Ashwagandha, L-Theanine, and Magnesium for Anxiety and Stress
Clinical Context and Evidence-Based Guidelines
The pharmacological management of clinical anxiety disorders - encompassing generalized anxiety disorder (GAD), panic disorder, and social anxiety disorder - is governed by stringent, evidence-based clinical practice guidelines. Leading psychiatric and public health authorities, including the United Kingdom's National Institute for Health and Care Excellence (NICE) and the American Psychiatric Association (APA), uniformly recommend a stepped-care approach 112. First-line interventions consistently prioritize high-intensity cognitive behavioral therapy (CBT) alongside pharmacological treatments such as selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and, in specific cases, pregabalin 11346.
Currently, major clinical practice guidelines do not endorse dietary supplements, botanical extracts, or over-the-counter nutraceuticals as primary or standalone treatments for clinical anxiety disorders 167. The Japanese Society of Anxiety and Related Disorders, for example, explicitly omits herbal supplements from its 2023 treatment algorithms, focusing exclusively on SSRIs and cognitive-behavioral interventions 67.
Despite this lack of formal psychiatric endorsement for monotherapy, epidemiological data indicates substantial consumer reliance on alternative treatments. Surveys indicate that up to 72.8% of individuals experiencing anxiety symptoms utilize herbal medicines or nutraceuticals 59. This trend is largely driven by a desire to avoid the adverse effects frequently associated with standard pharmacotherapy, including the dependency risks of benzodiazepines and the sexual dysfunction, weight gain, and withdrawal syndromes often linked to long-term SSRI or SNRI utilization 39.
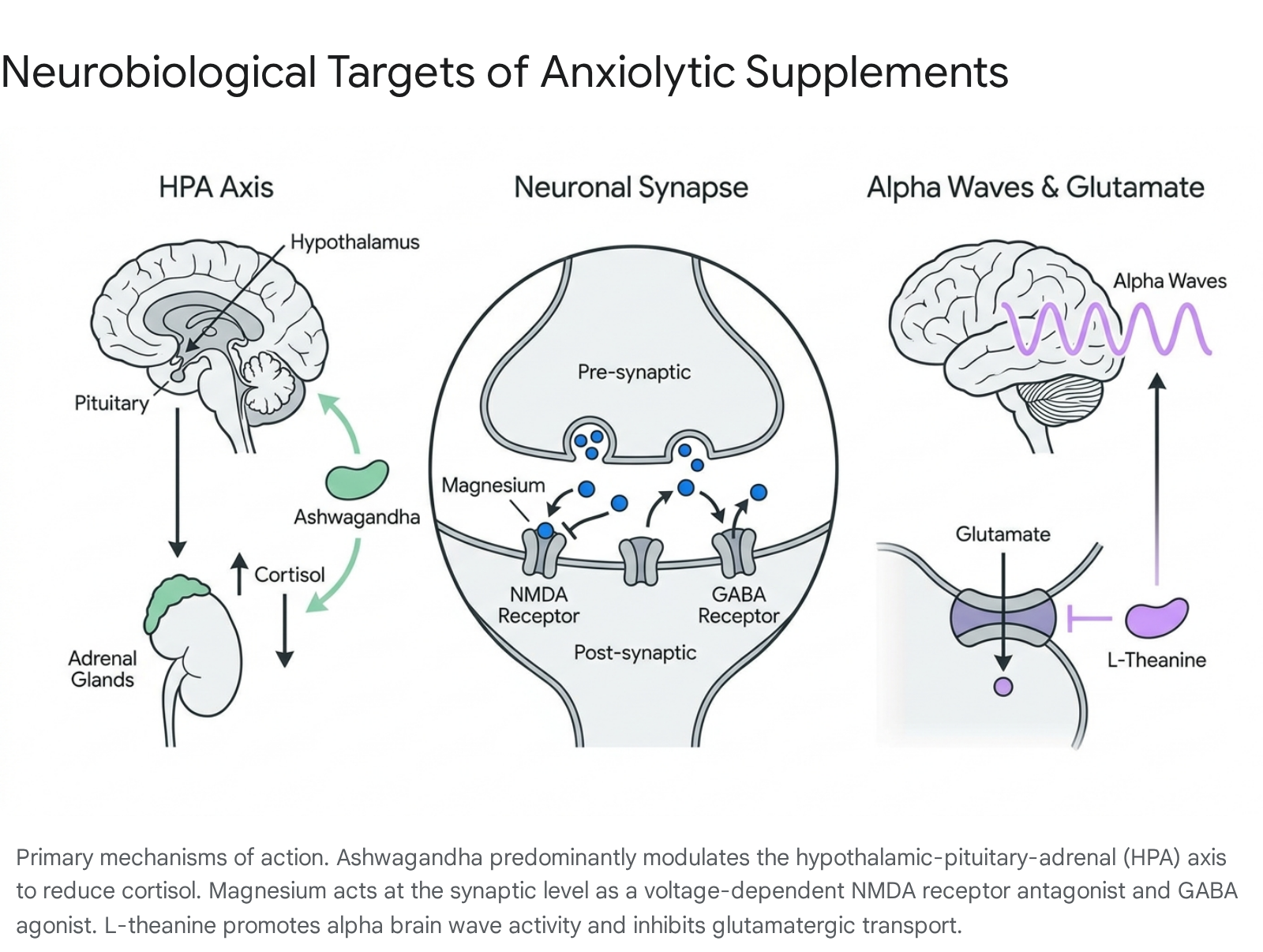
Within this landscape, three compounds command the most substantial evidence bases for the mitigation of anxiety and stress: ashwagandha (Withania somnifera), L-theanine, and magnesium glycinate. While these agents do not replace guideline-directed psychiatric care, extensive clinical literature, systematic reviews, and meta-analyses published between 2023 and 2026 indicate that they possess distinct, measurable neurobiological mechanisms. These compounds have demonstrated the capacity to modulate the hypothalamic-pituitary-adrenal (HPA) axis, regulate glutamatergic transmission, and facilitate GABAergic pathways, thereby offering significant utility as adjunctive therapies or interventions for subclinical, state-dependent stress 110678.
Ashwagandha (Withania somnifera)
Phytochemical Profile and Formulation Variances
Ashwagandha, an evergreen shrub native to India and Southeast Asia, is a foundational adaptogen within traditional Ayurvedic medicine, historically utilized as a rasayana (rejuvenator) to promote vitality, longevity, and stress resilience 91011. The plant's pharmacological activity is attributed to its complex phytochemical matrix, which includes alkaloids, saponins, and a prominent class of steroidal lactones known as withanolides 91213. Preclinical and clinical literature indicates that these withanolides, particularly withaferin A and withanolide D, are the primary bioactive constituents responsible for the herb's neuroprotective, anti-inflammatory, and anxiolytic effects 101012.
The clinical efficacy of ashwagandha is heavily contingent upon the method of preparation, the specific parts of the plant utilized (root versus leaf), and the standardization of active compounds. Traditional Ayurvedic formulations, such as Ashwagandha Ksheer Pak, involve boiling unstandardized raw root powder in milk. This lipid-based decoction is historically prescribed to enhance bioavailability, mitigate generalized weakness, and improve sleep and cardiovascular endurance 14151617. While traditional preparations maintain clinical relevance, modern psychiatric and pharmacological research predominantly relies on highly concentrated, standardized extracts.
The most extensively validated proprietary formulation in contemporary clinical trials is KSM-66. This full-spectrum extract is derived exclusively from the ashwagandha root using a water-based extraction process and is strictly standardized to contain at least 5% withanolides 1231819. Alternatively, formulations such as Sensoril incorporate both the root and the leaves, standardizing to a much higher concentration of 10% withanolide glycosides 232021. Because the leaves contain higher concentrations of cytotoxic withanolides like withaferin A, the dosing parameters for leaf-inclusive extracts differ significantly from root-only extracts 2022.
| Ashwagandha Formulation | Primary Plant Material | Standardization Profile | Typical Clinical Daily Dose | Evidence and Clinical Application |
|---|---|---|---|---|
| KSM-66 Extract | Root exclusively | 5% withanolides | 300 - 600 mg | Highest tier of modern RCT evidence. Validated for chronic stress reduction, cortisol lowering, and cognitive support 1231829. |
| Sensoril Extract | Root and Leaf | 10% withanolide glycosides | 125 - 250 mg | Strong evidence for stress and cortisol reduction. Lower required dosage due to higher concentration of specific glycosides 232021. |
| Unstandardized Root Powder | Root exclusively | Variable (batch dependent) | 3,000 - 6,000 mg | The traditional Ayurvedic baseline. Requires large physical volumes for efficacy; outcomes in clinical trials are highly variable 92023. |
| Ksheer Pak (Decoction) | Unstandardized Root | Variable | 10g powder boiled in milk | Traditional application for cardiovascular support, insomnia, and sports recovery. Modern robust meta-analytic data is limited 141516. |
Pharmacological Mechanisms and Efficacy in Anxiety
The consensus in the modern psychopharmacological literature is that ashwagandha exerts its primary stress-reducing and anxiolytic effects through the robust modulation of the hypothalamic-pituitary-adrenal (HPA) axis 10921. Chronic stress disrupts the HPA axis, leading to prolonged elevations in serum cortisol, which subsequently precipitates anxiety, sleep disruption, and metabolic dysfunction 921. Ashwagandha functions as an adaptogen by buffering this neuroendocrine response. Human clinical trials consistently demonstrate that supplementation with standardized root extract yields a statistically significant reduction in serum cortisol levels alongside subjective improvements in mood and stress resilience 10923.
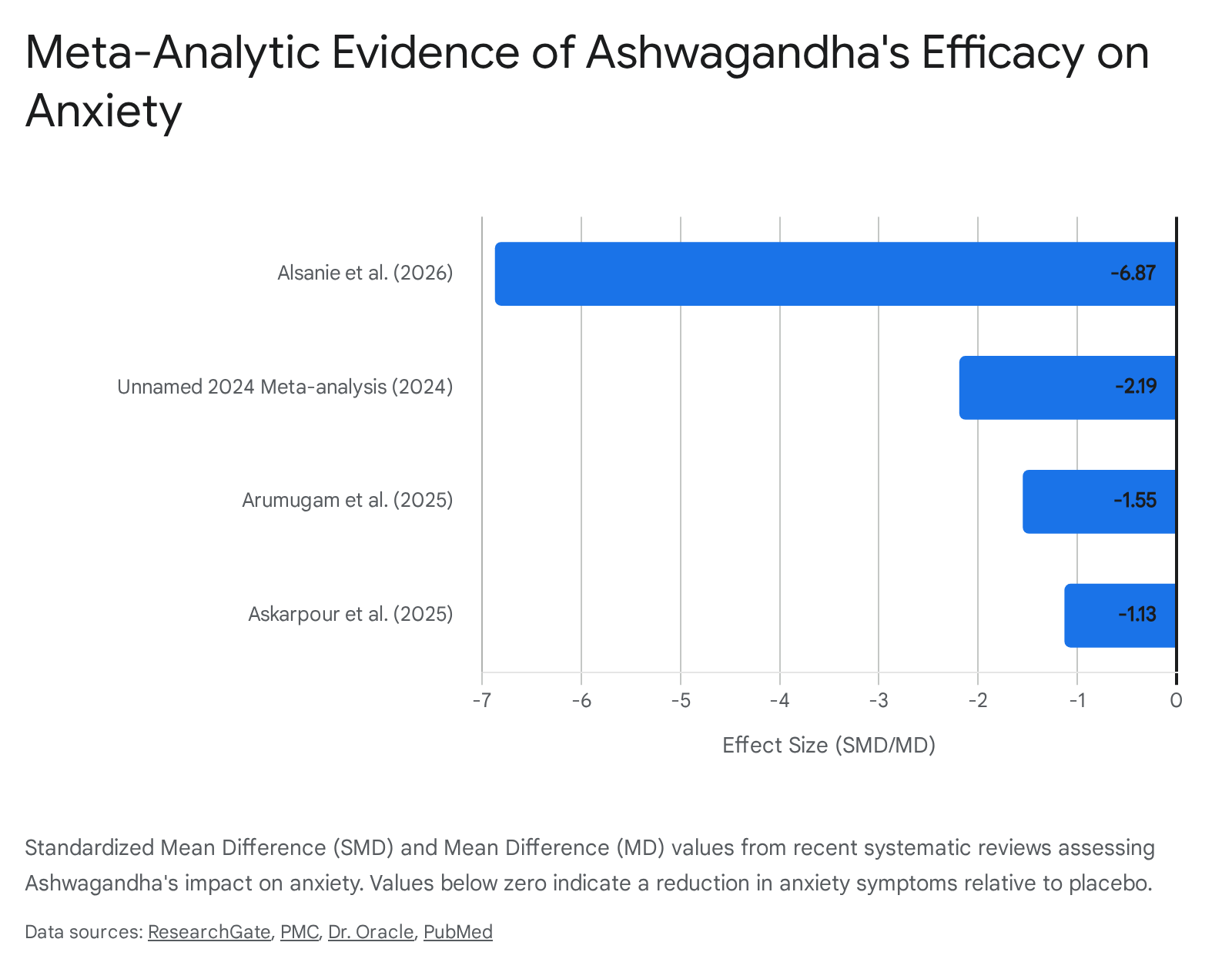
Recent systematic reviews and dose-response meta-analyses provide substantial empirical support for these mechanisms. A comprehensive 2026 meta-analysis by Alsanie et al., which pooled data from 22 randomized controlled trials, reported that ashwagandha supplementation significantly improved outcomes for stress, depression, and anxiety. The study identified a large standardized mean difference (SMD) of -6.87 (95% CI: -8.77 to -4.97) for anxiety reduction, alongside a linear and non-linear association between the administered dosage and stress levels 713.
Similarly, a 2025 systematic review and Bayesian meta-analysis by Askarpour et al., encompassing 14 studies and 360 treated patients, confirmed the efficacy of Withania somnifera in treating anxiety symptoms. This review calculated an outlier-corrected SMD of -1.13, representing a highly significant clinical effect size 2425. An additional 2024 meta-analysis encompassing 558 participants demonstrated marked reductions in both the Hamilton Anxiety Rating Scale (HAM-A) scores (Mean Difference = -2.19) and serum cortisol levels 3326.
Despite these robust effect sizes, researchers uniformly emphasize a need for calibrated interpretation. The certainty of the evidence is frequently downgraded due to substantial inter-study heterogeneity (with I2 statistics frequently exceeding 90%), publication bias, and the relatively small sample sizes of individual trials, which typically range from 50 to 100 participants 132433. Furthermore, the temporal dynamics of ashwagandha require a chronic dosing protocol; maximal anxiolytic and cortisol-regulating effects are generally observed only after 8 to 12 weeks of continuous administration 1923.
Hepatotoxicity Case Reports and Systemic Safety
Ashwagandha is broadly considered safe and well-tolerated in short-term human interventions. In rigorously monitored double-blind trials, adverse events are typically mild, consisting primarily of transient gastrointestinal discomfort, diarrhea, nausea, and mild somnolence 111927. A prospective 12-month observational study investigating the long-term administration of the standardized KSM-66 root extract in healthy adults reported no deleterious effects on hepatic, renal, or thyroid function parameters 22.
However, emerging pharmacovigilance data has introduced complexities regarding hepatic safety. A 2023 literature review identified 23 global cases of clinically apparent liver injury associated with commercial products labeled as containing ashwagandha 1128. The presentation typically involves a cholestatic or mixed pattern of liver enzyme derangement, accompanied by jaundice and pruritus, emerging 2 to 12 weeks after the initiation of the supplement 1128. While the vast majority of these instances resolve spontaneously within one to five months following cessation of the herb, rare cases of severe chronic injury or fatal liver failure have been reported 1128. The Netherlands Pharmacovigilance Centre (Lareb) also documented eight subsequent reports of liver toxicity linked to ashwagandha between September 2023 and June 2025 27.
The specific mechanism of hepatotoxicity remains a subject of intense scientific debate. Some pharmacological models propose that certain withanolides, specifically withanone, may induce hepatocellular DNA damage and deplete liver antioxidant capacity (glutathione), thereby causing direct cellular injury 2829. Conversely, industry analysts and botanical researchers argue that these case reports frequently involve unbranded, non-standardized products, raw powders, and multi-ingredient herbal jams acquired from local markets, raising the probability of adulteration, heavy metal contamination, or misidentification of the plant species 30. Furthermore, comprehensive genomic toxicity studies compliant with OECD standards demonstrate that high-quality, standardized root extracts do not exhibit mutagenic or hepatotoxic properties 29. As a calibrated clinical precaution, patients with pre-existing hepatic impairment or those utilizing multiple potentially hepatotoxic medications are advised to exercise vigilance and monitor liver function if initiating high-dose ashwagandha protocols.
The Anhedonia and Receptor Subsensitivity Debate
A secondary safety concern surrounding ashwagandha stems largely from anecdotal reports circulating on social media platforms, wherein users describe symptoms of "emotional blunting," apathy, or anhedonia (the inability to experience pleasure) following chronic, long-term administration 313233. The theoretical neuropharmacological mechanism proposed for this phenomenon suggests that by increasing the synaptic availability of serotonin, prolonged ashwagandha use might induce 5-HT1A receptor subsensitivity and downregulation - a neuro-adaptive process well-documented in the chronic use of SSRIs 103132.
Despite the proliferation of these claims, rigorous review of the clinical literature published through 2025 reveals no empirical substantiation linking ashwagandha to clinical anhedonia 3233. Across numerous double-blind, placebo-controlled trials designed to measure mood, quality of life, and cognitive function, ashwagandha consistently demonstrates broad improvements in emotional health without inducing emotional numbness or apathy 323334. Medical providers evaluating patients for emotional blunting during ashwagandha use prioritize ruling out underlying depressive disorders, natural disease progression, or unacknowledged polypharmacy interactions 43. Nonetheless, because the long-term safety profile of continuous ashwagandha administration beyond 90 days remains incompletely mapped, many holistic practitioners suggest cycling the supplement (e.g., 8 weeks on, 4 weeks off) to prevent theoretical receptor attenuation 2333.
Magnesium Glycinate
Neurobiological Mechanisms and Glutamatergic Regulation
Magnesium is the seventh most abundant element on Earth and a critical intracellular cation within human physiology, serving as a requisite cofactor in over 300 enzymatic reactions, ranging from ATP synthesis to DNA repair and neuromuscular function 35364647. Within the central nervous system, magnesium plays an indispensable role in maintaining neuro-electrical stability, modulating neuroinflammation, and regulating neurotransmitter dynamics 474849.
The primary psychiatric relevance of magnesium lies in its function as a physiological "brake" on the nervous system. It achieves this by acting as a voltage-dependent endogenous antagonist at the N-methyl-D-aspartate (NMDA) receptor 64950. The NMDA receptor is the primary excitatory gateway in the brain, activated by glutamate. Under conditions of acute or chronic stress, excessive glutamatergic transmission leads to hyper-arousal and excitotoxicity. Magnesium physically blocks the calcium channel of the NMDA receptor, preventing this pathological influx of calcium and thereby mitigating neurological overstimulation 4749.
Simultaneously, magnesium acts synergistically with Gamma-Aminobutyric Acid (GABA), the central nervous system's principal inhibitory neurotransmitter. It enhances the binding potential of GABA to its respective receptors, facilitating postsynaptic inhibitory potentials that promote deep physiological relaxation and a dampening of sympathetic nervous system outflow 484950. Clinical research corroborates these mechanistic models, demonstrating a clear inverse correlation between serum or cerebrospinal fluid magnesium levels and the manifestation of anxiety and mood disorders; individuals with magnesium insufficiency frequently exhibit heightened stress reactivity, fragmented sleep architecture, and autonomic instability 64851.
Formulation Comparisons and Bioavailability
The clinical efficacy of any magnesium intervention is fundamentally constrained by its bioavailability, absorption kinetics, and gastrointestinal tolerability. The specific molecule to which the elemental magnesium is bound dictates these variables.
Magnesium oxide is the most ubiquitous and inexpensive form available commercially. However, it is an inorganic salt characterized by exceptionally poor fractional absorption, estimated at approximately 4% 465253. Because the vast majority of the compound remains unabsorbed in the intestinal lumen, it exerts a strong osmotic effect, drawing water into the bowel. Consequently, magnesium oxide is highly effective as an acute laxative for constipation but is clinically inadequate for raising systemic or neural magnesium levels to treat psychiatric or cognitive conditions 465253. Magnesium citrate offers improved bioavailability over oxide, utilizing an organic acid bond, but it retains mild to moderate osmotic laxative properties at therapeutic doses, limiting its tolerability for daily psychiatric supplementation 4654.
For the targeted treatment of anxiety, hyper-arousal, and insomnia, magnesium glycinate (also referred to as magnesium bisglycinate) is the established clinical standard. This formulation utilizes an amino acid chelate, binding elemental magnesium to two molecules of glycine 365254. This chelation allows the compound to bypass competitive mineral absorption pathways in the small intestine, resulting in high systemic bioavailability without the osmotic gastrointestinal disruption associated with inorganic salts 5254. Crucially, the glycine carrier contributes an independent pharmacological benefit: glycine acts as an inhibitory neurotransmitter in its own right, further modulating NMDA receptors and amplifying the profound calming effect on the central nervous system 465254.
Blood-Brain Barrier Permeability and Clinical Efficacy
A significant theoretical debate within nutritional psychiatry concerns the relative ability of different magnesium formulations to cross the highly selective blood-brain barrier (BBB). Standard forms, including glycinate, citrate, and chloride, are undeniably effective at raising systemic serum levels, which indirectly supports overall neurological function and corrects systemic deficiencies 5537.
However, a patented compound known as magnesium L-threonate (Magtein) was specifically engineered to maximize BBB permeability. Synthesized by bonding magnesium to L-threonic acid (a metabolite of vitamin C), preclinical rodent models and early human trials suggest that L-threonate can uniquely elevate magnesium concentrations directly within the cerebrospinal fluid 53373839. This targeted neural delivery has led to its promotion primarily for cognitive applications, such as enhancing working memory, mitigating neurodegeneration, and improving synaptic plasticity 473839.
Despite the targeted neural absorption of L-threonate, magnesium glycinate remains the superior choice for the specific indications of sleep architecture disruption and state anxiety. The established clinical data for glycinate demonstrates robust reductions in somatic tension and improved sleep onset latency, driven by the synergistic GABAergic properties of both the magnesium ion and the glycine molecule 54553940.
A 2024 systematic review investigating the effects of supplemental magnesium on subjective anxiety and sleep quality identified 15 interventional trials that met rigorous inclusion criteria 641. Five out of seven studies specifically measuring anxiety-related outcomes (utilizing tools such as the Hamilton Anxiety Rating Scale) reported positive results, indicating significant reductions in self-reported anxiety 6. The magnitude of the anxiolytic effect was frequently dose-dependent, with the most pronounced clinical improvements observed in trials utilizing higher comparative doses (e.g., 300 mg or more of elemental magnesium daily) and in patient cohorts exhibiting baseline hypomagnesemia or high vulnerability to stress 64842. The systematic reviews conclude that, while large-scale randomized trials remain necessary to definitively establish standardized psychiatric protocols, highly bioavailable forms like magnesium glycinate represent a safe and effective mechanism for alleviating mild-to-moderate anxiety and correcting stress-induced sleep disturbances 65041.
| Magnesium Formulation | Bonding Agent | Bioavailability & Tolerability | Primary Clinical Indication |
|---|---|---|---|
| Magnesium Glycinate | Glycine (amino acid) | High absorption; bypasses osmotic pathways; minimal GI disruption. | Generalized anxiety, sleep onset insomnia, nocturnal muscle cramps 46543940. |
| Magnesium L-Threonate | L-threonic acid (Vitamin C derivative) | High absorption; specifically engineered for enhanced blood-brain barrier transport. | Cognitive enhancement, working memory support, neuroprotection 46533839. |
| Magnesium Citrate | Citric acid | High absorption; exerts mild to moderate osmotic laxative effects. | General systemic magnesium repletion, mitigation of mild constipation 4654. |
| Magnesium Oxide | Oxygen (inorganic salt) | Exceptionally low absorption (~4%); strong osmotic pull. | Acute relief of severe constipation; ineffective for psychiatric or neurological outcomes 465253. |
L-Theanine: Acute Stress Modulation
Pharmacodynamics and Alpha Wave Induction
L-theanine (γ-glutamylethylamide) is a naturally occurring, non-proteinogenic amino acid found predominantly in the leaves of the green tea plant (Camellia sinensis) 843. In stark contrast to ashwagandha or magnesium - which function as systemic regulators requiring days or weeks to achieve steady-state therapeutic efficacy - L-theanine exhibits a rapid and acute pharmacokinetic profile. Following oral administration, the compound permeates the blood-brain barrier via the leucine-preferring transport system within 30 minutes, achieving peak plasma concentrations between 30 and 120 minutes 8.
The anxiolytic mechanism of L-theanine operates through multiple, simultaneous pathways in the central nervous system. Primarily, it acts as a competitive inhibitor of the glutamine transporter, directly suppressing the conversion of glutamine into the excitatory neurotransmitter glutamate 8. Concurrently, it facilitates the release of GABA and modulates the concentration of monoamines, including dopamine and serotonin, in specific cortical and striatal regions 8.
The most distinguishing clinical feature of L-theanine is its capacity to significantly increase the generation of alpha brain wave activity (8 - 12 Hz) 63. Alpha waves are the electroencephalographic (EEG) correlate of a state of "relaxed wakefulness" and focused attention. By inducing this neuro-electrical state, L-theanine effectively attenuates subjective stress and hyper-arousal without inducing the somnolence, motor impairment, or cognitive blunting characteristic of traditional pharmacological sedatives or benzodiazepines 4963.
Clinical Efficacy in State Anxiety vs. Trait Anxiety
The clinical evidence base dictates that L-theanine is highly effective for highly specific, event-driven use cases, but lacks the robust data required to support its use as a continuous monotherapy for chronic psychiatric disorders.
A comprehensive 2024 systematic review evaluating 11 randomized controlled trials (RCTs) across multiple countries concluded that L-theanine supplementation significantly reduced psychiatric symptoms in cohorts diagnosed with anxiety disorders, schizophrenia, and Attention-Deficit/Hyperactivity Disorder (ADHD) compared to placebo controls 744. In specific stress-induction models, daily doses of 200 to 400 mg over 28 days yielded measurable decreases in Perceived Stress Scale scores, improved sleep quality, and enhanced selective attention during cognitively demanding tasks 763.
However, the efficacy of the compound diminishes significantly when evaluated against generalized, unprovoked anxiety (trait anxiety). A rigorously designed 2019 double-blind RCT involving patients explicitly diagnosed with DSM-5 Generalized Anxiety Disorder (GAD) found that adjunctive L-theanine (administered at high doses of 450 to 900 mg daily) failed to outperform a placebo in reducing baseline anxiety on validated rating scales over an eight-week period 7. Furthermore, an earlier experimental study comparing the acute effects of 200 mg of L-theanine directly against the benzodiazepine alprazolam during an induced anxiety state found no significant anxiolytic superiority for the amino acid 743.
Consequently, evidence-based psychiatric guidelines do not position L-theanine alongside SSRIs for the structural management of GAD or panic disorder. Instead, its clinical utility is optimized as an acute, prophylactic interventional tool. It is most effectively utilized at doses of 200 to 400 mg, administered 30 to 60 minutes prior to a known psychological stressor (such as public speaking, intense cognitive tasks, or acute situational panic) to blunt sympathetic nervous system hyperactivation and maintain executive function 178.
Comparative Pharmacodynamics and Adjunctive Strategies
When integrating these three compounds into a broader strategy for mental health and neurological resilience, clinicians and patients must differentiate between continuous physiological regulation and acute symptom management. The interventions do not function interchangeably; rather, they address distinct biological timelines and targets within the stress-response architecture.
Ashwagandha operates as a long-wave intervention. It requires 4 to 8 weeks of continuous, daily dosing to sufficiently downregulate HPA axis hypersensitivity, lower baseline cortisol levels, and restore endocrine balance 1923. It is clinically optimized for chronic stress profiles, occupational burnout, and sustained, low-grade generalized anxiety.
Magnesium glycinate functions as a foundational neuro-electrical stabilizer. While patients may perceive mild immediate relaxation due to the glycine component, its primary psychiatric value lies in correcting the underlying systemic mineral deficiencies that exacerbate neurotransmitter imbalances, NMDA hyperactivation, and the degradation of sleep architecture. Tangible results typically manifest within 1 to 2 weeks of consistent administration 14854.
L-theanine, conversely, provides immediate, event-driven relief. Its rapid BBB penetration, glutamatergic inhibition, and alpha-wave induction render it a highly effective prophylactic agent against acute panic or situational stress, providing measurable anxiolytic effects within an hour of oral ingestion 18.
| Compound | Target Mechanism | Onset of Action | Primary Clinical Application |
|---|---|---|---|
| Ashwagandha (KSM-66) | HPA Axis regulation; cortisol reduction. | 4 to 8 weeks of continuous use 123. | Chronic stress, prolonged generalized anxiety, endocrine exhaustion 19. |
| Magnesium Glycinate | NMDA antagonism; GABA receptor facilitation. | 1 to 2 weeks of continuous use 154. | Correcting neuro-electrical instability, treating sleep-onset insomnia, baseline hyper-arousal 649. |
| L-Theanine | Glutamate inhibition; Alpha brain wave induction. | 30 to 60 minutes post-ingestion 18. | Acute situational stress, performance anxiety, maintaining focus without sedation 78. |
The simultaneous integration of these three supplements is increasingly common in both clinical nutritional psychiatry and the consumer wellness market. This poly-supplementation is generally considered safe and mechanistically sound, as the compounds possess non-overlapping primary mechanisms of action and present a low risk of adverse drug-drug interactions. However, polypharmacy - even involving natural compounds - requires diligent clinical monitoring, particularly regarding cumulative mild sedating effects and potential interactions with prescribed psychiatric medications. Ultimately, while none of these compounds are recommended as replacements for pharmaceutical interventions when clinical severity dictates the need for SSRIs or CBT, they represent the most scientifically validated, evidence-backed adjunctive tools available for the non-pharmacological regulation of the human stress response 16.