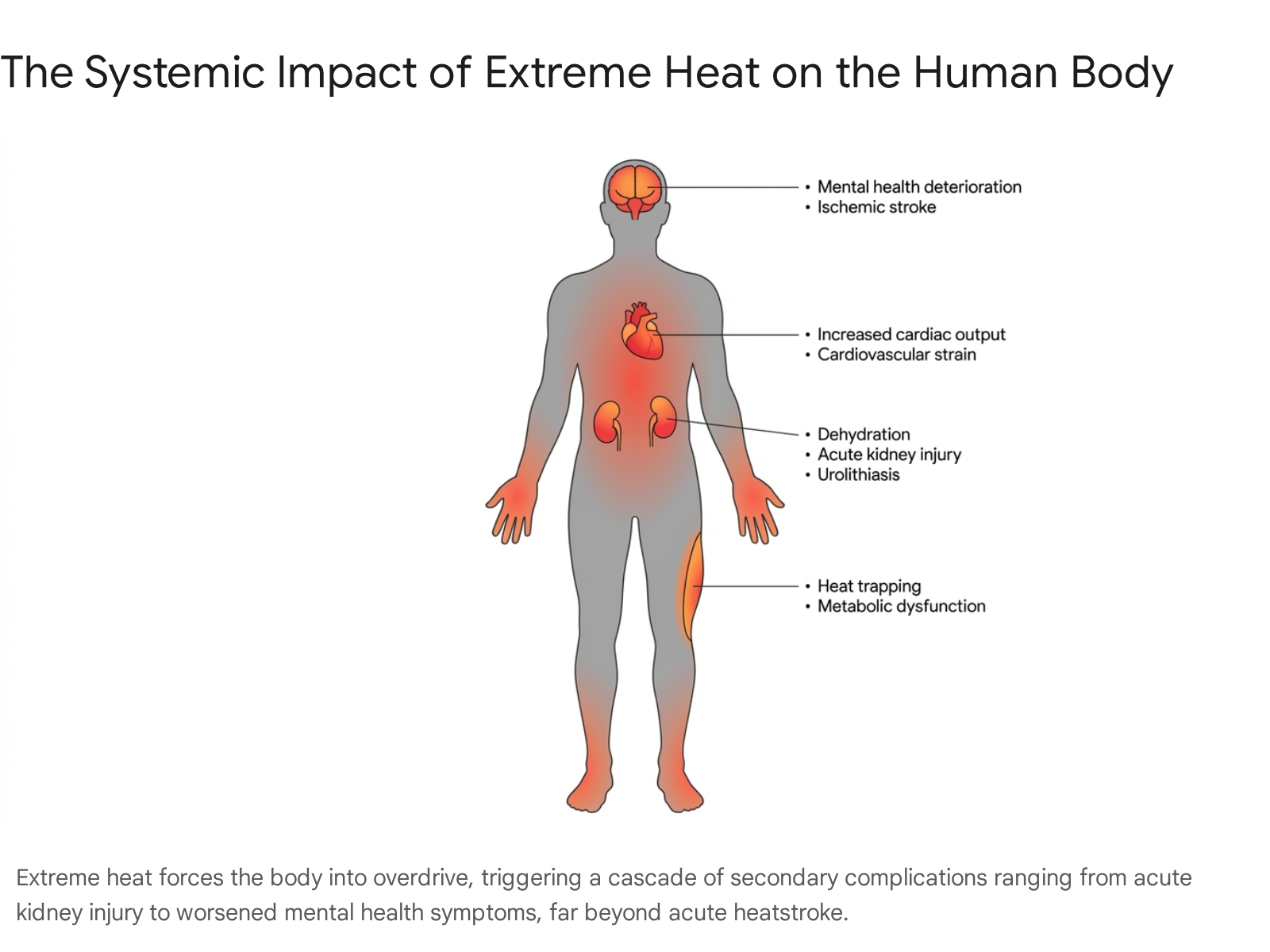
The heatwave illusion: Moving beyond heatstroke
When record-breaking temperatures blanket a region, public attention instinctively turns to heatstroke and dehydration. While heatstroke is a severe and acute medical emergency with a high case fatality rate, it represents only a fraction of the hospitalizations triggered by a heatwave. A deep dive into global hospital admission data reveals that extreme ambient heat acts as a systemic stressor, exploiting preexisting physiological vulnerabilities across almost every major organ system.
An exhaustive analysis of 11.2 million emergency hospital admissions in Spain over a 13-year period paints a detailed picture of this physiological breakdown 12. The diseases most heavily impacted by extreme summer temperatures are not traditional heat illnesses. Instead, the risk of hospital admission for metabolic disorders and obesity-related complications nearly doubles on the hottest days 123.
The biology behind this phenomenon is well-documented. In a healthy physiological response, the human body regulates its internal thermostat through vasodilation (widening blood vessels to push heat to the skin) and sweating. However, in individuals with metabolic disorders or high body fat, these responses are severely blunted. Adipose tissue acts as a potent insulator, trapping heat inside the core, while metabolic dysfunction prevents blood vessels from dilating effectively to release that heat 23.
Beyond metabolic conditions, heatwaves trigger a surge in emergency admissions for acute kidney failure, urinary tract infections, sepsis, and urolithiasis (kidney stones) 14. When the body sweats profusely in an attempt to cool down, it rapidly loses fluid. Without adequate and continuous rehydration, overall blood volume drops. This forces the kidneys to filter highly concentrated, toxin-rich blood, establishing a direct dehydration pathway that drives the sharp increase in acute renal injuries 14.
Cardiovascular and respiratory systems face similar, often fatal, strains. The sheer effort required to pump blood to the skin surface places immense demand on the heart, triggering ischemic strokes and heart attacks 4. Simultaneously, extreme heat often traps atmospheric pollutants - like ground-level ozone and particulate matter (PM2.5) - close to the ground, creating dangerous smog that severely exacerbates asthma, bronchitis, and chronic obstructive pulmonary disease (COPD) 55.
Demographic divides: Who is filling the emergency rooms?
The burden of extreme heat is not distributed equally. Epidemiological syndromic surveillance consistently identifies stark demographic divides in who requires emergency hospitalization when temperatures spike.
Age is the most significant physiological risk factor. Hospital admissions overwhelmingly skew toward the two extremes of life: infants under one year of age and adults over 85 26. Infants lack fully developed thermoregulatory systems and cannot independently hydrate or seek cooler environments. Conversely, the elderly naturally lose the physiological ability to sweat efficiently, often suffer from compounding chronic illnesses, and may have limited mobility 7. In Europe, during the lethal 2024 heatwaves, the heat-related mortality rate for individuals over 75 was calculated to be a staggering 323% higher than all other age groups combined 8.
However, emergency department (ED) visit data reveals a different trend for morbidity (illness) compared to mortality (death). According to the U.S. Centers for Disease Control and Prevention (CDC), during the 2023 warm season, the highest rate of heat-related illness ED visits was actually among adults aged 18 to 64 911. Specifically, those aged 26 to 54 experienced a high visit rate of 222 per 100,000 ED visits 9. This is heavily correlated with occupational exposure, as working-age adults - particularly those in agriculture, construction, and delivery - are disproportionately exposed to ambient heat during peak daylight hours.
Gender also plays a nuanced, scientifically documented role in heat vulnerability. During peak heat days, men demonstrate a significantly higher risk of hospitalization for trauma, injuries, and occupational accidents 25. Women, however, show a significantly higher risk of hospital admission for parasitic, endocrine, metabolic, respiratory, and urinary diseases 2. Researchers suggest this is partially because women generally have a higher core temperature threshold before their bodies trigger the sweating mechanism, slightly delaying the onset of natural evaporative cooling 3. Furthermore, because women tend to live longer than men on average, a higher proportion of women occupy the most vulnerable, elderly age brackets 8.
| Disease/Risk Category | Primary Demographic Affected | Physiological & Environmental Mechanisms |
|---|---|---|
| Metabolic & Obesity | All ages | Adipose tissue insulates the core; blood vessels fail to dilate efficiently to release heat 12. |
| Renal & Urinary | Women, Elderly | Severe fluid loss via sweat concentrates toxins in the blood, leading to kidney injury and urolithiasis 14. |
| Mental Health | Psychiatric patients | Heat severely disrupts sleep and cognitive function; common psychotropic medications disable sweating 10. |
| Respiratory | Elderly, Children | Heat traps ground-level ozone and particulate matter, triggering acute asthma and COPD exacerbations 55. |
| Trauma & Injuries | Men, Outdoor workers | Fatigue and cognitive decline lead to a spike in occupational and vehicular accidents 210. |
The hidden psychiatric toll of rising temperatures
One of the least discussed but most alarming drivers of heat-related hospital visits is the sudden deterioration of mental health. Prolonged heat severely disrupts sleep architecture, leaving individuals chronically fatigued and cognitively impaired. A vast body of research demonstrates a 10% increase in mental health-related emergency department admissions during periods of sustained heat 10.
The direct impact on psychiatric mortality is even more severe. Epidemiological studies conducted across the U.S. and Mexico indicate that suicide risk doubles when ambient temperatures reach 32°C (89.6°F) compared to a baseline of 22°C (71.6°F) 10. Heat also causes a measurable decline in cognitive function - studies note that individuals in hot environments perform up to 13% worse on cognitive processing tests and exhibit significantly slower reaction times, which also contributes to the spike in physical accidents 10.
This psychiatric crisis is heavily compounded by pharmacology. Millions of individuals globally rely on daily psychiatric medications, including SSRIs (antidepressants), antipsychotics, and mood stabilizers. Many of these medications inherently interfere with the brain's hypothalamus or have anticholinergic effects, which effectively blunt the body's ability to sense heat or generate sweat 10. During a heatwave, these life-saving medications transform into dangerous liabilities, silently accelerating the path to hyperthermia for highly vulnerable patients who may not realize their core temperature is rising.
Epidemiology 101: Making sense of "excess mortality"
When a sudden natural disaster strikes, the death toll is usually direct and highly visible. Heatwaves, however, kill quietly behind closed doors. To understand the true scale of a heatwave, epidemiologists do not rely solely on hospital discharge codes; instead, they utilize a vital statistical metric known as "excess mortality."
Excess mortality measures the difference between the total number of deaths observed during a specific period (such as a two-week July heatwave) and the historical baseline of deaths that would be expected if that heatwave had never occurred 1112. This metric is crucial because medical examiners rarely write "heat exposure" on a death certificate. If an elderly patient with preexisting heart disease suffers a fatal myocardial infarction on a 40°C day because their heart could not handle the thermoregulatory strain, the official cause of death will likely be recorded as cardiovascular failure 1113. By calculating excess all-cause mortality, public health officials capture the true, invisible ripple effect of the heat.
Different statistical models yield slightly different estimates, but the overarching trend is clear. A study examining excess mortality in the Veneto region of Italy during the pandemic utilized various forecasting models, including Seasonal Autoregressive Integrated Moving Average (SARIMA) and Generalized Estimating Equations (GEE) 13. The study found that simply comparing current deaths to a five-year historical average can sometimes underestimate the true burden if pre-existing downward trends in mortality (like dropping cardiovascular death rates) are not accounted for. When sophisticated GEE models are applied to weather data, the true lethality of heatwaves comes into sharp focus 13.
The numbers revealed by excess mortality tracking are staggering. Between 2000 and 2019, an estimated 489,000 heat-related excess deaths occurred annually worldwide 7. When researchers look closely at recent regional data, the hidden toll is undeniable. During the summer of 2024, Europe recorded over 62,700 heat-related deaths, a 23% increase compared to 2023 8. By encompassing deaths from all causes, excess mortality bypasses the inconsistencies in hospital coding and exposes extreme heat for what it is: a systemic, mass-casualty killer.
The "credit limit" of hospital capacity
The surge in physiological distress caused by heatwaves leads to a secondary, systemic crisis: the physical and operational breakdown of hospital infrastructure. Modern healthcare systems are designed to run efficiently, which often means they operate with very little spare capacity.
In financial economics, taking on debt works perfectly fine until a consumer crosses their strict credit limit; once that threshold is breached, they are hit with cascading penalties, exorbitant fees, and severe financial distress 16. Hospitals operate on a similar "capacity budget." When patient demand is within expected norms, the system functions. But when a prolonged heatwave pushes hospital ward and intensive care unit (ICU) occupancy past a critical threshold, the system crosses its clinical credit limit. The penalty for exceeding this limit is exponential human mortality.
Data indicates that U.S. hospitals have already shifted from a historical mean occupancy of 64% (between 2009 and 2019) to a dangerous new normal of 75% occupancy going into 2024 14. This shift is largely driven by persistent workforce shortages and a 16% reduction in the number of staffed hospital beds over recent years 14. When extreme heat events strike these already-strained systems, the results are mathematically brutal.
Epidemiological modeling of U.S. hospital strain demonstrates a sharp, non-linear relationship between capacity and death. Data indicates that if nationwide ICU bed use reaches 75% capacity, the healthcare system will experience an estimated 12,000 excess deaths over the following two weeks due to delayed and compromised care 15. If a severe heatwave pushes hospital ICU capacity to 100%, the mortality penalty skyrockets exponentially to an expected 80,000 excess deaths within a 14-day window 15. As intensive care units exceed these thresholds, the quality of care degrades rapidly, leading to a severe spike in preventable mortality.
The deadly reality of emergency room boarding
This capacity crisis manifests visibly in emergency department "boarding" times. Boarding occurs when a patient is officially admitted to the hospital by an ER physician but must wait in the emergency department - often on a gurney in a hallway - because no inpatient beds are available upstairs.
Historically, waiting 24 hours for an inpatient bed was a rare anomaly. However, recent health policy studies reveal a nationwide deterioration in admission logistics. By 2024, during peak strain periods, up to 40% of admitted emergency patients waited four or more hours for a bed, and nearly 5% waited a full 24 hours 16. This boarding crisis disproportionately impacts older adults, non-English speakers, and minority patients, indicating deep systemic disparities 16.
The danger of this hospital congestion cannot be overstated. An exhaustive analysis of national hospital data from Austria proved that this physical gridlock directly kills patients. Researchers found that when individuals aged 75 and older are exposed to 14 consecutive days of temperatures above 30°C (86°F), their risk of dying inside the hospital increases by 32% 20. Alarmingly, heatwaves increase mortality risk by 5% even among patients who were already admitted to the hospital before the heatwave began 21. This proves that extreme heat does not simply send more people to the hospital; it clogs the arteries of the hospital itself, compromising care for everyone inside the building, whether they are suffering from heatstroke, recovering from surgery, or battling cancer 2021.
| Hospital Strain Metric | Current Baseline / Observation | Impact During Extreme Heat Events |
|---|---|---|
| National ICU Occupancy | Averaging 75% post-pandemic 14. | Hitting 75% triggers ~12,000 excess deaths over 2 weeks; hitting 100% triggers ~80,000 excess deaths 15. |
| ED Boarding Times | 25% of patients wait >4 hours in non-peak months 16. | Spikes to 40% waiting >4 hours; 5% wait >24 hours for a bed, severely degrading emergency care 16. |
| In-Hospital Mortality | Standard baseline for admitted patients. | Risk of dying inside the hospital jumps 32% for patients 75+ after 14 days of >30°C heat 20. |
| Critical Care Deserts | 80% of U.S. counties lack adequate broader healthcare access 6. | High-heat states (e.g., Arizona, Nevada) show massive mismatches between high mortality and low ICU bed availability 17. |
Regional epicenters: South Asia's escalating crisis
While extreme heat is a global phenomenon, epidemiological data points to two distinct regional epicenters where the intersection of climate change, population density, and health system strain is resulting in massive casualties.
South Asia has rapidly emerged as the most vulnerable region on the planet to heat-related mortality. Home to over two billion people, the subcontinent faces an existential threat from rising baseline temperatures compounded by lethal humidity. According to the Global Burden of Disease (GBD) 2021 study, South Asia recorded nearly 210,000 deaths directly attributable to extreme heat in that year alone, alongside over 6.7 million disability-adjusted life years (DALYs) lost 18. By comparison, Southeast Asia recorded roughly 32,000 heat-related deaths in the same period 18.
The situation has deteriorated further since 2021. During the pre-monsoon season of 2026, a brutal, persistent heatwave gripped India and Pakistan, with maximum temperatures soaring above 49°C (120°F) in urban centers like New Delhi 1920. This extreme heat dome triggered massive spikes in emergency hospital admissions for dehydration and cardiovascular complications, collapsed local power grids, and induced agricultural droughts across a million square kilometers 1921. The economic toll is equally devastating; extreme heat exposure in India recently led to 247 billion potential labor hours lost in a single year, resulting in an estimated $194 billion loss in income 22.
The lethality in South Asia is driven by the "wet-bulb" temperature - a metric that combines heat and humidity. When wet-bulb temperatures cross 35°C (95°F), the human body loses the physical ability to cool itself through sweating, as the surrounding air is too saturated to allow for evaporation. Prolonged exposure at this threshold is fatal, even for young, healthy resting adults 20. Epidemiological projections warn that if current greenhouse gas emission trajectories continue, annual heat-related deaths in South Asia could double, exceeding 400,000 by the year 2045, with population growth and aging serving as primary multipliers 1823.
Europe: Rapid warming in the Global North
Meanwhile, Europe holds the alarming title of the world's fastest-warming continent, heating at twice the global average 8. While the absolute number of heat-related deaths is lower than in South Asia, the relative impact on Europe's rapidly aging population is catastrophic.
In 2024, the hottest year on record globally, Europe experienced over 62,700 heat-related deaths - a 23% surge from the mortality seen in 2023 8. Southeastern Europe and the Mediterranean basin are emerging as primary climate change hotspots. During the summer of 2024, local populations in Southeastern Europe endured "strong heat stress" for 66 days, more than double the historical average of 29 days 24.
The future outlook for European healthcare infrastructure is daunting. Comprehensive health impact assessments project that the number of heat-related respiratory hospital admissions will nearly triple in Southern Europe by the 2050s 2526. Across the entire continent, heat-related respiratory admissions are projected to jump from an historical baseline of 11,000 annually to 26,000 annually by 2050, placing immense strain on nationalized health services 2526.
Early season heatwaves and the changing climate calendar
Epidemiologists note that the timing of a heatwave is often just as critical as its absolute temperature. A 35°C (95°F) day in May is statistically much deadlier than a 35°C day in August. This is due to a physiological process called acclimatization. It takes the human body several weeks to adjust to warmer weather - altering sweat rate, blood volume, and cardiovascular efficiency. When extreme heat strikes early in the year, populations are caught physiologically unprepared.
This dynamic was glaringly apparent in late May 2026, when an exceptionally early and powerful heat dome settled over Western Europe. Temperatures smashed historical records, with the UK recording its earliest ever "tropical night" (where temperatures do not drop below 20°C) and France reporting temperatures pushing 39°C (102°F) well before the official start of summer 2728. These unseasonal heat domes, exacerbated by shifting jet streams and phenomena like Super El Niño, drive immediate spikes in hospital admissions because neither the population's physiology nor the local infrastructure (such as municipal cooling centers) has transitioned out of winter/spring modes 29.
Can health systems adapt to the new normal?
The 2025 report of the Lancet Countdown on Health and Climate Change offers a stark warning: delays in climate action and backsliding on fossil fuel commitments are actively costing millions of lives and threatening human wellbeing globally 30. However, the report also emphasizes that targeted adaptation and resilience planning can offer a vital lifeline. Countries and communities that are proactively leading the transition are already observing measurable health and economic gains 30.
To prevent hospitals from becoming overwhelmed, governments must implement robust, tiered heat-health early warning systems. These systems - such as those actively used in Italy since 2004 - rely on meteorological forecasts to predict excess mortality risk and trigger immediate, coordinated public health responses, such as deploying cooling centers and checking on isolated elderly populations 7.
Furthermore, the hospitals themselves must physically adapt. During recent European heatwaves, critical data cooling systems failed at two major London hospitals, costing the National Health Service £1.5 million and severely delaying life-saving patient treatments 10. Protecting human life now requires retrofitting healthcare facilities with redundant microgrids for power resilience, high-capacity climate control systems, and flexible clinical triage protocols to ensure that when the next heat dome settles, the hospital's operational "credit limit" can withstand the inevitable surge of patients 1031.
Bottom line
Extreme heat is fundamentally reshaping the landscape of global public health, turning predictable summer weather into severe mass-casualty events that push hospital occupancy past dangerous physical and operational limits. While the exact trajectory of future hospital capacity remains somewhat uncertain due to shifting political commitments to climate adaptation, the epidemiological evidence is undeniable: without immediate, systemic interventions to curb emissions and reinforce medical infrastructure, the death toll from metabolic, renal, and respiratory failures triggered by extreme heat will exponentially rise.