Creatine Supplementation for Brain Health and Cognitive Function
Creatine monohydrate is one of the most rigorously studied and widely consumed ergogenic supplements in human history. Historically, its application has been relegated primarily to the domains of sports medicine, exercise physiology, and skeletal muscle hypertrophy 12. However, a significant paradigm shift has emerged in recent years, repositioning creatine as a critical modulator of brain bioenergetics, neurological health, and cognitive performance 23.
The human brain is a disproportionately energy-demanding organ. While it accounts for approximately 2% of total body mass, it consumes roughly 20% of the body's total resting energy 4567. The relentless metabolic demands necessary for maintaining ion gradients, facilitating neurotransmitter exocytosis, and enabling synaptic plasticity require a rapid, continuous supply of adenosine triphosphate (ATP) 368. Creatine acts as a vital spatial and temporal energy buffer within this highly oxidative system. Despite the strong mechanistic rationale for cognitive enhancement, translating exogenous creatine supplementation into clinical and cognitive outcomes is complicated by the unique pharmacokinetics of the central nervous system, blood-brain barrier transport limitations, and varying baseline dietary statuses.
This report systematically examines the exhaustive evidence regarding creatine supplementation beyond skeletal muscle. It details its mechanisms of neural uptake, its efficacy across distinct cognitive domains and physiological stress states, its potential neuroprotective role in aging and neurodegenerative disease, and the safety parameters governing high-dose clinical protocols.
Cellular Bioenergetics and Brain Metabolism
To objectively evaluate the cognitive and neurological effects of creatine, it is necessary to examine the metabolic architecture of the brain and the specific cellular machinery responsible for creatine synthesis, transport, and utilization.
The ATP-Phosphocreatine System in Neural Tissue
Creatine (methylguanidine acetic acid) is a nitrogenous organic compound endogenously synthesized primarily in the liver and kidneys from the amino acids arginine, glycine, and methionine 6978. Inside the cell, roughly one-third of creatine exists in a free, unphosphorylated state, while the remaining two-thirds are phosphorylated to form phosphorylcreatine (PCr) 67. Through a reversible reaction catalyzed by the enzyme creatine kinase (CK) - specifically the brain-specific isoform BB-CK in neural tissue - PCr donates its high-energy phosphate group to adenosine diphosphate (ADP) to rapidly resynthesize ATP 369.
This ATP-PCr system operates as an essential spatial and temporal energy buffer. It bridges the critical metabolic gap during brief, intense periods of cellular energy demand before mitochondrial oxidative phosphorylation and glycolysis can adequately upregulate to meet the cellular requirements 7910. In the central nervous system, these spikes in energy demand occur continuously during complex cognitive tasks, periods of sleep deprivation, or following acute neurotrauma 6911. When neurons fire rapidly, localized ATP stores are rapidly depleted, forcing the brain to rely heavily on the intracellular PCr pool to maintain neurotransmitter exocytosis, stabilize cellular membranes, and sustain critical ionic gradients 6911.
Blood-Brain Barrier Permeability and the SLC6A8 Transporter
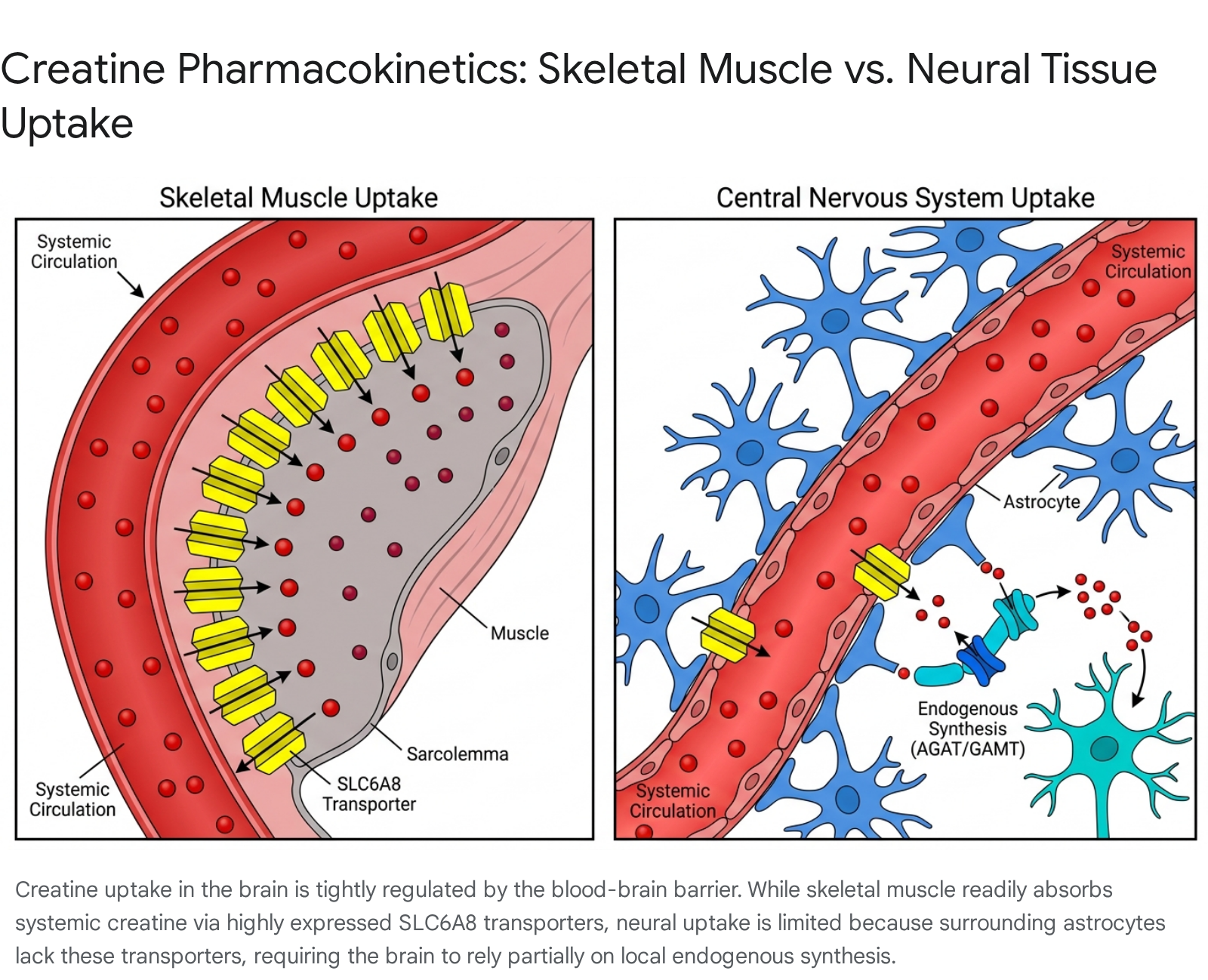
The pharmacokinetics of creatine in the central nervous system differ drastically from those observed in skeletal muscle. Skeletal muscle lacks the enzymatic capacity to synthesize its own creatine; therefore, while it stores approximately 95% of the body's total creatine pool, it relies entirely on exogenous dietary intake or hepatic synthesis 56912. Systemic creatine enters the skeletal muscle via a highly efficient, sodium- and chloride-dependent cotransporter known as SLC6A8 (or CRT1) 67912.
Conversely, the brain exhibits a high degree of biochemical autonomy regarding creatine metabolism. Neural tissue is capable of synthesizing its own creatine locally, utilizing the enzymes L-arginine:glycine amidinotransferase (AGAT) and guanidinoacetate N-methyltransferase (GAMT), which are expressed in neurons, oligodendrocytes, and astrocytes 212131415. While the brain does import systemic creatine across the blood-brain barrier (BBB), this transport process is remarkably inefficient compared to muscular uptake 61215.
The SLC6A8 transporter - a 635-amino acid, ~70.5 kDa protein operating with a 2 Na+: 1 Cl-: 1 creatine stoichiometry - is expressed on the microcapillary endothelial cells of the BBB, allowing initial passage from the systemic bloodstream 912. Kinetic analyses of SLC6A8 reveal a maximum transport rate (Vmax) of approximately 838.8 pmol/h/oocyte and a Michaelis constant (Km) of 567.4 μM, with its activity upregulated by serum and glucocorticoid inducible kinases such as SGK1 and SGK3 1620. However, while the transporter is present on the endothelium, SLC6A8 is notably absent from the astrocyte end-feet that ensheath these cerebral capillaries 6121314. Because astrocytes mediate nutrient transfer between the cerebral vasculature and the deeper neuronal networks, the absence of astrocytic SLC6A8 creates a severe physiological bottleneck, drastically limiting the uptake of exogenous systemic creatine into the brain parenchyma 6131415.
Consequently, while standard dosing protocols (e.g., 5g per day) can saturate skeletal muscle stores by roughly 20% over 30 days, similar systemic doses yield marginal, often statistically insignificant, increases in neural total creatine content (typically less than a 6% increase) 271117. Studies utilizing magnetic resonance spectroscopy (MRS) indicate that aggressive dosing regimens - often 10 to 20g per day for prolonged periods spanning several weeks - are necessary to overcome this BBB resistance and reliably elevate regional brain creatine concentrations by 8% to 11% 26111718. Animal models utilizing GAMT-deficient (GAMT-/-) mice further confirm these disparate tissue kinetics, demonstrating that upon initiation of creatine supplementation, skeletal muscle saturation occurs rapidly in a biphasic manner, whereas cerebral uptake is a significantly slower, protracted process 19.
Creatine Transporter Deficiency (CTD)
The indispensable nature of the SLC6A8 transporter for normal neural development is starkly illustrated by Creatine Transporter Deficiency (CTD), an X-linked metabolic disorder 9121520. Caused by missense or nonsense mutations in the SLC6A8 gene, CTD results in profound cerebral creatine depletion 9152021. Clinically, this manifests as severe intellectual disability, delayed speech acquisition, autism-spectrum behaviors, motor dysfunction, and treatment-resistant epilepsy 9152021.
Because the pathophysiological defect lies fundamentally within the plasma membrane transport mechanism itself, rather than a failure of synthesis, male patients with CTD generally do not experience clinical improvement following standard oral creatine supplementation 1520. This clinical reality unequivocally underscores the absolute necessity of functional SLC6A8 transporters for the integration of exogenous systemic creatine into the neuronal bioenergetic pool 1520.
Efficacy of Creatine on Cognitive Domains
With the biological transport mechanisms established, contemporary clinical attention has pivoted toward whether augmenting these brain creatine reserves translates to measurable, statistically significant improvements in human cognitive performance.
Memory, Attention, and Processing Speed
Recent rigorous meta-analyses provide a highly nuanced view of creatine's pro-cognitive potential, dispelling the notion that it acts as a universal nootropic. A comprehensive 2024 systematic review and meta-analysis published in Frontiers in Nutrition evaluated 16 randomized controlled trials (RCTs) encompassing 492 participants aged between 20.8 and 76.4 years 4222324. The findings clearly indicate that creatine monohydrate supplementation is highly domain-specific in its cognitive effects.
The meta-analysis revealed statistically significant positive effects on memory function (Standardized Mean Difference [SMD] = 0.31, 95% CI: 0.18 - 0.44), attention time (SMD = -0.31, 95% CI: -0.58 to -0.03), and information processing speed (SMD = -0.51, 95% CI: -1.01 to -0.01) 222324. However, there were no significant improvements observed for overall global cognitive function or specific tests measuring complex executive function (e.g., higher-order planning, cognitive flexibility, task switching) 222324.
When applying the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework, researchers determined a "moderate" certainty of evidence for memory improvements, indicating a reasonable level of clinical confidence in this specific effect 4222324. In contrast, the evidence supporting enhancements in processing speed and attention remains of "low" certainty, constrained by high inter-study heterogeneity, varying cognitive testing modalities, and relatively small sample sizes across the available literature 222324.
| Cognitive Domain | Standardized Mean Difference (SMD) | 95% Confidence Interval | Statistical Significance | Certainty of Evidence (GRADE) |
|---|---|---|---|---|
| Memory Function | 0.31 | 0.18 to 0.44 | Significant Positive Effect (p < 0.00001) | Moderate |
| Attention Time | -0.31 | -0.58 to -0.03 | Significant Positive Effect | Low |
| Processing Speed Time | -0.51 | -1.01 to -0.01 | Significant Positive Effect (p = 0.04) | Low |
| Overall Cognitive Function | 0.34 | -0.20 to 0.88 | Not Significant (p = 0.22) | Low |
| Executive Function | N/A | N/A | Not Significant | Low |
Table 1: Aggregated data from a 2024 systematic review of 16 RCTs evaluating creatine monohydrate supplementation. Note: Negative SMDs for attention and processing speed denote a reduction in the time required to complete the tasks, which constitutes a functional improvement in performance 222324.
Subgroup analyses from this meta-analysis further indicated that specific populations are significantly more responsive to supplementation. Notably, females, younger to middle-aged adults (18-60 years), and individuals facing acute metabolic or physiological stress exhibited more pronounced cognitive benefits than unstressed, healthy male controls 42224.
Differential Effects in Vegetarians and Omnivores
Because dietary creatine is sourced almost exclusively from animal products (primarily red meat, poultry, and seafood), individuals adhering to vegetarian or vegan diets present with chronically lower baseline levels of systemic and intramuscular creatine 5292526.
The prevailing "ceiling effect" hypothesis posits that omnivores may not experience significant cognitive enhancement from supplementation because their cerebral and systemic creatine stores are already operating near maximum physiological saturation 72925. Early landmark studies appeared to support this theory. A double-blind trial involving 128 young adult females found that a 5-day loading protocol of 20g/day significantly improved memory performance exclusively in vegetarians; omnivores exhibited no such benefit, and in some task variables, actually demonstrated slightly poorer performance compared to baseline metrics 526. Similarly, a 2019 study measuring neurocognitive function via the standardized ImPACT test demonstrated that a vegetarian cohort scored significantly higher following four weeks of supplementation compared to a meat-eating control group whose scores remained stagnant 25.
However, the assumption that dietary creatine significantly alters brain creatine baseline levels remains fiercely debated in the literature. While muscle creatine is unarguably lower in vegetarians, MRS imaging studies suggest that baseline brain creatine content between healthy vegetarians and omnivores does not differ dramatically, likely due to the brain's robust capacity for autonomous endogenous synthesis 27.
This controversy was highlighted by a large 2023 crossover, double-blind trial involving 123 subjects (evenly split between vegetarians and omnivores) that sought to replicate earlier positive findings regarding abstract reasoning (Raven's Advanced Progressive Matrices) and working memory (Backward Digit Span) 27. The researchers found no statistically significant interaction between dietary style and the cognitive benefits of a 6-week, 5g/day creatine intervention (BDS: p = 0.064; RAPM: p = 0.327) . Bayesian analyses indicated only weak evidence for a highly modest global cognitive benefit, actively challenging the notion that vegetarians inherently experience dramatic neurological transformations from creatine supplementation compared to omnivores 27.
Cognitive Resilience Under Metabolic Stress
One of the most consistent and scientifically compelling findings in contemporary creatine research is that supplementation is profoundly more effective when the brain is operating under acute metabolic stress - such as sleep deprivation, mental fatigue, or hypoxia 24342829. Under normal basal conditions, the healthy brain easily maintains ATP homeostasis. However, when metabolically challenged, standard ATP regeneration pathways falter, and the exogenous PCr pool becomes critical to prevent systemic cognitive failure 28929.
Sleep Deprivation
Acute sleep deprivation induces severe metabolic alterations in the brain, including diminished synaptogenesis, altered glutamate signaling, reductions in available ATP, and localized intracellular acidification 28. A pivotal 2024 double-blind clinical trial by Gordji-Nejad et al. administered a single, acute high dose of creatine (0.35g/kg of body weight, equating to roughly 20-25g for an average adult) to subjects undergoing 21 hours of continuous supervised wakefulness 2837.
Utilizing combined 31P-MRS and 1H-MRS neuroimaging to track real-time brain chemistry, researchers observed that the high dose of creatine effectively reversed the metabolic deterioration normally caused by sleep deprivation. The supplementation prevented the expected drop in brain pH (reducing deleterious cellular acidification), stabilized intracellular PCr and ATP levels, and resulted in significantly improved short-term memory, processing speed, and executive reasoning compared to the placebo group 2783730. Furthermore, self-reported fatigue and drowsiness scales were significantly improved 37. Crucially, these metabolic and cognitive effects peaked roughly four hours post-administration and persisted for up to nine hours, suggesting that acute high-dose protocols can serve as an immediate, on-demand metabolic buffer during periods of extreme fatigue, highly relevant for shift workers, medical professionals, or military personnel 83730.
Hypoxic Stress
Hypoxia (oxygen deprivation) similarly models an acute metabolic failure state and shares distinct pathological characteristics with mild traumatic brain injuries 2. In a rigorous randomized, double-blind crossover trial, healthy adults were supplemented with 20g of creatine daily for seven days before being exposed to a controlled hypoxic gas mixture (10% oxygen) for 90 minutes 228. The hypoxic environment predictably impaired a wide range of neuropsychological processes. However, subjects who received the creatine pretreatment demonstrated a 9.2% increase in regional brain creatine levels prior to the event, which effectively restored hypoxia-induced decrements in continuous performance tests and significantly attenuated omission errors compared to the placebo state 228.
Aging, Neurodegeneration, and the Muscle-Brain Axis
As the global population ages, interventions capable of preserving cognitive integrity have become a primary focus of neurogerontology. Age-related cognitive decline intimately involves mitochondrial dysfunction, increased oxidative stress, and deteriorating cellular bioenergetics 1823.
Age-Related Cognitive Decline
A 2026 systematic review specifically analyzed creatine's independent effects on older adults (aged 55 and older). Reviewing six distinct studies encompassing 1,542 participants, the analysis found that 83.3% of the included studies reported a positive association between creatine intake and cognitive function, most notably in the domains of memory and attention 31. Separate meta-analyses corroborate this age-dependent efficacy, showing that memory improvements are significantly more pronounced in older adults (aged 66 - 76) compared to younger cohorts (aged 11 - 31) 111.
Despite these positive signals, the existing literature assessing geriatric populations is constrained by methodological limitations. Many studies in older demographics actively combine creatine supplementation with resistance training interventions, making it difficult to isolate the independent cognitive effects of the dietary supplement versus the well-documented neurogenic benefits of physical exercise 3132. Ongoing long-term clinical trials - such as a 26-week randomized control trial initiated to evaluate visuospatial working memory and cerebral blood flow - are currently seeking to disentangle these variables by testing creatine and resistance training independently and synergistically in older adults diagnosed with mild cognitive impairment (MCI) 32.
The Muscle-Brain Axis and Myokine Signaling
While direct neural uptake via SLC6A8 represents the primary mechanism for direct cognitive enhancement, emerging research indicates an indirect, endocrine-like relationship between creatine-supplemented skeletal muscle and the brain, increasingly referred to as the "muscle-brain axis" 710.
Skeletal muscle acts as a complex endocrine organ, releasing specific cytokines and peptides known as myokines into the systemic circulation in response to mechanical contraction and loading 710. Creatine supplementation is definitively known to increase muscle work capacity, thereby enhancing the volume and intensity of resistance training a subject can perform 101734.
This increased muscular exertion heavily upregulates the secretion of specific myokines, most notably irisin 7. Irisin is capable of crossing the blood-brain barrier, where it actively stimulates the expression of Brain-Derived Neurotrophic Factor (BDNF) in the hippocampus 710. BDNF is a critical neurotrophin responsible for promoting neurogenesis, supporting synaptic plasticity, and facilitating long-term memory consolidation 710. Furthermore, creatine enhances insulin signaling and glucose uptake via GLUT-4 receptor translocation in skeletal muscle, which may independently potentiate the exercise-induced release of systemic neurotrophic factors 71033. Therefore, particularly in aging populations facing sarcopenia, the cognitive benefits of creatine may partially stem from its peripheral ability to maximize the neurogenic benefits of physical exercise.
Alzheimer's Disease and Dementia
Alzheimer's disease (AD) is characterized pathologically by amyloid-beta plaques and tau tangles, but it is increasingly viewed through the lens of profound metabolic dysfunction. Patients with AD exhibit severe deficits in cerebral glucose utilization, mitochondrial efficiency, and ATP regeneration - a cascading cellular energy crisis that actively accelerates neuronal death 18343536.
Until recently, evidence for creatine's efficacy in neurodegenerative disease was strictly preclinical. However, in 2025, researchers at the University of Kansas Medical Center completed the "Creatine to Augment Bioenergetics in Alzheimer's" (CABA) trial, marking the first interventional clinical investigation of creatine monohydrate supplementation in human AD patients 183435363738.
The single-arm pilot trial involved 20 patients (aged 60-90) diagnosed with AD, administering a high dose of 20g/day of creatine monohydrate over an eight-week period 1834353638. While the primary goal was to establish feasibility and safety, the secondary outcomes yielded highly encouraging quantitative data: 1. Brain Saturation: Magnetic resonance spectroscopic imaging (MRSI) confirmed that the high-dose supplementation successfully penetrated the BBB, resulting in an average 11% increase in total brain creatine levels across 85% of the participants (p < 0.001) 21834353638. 2. Cognitive Improvement: Cognitive performance, evaluated via the rigorous NIH Toolbox Cognition Battery, demonstrated statistically significant improvements. Global cognition (p = 0.02) and fluid cognition (p = 0.004) scores rose, alongside specific improvements in working memory (improved by ~10%), list sorting (p = 0.001), oral reading (p < 0.001), and Flanker inhibitory control and attention tests (p = 0.05) 218343538. Notably, "crystallized intelligence" (acquired long-term knowledge) remained unchanged, indicating the intervention specifically aided active, energy-dependent cognitive processing rather than static knowledge recall 183435. 3. Skeletal Muscle Preservation: Given the high rate of physical frailty and dynapenia in AD patients, researchers also measured peripheral muscular parameters. Following the 8 weeks of supplementation, participants exhibited a significant 1.9 kg increase in hand-grip strength (p = 0.02), alongside targeted reductions in specific subcutaneous fat regions (rectus femoris and vastus lateralis), demonstrating concurrent physical benefits 37. Measures of neuromuscular junction (NMJ) integrity, assessed via plasma C-terminal agrin fragment (CAF) levels, remained unchanged 37.
While the CABA trial was a small, single-arm pilot study lacking a randomized placebo control group, it provides critical clinical proof-of-concept. It demonstrates that high-dose creatine is highly tolerable in geriatric dementia populations and is capable of modulating cerebral energy reserves to potentially delay or mitigate cognitive symptom severity 183538.
The Role of Creatine in Traumatic Brain Injury and Concussion
Mild traumatic brain injury (mTBI), commonly known as a concussion, initiates a complex and highly destructive neurometabolic cascade. The physical shearing forces of a concussion trigger a massive efflux of intracellular potassium and a corresponding influx of calcium, leading to indiscriminate and uncontrolled neurotransmitter release 947. To restore fundamental ionic homeostasis, the brain's membrane pumps engage in hyper-glycolysis, rapidly depleting local ATP stores and causing a buildup of intracellular lactate. This severe cellular energy crisis is compounded by reduced cerebral blood flow and subsequent mitochondrial dysfunction, leaving the brain highly vulnerable to secondary injury and cellular death 3947.
Given creatine's primary role in ATP buffering, reduction of oxidative stress, and stabilization of cellular membranes, its application as a neuroprotective agent for TBI has generated immense theoretical and clinical interest 947394041.
Preclinical Neuroprotection Mechanisms
In animal models, both prophylactic (pre-injury) and post-injury creatine administration have consistently demonstrated powerful neuroprotective effects. Rodent models of controlled cortical impact reveal that creatine supplementation significantly reduces post-injury lactate accumulation, maintains ATP availability, decreases oxidative stress, and limits the overall size of necrotic cortical lesions 3934394041. These preclinical models suggest that creatine directly mitigates the exact bioenergetic deficits that define the acute post-concussion period.
Clinical Trials and Current Medical Guidelines
Translating these preclinical successes into effective human clinical protocols has proven challenging. The human data regarding mTBI is currently limited to a few open-label trials, predominantly focusing on pediatric populations suffering from moderate to severe TBI. A notable randomized, open-label trial involving 39 children and adolescents administered an aggressive dosage of 0.4g/kg/day of creatine for six months following injury 2343942. The supplemented cohort demonstrated faster resolution of post-traumatic amnesia, a decreased incidence of chronic headaches, dizziness, and fatigue, and significantly improved cognitive and communicative recovery metrics compared to controls 343942.
Despite these highly promising signals, the current medical consensus regarding concussion management remains highly conservative. Major governing bodies, including the 2023 consensus statement by the American Academy of Physical Medicine and Rehabilitation (PM&R) and the 2021 JAMA Network Open systematic review, do not include creatine supplementation in their recommended treatment guidelines for acute concussion or persistent post-concussion symptoms (PPCS) 47.
The primary scientific barriers preventing formal clinical endorsement include: 1. Lack of High-Quality RCTs: There are currently no completed, large-scale, double-blind, placebo-controlled trials definitively demonstrating efficacy for creatine as a post-concussion treatment in human adults 47. 2. Pharmacokinetic Delays: Because neural uptake of creatine is slow and inefficient across the blood-brain barrier, initiating supplementation after a concussion may be too late to impact the immediate acute energy crisis (which resolves over a matter of days, while brain creatine saturation takes weeks of continuous high dosing) 4739. 3. Prophylactic Efficacy: Current pharmacokinetic evidence heavily suggests creatine is far more effective as a prophylactic measure - loading the brain's energy reserves prior to injury in high-risk populations (contact sport athletes, military personnel) - rather than as an acute post-injury therapeutic 4739.
Several clinical trials, such as ongoing unphased trials tracking Rivermead Post-Concussion Symptoms Questionnaire (RPQ) scores in athletes aged 18-35, are currently underway to close this evidential gap 43. Until these results are published and peer-reviewed, creatine cannot be formally classified as a primary medical treatment for TBI, though it remains a topic of intense investigative priority.
Dosing Protocols and Safety Considerations
The physiological divergence in transport mechanisms between skeletal muscle and neural tissue necessitates distinct clinical dosing protocols.
Compartmental Saturation Thresholds
For achieving skeletal muscle saturation, the International Society of Sports Nutrition (ISSN) and decades of sports science research have established that a standard maintenance dose of 3 to 5 grams per day for 28-30 days is entirely sufficient. This can optionally be preceded by a loading phase of 20g/day (divided into four 5g doses) for 5-7 days to achieve saturation more rapidly 444546.
However, due to the resistance of the blood-brain barrier and the lack of SLC6A8 receptors on astrocytes, standard 5g/day doses rarely alter brain PCr concentrations significantly in young, healthy populations 211. To achieve meaningful changes in central nervous system bioenergetics, researchers consistently utilize and recommend higher dosing ranges: * Neurological Maintenance/Loading: 10 to 20 grams per day, often administered continuously for several weeks or months, is required to elevate brain creatine by the target ~10% 21117344256. * Acute Stress Interventions: Single high doses of 0.35g/kg (approximately 20-25g for an average adult) administered 3 to 4 hours prior to a severe stressor (e.g., extreme sleep deprivation) 2837.
| Pharmacokinetic Parameter | Skeletal Muscle | Central Nervous System (Brain) |
|---|---|---|
| Total Body Creatine Distribution | ~95% | < 5% |
| Endogenous Synthesis Capacity | None (Relies strictly on uptake) | High (Possesses AGAT and GAMT enzymes locally) |
| SLC6A8 Transporter Expression | High (Sarcolemma) | Limited (Present on Endothelium, absent on Astrocytes) |
| Maximum Uptake Potential | ~20% total increase | ~3% to 11% total increase |
| Standard Efficacious Dose | 3-5 g/day | 10-20 g/day |
Table 2: Comparison of compartmental creatine kinetics underlying the disparate dosing requirements for physical versus cognitive enhancement.
Renal Function, Toxicity Claims, and Gastrointestinal Tolerability
Given the absolute requirement of high-dose regimens (20g+ daily) to achieve neurological benefits, safety profiles over long-term administration are of paramount clinical importance. Fortunately, over 25 years of rigorous clinical research demonstrates that creatine monohydrate is exceptionally safe for the general population, even at elevated neurological doses 845474849.
Renal Function Misconceptions
The most pervasive and historically enduring misconception regarding creatine supplementation is that it induces nephrotoxicity 454748495051. This stems from a fundamental misunderstanding of renal biomarker diagnostics. Creatine in the body is naturally degraded into creatinine at a relatively constant rate, which is then filtered and excreted by the kidneys 4750. High-dose creatine supplementation naturally elevates blood serum creatinine levels due to the increased total body pool 505152.
Because standard clinical metabolic panels use serum creatinine to calculate the estimated Glomerular Filtration Rate (eGFR), an artificially elevated creatinine level will generate a falsely low eGFR, clinically mimicking acute kidney injury 5053. However, gold-standard renal function tests - such as 51Cr-EDTA clearance or cystatin C measurements, which are entirely independent of creatine metabolism - consistently demonstrate that high-dose and long-term creatine ingestion (up to 30g/day for 5 years) causes absolutely zero impairment to actual glomerular filtration, renal architecture, or proteinuria rates in healthy individuals 4750. Claims by certain regulatory agencies (such as the historical AFSSA claims regarding mutagenicity via heterocyclic amines or formaldehyde excretion) have been rigorously investigated and dismissed as occurring well within normal, safe physiological ranges without impacting organ function 54.
Calibrated Caveat for Older Adults and Clinical Populations: While unarguably safe for healthy demographics, older adults and patients with pre-existing renal disease (e.g., stage III chronic kidney disease, severe diabetic nephropathy) must exercise specific medical caution 4447535455. In elderly populations, the Cockcroft-Gault formula is clinically required to accurately assess baseline creatinine clearance, as age-related sarcopenia naturally reduces baseline creatinine production, potentially masking underlying renal insufficiency prior to starting high-dose creatine 55. The American Geriatrics Society explicitly contraindicates high-dose creatine use if a patient's baseline creatinine clearance falls below 60 mL/min 55.
Gastrointestinal Distress and Hydration
While high doses do not damage organs, they can induce temporary, highly dose-dependent side effects. In clinical trials evaluating loading doses (20g/day), gastrointestinal distress is the most commonly reported adverse event. A 2025 single-blind, randomized clinical trial investigating fluid retention and GI distress found that nearly 79.2% of participants consuming a 20g/day loading dose reported some degree of undesired GI symptoms 475152. These symptoms, primarily reported by female participants (81%), included mild to moderate bloating, stomach discomfort, and transient diarrhea . These effects are generally driven by osmotic fluid shifts in the gut when large boluses of the highly osmotic powder are consumed simultaneously without adequate water solvent 4752. Splitting a 20g neurological dose into four distinct 5g intervals throughout the day drastically reduces the incidence of GI upset 944.
Additionally, historical claims that creatine causes systemic dehydration or muscle cramping are entirely unsupported by the modern literature. Research consistently demonstrates that creatine actually enhances cellular hydration and thermoregulation during intense exertion, statistically reducing the incidence of cramps compared to placebo 454751. The minor increase in body weight (1-2 kg) commonly observed during the first week of high-dose supplementation is entirely attributable to functional intracellular water retention in skeletal muscle, not systemic edema or adipogenesis 444852.
Conclusion
The scientific consensus surrounding creatine monohydrate is evolving rapidly. Long established as the premier ergogenic aid for muscular performance, an exhaustive body of modern, peer-reviewed research confirms that creatine operates as a potent modulator of central nervous system bioenergetics.
While the blood-brain barrier inherently limits neural creatine uptake compared to skeletal muscle due to the lack of astrocytic SLC6A8 transporters, targeted high-dose protocols (10-20g daily) have proven capable of penetrating this barrier, resulting in modest but clinically significant increases in total cerebral creatine pools. The cognitive benefits resulting from this saturation are heavily state-dependent. In healthy, unstressed individuals - particularly omnivores - the cognitive returns are modest, primarily restricted to marginal improvements in short-term memory and processing speed.
However, under conditions of acute metabolic stress (such as extreme sleep deprivation or hypoxia) or chronic cellular energy crises (aging, Alzheimer's disease), creatine serves as a critical energetic buffer. High-dose administration stabilizes intracellular pH, preserves ATP regeneration, and noticeably mitigates deficits in processing speed, attention, and executive reasoning. While current medical guidelines do not yet formally endorse creatine as a post-injury therapeutic for mild traumatic brain injury, the theoretical framework and preclinical neuroprotection data warrant continued aggressive exploration.
Ultimately, creatine monohydrate represents a remarkably safe, well-tolerated, low-cost intervention with profound pleiotropic effects, offering substantial neuroprotective and cognitive resilience benefits that extend far beyond the parameters of skeletal muscle hypertrophy.