Does Science Support Senolytics or Antioxidants for Aging
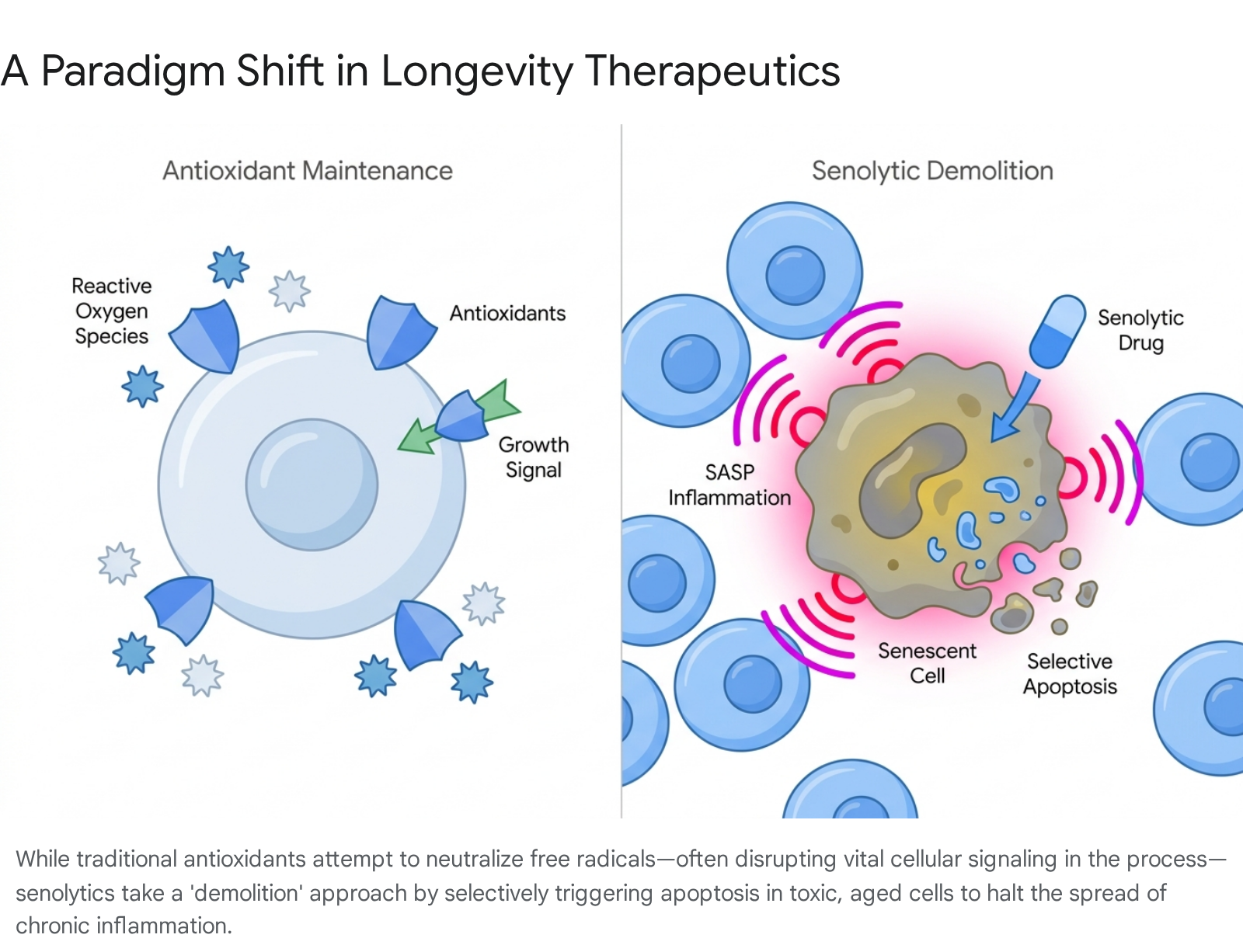
Science overwhelmingly demonstrates that daily antioxidant supplements fail to slow human aging and can actively interfere with the body's vital cellular repair mechanisms. In contrast, emerging clinical evidence supports senolytics - intermittent therapies that actively hunt and destroy toxic, aged cells - as a more promising, albeit highly experimental, strategy for reversing tissue dysfunction and extending human healthspan.
The Promise and Failure of the Antioxidant Paradigm
For decades, the global anti-aging industry has been heavily anchored to the free radical theory of aging. Conceived in the 1950s by Denham Harman, this theory provided a neat, intuitive explanation for why our bodies deteriorate over time 123. The premise relies on the fundamental mechanics of cellular respiration. When our mitochondria convert oxygen and nutrients into adenosine triphosphate (ATP) for energy, they inevitably produce highly unstable metabolic byproducts known as reactive oxygen species, or free radicals 234.
Because these molecules contain an unpaired electron, they aggressively seek out other molecules to steal electrons from, causing oxidative damage to cell membranes, proteins, and even nuclear and mitochondrial DNA 235. Over years and decades, this cumulative oxidative stress was believed to be the primary engine driving senescence, tissue degradation, and the onset of age-related conditions like cardiovascular disease, Alzheimer's, and cancer 2356.
The logical countermeasure birthed a multi-billion-dollar wellness industry: antioxidants. Antioxidants are molecules - either produced naturally by the body or consumed through diet and supplements - that can safely donate an electron to a free radical without becoming unstable themselves 2. The prevailing public assumption became that flooding the body with exogenous antioxidants, such as high-dose vitamin C, vitamin E, and beta-carotene, would neutralize the biological wear and tear of aging 17. Today, the global anti-aging supplement market continues to expand rapidly, projected to reach nearly ten billion dollars over the next decade 89.
Why Antioxidant Supplements Falter in Humans
Despite their popularity, the scientific consensus regarding antioxidant supplements has shifted dramatically. While antioxidants reliably quench free radicals in a test tube, human biology is far less accommodating. The vast majority of over-the-counter antioxidant supplements suffer from incredibly poor bioavailability. They are difficult for the human digestive tract to absorb, are often chemically transformed in the liver, and are rapidly eliminated before they can effectively reach target cells in meaningful concentrations 9.
More critically, rigorous epidemiological data has delivered a severe blow to the idea that antioxidant supplementation extends human lifespan. A sweeping meta-analysis analyzing mortality data from randomized controlled trials involving over two hundred thousand initially healthy subjects found no evidence that supplemental antioxidants improve survival 710. The data proved even more alarming: the analysis convincingly demonstrated that high-dose supplementation with specific antioxidants, including beta-carotene, vitamin A, and vitamin E, may actually increase all-cause mortality compared to placebo 710.
Furthermore, evidence suggests that excessive antioxidant intake can be specifically harmful in patients with active malignancies, as an overabundance of antioxidants can inadvertently protect cancer cells from the oxidative stress that would otherwise destroy them, potentially accelerating tumor growth 1. Acknowledging this mounting evidence, institutions like the United States Department of Agriculture went so far as to remove their database of antioxidant food values, citing that the numbers had no direct relevance to human health outcomes and were routinely misused by supplement manufacturers to market ineffective products 9.
The Hormesis Paradox and Exercise Interference
The most glaring flaw in the free radical theory of aging is its failure to account for the concept of mitohormesis. Hormesis is a biological phenomenon wherein exposure to a mild, transient stressor triggers an adaptive response that leaves the organism stronger and more resilient to future stress 12.
Reactive oxygen species are not universally destructive rogue elements; they play an indispensable role as intracellular signaling molecules. When you engage in physical exercise, your muscle cells demand massive amounts of energy, causing your mitochondria to produce a localized surge of free radicals 41113. Rather than causing permanent damage, this acute oxidative stress activates critical signaling pathways. Molecules like hydrogen peroxide act as messengers, signaling to kinases and transcription factors - such as AMPK, p38 MAPK, and the Keap1-Nrf2 pathway - that the muscle is under strain 41112.
These signals prompt the cell to adapt by building new, highly efficient mitochondria and massively upregulating the body's own endogenous antioxidant defense systems, such as superoxide dismutase, catalase, and glutathione peroxidase 131213. This intrinsic response is far more powerful than any pill.
However, when athletes or aging adults consume high doses of exogenous antioxidant supplements immediately before or after a workout, they artificially neutralize these free radicals before the signaling cascade can occur 1113. By muting the oxidative signal, the supplements effectively blind the cells to the stress of exercise. Extensive research demonstrates that this practice can blunt or entirely prevent the beneficial adaptations of physical training, including improvements in insulin sensitivity, vascular function, and muscle hypertrophy 111216. In short, the attempt to aggressively maintain cellular perfection with antioxidants actually prevents the body from fortifying itself.
The Biology of Cellular Senescence
With the limitations of the antioxidant paradigm clearly established, the field of geroscience shifted its focus toward a much more fundamental root cause of aging and chronic disease: cellular senescence.
The concept was first documented in 1961 by scientists Leonard Hayflick and Paul Moorhead, who observed that normal human somatic cells grown in a laboratory do not divide infinitely 141516. After a certain number of population doublings - now known as the Hayflick limit - the cells cease replication entirely 1516. We now understand that this replicative senescence is primarily driven by telomere attrition. With each cell division, the protective caps at the ends of our chromosomes shorten. Once they become critically short, the cell triggers a permanent arrest of the cell cycle to prevent the replication of corrupted genetic material 131517.
However, telomere shortening is not the only trigger. Cells can be forced into premature senescence by a variety of severe intrinsic and extrinsic stressors. These include irreparable DNA double-strand breaks, severe oxidative stress, oncogene activation, radiation exposure, and profound mitochondrial dysfunction 131516.
How a Healthy Cell Becomes a Zombie
When a cell detects critical damage, it faces a biological crossroads. If the damage is overwhelming, the cell may trigger apoptosis, a clean, highly regulated form of programmed cell death where the cell is dismantled and its components are recycled by the immune system 318. Alternatively, the cell may activate tumor suppressor pathways, primarily the p53/p21CIP1 and p16INK4A/pRB networks, locking the cell into a state of essentially irreversible growth arrest 151619.
In a young, healthy organism, this senescence program is a highly beneficial, evolutionarily conserved defense mechanism. It is a potent anti-cancer safeguard, ensuring that mutated or severely damaged cells cannot proliferate and form tumors 151619. Furthermore, transient senescence plays vital physiological roles during embryonic development and tissue repair. For example, during wound healing, senescent cells help coordinate the initial stages of tissue remodeling before being efficiently cleared away by a robust immune system 1920.
The problem arises chronologically. As we age, the rate at which we generate damaged cells increases, while our immune system's ability to locate and eliminate these cells simultaneously declines - a phenomenon known as immunosenescence 1417. Consequently, these non-dividing, damaged cells begin to accumulate in our skin, blood vessels, adipose tissue, joints, and brain 1421.
The Senescence-Associated Secretory Phenotype (SASP)
Senescent cells are frequently referred to as "zombie cells" in popular media because they refuse to undergo normal cell death, yet they are far from biologically inactive. Once a cell enters a persistent senescent state, it undergoes dramatic metabolic reprogramming and begins to express what is known as the Senescence-Associated Secretory Phenotype, or SASP 151619.
The SASP is a complex, toxic localized environment. The zombie cell continuously secretes a potent cocktail of pro-inflammatory cytokines (such as Interleukin-6 and Interleukin-1-beta), chemokines, growth factors, and tissue-degrading matrix metalloproteinases 131519. Originally, the evolutionary purpose of this secretion was to act as an emergency flare, signaling the immune system to come and clear the damaged cell while temporarily halting the growth of nearby healthy cells 1319.
However, when senescent cells persist for months or years, their continuous SASP secretions wreak havoc on surrounding tissue architecture. This chronic, sterile, low-grade inflammation is termed "inflammaging," and it is widely considered a root driver of tissue degeneration 1417. The SASP degrades the extracellular matrix, impairs the function of local adult stem cells, and can even induce neighboring, perfectly healthy cells to become senescent in a destructive paracrine cascade 141922.
Preclinical studies underscore just how destructive these cells can be. Researchers have demonstrated that injecting a vanishingly small number of senescent cells - as few as one in ten thousand - into the knee joints or abdominal cavities of young, healthy mice is sufficient to induce physical frailty, osteoarthritis-like symptoms, and significantly shorten their natural lifespan 2123. Conversely, researchers theorized that if they could safely remove these accumulating zombie cells, they might fundamentally delay or alleviate multiple age-related disorders simultaneously 141521.
Senolytics: The Demolition Strategy for Longevity
The realization that senescent cells act as active drivers of age-related pathology birthed a completely new therapeutic paradigm. In 2015, researchers at the Mayo Clinic, led by Dr. James Kirkland and Dr. Tamar Tchkonia, coined the term "senolytics" - a portmanteau of senescence and lytic (destroying) 142122. Unlike antioxidants, which attempt to maintain and protect existing cellular machinery, senolytics are demolition agents designed to selectively hunt and kill senescent cells without harming healthy tissue 182224.
The central challenge of developing a senolytic is selectivity. How do you kill a senescent cell while sparing the healthy cells surrounding it? The answer lies in the zombie cell's own defense mechanisms.
Exploiting Anti-Apoptotic Pathways (SCAPs)
Because senescent cells are constantly generating an incredibly toxic, pro-inflammatory internal environment, they should theoretically self-destruct 22. To survive their own toxicity, senescent cells uniquely upregulate a series of pro-survival networks known as Senescent Cell Anti-Apoptotic Pathways, or SCAPs 1828. These molecular shields - which include the BCL-2 protein family, PI3K/Akt pathways, and specific tyrosine kinases - prevent the cell from undergoing programmed apoptosis 131825.
Senolytic agents exploit this specific biological vulnerability. By deploying drugs that temporarily disable these SCAP networks, the senescent cell's biological shields drop. Unable to withstand its own toxic environment, the senescent cell rapidly undergoes apoptosis 182830. Healthy cells, which do not rely on these hyper-activated survival pathways, remain largely unaffected by the brief chemical intervention 1828.
The Crucial Hit-and-Run Dosing Protocol
Perhaps the most radical departure from traditional pharmacological treatments and nutritional supplementation is how senolytics are administered. Chronic diseases like hypertension or hypercholesterolemia generally require continuous, daily medication. Antioxidant supplements are similarly consumed every single morning. Senolytics, however, are administered using an intermittent, "hit-and-run" protocol 223126.
The biological rationale for this is straightforward. It takes a damaged cell roughly two to six weeks to fully enter a senescent state and develop the tissue-damaging SASP profile 252734. Therefore, there is no need to keep senolytic drugs continuously circulating in the bloodstream. In clinical trials, patients typically consume high doses of senolytics for just two or three consecutive days, followed by a prolonged treatment-free window of several weeks or even months 2829.
This hit-and-run approach offers immense clinical advantages. First, the goal is not to achieve a steady-state blood concentration, but rather to trigger the apoptotic cascade; once the suicide sequence is initiated in the zombie cell, the drug's job is done and it can be rapidly cleared from the body 2630. Second, minimizing the patient's exposure time to these highly potent compounds drastically mitigates the risk of severe side effects, off-target toxicity, and immune suppression 312628.
When Antioxidants Become Targeted Toxins
A fascinating nuance in senotherapeutics is that some of the most promising natural senolytic compounds - like quercetin and fisetin - are actually classified as flavonoids and dietary antioxidants 162829. This begs the question: how does an antioxidant kill a cell?
The answer lies in the unique metabolic state of the senescent cell, combined with the massive doses utilized in senolytic protocols. While these compounds may act as gentle free radical scavengers at standard dietary levels, they exhibit powerful prooxidant activities when administered in heavy, concentrated bursts 30. Senescent cells tend to accumulate high intracellular levels of transition metals, particularly iron and copper. When high-dose flavonoids interact with these metals inside the zombie cell, the reaction amplifies the prooxidant effect, generating massive oxidative damage that overloads the senescent cell's defenses and kills it 30.
Thus, in the context of senolytic therapy, these compounds are not functioning to buffer age-related wear and tear; they are being weaponized to target the unique metabolic vulnerabilities of aged cells.
Strategy Comparison Summary
| Feature | The Antioxidant Paradigm | The Senolytic Paradigm | The Senomorphic Paradigm |
|---|---|---|---|
| Primary Mechanism | Neutralizes reactive oxygen species (ROS) to prevent molecular oxidation and DNA damage. | Disables anti-apoptotic pathways (SCAPs) to induce death in senescent cells. | Modulates cellular pathways to suppress the inflammatory SASP without killing the cell. |
| Dosing Schedule | Continuous, daily nutritional supplementation. | Intermittent "hit-and-run" (e.g., 2 days on, weeks/months off). | Chronic or sustained administration, similar to traditional disease management. |
| Impact on Signaling | Can inadvertently blunt vital physiological adaptations, such as exercise-induced mitochondrial growth. | Halts pathological signaling permanently by removing the cells generating the SASP. | Reversibly suppresses pathological signaling; inflammation may return if the drug is stopped. |
| Clinical Efficacy | Failed to extend lifespan in rigorous human trials; high doses may increase all-cause mortality. | Shown to extend healthspan in mice; early human trials show reduced senescent burden and functional benefits. | Strong preclinical data for alleviating fibrosis and neurodegeneration; early human trials ongoing. |
| Current Safety Profile | Generally safe at dietary levels, but high-dose isolates suffer from poor bioavailability and toxicity risks. | Investigational. Carries risks of cytopenia and off-target cell death depending on the pharmaceutical agent used. | Investigational. Carries risks of broad immune suppression due to sustained pathway inhibition. |
Leading Senolytic Agents in Clinical Development
The field of senotherapeutics is highly diverse, utilizing everything from repurposed chemotherapy agents to synthetic peptides and concentrated plant extracts. Because senescent cells are highly heterogeneous - meaning a senescent fat cell utilizes different survival mechanisms than a senescent brain cell - no single drug clears all zombie cells throughout the body 2231. Consequently, researchers frequently combine agents.
Dasatinib and Quercetin (D+Q)
The most extensively documented and rigorously tested senolytic regimen to date is the combination of Dasatinib and Quercetin (D+Q) 283233. Dasatinib is an FDA-approved tyrosine kinase inhibitor originally developed as a targeted chemotherapy for chronic myeloid leukemia 2834. Quercetin is a naturally occurring plant polyphenol found in apples, onions, and capers 162932.
The rationale for the combination is purely synergistic. In preclinical screening, researchers discovered that Dasatinib is highly effective at inducing apoptosis in senescent human preadipocytes (fat cells) and endothelial cells, while Quercetin more efficiently targets senescent human endothelial cells and bone marrow-derived mesenchymal stem cells 2842. By combining them, researchers cast a wider biological net, successfully clearing a broader range of tissue-damaging cells.
In animal models, the D+Q cocktail has demonstrated staggering results, delaying or alleviating over 40 age-related conditions, including osteoporosis, insulin resistance, vasomotor dysfunction, liver steatosis, and neurodegeneration, while extending the healthspan of naturally aged mice 253033.
However, Dasatinib is a highly potent pharmaceutical with a non-trivial risk profile. When used continuously in oncology, it carries severe hematologic toxicity risks, including life-threatening neutropenia and thrombocytopenia (dangerously low platelet counts), as well as pleural effusion (fluid around the lungs) 183028. Dasatinib is also a CYP3A4 substrate, meaning it interacts dangerously with common medications like erythromycin and certain antifungals 30. While the hit-and-run dosing schedule minimizes these dangers, D+Q remains an aggressive experimental intervention, not a consumer wellness supplement 312628.
Fisetin: The Strawberry Flavonoid
Driven by the need for safer, lower-toxicity alternatives, researchers expanded their screening of natural compounds. Fisetin, a flavonoid structurally similar to quercetin and found naturally in strawberries and cucumbers, quickly emerged as a frontrunner 162831.
In a comprehensive panel testing ten different flavonoids in mice suffering from accelerated aging (progeria), fisetin proved to be the most potent senolytic monotherapy, successfully reducing the accumulation of p16 and p21-positive senescent cells in adipose tissue, the spleen, liver, and kidneys 2942. Remarkably, even when administered to mice very late in life - roughly equivalent to a human starting treatment at age 60 or 70 - fisetin preserved grip strength, reduced systemic inflammation, and extended their remaining lifespan 2531.
Fisetin's appeal lies in its dual action and safety profile. It acts as both a senolytic (killing cells by exploiting prooxidant vulnerability) and a potent senomorphic (inhibiting the mTOR pathway to slow the rate at which healthy cells become senescent) 222831. It lacks the severe hematologic risks associated with chemotherapy drugs, making it an attractive candidate for human clinical translation 3031.
It is vital to note that dietary consumption of strawberries cannot replicate these effects. To achieve the necessary pharmacokinetic threshold for senolysis in humans, clinical trials utilize massive oral doses of highly bioavailable fisetin extract (typically 20 mg/kg/day) - a concentration equivalent to consuming 15 pounds of raw strawberries in a matter of minutes 3435.
BCL-2 Inhibitors and Navitoclax
Beyond D+Q and fisetin, synthetic molecules designed to inhibit specific anti-apoptotic proteins are moving through the pipeline. Navitoclax (ABT-263), a potent inhibitor of the BCL-2 family of survival proteins, has shown high efficacy in clearing senescent cells in varied tissues in mice 182844. However, its clinical development as a systemic anti-aging drug has been severely hampered by dose-limiting toxicity. Because platelets heavily rely on the BCL-xL protein for survival, Navitoclax causes immediate and profound thrombocytopenia, rendering it too dangerous for broad prophylactic use in otherwise healthy older adults 1831. Consequently, companies are exploring localized delivery systems for these potent synthetics, such as injecting them directly into arthritic joints or the eye 3136.
Human Clinical Trials: What the Data Shows So Far
The transition from extending the healthspan of mice to treating chronic human disease is currently unfolding across dozens of registered clinical trials worldwide 2337. Because it is difficult to gain regulatory approval to treat "aging" as a disease, the first wave of human senolytic trials is explicitly targeting severe, localized conditions driven by cellular senescence 2538.
Idiopathic Pulmonary Fibrosis and Kidney Disease
The very first proof-of-concept human trials for senolytics targeted idiopathic pulmonary fibrosis (IPF) - a fatal, progressive scarring of the lungs where senescent cells are known to aggregate and drive fibrotic tissue remodeling 253638. In a pilot study, patients with IPF received nine intermittent doses of D+Q over three weeks. The results demonstrated the first evidence of functional improvement in humans, with patients exhibiting measurable increases in their six-minute walk distance, walking speed, and chair-rise ability - improvements rarely seen in a disease characterized by relentless decline 3839.
Subsequent phase 2 trials at the Mayo Clinic evaluated D+Q in patients suffering from diabetic chronic kidney disease. Following a brief three-day treatment regimen, researchers biopsied the patients' adipose tissue and drew blood. The data proved critical: the short burst of D+Q successfully reduced the total burden of senescent cells in the fat tissue and significantly decreased the levels of circulating inflammatory SASP factors in the bloodstream 303149. This confirmed that senolytics successfully engage their biological targets in living humans.
Alzheimer's Disease: The SToMP-AD Trial
Given the devastating lack of curative treatments for neurodegeneration, the potential for senolytics to treat Alzheimer's disease is generating massive scientific interest. Preclinical models established that cellular senescence is mechanistically linked to the accumulation of toxic tau proteins and amyloid-beta plaques in the brain 404152.
The SToMP-AD phase 1 clinical trial, conducted by the University of Texas Health Science Center, was the vanguard study testing senolytics in the human brain. Five patients (aged 70 to 82) with early-stage symptomatic Alzheimer's disease were administered intermittent D+Q over 12 weeks 405342.
The primary goal of the trial was safety and to determine if the drugs could cross the highly selective blood-brain barrier. The trial succeeded on both fronts: dasatinib was clearly detected in the cerebrospinal fluid (CSF) of the participants, and the regimen was well-tolerated with no severe adverse events or early discontinuations 404152. Biomarker analysis revealed significant increases in IL-6 and GFAP levels in the CSF immediately post-treatment, coupled with decreases in other senescence-related chemokines 4152. Researchers hypothesize that this transient spike in specific inflammatory markers indicates target engagement - the senescent astrocytes in the brain were actively dying and bursting open, releasing their internal contents 43.
However, the trial was explicitly designed for safety, not efficacy. As expected in a 12-week study involving advanced neurodegeneration, the patients exhibited no statistically significant improvements in cognitive testing or structural neuroimaging 405253. While the trial paves the way for larger placebo-controlled studies, it underscores that clearing out cellular debris may not immediately repair complex neurological damage.
Diabetic Macular Edema and Vision Restoration
One of the most encouraging clinical readouts to date comes from targeted, localized senotherapy. In 2024, Unity Biotechnology reported phase I and IIa trial results for UBX1325, a potent BCL-xL inhibitor designed to treat diabetic macular edema by clearing senescent blood vessels in the retina 213644.
Rather than risking systemic toxicity by administering the BCL-xL inhibitor orally, the drug was injected directly into the eye. A single injection led to significant clinical improvements: 62.5% of treated patients gained at least five letters on a vision chart, and 50% gained ten or more letters, effectively halting and partially reversing the progression of vision loss without dose-limiting toxicity 3644.
The Epigenetic Clock Twist
A fascinating 2024 longitudinal study highlighted a complex biological nuance regarding systemic senolytic administration. Researchers sought to determine if clearing senescent cells would rewind a patient's biological age, as measured by DNA methylation "epigenetic clocks" 4546.
Nineteen healthy participants underwent a six-month intermittent regimen of D+Q. Surprisingly, the D+Q treatment resulted in statistically significant increases in epigenetic age acceleration and a notable decrease in telomere length 394546. Researchers theorize that while D+Q efficiently clears out toxic cells, the body must subsequently engage in rapid cellular division to replace the dead tissue. This sudden wave of cellular replication may temporarily shorten telomeres and stress the body's epigenetic markers 4546.
However, the study provided a crucial secondary finding. When researchers initiated a subsequent trial adding Fisetin to the D+Q regimen (creating a D+Q+F cocktail), the epigenetic age acceleration was heavily mitigated, resulting in statistically non-significant changes 394546. Because fisetin possesses both senolytic and broad senomorphic (inflammation-modulating) properties, it appears to cushion the biological stress of cell clearance, underscoring the potential necessity of combination therapies that address both cell death and tissue recovery 294546.
Senomorphics: Silencing Without Killing
While the demolition approach of senolytics is highly appealing, the potential for off-target toxicity and tissue regeneration imbalances has led many researchers to pursue a parallel strategy: senomorphics 183127.
Rather than inducing apoptosis, senomorphic agents are designed to modulate the genetic and metabolic pathways within the senescent cell, effectively silencing the destructive SASP without actually killing the cell 131831. Because they do not force the body to continuously clear and replace dead tissue, senomorphics may offer a safer route for chronic, long-term administration in older, frail adults 1827.
Rapamycin and Repurposed Therapeutics
Many of the most promising senomorphics are drugs already approved for other conditions. Rapamycin, a potent immunosuppressant used in organ transplants, is the gold standard gerostatic compound 2228. It works by inhibiting the mTOR signaling pathway, which is a master regulator of cell growth and metabolism 2228. By dampening mTOR, rapamycin effectively slows the rate at which healthy cells convert into senescent cells and suppresses the secretion of inflammatory cytokines from cells that are already senescent 222831. While rapamycin drastically extends lifespan in mice, it must be administered carefully in humans to avoid broad immune suppression 222627.
Other common pharmaceuticals are exhibiting surprising senomorphic capabilities. JAK inhibitors, such as ruxolitinib, have shown profound efficacy in suppressing the inflammatory components of the SASP in mouse models of frailty, offering a way to calm systemic inflammation while preserving the beneficial, early-stage functions of senescence 182831. In a recent randomized controlled trial involving type 2 diabetics, the administration of lipophilic statins (rosuvastatin combined with ezetimibe) successfully reduced the burden of senescent immune cells and lowered systemic inflammation, independent of their cholesterol-lowering effects 36.
Global Frontiers in Senotherapy
The pursuit of human longevity is rapidly accelerating, shifting from basic molecular screening toward highly advanced biotechnology and shifting geographically toward heavily funded initiatives in Asia 443747.
The Senolytic Vaccine Breakthrough in Japan
While small molecule drugs dominate current clinical trials, the future of senolytics may lie in precision immunotherapy. In a landmark 2021 study, researchers at Juntendo University in Japan sought to identify specific protein markers that exist on the surface of senescent cells but not on healthy cells 4849. Using transcriptome analysis, they discovered that a protein called GPNMB is highly expressed on the surface of senescent vascular cells 49.
Armed with this biological target, the team engineered a peptide vaccine designed to train the mouse's own immune system to hunt and destroy any cell displaying the GPNMB antigen 49. The results were staggering: the senolytic vaccine successfully eliminated GPNMB-expressing cells, significantly improved metabolic function and arterial stiffness in mice fed high-fat diets, and measurably extended the lifespan of progeroid mice suffering from accelerated aging 49. This research provides a proof-of-concept that we may eventually be able to inoculate patients against the cellular drivers of aging using individualized seno-antigen therapies.
Systemic Spread and Tissue Lineage Discoveries
Recent breakthroughs out of South Korea and China are fundamentally altering our understanding of how aging cascades through the body.
In 2025, a research team at Korea University discovered how cellular aging spreads systemically through the bloodstream. They identified a specific, redox-sensitive SASP factor called ReHMGB1 that is secreted by senescent cells, travels through the circulatory system, and robustly induces senescence in remote, previously healthy tissues 50. When researchers administered anti-HMGB1 antibodies to middle-aged mice suffering from muscle injury, the treatment halted this systemic spread, allowing the muscle to regenerate and significantly improving the animals' physical performance 50.
Simultaneously, researchers in China - which has recently eclipsed Europe in the volume of initiated clinical trials - developed a highly advanced genetic tracking system known as Sn-cTracer 475152. This system allowed researchers to selectively track and eliminate senescent cells based on their specific cellular lineage. The study revealed a critical nuance: while removing most senescent cells is beneficial, selectively destroying senescent endothelial cells in the liver actually triggered an accumulation of fibroblasts and dramatically worsened liver fibrosis 51. This highlights the absolute necessity of precision medicine in longevity therapeutics; the blind, systemic removal of all senescent cells could trigger unintended catastrophic damage in certain organs 203151.
Bottom line
The scientific community is pivoting definitively away from the antioxidant paradigm, as decades of clinical data confirm that daily antioxidant supplements fail to extend human lifespan and can actively disrupt the body's natural cellular repair mechanisms. In its place, the targeted demolition strategy of senolytics offers immense promise, fundamentally addressing chronic inflammation by forcing toxic, aged cells into apoptosis. However, while early human clinical trials involving compounds like Dasatinib, Quercetin, and Fisetin prove that we can successfully clear senescent cells from human tissue, these interventions remain highly experimental; their long-term impact on immune function, tissue regeneration, and epigenetic aging requires extensive validation before they can transition from targeted disease treatments into prophylactic anti-aging therapies.