Effects of vagus nerve stimulation on anxiety
1. Introduction: The Renaissance of Autonomic Neuromodulation in Psychiatric Medicine
The vagus nerve, designated as the tenth cranial nerve and universally recognized as the primary neural superhighway of the parasympathetic nervous system, has emerged as the central focus of a profound paradigm shift within contemporary neuroscience, biological psychiatry, and clinical physiology. Historically relegated to its fundamental evolutionary role in basic autonomic maintenance - specifically mediating the "rest and digest" physiological states that counterbalance sympathetic arousal - the vagus nerve is now comprehensively understood to be a highly complex, bidirectional communication network. This vast neuroanatomical infrastructure exerts profound, ongoing influence over systemic neuroinflammation, the synthesis and release of monoamine neurotransmitters, global mood regulation, and the physiological and cognitive manifestations of clinical anxiety 123. The therapeutic application of this extensive neurobiological knowledge, broadly termed vagus nerve stimulation (VNS), has evolved at a remarkable pace. It has transitioned from a highly invasive, surgically implanted intervention originally developed for refractory epilepsy to a rapidly expanding, highly accessible frontier of non-invasive transcutaneous vagus nerve stimulation (tVNS) 23.
Simultaneously, the popularization of the vagus nerve and its role in stress regulation within public discourse has catalyzed a viral, consumer-driven "biohacking" movement. Digital and social media platforms are currently replete with an abundance of unverified claims surrounding instantaneous "vagus nerve resets," which are purported to be easily achieved through superficial ocular movements, vigorous ear manipulations, facial ice water immersion, and acoustic sonic vibrations 45. This rapid commercialization, democratization, and ultimate dilution of rigorous autonomic terminology have created a profound and concerning schism between rigorously validated clinical neuroscience and reductive lifestyle wellness trends . Complex neuropsychiatric pathologies, such as Generalized Anxiety Disorder (GAD) and treatment-resistant trauma, are increasingly being marketed as conditions that can be permanently resolved through momentary somatic parlor tricks, fundamentally misrepresenting the nature of autonomic recalibration.
This comprehensive research report systematically evaluates the current, evidence-based landscape of vagal neuromodulation. It delineates the precise anatomical pathways, the intricate neuroimmune gut-brain axis, and the specific nerve fiber recruitment mechanisms that govern the vagus nerve, explicitly contrasting the mechanisms of surgically implanted VNS (iVNS) with the emerging tier of FDA-cleared and consumer-grade transcutaneous devices. Furthermore, the analysis synthesizes high-tier clinical evidence, systematically reviewing recent clinical trials, meta-analyses, and longitudinal data published between 2023 and 2026. This evaluation focuses specifically on the long-term therapeutic outcomes of tVNS for the management of clinical anxiety. Finally, the report significantly broadens its analytical scope to objectively evaluate highly structured behavioral interventions - ranging from the physiological hormesis of cold water immersion to the respiratory mechanics of traditional Indian Pranayama and chanting. By doing so, it bridges the gap between ancient cultural practices, viral wellness trends, and the uncompromising rigor of evidence-based physiological science.
2. Anatomical Pathways, Fiber Classification, and the Gut-Brain Axis
To comprehend precisely how vagal stimulation successfully modulates clinical anxiety and systemic stress responses, one must first deconstruct the highly intricate neuroanatomy of cranial nerve X.
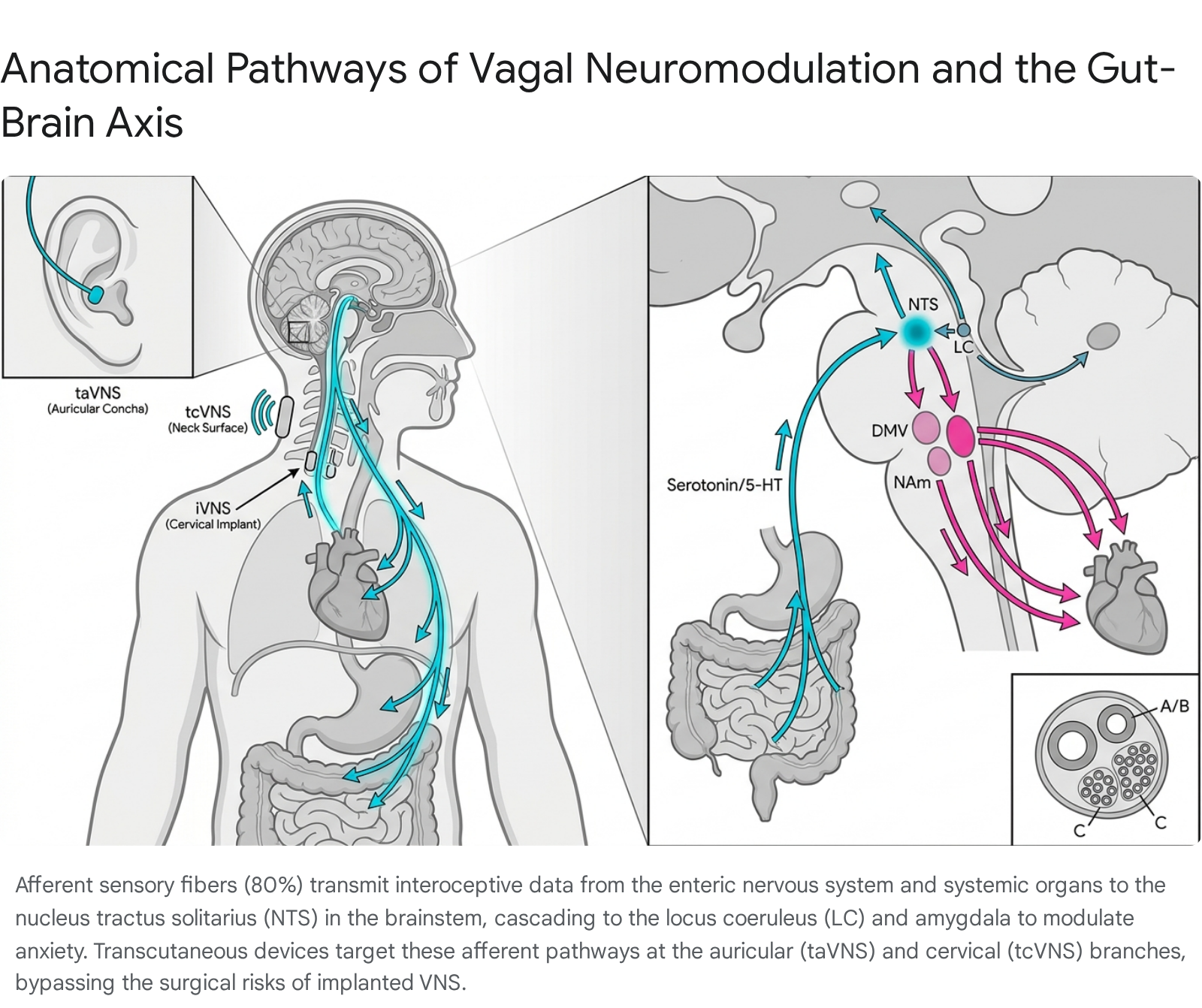
The vagus nerve is entirely distinct from a monolithic, unidirectional biological wire; rather, it functions as a highly arborized, bidirectional network composed of approximately 80% to 90% ascending afferent (sensory) fibers and 10% to 20% descending efferent (motor) fibers 123. This striking asymmetrical ratio fundamentally underscores its primary evolutionary and physiological function: to serve as the brain's ultimate interoceptive sensory conduit, continuously monitoring the homeostatic and visceral state of the organism and relaying this critical survival data back to the central nervous system (CNS) for processing and response 24.
2.1 The Ascending Afferent and Descending Efferent Pathways
The ascending, or afferent, signals of the vagus nerve originate in a multitude of peripheral organs, densely innervating the mucosa and muscle layers of the gastrointestinal tract, the cardiac tissue, the pulmonary structures, and the spleen. These sensory signals, generated by tension receptors, chemoreceptors, and mechanoreceptors, travel superiorly via the nodose (or tuberous) ganglion to terminate primarily in the nucleus tractus solitarius (NTS), a highly specialized integration hub located within the medulla oblongata of the brainstem 15. The NTS acts as the master integration center for all autonomic functioning. From the NTS, incoming interoceptive signals are broadly and powerfully projected to higher-order brain regions that are deeply implicated in emotional regulation, threat detection, and the stress response. These critical higher-order projections include pathways to the locus coeruleus (LC), the dorsal raphe nucleus (DRN), the amygdala, the hippocampus, and various regions of the cerebral cortex 12.
Conversely, the descending, or efferent, pathways originate from two primary brainstem nuclei: the Nucleus Ambiguus (NAm) and the Dorsal Motor Nucleus of the Vagus (DMV). The NAm primarily governs the myelinated efferent fibers that are responsible for regulating cardiac chronotropy (controlling the slowing of the heart rate) as well as branchial motor functions such as vocalization, swallowing, and the gag reflex 16. The DMV, on the other hand, gives rise to the unmyelinated efferent fibers that primarily modulate sub-diaphragmatic visceral functions, distributing critical parasympathetic signals to the stomach, bronchi, small intestine, and pancreas to dictate muscle contraction, enzymatic secretion, and global gastrointestinal motility 16.
2.2 The Gut-Brain Axis and Neurotransmitter Modulation
The vagus nerve serves as the principal, high-speed neural axis connecting the complex enteric nervous system of the gut directly to the brainstem, thereby forming the structural and functional basis of the much-studied gut-brain axis. Within the gastrointestinal epithelium, specialized sensory cells known as enterochromaffin (EC) cells act as the body's primary visceral chemosensors 1. In response to mechanical stretch, localized chemical stimuli, or the presence of microbiome-derived inflammatory metabolites, these EC cells synthesize and release vast quantities of peripheral serotonin (5-HT) 1. This localized serotonin rapidly binds to 5-HT3 receptors located directly on the terminals of the adjacent vagal afferent fibers, initiating an action potential that travels upward through the vagal trunk to the NTS 1.
Upon reaching the NTS, this ascending interoceptive information exerts a profound, cascading influence over the central synthesis and release of key monoamine neurotransmitters that dictate human mood and anxiety. Projections extending from the NTS to the Dorsal Raphe Nucleus (DRN) modulate central serotonin levels, an interaction that is absolutely critical for mood stabilization, emotional buffering, and the clinical alleviation of severe anxiety 1. Concurrently, efferent projections from the NTS to the locus coeruleus (LC) regulate the central release of norepinephrine (NE), a potent neurotransmitter that dictates global cognitive arousal, vigilant attention, and the sympathetic "fight or flight" response 16. The precise, bidirectional modulation of this serotonin-norepinephrine interplay by the vagus nerve lies at the very center of the pathophysiology, and consequently the clinical treatment, of Generalized Anxiety Disorder (GAD), Post-Traumatic Stress Disorder (PTSD), and treatment-resistant major depression 123.
2.3 Fiber Morphology: A, B, and C Recruitment Thresholds
The clinical efficacy and the specific safety profile of both invasive surgical VNS and non-invasive transcutaneous VNS fundamentally depend on the differential electrical recruitment of distinct vagal fiber types. These fibers are traditionally categorized based on their degree of myelination, physical diameter, and resulting conduction velocity:
- A-Fibers: These are the largest-diameter, heavily myelinated fibers within the vagus nerve. Because of their heavy myelination, they possess the fastest conduction velocities and the lowest electrical recruitment thresholds. Experimental in vivo data indicates that A-fibers are recruited at minimal stimulus strengths (designated as T, typically varying between 0.05 and 0.1 V in experimental animal models). They primarily serve as rapid somatic and visceral afferents, such as pulmonary stretch receptors that mediate respiratory reflexes 7.
- B-Fibers: These are medium-diameter, lightly myelinated fibers with moderate electrical recruitment thresholds, requiring stimulation intensities approximately 2.5 to 5 times greater than the threshold of A-fibers (2.5 to 5T). These fibers predominantly comprise the parasympathetic preganglionic efferents that are directly responsible for initiating bradycardia (the sudden, reflexive slowing of the heart rate) 78.
- C-Fibers: Comprising the vast, overwhelming majority (up to 80%) of the cervical vagus nerve structure, C-fibers are exceedingly small, completely unmyelinated, and slow-conducting. Because they lack a myelin sheath, they possess the highest electrical recruitment thresholds, requiring powerful stimulation intensities 25 to 67 times greater than those needed to recruit A-fibers (25 to 67T). C-fibers primarily function to transmit slow, diffuse nociceptive (pain) signals and convey visceral inflammatory states to the brain 79.
In the early decades of VNS research, it was widely, yet incorrectly, hypothesized that the maximal recruitment of these abundant C-fibers was an absolute necessity for achieving therapeutic efficacy, particularly in the realm of seizure suppression for epilepsy 9. However, subsequent sophisticated neurological models and modern optogenetic studies definitively demonstrated that the targeted chemical destruction or localized blockade of peripheral C-fibers did absolutely nothing to diminish the antiepileptic or anxiolytic effects of VNS therapy 910. Today, the therapeutic benefits of VNS - particularly regarding mood regulation, anti-inflammatory action, and anxiety reduction - are entirely attributed to the maximal, targeted recruitment of the thick, myelinated A and B afferent fibers 9.
This specific electrophysiological distinction is the functional cornerstone of non-invasive transcutaneous VNS (tVNS). Because tVNS devices utilize specialized, meticulously calibrated pulse widths and frequencies designed to selectively depolarize A and B fibers while remaining safely below the high-voltage threshold required to trigger unmyelinated C-fibers, patients can receive profound autonomic neuromodulation without experiencing the severe nociceptive pain and extreme bradycardia that would inevitably accompany total C-fiber activation 789. Advanced computational modeling software, such as the ASCENT framework, has recently validated that appropriately calibrated surface electrodes can accurately predict and achieve specific A and B fiber activation across human, porcine, and rodent models, providing a robust engineering foundation for the current generation of non-invasive therapeutics 8.
3. The Dichotomy of Intervention: Surgically Implanted VNS vs. Transcutaneous VNS
Understanding the clinical trajectory of vagal neuromodulation requires a precise differentiation between the historically dominant surgical methods and the modern proliferation of surface-level bioelectronic therapeutics.
3.1 Surgically Implanted VNS (iVNS): The Invasive Gold Standard
Invasive Vagus Nerve Stimulation (iVNS) represents the absolute genesis of clinical autonomic neuromodulation. The physical procedure is highly invasive, involving the permanent surgical implantation of a programmable, battery-powered pulse generator - conceptually and physically analogous to a cardiac pacemaker - subcutaneously within the upper left chest wall. From this generator, a bipolar helical lead is meticulously tunneled beneath the skin of the chest and neck, where it is wrapped directly around the left cervical trunk of the vagus nerve, residing within the carotid sheath 81112.
Because of its direct, unimpeded access to the nerve trunk, iVNS received formal approval from the U.S. Food and Drug Administration (FDA) for the treatment of severe, medication-refractory epilepsy in 1997, followed by a landmark approval for severe Treatment-Resistant Depression (TRD) in 2005 1112. The evidence for the extreme long-term efficacy of iVNS in deeply intractable psychiatric populations is profound and remains the gold standard against which all other neuromodulation is measured.
The multi-center RECOVER trial, an exhaustive observational study which published highly anticipated 24-month follow-up data in early 2026, evaluated 214 adults suffering from extreme, higher-grade TRD. The participants in this trial represented the most severe psychiatric cohort ever studied in such a context, possessing an average history of 13.5 failed prior treatment regimens, with a vast majority having already failed exhaustive courses of neurostimulation interventions such as electroconvulsive therapy (ECT) and transcranial magnetic stimulation (TMS) 131415. The trial data revealed a paradigm-shifting durability of effect: among those participants who achieved a clinically meaningful benefit from iVNS at the 12-month mark, over 80% successfully maintained that exact level of benefit through the 18-month and 24-month assessments 1314. Furthermore, an astonishing 21.5% of these profoundly ill patients achieved full, clinical remission of all depressive and anxious symptoms as measured by the Montgomery-Åsberg Depression Rating Scale (MADRS) at the two-year mark 1314. The study also noted an incredible secondary phenomenon: clinical benefit from iVNS often continues to accrue slowly over time, with approximately 30% to 40% of non-responders at the 12-month mark converting into positive responders by the 24-month evaluation 14.
However, the broad clinical application of iVNS is inherently bottlenecked by the reality of its profound invasiveness. The initial implantation surgery carries distinct perioperative risks, including the potential for severe surgical site infection and permanent vocal cord paralysis resulting from iatrogenic nerve trauma. Moreover, the direct, chronic, and indiscriminate electrical stimulation of the entire cervical vagus trunk - including vast swathes of efferent motor fibers - frequently induces highly disruptive off-target side effects. Patients commonly report experiencing significant dyspnea (shortness of breath), uncontrollable coughing fits, and severe voice hoarseness that specifically correlate with the active, "on" cycles of the implanted pulse generator 162017.
3.2 Transcutaneous VNS (tVNS): Expanding Access through Bioelectronic Innovation
To circumvent the prohibitive surgical risks, severe off-target side effects, and immense economic barriers associated with iVNS, the field of bioelectronic medicine has aggressively advanced the development and refinement of transcutaneous Vagus Nerve Stimulation (tVNS). This completely non-invasive modality relies on the delivery of targeted, precisely calibrated electrical currents across the epidermal boundary to depolarize and activate the underlying afferent vagal branches. Currently, clinical tVNS is primarily administered via two distinct anatomical pathways:
- Transcutaneous Cervical VNS (tcVNS): This method utilizes handheld devices applied externally to the skin on the side of the neck. The electrical current travels through the skin and subcutaneous tissue to target the main cervical branch of the vagus nerve as it descends within the carotid sheath. While effective, it generally requires manual application by the patient and the use of conductive gels to ensure adequate signal penetration 29.
- Transcutaneous Auricular VNS (taVNS): Human anatomical mapping has conclusively demonstrated that the external ear is the absolute only anatomical region in the entire human body where an afferent branch of the vagus nerve projects directly to the epidermal surface 18. taVNS devices capitalize on this unique anatomical quirk by utilizing customized wearable earpieces or specialized electrode clips that attach directly to the cymba conchae or the tragus of the left ear. This allows for the direct, highly localized stimulation of the auricular branch of the vagus nerve (ABVN) 91018.
Extensive functional magnetic resonance imaging (fMRI) studies and advanced neuroimaging analyses have rigorously validated that non-invasive taVNS robustly activates the exact same brainstem nuclei (specifically the NTS and LC) and higher-order limbic structures (such as the amygdala and prefrontal cortex) that are targeted by surgically implanted iVNS 510. Because it successfully replicates the central nervous system activation patterns of a surgical implant while completely bypassing the efferent fibers that cause hoarseness and coughing, tVNS is rapidly transitioning from a theoretical, experimental alternative into a primary, first-line clinical intervention for autonomic dysfunction, chronic pain, and severe anxiety disorders 1819.
4. Evaluation of the tVNS Hardware Landscape: FDA-Cleared Medical Devices vs. Consumer Wearables
The rapid commercialization of non-invasive neuromodulation has resulted in a highly saturated, occasionally deceptive technological market. For clinical practitioners and patients alike, it is fundamentally required to establish a rigorous differentiation between clinically validated, highly regulated medical devices and the proliferation of consumer-grade wellness products that often co-opt the terminology of neuroscience without providing the corresponding physiological mechanism of action.
4.1 Clinically Validated Electrical Neuromodulators
GammaCore (tcVNS): Developed by electroCore Medical LLC, GammaCore represents the premier FDA-cleared prescription tcVNS device on the modern market. It is utilized primarily for the acute treatment and clinical prevention of both episodic and chronic cluster headaches, as well as severe migraine variants 162425. Applied manually to the left or right side of the neck using a proprietary conductive gel, the device delivers a specifically calibrated, high-frequency electrical signal. While its official FDA clearance is strictly limited to headache management, a robust array of off-label clinical trials has increasingly investigated GammaCore for complex psychiatric and systemic conditions. A highly notable 2021 pilot study - which subsequently led to an expedited FDA "breakthrough device" designation for the technology - demonstrated that three months of twice-daily tcVNS use significantly reduced clinical stress and trauma symptoms by 31% in a cohort of patients with severe Post-Traumatic Stress Disorder (PTSD) 2. Crucially, the study also documented a significant, measurable blunting of systemic interleukin-6 (IL-6) inflammatory responses following exposure to personalized traumatic scripts, validating the device's ability to trigger the vagal anti-inflammatory reflex 226.
Nurosym (taVNS): Operating within the auricular domain, Nurosym (developed by Parasym) is a CE-marked, highly advanced wearable taVNS device that specifically targets the auricular branch of the vagus nerve via an electrode clip placed on the tragus of the left ear. Unlike manual cervical stimulators, Nurosym has amassed a massive body of first-tier clinical evidence through double-blind, randomized, placebo-controlled trials conducted at prestigious institutions, including Harvard University, UCLA, and the University of Chicago Medical School 2728. Utilizing its proprietary Auricular Vagal Neuromodulation Therapy (AVNT) signal, the device delivers precise, algorithmic electrical impulses that are clinically proven to maximize afferent recruitment. Aggregate clinical data derived from extensive 2024 studies reports staggering therapeutic outcomes across a spectrum of autonomic measures: a 45% clinical improvement in standardized depression scores, a 35% overall reduction in anxious thoughts, an 18% permanent increase in resting Heart Rate Variability (HRV), a 48% improvement in chronic fatigue symptoms, and a 78% reduction in systemic inflammatory markers 242829. Unlike implanted devices or manual tcVNS applicators, Nurosym's design allows for continuous 30-to-60-minute stimulation protocols that can be passively integrated into a patient's daily routine - such as while reading or working - radically enhancing long-term patient compliance for chronic anxiety management 20.
Emerging Trigeminal Nerve Stimulation (TNS): While not exclusively vagal, it is highly relevant to note the emergence of external trigeminal nerve stimulation (eTNS) as a parallel non-invasive modality for anxiety and mood disorders. 2024 clinical trials evaluating eTNS (which delivers mild electrical pulses directly to the forehead) for patients with Generalized Anxiety Disorder who have failed to respond to standard SSRI/SNRI regimens have demonstrated a highly favorable safety profile, minimal adverse effects, and significant potential for rapid mood stabilization, further validating the broad efficacy of cranial nerve neuromodulation 31.
4.2 The Acoustic and Vibratory Wearable Market
In stark contrast to electrical neuromodulators, the consumer market is increasingly populated by wellness devices such as Sensate and Sona, which aggressively claim to stimulate the vagus nerve using entirely different physical mechanisms. Sensate, for instance, relies on the delivery of infrasound sonic vibrations and acoustic frequencies. The device is placed physically on the sternum (chest bone), utilizing bone conduction to transmit low-frequency sound waves into the thoracic cavity 242932.
While users of devices like Sensate frequently report feelings of acute, subjective relaxation and improved sleep, there is a massive and critical distinction in the underlying neurobiological mechanism of action. Devices relying on acoustic resonance and physical vibration induce a generalized, somatic relaxation response - they absolutely do not directly or electrically depolarize the cellular action potentials of the vagal afferent nerve fibers 2432. Exhaustive medical reviews and technological analyses published in 2024 clearly state that there is an absolute absence of peer-reviewed, double-blind RCTs proving that vibratory consumer wearables directly engage the NTS-parasympathetic neural circuits in the precise, quantifiable manner achieved by electrical taVNS devices like Nurosym or GammaCore 24. Consequently, while potentially useful as adjunctive stress-relief tools, they must be strictly classified as low-risk wellness accessories rather than verified clinical neuromodulators.
5. Clinical Evidence for tVNS in Generalized Anxiety Disorder (2023 - 2026)
Generalized Anxiety Disorder (GAD) is a pervasive psychiatric pathology characterized by chronic, uncontrollable worry, systemic autonomic hyperarousal, and a pathological, baseline dysregulation of the sympathetic nervous system 26. Over the past three years, the clinical evaluation of tVNS for the treatment of severe anxiety has matured rapidly, evolving from small-scale pilot feasibility studies to robust, large-scale randomized controlled trials (RCTs) and highly powered systematic meta-analyses. This wealth of recent data has firmly established non-invasive vagal modulation as both a standalone therapeutic and a highly synergistic adjunctive treatment.
5.1 Acute Anxiolytic Efficacy and Neuroimaging Validation
Systematic reviews and clinical trials conducted between 2023 and 2025 conclusively demonstrate that tVNS induces rapid and profound anxiolytic effects. A landmark 2024 longitudinal, randomized, placebo-controlled study evaluating the Roga taVNS device on a cohort of 32 participants with moderate-to-severe baseline anxiety reported unprecedented acute changes. Participants who received active, daily taVNS stimulation over a standard four-week period demonstrated a massive 47% decrease in their Generalized Anxiety Disorder Scale (GAD-7) scores - representing a total clinical shift from "severe" to "mild" anxiety classifications 33. Concurrently, their State-Trait Anxiety Inventory (STAI-S) scores decreased by 14%, with highly significant divergence from the sham placebo group emerging as early as the two-week clinical mark 33.
These subjective psychometric improvements are now fully supported by objective neurological data. A critical 2025 single-blinded RCT conducted by Jackowska et al., published in Biological Psychology, evaluated 70 participants across different temporal phases of active versus sham taVNS (delivered continuously for 4 hours daily). The study established beyond doubt that active tVNS was vastly superior to sham stimulation in the early treatment phases for rapidly mitigating both clinical anxiety symptoms and general perceived stress, acting directly to lower neurobiological stress vulnerability even in non-clinical, aging populations 2621. Mechanistically, functional magnetic resonance imaging (fMRI) studies involving 60 GAD patients have revealed that acute taVNS achieves this rapid anxiolysis by instantly regulating the Amplitude of Low-Frequency Fluctuations (ALFF) and functional connectivity (FC) within the brain's Default Mode Network (DMN) and Cognitive Control Network (CCN) 352223. By doing so, taVNS directly and physically attenuates the amygdala's pathological hyper-responsivity to ambiguous or minor environmental threats, fundamentally rewriting the brain's baseline fear processing algorithms 3524.
5.2 Long-Term Durability and Superiority Over Pharmacotherapy
The long-term durability of tVNS for chronic anxiety marks a vital advancement over standard, highly flawed psychotropic regimens. Conventional pharmacological treatments for GAD - primarily Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) - are moderately effective in the short term. However, they suffer from exceptionally high patient attrition rates due to severe, systemic adverse side effects (such as gastrointestinal distress, weight gain, and profound sexual dysfunction), a delayed onset of action often exceeding six weeks, and a remarkably low quality of comparative long-term evidence. As highlighted in a comprehensive 2023 network meta-analysis published in the Ge-Bu Bulletin, the actual, clinically relevant difference between SSRIs/SNRIs and placebo in the long-term management of panic and anxiety disorders is often statistically marginal and heavily skewed by massive placebo effects 25.
In stark contrast, retrospective data and observational studies from 2023 and 2024 regarding the long-term, repeated application of tVNS suggest deeply sustained, side-effect-free therapeutic benefits. An exhaustive 2023 retrospective chart review evaluating 18 patients with high baseline anxiety treated in an outpatient psychiatric clinic demonstrated that repeated tVNS treatments (between 10 to 15 total administrations, using a 20 Hz frequency) led to highly significant, persistent decreases in self-reported tension (p = 0.004) and restlessness (p = 0.021), coupled with significant, lasting increases in parasympathetic relaxation (p = 0.007) 11.
Moreover, a massive 2023 systematic review and meta-analysis covering the use of taVNS for comorbid depressive and anxiety disorders found that combining daily taVNS with standard antidepressant pharmacotherapy yielded clinical response rates that were entirely comparable to - and in certain cohorts, vastly superior to - using heavy doses of antidepressants alone 40. Crucially, this combination therapy resulted in a vastly reduced systemic side-effect profile 40. The long-term safety profile of continuous tVNS usage is overwhelmingly favorable across all available literature; adverse events are generally limited to highly transient, minor local skin erythema (redness) or mild tingling at the electrode site on the ear or neck, completely bypassing the debilitating neurochemical cascades that plague long-term SSRI usage 112440. Currently, massive 2024 - 2025 RCTs involving double-blind, parallel-controlled medication-combined taVNS groups are actively evaluating patients over 8-week to 6-month horizons to definitively codify taVNS as a permanent, first-line standard of care for GAD 2341.
6. The "Biohacking" Phenomenon: Deconstructing Social Media Myths and Validating Neuroscience
The rapid, highly publicized clinical validation of the vagus nerve has, somewhat inevitably, spawned a massive, entirely unregulated wellness industry on digital platforms like TikTok, Instagram, and Lemon8. This environment is largely characterized by the viral, pseudo-scientific phenomenon of the "Vagus Nerve Reset." Influencers, often completely lacking in neurobiological training, routinely prescribe wildly oversimplified somatic exercises - such as splashing ice water directly onto the face, aggressive and rhythmic ear pulling, or the widely shared "Stanley Rosenberg Basic Exercise" (which involves interlocking the fingers behind the user's head and rolling the eyes to the extreme lateral periphery until a spontaneous yawn or swallow is elicited) - as instant, permanent panaceas for clinical anxiety, complex developmental trauma, and severe nervous system dysregulation 454243.
6.1 Neurological Critique of Somatic "Resets"
Eminent neuroscientists and clinical physiologists assert uniformly that these viral trends represent a gross, fundamental oversimplification of autonomic neurobiology that borders on absolute pseudoscience . For instance, a biomechanical analysis of the widely touted Stanley Rosenberg eye-rolling technique reveals that it relies entirely on the known anatomical fascial connections that exist between the eight suboccipital muscles located at the base of the skull and the extraocular muscles controlling eye movement 434445. While actively stretching these muscles through extreme eye deviation can certainly release localized fascial tension, alleviate mechanical neck stiffness, and potentially increase highly transient regional blood flow to the brainstem, suggesting that this brief biomechanical stretch fundamentally "rewires the brain from anxiety" or functionally "resets the vagus nerve" is scientifically unfounded and highly misleading 4445.
Similarly, while manual auricular acupressure (such as rhythmic ear massage) may occasionally induce minor, incredibly short-term fluctuations in heart rate variability (HRV) due to extremely mild, superficial tactile nerve stimulation, peer-reviewed clinical studies unequivocally confirm that there is absolutely no direct evidence that manual rubbing can achieve the deep, sustained neuronal depolarization required to mimic the profound therapeutic efficacy of electrical tVNS 45. The overwhelming clinical consensus maintains that attempting to treat complex, chronic neuropsychiatric disorders with simplistic eye movements or ice splashing confuses a transient, momentary relaxation response - or simply the psychological benefit of behavioral distraction - with a systemic, permanent neurobiological cure .
6.2 The Polyvagal Theory Controversy
The theoretical foundation most frequently cited by somatic biohackers to justify these physical manipulations is Dr. Stephen Porges' Polyvagal Theory. This theory posits an evolutionary hierarchy of autonomic responses mediated by distinct branches of the vagus nerve (proposing a "social engagement" ventral vagus distinct from an older, "freeze-response" dorsal vagus) 46. However, this theory remains highly controversial and fiercely debated within the upper echelons of elite biological psychiatry and comparative anatomy.
A major, highly publicized 2023 scientific critique spearheaded by Paul Grossman in a special issue of Biological Psychology argued aggressively that Polyvagal Theory relies on fundamental "categorical misunderstandings" of neuroanatomy. Grossman's critique asserted that the theory's foundational claims regarding Respiratory Sinus Arrhythmia (RSA) as an exclusive metric of mammalian vagal tone are anatomically flawed, relying on respiratory artifacts and "strawman arguments" regarding phylogenetic evolution 46. Porges responded vigorously in a February 2026 scholarly rebuttal, utilizing cutting-edge 2024 transcriptomic and optogenetic data from Strain et al. This new data demonstrated that optogenetically stimulating specific dorsal motor nucleus (DMNX) neurons successfully modulates anxiety and produces bradycardia without triggering the evolutionary "freeze" or locomotor suppression response, thereby fiercely defending the functional separation of the vagal nuclei proposed by his original theory 46. Regardless of the outcome of this intense academic debate, both critics and proponents agree completely on one singular fact: social media influencers have severely and recklessly distorted the theory, stripping away its vast anatomical rigor to peddle commercialized, instant-fix somatic therapies to a vulnerable public 4246.
7. Global Paradigms: Structured Breathwork, Chanting, and Thermal Hormesis
While dismissing viral pseudo-neurology is clinically necessary, modern physiological science is simultaneously validating several ancient, highly structured behavioral practices by accurately quantifying their direct, measurable impact on vagal tone and parasympathetic activation. These practices, when applied with rigor, offer low-cost, evidence-based physiological adjuncts to technological tVNS.
7.1 Traditional Breathwork, Pranayama, and Western HRV Biofeedback
Eastern contemplative traditions, specifically the Indian yogic science of Pranayama (breath control), have actively utilized vagal modulation for millennia. Western respiratory physiology has recently begun to quantify the efficacy of these traditional practices through the clinical lens of Heart Rate Variability (HRV) biofeedback 26.
A highly controlled, randomized crossover clinical trial published in 2021 and evaluated heavily through 2024 investigated the specific effects of the Sheetali and Sheetkari Pranayama techniques. The study demonstrated that these highly structured, internally paced breathing exercises - which involve specific manipulations of the tongue and facial musculature to cool inhaled air - significantly increased the Root Mean Square of Successive Differences (RMSSD), which is the primary, universally accepted time-domain index of vagally mediated parasympathetic tone 2627. The physiological increase in RMSSD was significantly greater than that achieved during simple, unpaced deep breathing, providing concrete evidence for the specific autonomic utility of the traditional practice 27.
The modern Western clinical equivalent of these practices, known as "Resonant Breathing," dictates that the patient breathes precisely at a rate of 5.5 to 6 breaths per minute. This specific frequency has been shown to perfectly synchronize cardiac and respiratory rhythms, thereby maximizing Respiratory Sinus Arrhythmia (RSA) and optimizing the efficiency of pulmonary gas exchange 50. A rigorous 2026 RCT published in General Psychiatry evaluated the implementation of resonant breathing protocols in a highly complex population of acutely ill psychiatric inpatients suffering from severe somatic symptoms. The study found that while short-term breathing sessions did not immediately resolve deep-seated somatic pathology or generalized arousal, resonant breathing protocols significantly reduced clinical anxiety and intractable insomnia, providing a highly measurable, acute increase in baseline parasympathetic regulation for hospitalized patients 28. It is important to note, however, that the scientific literature remains nuanced; some 2024 sports intervention studies evaluating 12 sessions of standard HRV biofeedback in adolescent athletes failed to find significant long-term increases in resting vagal tone (vmHRV) between sessions, suggesting that the benefits of breathwork may be highly transient and highly dependent on sustained, daily practice 2953.
Vocalizations such as rhythmic humming, traditional religious chanting (e.g., the prolonged "Om" mantra), and structured singing have similarly been shown to mechanistically activate the vagus nerve. The vagus nerve directly innervates the vocal cords and the muscular architecture of the pharynx and larynx via the recurrent laryngeal nerve. The sustained mechanical vibration generated deep in the throat during vocalization physically and mechanically stimulates these efferent vagal fibers, triggering a massive proprioceptive biofeedback loop that travels back to the brainstem, thereby increasing global vagal tone and forcing the downregulation of the sympathetic nervous system 5.
7.2 The Complex Physiology of Cold Water Immersion (CWI)
Deliberate cold exposure (including ice baths, cold showers, and winter plunge pools) is perhaps the most widely recognized and aggressively marketed biohacking trend, almost universally touted by influencers as an immediate, shock-therapy cure for daily stress. However, recent, highly powered clinical meta-analyses reveal a far more complex, biphasic physiological mechanism that completely contradicts the "instant relaxation" narrative.
When a human body is submerged in water below 15°C (59°F), two intensely competing autonomic reflexes are immediately triggered. Facial immersion rapidly activates the trigeminal nerve, triggering the ancient "mammalian diving reflex." This reflex powerfully stimulates vagal parasympathetic pathways to cause rapid bradycardia (heart slowing) and peripheral vasoconstriction in a desperate biological attempt to conserve oxygen 54. Conversely, total body skin immersion triggers the massive "cold shock response," resulting in explosive sympathetic nervous system activation. Clinical studies indicate that acute cold immersion spikes plasma norepinephrine levels by an astonishing 530% and dopamine levels by 250% 55.
A landmark January 2025 systematic review and meta-analysis published in PLOS ONE, which aggregated rigorous data from 11 RCTs involving 3,177 participants (with a solid mean PEDro quality score of 6.4), clarified the exact timeline of these physiological effects. The meta-analysis confirmed unequivocally that immediately following, and exactly one hour after cold water immersion, humans experience a massive, significant increase in systemic inflammation (SMD: 1.03 to 1.26) and profound sympathetic stress 303158. However, the study observed a highly significant, massive reduction in clinical stress (SMD: -1.00) and an increase in overall mood and mental well-being that occurred exactly 12 hours post-immersion 3031. Therefore, cold exposure absolutely does not induce an instant "vagal rest and digest" state as claimed by social media; rather, it is a potent form of acute hormetic stress. It intentionally subjects the body to extreme sympathetic panic in order to train the autonomic nervous system to become more resilient over time, resulting in a delayed, highly beneficial, and permanent recalibration of baseline vagal tone and stress resilience 5455.
8. Categorization and Evidence Tiers of Autonomic Interventions
To systematically synthesize the highly diverse modalities of vagal neuromodulation and autonomic regulation discussed within this report, the following table categorizes specific interventions by their specific anatomical mechanism, their short-term physiological effect, and their current, rigorous tier of clinical evidence.
(Note: Evidence tiers are defined by the highest clinical standards: Tier 1 requires robust RCT data with >200 participants, 8-12 weeks duration, parallel design, and minimal bias; Tier 2 implies adequate data but minor methodological flaws or shorter durations; Tier 3 implies highly biased, very small sample sizes, or purely subjective reporting 326033.)
| Intervention Modality | Specific Technique / Device | Proposed Mechanism of Action | Short-Term Physiological Effect | Current Tier of Clinical Evidence |
|---|---|---|---|---|
| Surgical Neuromodulation | Implanted VNS (iVNS) | Direct, continuous electrical stimulation of the left cervical vagus nerve trunk. | Recruits A, B, and C fibers; deeply alters monoamines; frequently causes dyspnea/hoarseness. | Tier 1: FDA-approved with robust 24-month durability data for Refractory Epilepsy and Severe Treatment-Resistant Depression (TRD). |
| Transcutaneous Neuromodulation | taVNS (e.g., Nurosym, Roga) & tcVNS (e.g., GammaCore) | Targeted electrical stimulation of the auricular (ear) or cervical (neck) vagus branches across the skin. | Selective recruitment of myelinated A/B afferents; massive sympathetic withdrawal; rapid amygdala suppression. | Tier 1 to Tier 2: FDA-cleared for cluster headache; exceptionally strong RCT/meta-analysis support for clinical Anxiety & MDD management. |
| Acoustic / Vibratory Stimulation | Consumer Wearables (e.g., Sensate, Sona) | Delivery of infrasonic vibrations to the sternum utilizing bone conduction. | Acoustic resonance induces a subjective, localized somatic relaxation response. | Tier 3: Anecdotal and subjective reporting; absolute lack of peer-reviewed double-blind RCTs proving direct vagal cellular depolarization. |
| Structured Breathwork | Resonant Breathing (6 bpm) & traditional Pranayama (Sheetali) | Mechanical expansion of the diaphragm; precise synchronization of pulmonary and cardiac rhythms. | Maximizes Respiratory Sinus Arrhythmia (RSA); provides acute, measurable increases in HRV and RMSSD. | Tier 1 to Tier 2: Strong empirical support from crossover trials for acute anxiety reduction and acute autonomic regulation; long-term durability debated. |
| Vocal Stimulation | Humming, Chanting (Om), Singing | Mechanical vibration of the larynx and pharynx via the recurrent laryngeal nerve. | Localized efferent vagal activation; moderate parasympathetic upregulation via proprioceptive feedback. | Tier 2: Moderate clinical evidence supporting transient improvements in autonomic tone and acute stress reduction. |
| Thermal Exposure (Hormesis) | Cold Water Immersion (CWI) | Activation of the mammalian diving reflex (trigeminal nerve) competing with massive systemic cold shock. | Immediate massive spike in norepinephrine/dopamine & inflammation; delayed (12-hour) reduction in clinical stress. | Tier 2: Supported by massive 2025 meta-analyses confirming delayed stress resilience via physiological hormetic adaptation. |
| Somatic / Mechanical Manipulation | "Vagus Reset" (Eye-rolling, Ear pulling, Rosenberg Exercise) | Stretching suboccipital fascial chains linked to extraocular muscles; superficial tactile input to the ear. | Mild, highly transient shifts in proprioception and localized fascial tension release; psychological distraction. | Tier 3 / Anecdotal: No validated neuroscientific evidence of systemic vagal reprogramming, central depolarization, or clinical anxiolytic efficacy. |
9. Conclusion
The landscape of vagus nerve stimulation and autonomic regulation is currently undergoing a rapid, highly critical maturation process. The field is aggressively moving away from the blunt, highly invasive instrument of surgical implantation, shifting decisively toward the precise, non-invasive targeting provided by advanced bioelectronic wearables. The extensive, highly powered clinical data published between 2023 and 2026 firmly establishes transcutaneous Vagus Nerve Stimulation (tVNS) as a remarkably safe, exceptionally effective, and highly durable clinical intervention for Generalized Anxiety Disorder, Treatment-Resistant Depression, and a multitude of complex mood pathologies. By intelligently and electrically targeting myelinated afferent pathways, modern medical-grade devices successfully bypass the nociceptive pain and severe perioperative risks associated with early-generation surgical implants. In doing so, they offer staggering therapeutic outcomes - including high rates of total clinical remission - that readily rival traditional pharmacotherapy, while entirely avoiding the deleterious, treatment-ending systemic side effects of SSRIs and SNRIs.
Simultaneously, as public interest in the nervous system surges to unprecedented levels, the critical necessity for stringent scientific literacy has never been higher. The viral proliferation of pseudo-neurological somatic exercises on social media - practices that promise instantaneous, permanent mental health cures through simplistic physical maneuvers - threatens to dilute and totally obscure the genuine, scientifically validated promise of autonomic medicine. True vagal neuromodulation, whether it is achieved through the precise, algorithmic electrical parameters of a clinical tVNS device, the highly disciplined physiological synchronization of resonant breathwork and Pranayama, or the extreme hormetic adaptation forced by cold water immersion, requires sustained, targeted, and biologically demanding engagement of the brainstem networks. As the field progresses into the future, the integration of rigorous, closed-loop electrical neuromodulation with scientifically validated, culturally rich behavioral practices promises to fundamentally redefine the future of psychiatric care, stress resilience, and human autonomic regulation.