Do Senolytics Work and What the 2026 Trials Show
Senolytics are an emerging class of drugs designed to selectively hunt and destroy damaged, non-dividing "zombie cells" that accumulate in the body and drive the biological aging process. As of 2026, clinical trials show that while a systemic "anti-aging" pill is not yet a proven reality, senolytics demonstrate significant, measurable success in treating localized age-related conditions, accelerating wound healing, and addressing therapy-induced frailty. The underlying science is robust, but the transition from mouse rejuvenation to human longevity requires precise biomarker targeting, highly regulated dosing, and a healthy dose of caution regarding unregulated commercial supplements.
What exactly are "zombie cells"?
To understand the promise and the limitations of senolytics, one must first understand the biological problem they are attempting to solve: cellular senescence.
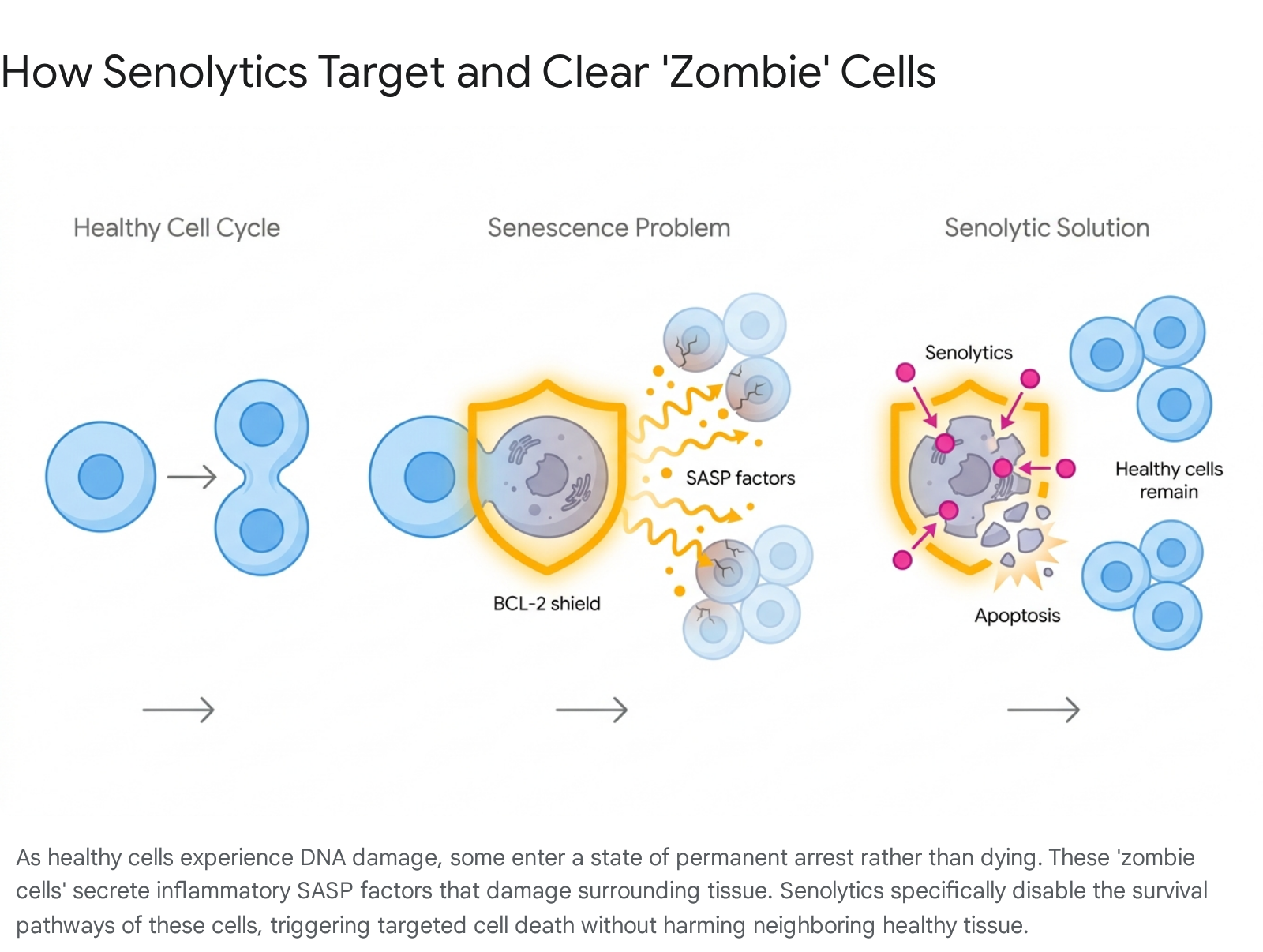
Every cell in the human body has a functional expiration date. When healthy cells experience severe physiological stress, accumulate significant DNA damage, or simply reach the end of their natural division cycle - a biological boundary known as the Hayflick limit, governed by the gradual shortening of their telomeres - they are supposed to safely self-destruct 121. This natural process of programmed cellular death is called apoptosis 12.
However, as the human body ages, a fraction of these severely damaged cells stubbornly refuse to die. They enter a state of permanent developmental arrest known as cellular senescence 153.
In popular science, these persistent, dysfunctional entities are commonly referred to as "zombie cells." While they permanently stop dividing, they do not sit quietly. They remain metabolically active and begin secreting a toxic, highly inflammatory cocktail of cytokines, chemokines, matrix metalloproteinases, and growth factors 125. Cellular biologists refer to this biological exhaust as the senescence-associated secretory phenotype, or SASP 278.
The dual nature of the SASP
It is a common misconception that cellular senescence is an entirely biological error. Initially, this senescence mechanism evolved as a vital, life-saving safeguard against cancer. By forcing severely mutated or precancerous cells to permanently stop replicating, the body prevents the formation of deadly tumors 29.
Furthermore, the SASP is actively useful in young, healthy bodies. When a young person suffers an acute tissue injury, such as a severe cut, a temporary burst of senescent cells at the wound site releases SASP factors. These inflammatory signals act as a biological flare gun, calling the immune system to the area to clear the damaged cells and initiate the early stages of tissue repair and collagen production 4.
The problem arises when senescence transitions from an acute, temporary response to a chronic condition. As the immune system gradually weakens with age - a phenomenon known as immunosenescence - it loses its ability to efficiently hunt down and clear out these zombie cells. Consequently, senescent cells begin to accumulate in tissues across the body. In aged human skin, for example, senescent cells can eventually make up roughly 15% of the outer and middle layers 5.
The chronic, low-grade inflammation generated by their relentless SASP begins to degrade surrounding healthy tissue. This intercellular miscommunication disrupts organ function and is now recognized as a primary driver of many hallmarks of aging, including joint stiffness, vascular stiffening, reduced immune function, cognitive decline, metabolic dysfunction, and an increased risk of late-life cancers 1256.
How do senolytics work?
Senolytics are pharmacological compounds specifically engineered to exploit the unique, hidden vulnerabilities of senescent cells.
To survive the highly toxic, inflammatory microenvironment they create for themselves, zombie cells must continuously upregulate a network of anti-apoptotic pathways. Essentially, they build internal chemical shields - often relying on the BCL-2, BCL-xL, and BCL-W protein families, or the FOXO4-p53 axis - that protect them from their own toxic exhaust and allow them to evade normal programmed cell death 78910.
Senolytic drugs are designed to temporarily disable these specific survival pathways 710. When the chemical shield drops, the senescent cells are finally forced to undergo the apoptosis they have been evading for years. Because surrounding, healthy, youthful cells do not rely on these specific stress-survival pathways to stay alive, they are largely left unharmed by the senolytic intervention 1011.
The clinical rationale for "hit-and-run" dosing
One of the most critical and widely misunderstood aspects of senolytic therapy is that it does not require a daily pill. Because senescent cells take weeks, months, or even years to accumulate to dangerous levels, senolytics are administered using a highly intermittent "hit-and-run" dosing strategy 1779.
In a typical clinical protocol, a patient might take a high, highly concentrated dose of a senolytic for just two to three consecutive days. This achieves peak tissue concentrations sufficient to trigger mass apoptosis in the zombie cell population 17. The drug is then stopped entirely. The healthy cells recover from the brief chemical exposure, the zombie cells undergo apoptosis and are subsequently cleared by scavenging immune cells, and the patient may not require another dose for an entire month, or sometimes even a quarter 11912.
This intermittent scheduling is not merely a convenience; it is biologically vital. Continuous, daily exposure to these powerful biological agents can lead to severe, cumulative toxicity and unintended off-target effects 2712.
The 2026 clinical trial landscape: Do they actually work?
By early 2026, longevity medicine transitioned definitively from the realm of academic speculation and Silicon Valley biohacking to rigorous, heavily funded global clinical trials 102122. The U.S. Food and Drug Administration (FDA) and other global regulatory bodies have even begun shifting their frameworks, exploring "geroscience" and formally recognizing "aging itself" as an intervenable medical indicator, rather than requiring drug companies to target only specific, downstream terminal diseases 1021.
This regulatory and scientific maturation has unlocked massive capital. The global senolytic therapeutics market, fueled by an influx of venture capital and expanding pipelines from major pharmaceutical giants like Novo Nordisk and Eli Lilly, reached a valuation of $31.63 billion in 2025 and is projected to surpass $68 billion by 2034 1023. Globally, there are now more than 85 active clinical trials evaluating senolytic or related senomorphic agents 10.
However, the clinical picture is deeply nuanced and far more complex than initial preclinical mouse studies suggested. The science looks incredibly strong when senolytics are treated as highly targeted therapies for specific, localized diseases with a clear, measurable burden of senescent cells. The evidence looks much weaker when these drugs are aggressively pitched as sweeping, whole-body "anti-aging" panaceas 8.
Comparing the leading senolytic compounds
Several distinct classes of senolytics are currently making their way through human trials. They range from repurposed cancer drugs and naturally occurring flavonoids to entirely novel synthetic molecules. Here is a breakdown of the most clinically advanced therapies evaluated as of 2026.
| Compound / Drug | Mechanism of Action | Clinical Status (2026) | Primary Findings & Limitations |
|---|---|---|---|
| Dasatinib + Quercetin (D+Q) | Tyrosine kinase inhibitor + flavonoid; broadly targets multiple survival pathways. | Phase 2 (Multiple systemic indications) | The most extensively studied combination. Showed improved physical function in pulmonary fibrosis 13 and reduced senescent burden in kidney disease 25. Limited by gastrointestinal side effects and potential off-target toxicity 7. |
| Fisetin | High-potency natural flavonoid extract. | Phase 2 (TROFFi, SENECA trials) | Demonstrated the highest senolytic potency among tested flavonoids in mice 114. Currently tested for post-chemotherapy frailty 15 and general aging 21. Enjoys a safer profile, but broad systemic efficacy in humans remains uncertain 6. |
| Navitoclax (ABT-263) | Synthetic BCL-2 / BCL-xL dual inhibitor. | Phase 2 (Oncology / Localized Wound Healing) | Highly effective at clearing senescent cells in vitro, but systemic oral use is severely limited by dose-limiting thrombocytopenia (platelet depletion) 789. Showing massive clinical promise in topical, localized delivery 24. |
| Foselutoclax (UBX1325) | Synthetic, highly targeted BCL-xL inhibitor. | Phase 2b completed | Delivered locally via direct eye injection for diabetic macular edema. Demonstrated non-inferiority to standard-of-care treatments, though commercial and strategic progress has stalled 102116. |
| RS5614 | Novel PAI-1 inhibitor. | XPRIZE Semi-finalist / Phase 3 (Oncology) | A novel oral senolytic from Japan. Early 2026 XPRIZE data showed an epigenetic clock reversal of 1.9 to 3.4 years and immune function improvements in older adults over four months 29. |
| SGLT2 Inhibitors (e.g., Dapagliflozin) | Immune-mediated clearance. | Phase 2 | A newly identified mechanism (2024-2025). Does not directly kill cells, but strips their PD-L1 "don't eat me" signals, allowing the body's natural immune system to clear them 1214. |
The shift from systemic anti-aging to localized repair
One of the defining lessons of senolytic research over the past few years is that systemic human biology is vastly more complex than that of laboratory mice. A drug that successfully rejuvenates an inbred, genetically identical mouse in a sterile cage often struggles to show the same sweeping benefits in genetically diverse humans with decades of accumulated environmental damage.
As a result, some of the most successful clinical trials have abandoned the idea of a systemic "anti-aging pill" that treats the whole body at once, focusing instead on delivering drugs directly to the localized site of specific age-related diseases 84.
Breakthroughs in skin rejuvenation and wound healing
Perhaps the most universally hailed and clinically tangible senolytic breakthrough of early 2026 involves the treatment of chronic wounds. As human skin ages, the buildup of zombie cells weakens its structural integrity and drastically slows its ability to repair itself after surgery, trauma, or injury 45. Older patients face exceptionally high risks of chronic, non-healing wounds and dangerous post-surgical infections 23.
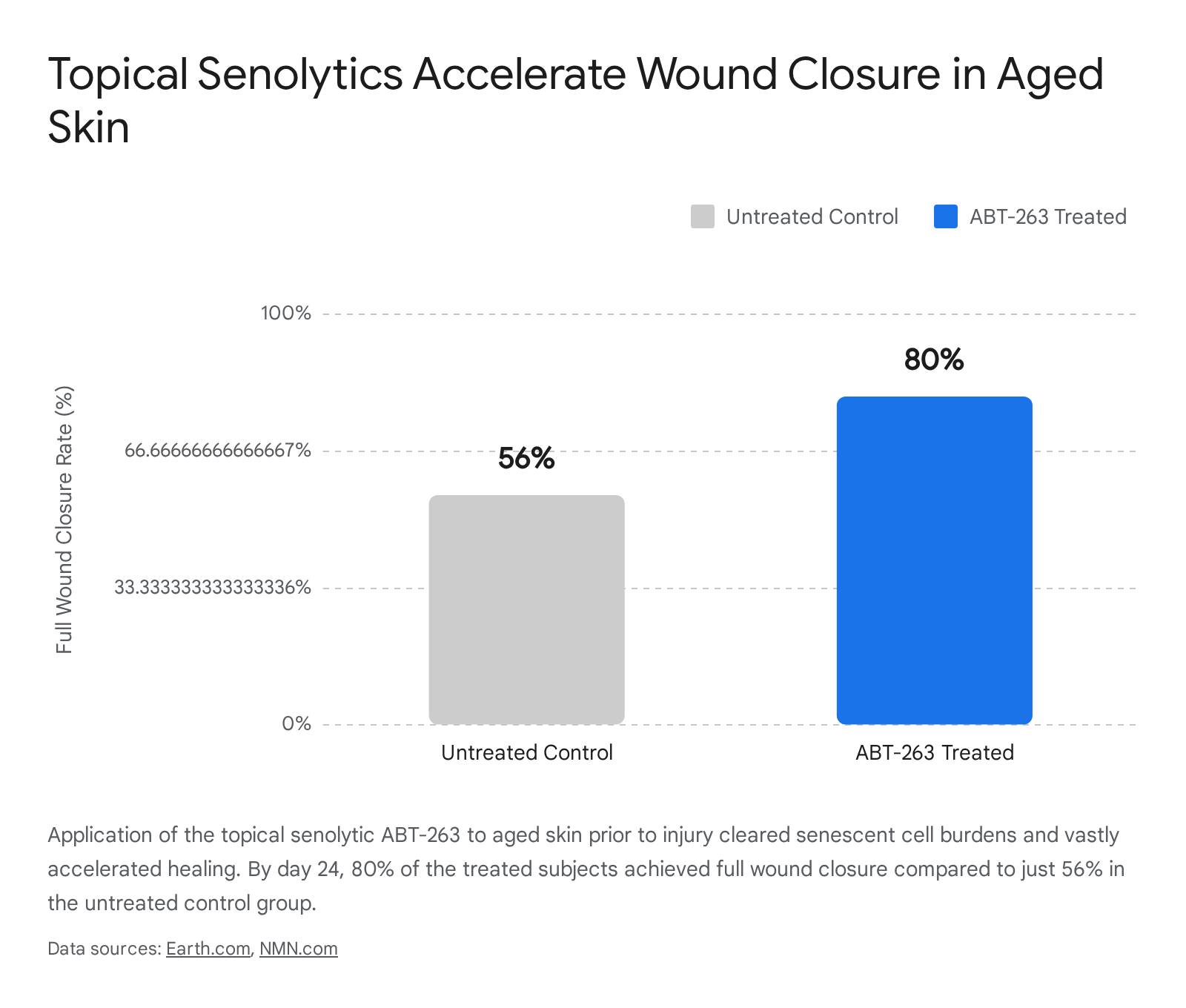
Researchers recognized that systemic BCL-xL inhibitors like Navitoclax (ABT-263) were too toxic for oral use, but hypothesized they might work if applied locally. They tested whether applying Navitoclax topically - as an ointment directly on the skin - could clear these cells without triggering the dangerous platelet-depleting side effects that occur when the drug circulates through the bloodstream 45.
The results were striking. In a landmark study published in Aging, researchers applied the senolytic to aged skin prior to any injury. This localized preventative treatment successfully cleared out the senescent cell burden and effectively switched on genes tied to collagen production, extracellular matrix remodeling, and new blood vessel formation 345.
When the skin was subsequently wounded, it healed at a dramatically accelerated pace, behaving much like youthful tissue. By day 24, a remarkable 80% of the senolytic-treated group had achieved full wound closure, compared to only 56% of the untreated control group 25.
This localized approach successfully bypassed the systemic toxicity of BCL-xL inhibitors and has prompted the rapid development of specialized wound dressings. It demonstrates that prophylactically "priming" aged tissue prior to elective surgery could soon become a standard clinical practice in geriatric medicine 34. Similarly, biotech firms like Rubedo Life Sciences have advanced topical senolytics (RLS-1496) into Phase 1 human trials in Europe for chronic inflammatory skin conditions like psoriasis and actinic keratosis 816.
Treating localized vision loss
Another major validation for localized delivery comes from the field of ophthalmology. Diabetic macular edema is a severe, vision-threatening condition where damaged, senescent blood vessels leak fluid directly into the retina.
Unity Biotechnology developed foselutoclax (UBX1325), a potent BCL-xL inhibitor senolytic designed to be injected directly into the eye, confining the drug's activity to the diseased tissue. In a robust Phase 2b trial (the ASPIRE and BEHOLD studies), this localized delivery achieved its primary endpoint, successfully improving visual acuity and demonstrating non-inferiority to aflibercept, the current standard-of-care anti-VEGF treatment 8102116.
While corporate maneuvering and strategic shifts have currently stalled the drug's wider commercial advancement, the biological proof-of-concept remains an anchor for the senolytic field: when you clear senescent cells from a specific, degraded tissue, functional recovery is possible 8.
Mixed results in systemic clinical trials
When researchers move away from targeted, local delivery and attempt to treat broad, systemic aging conditions with oral senolytics, the clinical trial results become much more complicated and yield deeply mixed results.
Bone health and the complexity of osteoporosis
Osteoporosis is driven heavily by the accumulation of senescent cells within the bone microenvironment. Healthy bone requires a delicate balance of continuous remodeling: osteoclasts break down old bone tissue, while osteoblasts build new bone. However, zombie cells in the bone marrow secrete inflammatory SASP factors that hyper-activate the bone-destroying osteoclasts while simultaneously suppressing the bone-building osteoblasts, leading to rapid, age-related bone density loss 17.
In a highly anticipated Phase 2 randomized controlled trial, researchers from the Mayo Clinic attempted to treat postmenopausal osteoporosis using the Dasatinib plus Quercetin (D+Q) hit-and-run oral protocol 19. The top-line, overall results were a disappointment: the treatment did not significantly reduce markers of bone resorption across the entire study group of postmenopausal women 819.
However, a deeper, exploratory analysis of the data revealed a crucial insight that is reshaping the future of senolytic medicine. The senolytic therapy did work - successfully increasing bone mineral density at the radius and boosting bone formation markers - but only in a specific subset of women who possessed a remarkably high baseline burden of senescent cells, identified by elevated levels of a specific T-cell biomarker called p16_variant 5 1918.
This finding proved a critical, sobering point: senolytics cannot reverse aging damage if there aren't enough zombie cells currently present to justify the pharmacological intervention 1919. A patient might be aging, but if their osteoporosis is driven by hormones rather than a high senescence burden, the drug will fail. To follow up on these mechanisms, the ongoing SENIOR trial in Europe (Denmark) is currently testing the D+Q senolytic combination against NAD+ boosting antioxidant therapies (Nicotinamide Riboside) to precisely measure changes in bone resorption and formation over a 21-week period 3320.
Cognitive decline and Alzheimer's disease
Can clearing zombie cells protect the aging brain? Cellular senescence is heavily implicated in chronic neuroinflammation, which is a core driver of Alzheimer's disease and other forms of dementia 78.
A closely watched 2025 pilot study conducted jointly by Harvard Medical School, the Mayo Clinic, and Cedars-Sinai investigated the D+Q senolytic combination in older adults experiencing mild cognitive impairment and abnormally slow gait speed - two common early clinical indicators of Alzheimer's risk 1021. The trial successfully proved two vital concepts: the drugs could successfully penetrate the central nervous system (crossing the blood-brain barrier), and the intermittent dosing regimen was entirely safe and tolerable in this vulnerable geriatric population, with no serious adverse events reported 2122.
While the pilot study was intentionally too small to definitively prove that senolytics can halt or reverse dementia, researchers found a highly promising biological correlation. Patients who experienced significant reductions in tumor necrosis factor-alpha (TNF-α) - a prominent, inflammatory SASP molecule secreted by senescent cells - also showed corresponding improvements in their Montreal Cognitive Assessment (MoCA) screening scores 1021.
Reversing post-chemotherapy frailty in cancer survivors
Chemotherapy remains one of the most effective tools for killing rapid-dividing cancer cells. However, the intense, indiscriminate cellular stress that chemotherapy inflicts on the body forces many surviving, healthy cells into premature senescence. This sudden, massive accumulation of therapy-induced zombie cells is a primary reason why up to a third of breast cancer survivors experience severe, persistent frailty, fatigue, and sharp physical decline that fails to resolve long after their cancer is successfully cured 15372324.
To combat this accelerated aging phenotype, oncologists have launched the TROFFi trial (Targeting Senescence to Improve Physical Function in Breast Cancer Survivors). This multicenter, randomized, double-blind Phase 2 trial is evaluating whether high-dose, pulsed supplementation with Fisetin can clear these chemotherapy-induced senescent cells in postmenopausal women 1525.
Researchers are meticulously tracking whether the senolytic can significantly improve patients' physical endurance, primarily measured by their 6-minute walk distance (6MWD), as well as their overall grip strength and self-reported fatigue levels 232627.
Simultaneously, the SENECA trial is utilizing the same Fisetin hit-and-run protocol to treat general, age-related frailty in 500 adults over the age of 70, measuring comprehensive frailty indices 21. Fisetin is currently highly favored in these extensive human trials because it boasts a much cleaner, more tolerable safety profile than synthetic BCL inhibitors, although its overall potency and bioavailability in human tissue compared to mice is still a subject of scientific debate 7643.
New frontiers in senolytic mechanisms
As the field of longevity medicine matures, researchers are discovering entirely new, elegant ways to clear senescent cells without relying exclusively on the traditional, blunt-force BCL-shield-breaking mechanisms.
SGLT2 inhibitors and immune-mediated clearance
In late 2024 and 2025, scientists uncovered that SGLT2 inhibitors - a class of drugs like dapagliflozin, originally developed and widely prescribed for managing type 2 diabetes - possess unexpected, immune-mediated senolytic properties 1214.
Unlike D+Q or Navitoclax, SGLT2 inhibitors do not directly poison or kill the zombie cells. Instead, they act on the cell's surface. Senescent cells evade the immune system by expressing a specific surface protein called PD-L1, which acts as a "don't eat me" signal to passing immune cells. SGLT2 inhibitors effectively strip away this PD-L1 signal. Once the camouflage is removed, the body's own cytotoxic T-cells can finally recognize the senescent cells as aberrant and naturally clear them from the tissue 1214. This represents a fundamentally different, and potentially safer, approach to continuous senolytic therapy.
Epigenetic reversal and the XPRIZE Healthspan
In Japan, an experimental oral drug called RS5614 (a PAI-1 inhibitor developed by Renascience) has produced striking, unprecedented results as a semi-finalist in the global XPRIZE Healthspan competition 29.
In early 2026, researchers released clinical trial data revealing that just four months of administering the drug to older adults actively reduced their biological age. This was not measured by functional tests, but by highly sensitive DNA methylation "epigenetic clocks" (the Horvath and PC-Horvath methods), which indicated a systemic age reversal of 1.9 to 3.4 years 29. Beyond epigenetic changes, the drug triggered a functional recovery and rejuvenation of hematopoietic stem cells and immune cells, and significantly reduced markers of systemic oxidative stress 29.
Stem cell integration and global anti-aging initiatives
The urgency of the aging crisis is also driving massive national trials. In China, which is grappling with rapid demographic aging, the renowned 301 Hospital in Beijing launched the country's first large-scale clinical study evaluating stem cells as a direct anti-aging intervention 28. The trial plans to enroll 2,000 adults over the age of 50 to test amimestrocel (Ruibosheng), a mesenchymal stem cell therapy derived from human umbilical cord tissue. Researchers are investigating whether infusing the body with fresh stem cells can help regulate inflammation, support tissue repair, and replace the functional capacity lost to cellular senescence 28.
Senolytics vs. Senomorphics: Understanding the difference
As you navigate the longevity space and review clinical trial data, you will frequently encounter the term "senomorphics." While they sound similar to senolytics and are often grouped together as "senotherapeutics," their biological mechanisms of action and clinical applications are fundamentally different 27.
The easiest way to understand the difference is to categorize them as assassins versus suppressors.
- Senolytics are the assassins. They selectively trigger apoptosis, physically killing the zombie cell and removing it from the tissue entirely 12. Because the source of the inflammation is permanently eradicated, the treatment only needs to be applied intermittently (the hit-and-run approach) 717.
- Senomorphics are the suppressors. They do not kill the senescent cell. Instead, they modulate the cell's internal behavior, successfully suppressing its ability to secrete the toxic, inflammatory SASP factors 1217.
| Therapeutic Paradigm | Primary Mechanism | Dosing Strategy | Clinical Examples (2026) |
|---|---|---|---|
| Senolytics | Directly induces apoptosis (cell death) in senescent cells by disrupting anti-apoptotic survival pathways (SCAPs). | Intermittent / "Hit-and-Run" (e.g., 3 days per month) to prevent cumulative toxicity. | Dasatinib + Quercetin (D+Q), Fisetin, Navitoclax, UBX1325. |
| Senomorphics | Modulates cellular signaling to suppress the secretion of inflammatory SASP factors, leaving the cell alive but silent. | Continuous / Chronic administration required to maintain suppression of the SASP. | Rapamycin (mTOR inhibitor), Metformin, Ruxolitinib (JAK inhibitor). |
Common senomorphics include some of the most famous longevity drugs currently under investigation, such as Metformin and Rapamycin 717. The Phase 3 TAME (Targeting Aging with Metformin) trial, enrolling 3,000 adults, is testing whether continuous Metformin use can delay a composite endpoint of death, dementia, and cancer 21. Similarly, the TRIIM-X trial demonstrated that low-dose Rapamycin significantly improved immune aging markers over 12 months 21.
Because senomorphics leave the zombie cells alive and in place within the tissue, the patient must take the drugs continuously to keep the toxic secretions suppressed. If the drug is stopped, the cell will resume pumping out inflammation 217. Currently, longevity researchers are exploring sophisticated combination therapies: using an intermittent senolytic blast to clear out the vast majority of the accumulated zombie cells, followed by a continuous, low-dose senomorphic regimen to manage and silence the remaining biological noise 21029.
Are over-the-counter senolytic supplements safe?
Given the undeniable biological excitement surrounding this science, the commercial, unregulated dietary supplement market has predictably exploded. You can readily purchase purported senolytic compounds, particularly Quercetin and Fisetin, online, at health food stores, or at a local pharmacy 630.
However, longevity researchers, geriatricians, and clinical pharmacologists from leading institutions like the Mayo Clinic and Cedars-Sinai strongly advise against healthy individuals attempting to biohack their own aging process with these easily accessible compounds 71330.
There are several critical, scientifically grounded reasons for this extreme caution:
- The Danger of Continuous Daily Dosing: Commercial supplements are almost universally marketed and designed to be taken daily as general antioxidants. However, as established, true senolytic therapy requires a high-dose, "hit-and-run" approach 11914. Taking low, continuous daily doses of these flavonoids likely confers only mild antioxidant effects and fundamentally fails to achieve the high tissue concentrations required to trigger senescent cell death 1. Conversely, ignoring the bottle and taking massive doses continuously can lead to severe cumulative toxicity and liver stress 226.
- Lack of Regulation and Purity: Over-the-counter supplements are not strictly regulated by the FDA. Independent laboratory analyses repeatedly show that commercial formulations vary wildly in their actual purity, bioavailability (how well the body absorbs them), and the actual amount of active compound present in the capsule 30.
- Unknown Long-Term Risks: The total safety database for all senolytic drugs in published human trials through 2025 accounts for fewer than 200 patient-years of exposure data 7. This is completely insufficient to detect rare but serious adverse events. We simply do not yet know the long-term biological consequences of repeatedly clearing senescent cells - which do play a role in tissue homeostasis - across a human lifespan 27.
- Off-Target Toxicity: Senescent survival pathways are not entirely unique to zombie cells. For example, Navitoclax targets BCL-xL, a protein that healthy blood platelets also require to survive. Using it improperly or systemically causes rapid, dangerous drops in platelet counts, increasing the risk of severe bleeding 58929.
As Dr. James Kirkland, a pioneer in senolytic research at the Mayo Clinic, explicitly warns: consumers should avoid experimenting with these drugs "until and unless we have really rigorous, reproducible scientific data that pharmaceutical regulators and the medical community accept" 1330. Clinicians note that any off-label prescription of clinical-grade senolytics must be accompanied by thorough medical oversight, including baseline complete blood counts (CBC), comprehensive metabolic panels, and lipid checks to monitor organ function 7.
The biomarker bottleneck: How do we measure aging?
The single greatest hurdle facing senolytic research and its translation to mainstream medicine in 2026 isn't the discovery of new drugs - it is the difficulty of objectively measuring whether those drugs are actually working.
Aging is not a single, easily defined disease; it is a gradual, highly variable, systemic decline. To definitively prove to regulatory agencies that a senolytic drug has reversed aging, scientists must rely on biomarkers. Historically, the field relied on macroscopic functional metrics (like grip strength or 6-minute walk tests) or counting the raw abundance of specific senescence markers like p16INK4a in tissue biopsies 2127.
However, as the osteoporosis trials demonstrated, senescent cells are incredibly heterogeneous 99. A senolytic drug might be highly effective at clearing a specific type of zombie fibroblast cell in the lungs, but be completely useless against a different type of senescent osteocyte in the bone or cartilage of a knee 8929.
To solve this translational bottleneck, a 2025 consensus among major longevity research institutions established a rigorous, composite framework for assessing biological age in clinical trials 21. This new gold standard combines: * First-generation clocks: DNA methylation tests (such as the Horvath clock and GrimAge) which track deep epigenetic changes over a cycle of 6 to 12 months 21. * Second-generation clocks: Advanced multi-omic panels tracking proteomic, metabolomic, and immune age, which are highly sensitive to intervention and can show measurable physiological changes in just 3 to 6 months 21. * Refined p16 and SASP Panels: Advanced tracking of specific genetic variants (such as the p16_variant 5 assay) and circulating SASP inflammation factors in the blood. This allows researchers to identify the specific patients who currently harbor enough zombie cells to actually benefit from treatment, preventing drugs from failing in clinical trials simply because they were given to the wrong patients 718.
This biomarker revolution is rapidly pushing longevity medicine away from the simplistic idea of a universal "anti-aging pill" and toward highly precise, personalized therapy 919. In the near future, a clinician will likely test your specific senescent cell burden, identify exactly which organ systems are failing due to SASP inflammation, and prescribe a localized senolytic perfectly matched to your unique biological profile 19.
Bottom line
Senolytics have conclusively proven their biological premise: they can successfully clear toxic, age-driving "zombie cells" and alter the fundamental biology of aging at a cellular level. As of 2026, the most compelling, undeniable human evidence exists in highly targeted, localized treatments, such as topical ointments that dramatically accelerate wound healing in the elderly, or specific clinical protocols aiming to reverse chemotherapy-induced frailty. However, the concept of a systemic, over-the-counter anti-aging pill remains unsupported by current clinical data, and patients should strictly avoid experimenting with unregulated supplements until long-term safety profiles and precision biomarker testing are fully established in the clinic.