Cognitive rest and recovery from mental exhaustion
The modern occupational and digital landscape places unprecedented demands on human executive function, leading to widespread phenomena such as vigilance decrement, directed attention fatigue, and clinical burnout. Understanding cognitive rest requires delineating it from absolute physical rest and examining the specific neurobiological mechanisms that govern energy depletion and restoration in the brain. This report provides an exhaustive analysis of cognitive rest, the theoretical frameworks that govern mental recovery, the efficacy of micro-interventions, and the clinical timelines required to recover from severe, chronic mental exhaustion.
Neurobiological Mechanisms of Cognitive Rest
Cognitive rest is not merely the cessation of physical activity or the absence of goal-directed work. True cognitive recovery is an active neurological process characterized by distinct shifts in brain network activation, metabolic clearing, and synaptic recalibration.
Default Mode Network and Task Positive Network
The neurocognitive mechanisms underlying mental fatigue and recovery involve a delicate balance between large-scale neural networks. When the human brain is engaged in concentrated effort, the frontoparietal control network - often referred to as the Task Positive Network (TPN) - dominates neural activity 12. The TPN is responsible for sustained attention, working memory, and executive function. However, the activation of the TPN occurs in an anticorrelated manner with the Default Mode Network (DMN), a system of interconnected brain regions including the medial prefrontal cortex, posterior cingulate cortex, and hippocampus 12.
The DMN is associated with self-referential thought, introspective processing, autobiographical memory consolidation, and creative insight 12. Continuous suppression of the DMN over extended periods leads to neural fatigue and attentional rigidity, manifesting behaviorally as "vigilance decrement" - a gradual reduction in task accuracy over time 12.
Cognitive rest occurs when the TPN is deactivated, allowing the DMN to momentarily reactivate. This oscillation between networks is physiologically necessary to reset synaptic efficiency and facilitate mental flexibility. Functional MRI analyses reveal that even brief rest intervals reactivate memory-encoding networks in the hippocampus and parietal cortex, strengthening synaptic connections involved in recently learned information 1.
| Neural Network | Primary Cognitive Function | Activation State | Consequences of Chronic Alteration |
|---|---|---|---|
| Task Positive Network (TPN) | Goal-directed attention, problem-solving, executive control. | Active during focused work and external stimulus processing. | Over-activation leads to vigilance decrement, cognitive fatigue, and depleted executive resources. |
| Default Mode Network (DMN) | Memory consolidation, introspection, future simulation, self-referential thought. | Active during rest, mind-wandering, and internally directed thought. | Maladaptive suppression prevents memory consolidation; maladaptive hyper-connectivity reinforces rumination and threat-anticipation. |
| Salience Network / Anterior Cingulate Cortex (ACC) | Conflict monitoring, threat detection, affect regulation. | Active during novel, uncertain, or threatening stimuli detection. | Persistent activation fosters a chronic state of physiological readiness and heightened stress reactivity. |
Neurological Signatures of Recovery
Recovery from acute cognitive load is marked by specific neurological signatures. Following an acute stressor or period of intense concentration, resilient individuals exhibit a measurable shift in brain activity within approximately 60 minutes 3. This shift is characterized by a decrease in salience-network activity (associated with alarm and threat detection) and an increase in DMN activation 3. Concurrently, electroencephalography (EEG) readings show a marked fall in high-beta EEG power, an indicator of settling neural arousal, alongside an increase in alpha wave synchronization, which denotes a state of wakeful relaxation 345.
These nonconscious brain changes continue to unfold even after the physical sensations of stress or fatigue have vanished, underscoring that cognitive recovery operates on a distinct, extended timeline compared to cardiovascular or muscular recovery 3.
Digital Interruption and Pseudo-Rest
A critical barrier to cognitive rest in contemporary environments is the reliance on digital devices during intended recovery periods. Behaviors such as scrolling through social media or consuming rapid-fire short-form videos fail to induce cognitive rest and instead exacerbate mental fatigue 767.
Digital consumption acts as a form of "pseudo-rest." While the individual is physically stationary, the brain's salience network and TPN remain highly engaged by the rapid succession of novel stimuli. Social media platforms exploit the brain's uncertainty reward loop, triggering dopamine-driven anticipation circuits similar to those activated by gambling 610. Each novel stimulus is often followed by a minor release of cortisol due to the brain's innate negativity bias, keeping the autonomic nervous system in a state of low-level hyperarousal 76.
This chronic autonomic arousal blunts interoception - the brain's ability to sense internal physiological states, processed largely in the anterior insula cortex 7. Consequently, individuals lose the ability to recognize their own fatigue. Furthermore, digital pseudo-rest leaves substantial "attention residue." The brain attempts to process unresolved emotional stimuli in the background, further depleting limited attention bandwidth upon returning to primary tasks 710. Extended periods of this behavior are linked to structural changes in both gray matter (the cortex responsible for emotional regulation and impulse control) and white matter tracts (the communication fibers between brain regions), resulting in diminished cognitive flexibility and reduced academic or professional performance 710.
Theoretical Models of Cognitive Recovery
Several theoretical models attempt to explain how cognitive resources are depleted and subsequently restored. These range from satiation-based metaphors of mental energy to environmental interaction theories that emphasize the restorative properties of specific surroundings.
Attention Restoration Theory
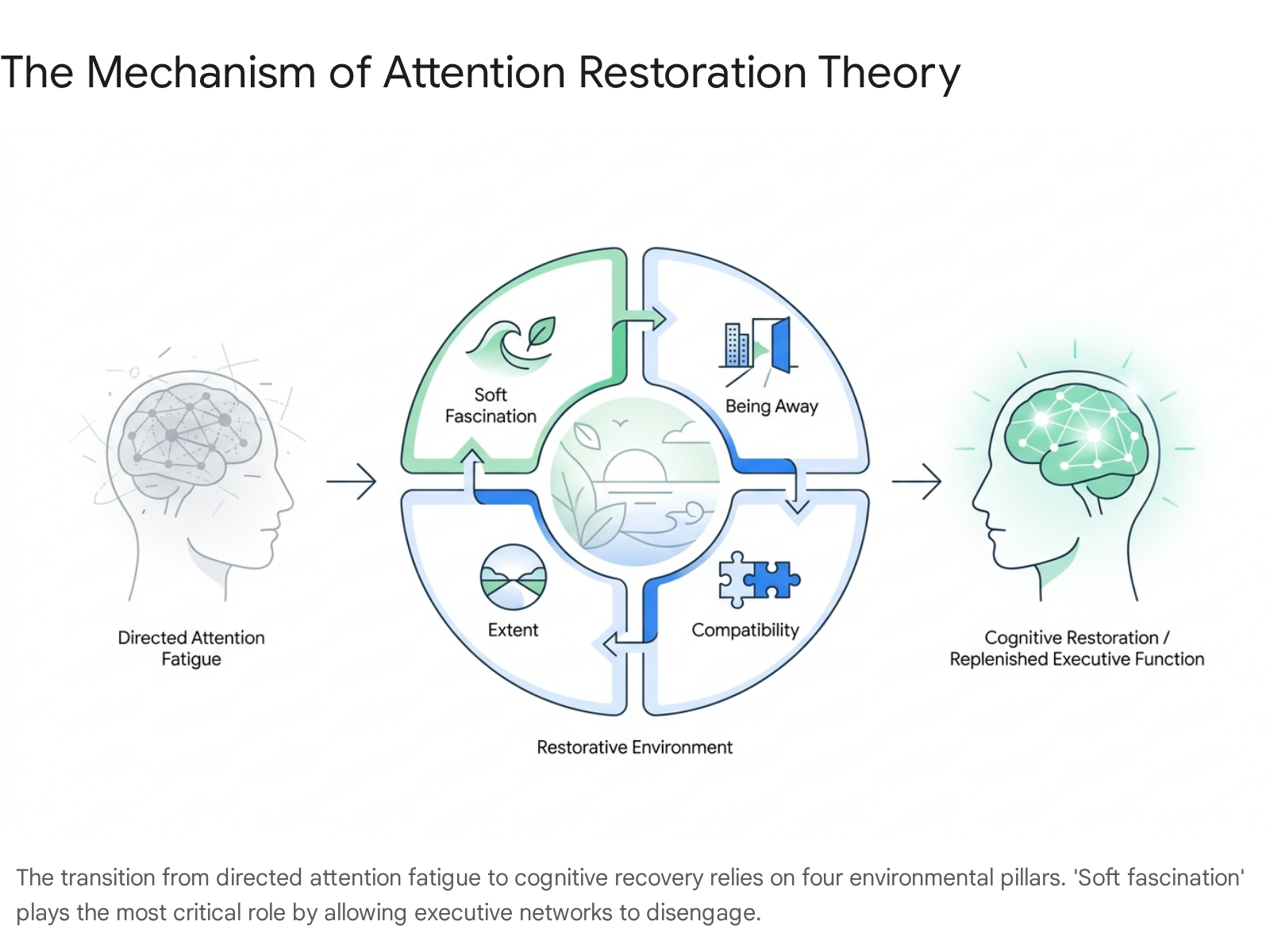
Attention Restoration Theory (ART), developed by Rachel and Stephen Kaplan in the 1980s, posits that the capacity of the brain to focus on specific stimuli is limited and highly susceptible to "directed attention fatigue" 118. ART suggests that recovery occurs not through absolute sensory deprivation, but through exposure to environments that engage involuntary attention without demanding executive control.
According to ART, a truly restorative environment must possess four distinct properties: 1. Extent: The environment must have sufficient scope to make the individual feel immersed, creating a coherent alternative world that occupies the mind without taxing it 118. 2. Being Away: The setting must provide psychological or physical detachment from routine daily demands, stressors, and habitual activities 813. 3. Soft Fascination: The environment must contain elements that capture attention effortlessly (e.g., rustling leaves, flowing water, cloud movements), allowing the executive attention system to rest. This contrasts with "hard fascination" (e.g., a fast-paced television show or high-stakes sporting event), which captures attention forcefully and prevents the cognitive control networks from disengaging 11813. 4. Compatibility: The environment must align with the individual's personal preferences, inclinations, and intended activities 118.
Empirical Evidence for Nature Exposure
Empirical evidence robustly supports ART, demonstrating that nature exposure acts as a powerful catalyst for cognitive rest. Electroencephalography (EEG) and functional imaging studies reveal that interaction with natural environments - or even high-fidelity natural imagery indoors - triggers measurable physiological recalibrations 49.
Exposure to green spaces or nature media is associated with an increase in alpha brain wave power (indicative of relaxed, inward-focused attention) and enhanced neural connectivity 5. Conversely, urban or highly cluttered visual environments elevate beta and gamma activity, which correspond to arousal, stress, and directed attention 5. EEG monitoring during cognitive tasks following nature exposure shows a lower delta-to-theta ratio (DTR), delta-to-alpha ratio (DAR), and alpha-to-beta ratio (ABR), collectively indicating improved working memory performance and lower cognitive load 4.
The brain processes the fractal patterns found in nature (such as branching trees or water ripples) with extreme efficiency. These patterns require significantly less mental effort to parse than the visually dense, fast-paced, and largely orthogonal stimuli of built or digital environments 910. Consequently, the visual cortex habituates more easily, sensory load eases, and the body shifts out of sympathetic "fight-or-flight" activation, marked by a measurable deactivation of the amygdala and a reduction in heart rate variability 1910.
| Environmental Type | Neurological Impact | Cognitive Outcome |
|---|---|---|
| Blue Spaces (Wetlands, Oceans) | Most rapid and pronounced stress recovery; strong alpha wave generation 5. | Accelerated emotional regulation and attenuation of rumination 59. |
| Green Spaces (Forests, Parks) | Reduced amygdala activation; lowered ABR and DTR ratios 49. | Restored directed attention; improved working memory 45. |
| Grey Spaces (Urban, Industrial) | Elevated beta and gamma activity; high sensory processing demand 5. | Increased cognitive fatigue; delayed or obstructed autonomic recovery 5. |
| Virtual/Indoor Nature | Moderate alpha wave increase; parasympathetic engagement 45. | Partial cognitive restoration; highly effective for micro-interventions 45. |
Active Recovery Versus Passive Recovery
Cognitive recovery strategies are broadly categorized into passive and active modalities, both of which are required depending on the depth of the exhaustion.
Passive recovery encompasses absolute sensory rest, deep sleep, and non-engagement. This is essential for cellular repair, toxin clearance during deep sleep phases, and basal metabolic recovery 1611. In deep rest, the parasympathetic nervous system governs physiological maintenance, orchestrated partially by the vagus nerve signaling safety to the brain and internal organs 12.
Conversely, active recovery involves low-intensity cognitive or physical engagement that maintains momentum while shifting the neural networks in use 1113. Examples include light walking, engaging in effortless hobbies, or practicing nature observation. Just as absolute physical immobilisation can lead to muscle atrophy and insulin resistance, absolute cognitive immobilisation can sometimes hinder the processing of trauma or complex emotions 1114. Active recovery prevents the absolute deconditioning of attention and has been shown to be highly effective in mitigating mental fatigue without requiring total disengagement 1113.
Efficacy and Parameters of Micro-Breaks
While long-term rest is necessary for chronic fatigue, the daily management of cognitive load relies heavily on "micro-breaks." A micro-break is defined as a short, informal pause taken between tasks during extended work sessions, typically lasting from 30 seconds to 10 minutes 1522.
Duration and Frequency Thresholds
The efficacy of micro-breaks is supported by extensive occupational health and cognitive psychology research. A comprehensive meta-analysis of 22 independent study samples (N = 2,335) assessed the impact of micro-breaks on well-being and performance 1516. The findings revealed statistically significant effects: micro-breaks boosted subjective vigor (Cohen's d = 0.36) and reduced fatigue (Cohen's d = 0.35) 1516.
The optimal duration of a micro-break depends heavily on the intensity of the preceding task. Studies indicate that for tasks requiring sustained visual attention (such as screen work), a micro-break as short as 40 seconds - particularly when viewing a natural scene - is sufficient to trigger DMN reactivation, interrupt habituation cycles, and prevent vigilance decrement 215. The "20-20-20 rule" (looking 20 feet away for 20 seconds every 20 minutes) functions by shifting the pattern of activation in the visual cortex, providing a tiny attentional reset that breaks the monotony driving cognitive decay 2.
An experiment evaluating university students engaging in a 45-minute continuous task found that a 5-minute break significantly preserved cognitive control and accuracy compared to continuous work 17. However, meta-regression analyses indicate that while micro-breaks of under 10 minutes are highly effective for preserving well-being and recovering from low-demand cognitive tasks, tasks requiring a high cognitive load necessitate longer recovery intervals for performance metrics to fully rebound 15161819.
Task Disengagement and Activity Types
The specific activity performed during a micro-break heavily influences its restorative potential. Research examining different interventions during mentally demanding tasks compared unstructured breaks with specific physical or relaxation exercises 20.
| Micro-Break Modality | Immediate Effect | Enduring Effect (20 min post-break) | Primary Neurological/Physiological Benefit |
|---|---|---|---|
| Unstructured Pause (No directed activity; remaining at desk) | Mild increase in subjective vigor 20. | Rapid decay of focus; limited impact on overall fatigue 2021. | Allows brief DMN activation, though the risk of digital distraction and attention residue remains high 720. |
| Relaxation Exercise (Deep breathing, meditation) | Moderate decrease in fatigue 20. | Maintained lower fatigue levels into subsequent tasks 20. | Autonomic recalibration; increases alpha wave activity, lowers cortisol, and promotes parasympathetic dominance 1220. |
| Physical Movement (Stretching, light walking) | Significant increase in vigor and decreased fatigue 20. | Sustained vigor and attention capacity 2022. | Increases cerebral blood flow; relieves musculoskeletal discomfort and sympathetic nervous system pooling 132223. |
Furthermore, the timing of micro-breaks should match the cognitive demands of the work. Heavy cognitive tasks (e.g., complex problem-solving, coding) benefit from high-frequency breaks (e.g., 5 minutes of rest for every 20-25 minutes of work), whereas tasks requiring flow-state momentum (e.g., writing, creative design) may benefit from longer, less frequent intervals (e.g., 10 minutes of rest after 45-50 minutes of work) 22.
Clinical Staging of Mental Exhaustion
When daily cognitive recovery is insufficient and micro-breaks are neglected, acute mental fatigue compounds into chronic exhaustion. The World Health Organization (WHO) formally classifies burnout in the 11th Revision of the International Classification of Diseases (ICD-11) as an occupational phenomenon resulting from chronic workplace stress that has not been successfully managed 24252627. It is characterized by three core dimensions: energy depletion or exhaustion, increased mental distance or cynicism toward one's job, and reduced professional efficacy 24252628.
Phases of Burnout Progression
Burnout is not a sudden collapse but a progressive physiological and psychological deterioration. Researchers and clinicians conceptualize this progression through identifiable phases, allowing for targeted interventions before total collapse occurs 293730.
| Burnout Phase | Psychological Experience | Physical & Behavioral Manifestations | Clinical Trajectory |
|---|---|---|---|
| Phase 1: The Stressed Phase (Perceived inability) | Anticipatory anxiety; racing thoughts about responsibilities; inability to detach during off-hours 373039. | Increased tension and hyperarousal; sleep onset issues; higher than normal energy expenditure 37. | Reversible with strict boundaries, workload management, and enhanced daily recovery protocols 37. |
| Phase 2: Chronic Exhaustion (Protective withdrawal) | Cynicism toward work; resentment of demands; diminishing sense of accomplishment 293039. | Persistent fatigue; procrastination; social withdrawal; medically unexplained muscle spasms or headaches 2940. | Requires structured time away from the stressor, therapeutic support, and significant lifestyle adjustments 2930. |
| Phase 3: Complete / Habitual Burnout (Confirmed collapse) | Profound identity crisis related to professional role; complete emotional detachment; despair 3739. | Inability to execute basic tasks; panic attacks; severe cognitive impairment; risk of major depressive disorder 2931. | Requires immediate medical intervention, extended sick leave (months to years), and comprehensive rehabilitation 2937. |
Stress-Induced Exhaustion Disorder
In clinical settings, particularly in Northern Europe, severe burnout is medicalized to facilitate rigorous treatment protocols. In Sweden, "Exhaustion Disorder" (ED) or utmattningssyndrom is recognized as a specific medical diagnosis (ICD-10-SE code F43.8) 32333435.
ED is delineated from standard adjustment disorders or depression, although it often presents with comorbid depressive and anxiety symptoms 323436. The diagnostic criteria established by the Swedish National Board of Health and Welfare dictate that the patient must have experienced at least six months of identifiable stress exposure 323447. This prolonged stress culminates in a severe lack of mental energy lasting for at least two weeks, accompanied by at least four out of six minor criteria, including sleep disruption, gastrointestinal distress, cardiovascular symptoms, and pronounced cognitive impairment 32343647.
The Karolinska Exhaustion Disorder Scale (KEDS) is a heavily utilized clinical assessment tool that isolates exhaustion symptoms from depression and anxiety. A cut-off score of 19 on the 54-point KEDS demonstrates high sensitivity and specificity (over 95%) in identifying patients suffering from severe ED 3237.
Cognitive Impairment Profiles
The cognitive deficits associated with chronic burnout and ED are measurable and profound, extending far beyond subjective feelings of tiredness. Systematic reviews and meta-analyses assessing cognitive function in clinical burnout demonstrate broad-spectrum impairment across multiple functional domains 3839.
Patients with clinical burnout exhibit small to moderate, but statistically significant, impairments in episodic memory, short-term and working memory, executive function, attention, processing speed, and verbal fluency 3839. Notably, crystallized intelligence and visuospatial abilities typically remain intact, suggesting that the deficit lies primarily in the dynamic, energy-intensive executive control networks (the TPN) rather than in stored knowledge structures 383940.
Biological Correlates of Exhaustion
The search for a single, definitive biological marker of burnout has yielded heterogeneous results. A scoping review of studies tracking biological biomarkers alongside validated burnout measures in acute care healthcare workers found no single reproducible biomarker 41.
While the hypothalamic - pituitary - adrenal (HPA) axis (specifically cortisol levels) and autonomic function (such as heart rate variability) are frequently disrupted in burned-out individuals, these markers are highly sensitive to circadian timing, shift work, sleep loss, and overlapping affective symptoms 41. Current evidence suggests that burnout induces multi-system dysregulation rather than a localized neurochemical deficit. As such, physiological markers are best interpreted as indicators of autonomic strain and impaired recovery capacity rather than standalone diagnostic tools 4142.
Clinical Milestones and Recovery Timelines
The timeline for recovery from mental exhaustion is highly variable and depends intrinsically on the severity of the depletion prior to intervention. It is a common misconception that a brief vacation or extended weekend can cure burnout; true physiological and neural recovery requires extended, phased rehabilitation 2443.
Short-Term Autonomic Stabilization
Clinical data suggests that burnout recovery follows a specific sequential hierarchy of symptom resolution 162931: * Weeks 2-4: Sleep and Nervous System Rest. The earliest phase of recovery requires massive autonomic nervous system regulation. Sleep architecture improves, and the body begins to process built-up stress hormones. Absolute cognitive rest and psychological detachment from work demands are functional requirements during this period 162531. * Weeks 4-8: Cognitive Re-emergence. Following physical stabilization, patients begin to experience a lifting of mental fog. Decision-making capacity slowly returns, and analysis paralysis decreases. However, cognitive stamina remains extremely low, and premature exposure to complex tasks can trigger rapid relapse 242931. * Weeks 8-12: Emotional Expansion. The final short-term milestone is the return of emotional bandwidth. Cynicism diminishes, emotional reactivity calms down, and individuals begin to experience genuine emotional ranges beyond irritability and apathy 242931.
For mild cases of burnout, this 4-to-12-week timeline may result in a near-complete functional return 2429. However, for moderate cases, tangible, robust recovery where stress resilience noticeably improves typically materializes between months 4 and 6 2429.
Long-Term Cognitive and Emotional Rehabilitation
For severe cases of clinical burnout and Exhaustion Disorder, full rehabilitation is a multi-year process. Evidence indicates that recovery for severe cases ranges from 1 to 3 years, and in some instances, up to 5 years 2431.
Disturbingly, longitudinal follow-ups of Swedish patients treated for ED demonstrate that subjective and objective cognitive difficulties often persist long after the emotional and physical symptoms have resolved. A 6-to-10-year follow-up study of ED patients found that while overall well-being improved, many patients reported lingering cognitive symptoms of varying severity, particularly regarding executive control and stress tolerance 4044. Approximately 50% of individuals diagnosed with ED report fatigue and decreased stress tolerance up to seven years after initial treatment 44. This suggests that severe, prolonged stress may induce long-lasting alterations in neural plasticity and network connectivity.
Return-to-Work Protocols and Reintegration
Because clinical burnout and Exhaustion Disorder result in long-term absenteeism, occupational health frameworks have developed structured models to facilitate the safe reintegration of workers. Evidence shows that abrupt returns to full-time capacity frequently result in immediate relapse. Reintegration must be managed as a therapeutic intervention rather than a purely administrative procedure 27474546.
The German Gradual Return-to-Work Model
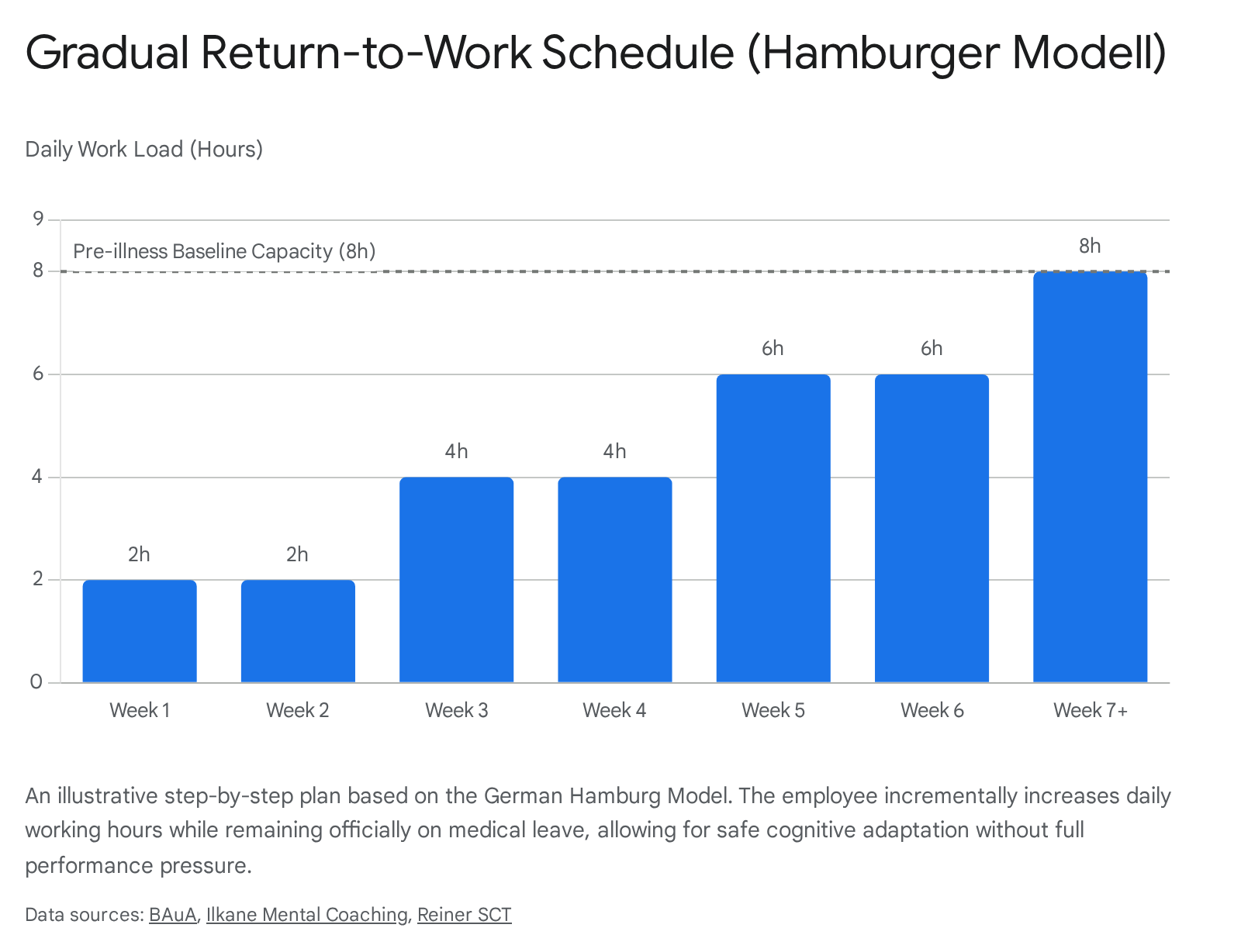
One of the most systematically studied and legally codified frameworks for cognitive and physical rehabilitation is the German Stufenweise Wiedereingliederung, commonly referred to as the "Hamburger Modell" (Hamburg Model) 464748.
Anchored in the German Social Code (SGB IX and SGB V), the Hamburger Modell is a voluntary, medical-therapeutic measure designed to gradually reintroduce an employee to their work environment over a period of 4 to 8 weeks (or considerably longer if clinically indicated) 47484950. During this entire period, the employee technically remains on medical sick leave and receives sick pay (Krankengeld) rather than standard wages. This distinction is vital, as it removes the contractual pressure of full productivity and legal liability for underperformance, allowing the individual to prioritize cognitive recovery without the fear of failure 474951.
The process begins with a physician drafting a highly individualized step-by-step plan (Stufenplan) in consultation with the patient, the employer, and the health insurance provider 474851.
The step plan frequently initiates at a minimal threshold - for example, 2 hours per day for the first two weeks 4748. As the worker's cognitive stamina is tested and validated, the workload incrementally increases (e.g., to 4 hours, then 6 hours) until baseline capacity is reached 4748.
The model allows for immediate roll-backs if symptoms flare, ensuring that the return to work is dictated by the nervous system's capacity rather than administrative deadlines.
European Occupational Health Interventions
Broader European occupational health guidelines mirror these principles, emphasizing that return-to-work is a dynamic and fragile process that requires systemic organizational support 45525354. Occupational health services (OHS) focus on designing phased RTW plans that account not just for time, but for specific cognitive, physical, and emotional demands 4555.
Effective interventions include: * Job Demands Adjustments: Temporarily removing highly demanding cognitive tasks (e.g., complex decision-making, conflict resolution, multitasking, heavy lifting) and replacing them with highly structured, predictable tasks to minimize the strain on the executive control networks 264755. * Ergonomic and Sensory Adjustments: Reducing sensory overload in the workplace (e.g., providing quiet spaces, limiting required screen time, allowing home-office days) to prevent rapid depletion of the individual's limited attention resources 264555. * Rehabilitation Coordination: Using a dedicated case manager or RTW coordinator to facilitate communication between the healthcare provider, the employee, and the management. Studies show that structured convergence dialogues between these parties significantly enhance RTW outcomes, balance relationships, and reduce the likelihood of relapse by shifting the focus toward sustainable health rather than immediate output 2835.
Cognitive rest is an active, neurobiologically essential process that requires intentional disengagement of the brain's executive networks to facilitate the consolidation of memory, the clearing of metabolic waste, and the resetting of synaptic efficiency. Brief micro-breaks and exposure to natural environments serve as highly effective daily interventions to mitigate vigilance decrement and preserve cognitive bandwidth. However, when these restorative practices are neglected and replaced with digital pseudo-rest or relentless occupational demands, the resultant chronic stress severely damages executive function, culminating in clinical burnout or Exhaustion Disorder. Recovery from such states transcends simple rest; it demands months to years of structural rehabilitation, encompassing nervous system regulation, gradual cognitive re-engagement, and carefully orchestrated return-to-work protocols. To sustain long-term occupational health, both individuals and organizations must recognize cognitive rest not as a luxury or a cessation of productivity, but as the fundamental biological prerequisite for sustained executive function and mental resilience.