5 Scenarios for Longevity Breakthroughs by 2040
By 2040, human longevity breakthroughs will likely emerge from five key areas: artificial intelligence-driven drug discovery, repurposed metabolic drugs, targeted senolytics, precise mTOR inhibition, and partial cellular reprogramming. Rather than extending the absolute biological limit of the human lifespan, these therapies will primarily focus on expanding the "healthspan" - the total years lived free of debilitating chronic disease. This biological compression of morbidity will not only redefine aging but will necessitate massive structural shifts in global pension systems, labor markets, and healthcare equity.
The Biological Ceiling vs. The Healthspan Revolution
For over a century, public health and medical advancements have steadily increased average human life expectancy. In the United States, life expectancy at birth increased from roughly 47 years at the beginning of the 20th century to nearly 78 years by the century's end 1. However, recent biodemographic data strongly suggests that humanity is asymptotically approaching a strict biological limit to maximum lifespan.
A landmark study published in Nature Aging demonstrated that while life expectancy at birth increased across the globe between 1990 and 2019, the maximum age of survival essentially stagnated 11. The longest-lived person on record remains Jeanne Calment, a French woman whose age at death in 1997 was verified at 122 years and 164 days 23. No one has verifiably surpassed this record in nearly three decades.
This stagnation points to what researchers call a "glass mortality floor." Medical and public health advances over the last thirty years have allowed more people to survive into their 80s and 90s, but they have failed to fundamentally slow the biological aging process itself 1. Evolution simply prioritizes the ability to pass on genes - favoring rapid growth and reproduction - rather than the biological maintenance required to sustain extreme old age 1. As a result, the age at death has been compressed into a shorter window, crowding more of the population closer to the limit without actually moving the limit 1.
Redefining the Goal: Extending Healthspan
The modern longevity movement has recognized the limitations of merely expanding the morbidity span - the period at the end of life characterized by chronic disease and medical interventions 46. If medical science only succeeds in pushing a frail body to live a few years longer, the achievement is hollow 67. Consequently, the new paradigm in aging research is "geroscience," which pursues the extension of healthspan 47.
Healthspan focuses on the period of life spent in good health, free from debilitating diseases, measuring vitality, mobility, and independence 67. Geroscience aims to target the underlying, root-cause mechanisms of aging - often referred to as the biological hallmarks of aging. By slowing these fundamental processes, interventions could theoretically delay the onset of multiple age-related diseases simultaneously, allowing an average person to reach 100 in the same robust health as a genetic centenarian 465.
If current scientific and regulatory trajectories hold, the next 15 years will be defined by five distinct scenarios for translating this geroscience into human clinical breakthroughs.
Scenario 1: AI Restructures Longevity Drug Discovery
The traditional pharmaceutical model is famously slow, incredibly expensive, and plagued by clinical trial failure rates that routinely exceed 90% 9. For decades, the use of artificial intelligence in drug discovery was viewed largely as a theoretical, curiosity-driven experiment 910. By early 2026, however, AI transitioned into a production-ready infrastructure, transforming molecular biology into an engineering discipline and radically accelerating the pace at which anti-aging therapeutics are discovered and tested 910.
The Clinical Validation of AI-Generated Compounds
As of early 2026, more than 173 AI-discovered programs are in active clinical development. This pipeline includes approximately 94 programs in Phase I, 56 in Phase II, and 15 in Phase III 11.
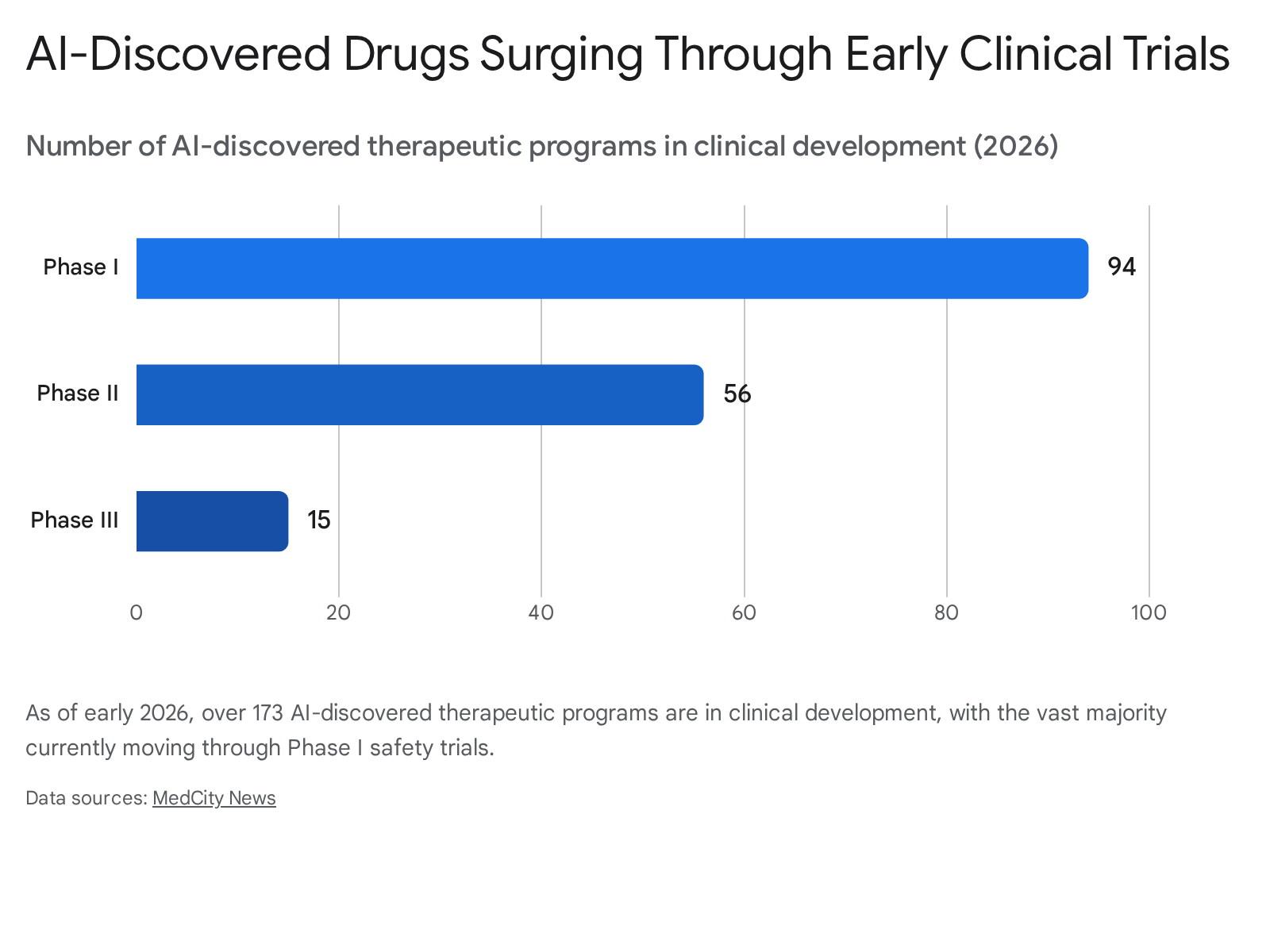
The early success metrics are unprecedented in the history of pharmacology. AI-discovered compounds are demonstrating 80% to 90% Phase I success rates, a stark contrast to the historical baseline of 40% to 65% for traditionally discovered drugs 11.
Furthermore, AI has drastically compressed discovery timelines. Companies like Insilico Medicine are moving from the initial identification of a biological target to the launch of Phase I human trials in under 30 months - a milestone that typically takes traditional pharmaceutical companies four to six years to achieve 11. Insilico Medicine built its platform, PandaOmics, specifically around aging biology, identifying dual-purpose targets linked to the core hallmarks of aging 11. Their success prompted a massive $2.75 billion partnership with Eli Lilly in 2025 to develop and commercialize novel oral therapeutics globally 11.
Other major collaborations are validating the sector. The biotechnology company Gero entered a joint research and license agreement with Chugai Pharmaceutical to develop novel antibody drugs for age-related diseases 1112. Utilizing a physics-informed AI model trained on human datasets, Gero identified novel anti-aging candidates that successfully extended lifespan in animal models, with over 70% of the identified compounds showing statistically significant results 1112. Similarly, companies like Chai Discovery have reported that their AI models can now move molecules from computational design to laboratory validation with reliability that far exceeds historical averages 9.
The 2040 Outlook for AI Geroscience
By 2040, it is highly probable that the primary engine for novel longevity therapeutics will be AI-driven structural biology and computational modeling. Current estimates suggest that the share of biotech-produced drugs will rise to almost 60% of global pharma sales by 2030, largely driven by AI integration 13.
However, the path to 2040 is not without friction. A 2025 study by MIT found that nearly 95% of enterprise generative AI pilots failed to deliver measurable business impact, often because the systems remained disconnected from real lab workflows, data foundations, and regulatory constraints 10. The next decade of AI in biotech will be defined not by new algorithms, but by building dependable, regulated discovery infrastructure 10. Additionally, while AI-discovered compounds show clear superiority in Phase I safety trials, current evidence from 2026 shows no demonstrated superiority in Phase II efficacy trials compared to traditional methods 11. The true test for the longevity industry will be whether these AI-designed molecules can successfully navigate the stringent efficacy requirements of Phase III trials over the next decade.
Scenario 2: Metabolic Repurposing Becomes the Healthspan Foundation
Before entirely novel, AI-generated gene therapies reach the public market, the most significant and immediate longevity breakthroughs by 2040 will likely come from repurposing existing, FDA-approved metabolic drugs. Two primary drug classes currently dominate the longevity clinical landscape: Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and biguanides, specifically metformin.
GLP-1 Agonists: Rebalancing the Aging Body
Initially developed to manage type 2 diabetes and obesity, GLP-1 RAs such as semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) are increasingly being viewed by researchers as practical, multi-system gerotherapeutics. Extensive preclinical and clinical data indicate that these drugs positively modulate all 12 hallmarks of aging, which include genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, mitochondrial dysfunction, cellular senescence, and chronic inflammation (inflammaging) 141516.
The clinical expression of this biological modulation is striking. Across massive, landmark cardiovascular outcomes trials such as LEADER, SUSTAIN-6, and SELECT, GLP-1 RAs demonstrated robust cardiovascular protection, yielding a 20% reduction in major adverse cardiovascular events (MACE), including heart attacks, strokes, and cardiovascular deaths 156. Importantly, these benefits extend to non-diabetic individuals, suggesting mechanisms of action that go far beyond simple glucose lowering 15.
Furthermore, GLP-1 therapies preferentially target visceral adipose tissue (VAT) - the metabolically harmful fat directly linked to cardiometabolic disease - rather than purely reducing lean muscle mass 15. Preclinical models also suggest significant neuroprotective potential, showing that GLP-1 therapies can reduce amyloid and tau pathology, enhance mitochondrial function, and lower neuroinflammation in the brain 15.
To formally test these capabilities against the aging process itself, the U.S. National Institute on Aging is funding the VITAL-H (Validation and Intervention Testing for Aging, Longevity and Healthspan) trial. Beginning in 2026, the five-year, $38 million trial will enroll over 700 adults in their 60s to compare semaglutide, dapagliflozin, and low-dose rapamycin against a placebo, specifically measuring improvements in intrinsic capacity and resilience 7.
The Complex Reality of Metformin
Metformin, a remarkably cheap and widely used diabetes drug, has long been hypothesized to possess systemic anti-aging properties. Observational data has historically suggested that diabetics taking metformin actually outlive non-diabetics, a striking finding that implied the drug conferred survival benefits 19. However, these studies often suffer from methodological concerns, including residual confounding and "healthy-adherer" bias, where patients who adhere to medication protocols are generally more health-conscious overall 19.
The gold-standard test for this hypothesis is the TAME (Targeting Aging with Metformin) trial. Authorized by the FDA, this ambitious, nationwide clinical trial aims to track thousands of older adults (aged 65 - 79) without diabetes to see if metformin delays a composite endpoint of age-related diseases - specifically cardiovascular events, cancer, dementia, and all-cause mortality 19202122. While TAME has faced funding and enrollment hurdles over the years, preliminary interim analysis in 2024 of 1,200 participants suggested a 14% reduction in the incidence of this composite age-related disease endpoint compared to placebo, with full results expected to solidify in 2026 1923.
Additionally, breakthrough 2024 primate research published in the journal Cell demonstrated metformin's ability to regress brain aging markers by up to six years, alongside significant improvements in DNA methylation and mitochondrial function 20. Because non-human primates share approximately 95% genetic similarity with humans, these results bolster confidence in metformin's cross-species efficacy as an anti-aging intervention 20.
If TAME successfully proves that metformin delays multimorbidity, its regulatory importance will dwarf its mechanistic novelty. It will serve as the crucial test case for whether the FDA will accept "aging" as a treatable indication by 2040, marking a paradigm shift from treating age-related diseases individually to targeting the aging process per se 1922.
Scenario 3: Senolytics Pivot to Precision Disease Targeting
One of the most intuitively powerful concepts in longevity science is the removal of senescent cells. As the body ages, damaged cells that stop dividing often refuse to undergo apoptosis (programmed cell death). Instead, these stubborn "zombie cells" accumulate in tissues and secrete a toxic, pro-inflammatory cocktail of molecules known as the senescence-associated secretory phenotype (SASP) 82526. This SASP damages surrounding healthy tissue, driving fibrosis, inflammation, and cellular dysfunction 825.
Senolytics are a class of drugs designed to selectively eliminate these senescent cells by disabling the pro-survival networks that defend them 827. In animal models, clearing senescent cells has yielded remarkable results: increasing lifespan, restoring vascular reactivity, decreasing liver fibrosis, and reducing frailty in aged mice 58.
The Clinical Reality in 2026
The commercial momentum behind senolytics is massive. In 2026, the global senolytic drugs market was valued at $2.8 billion, with projections pushing it to $9.6 billion by 2034 26. There are currently more than 45 active clinical trials investigating various senolytic compounds or combinations - up dramatically from fewer than 15 trials in 2021 26.
The Mayo Clinic's pioneering trials utilizing a combination of the leukemia drug dasatinib and the plant flavanol quercetin (D+Q) have shown positive biological signals in humans. In early trials, a brief oral course of D+Q reduced the senescent cell burden in adipose tissue and lowered circulating SASP factors in the blood of patients with diabetic kidney disease 5827. Another trial in patients with idiopathic pulmonary fibrosis (IPF) - a fatal senescence-associated disease - found signs of improved physical function after D+Q administration 527.
However, the field is currently undergoing a scientific reality check. While early human trials have generated proof-of-biology, clear, overwhelming evidence of clinical efficacy in broad, healthy human populations is still lacking 25. The science remains strongest when senolytics are targeted at specific disease indications with a clear senescence burden, rather than being utilized as a generalized "anti-aging" panacea 2527.
Furthermore, researchers are increasingly recognizing that cellular senescence is not purely pathological. It also plays a critical, protective role in tumor suppression, tissue remodeling, and acute wound repair 25. Completely wiping out senescent cells systemically could impair the body's natural healing responses. By 2040, the senolytics pipeline will likely have matured into highly selective, localized therapies, dosed intermittently to allow natural cell cleanup, and guided by advanced biomarker strategies to quantify a patient's exact senescence burden before treatment 825.
Scenario 4: Partial Cellular Reprogramming Enters the Clinic
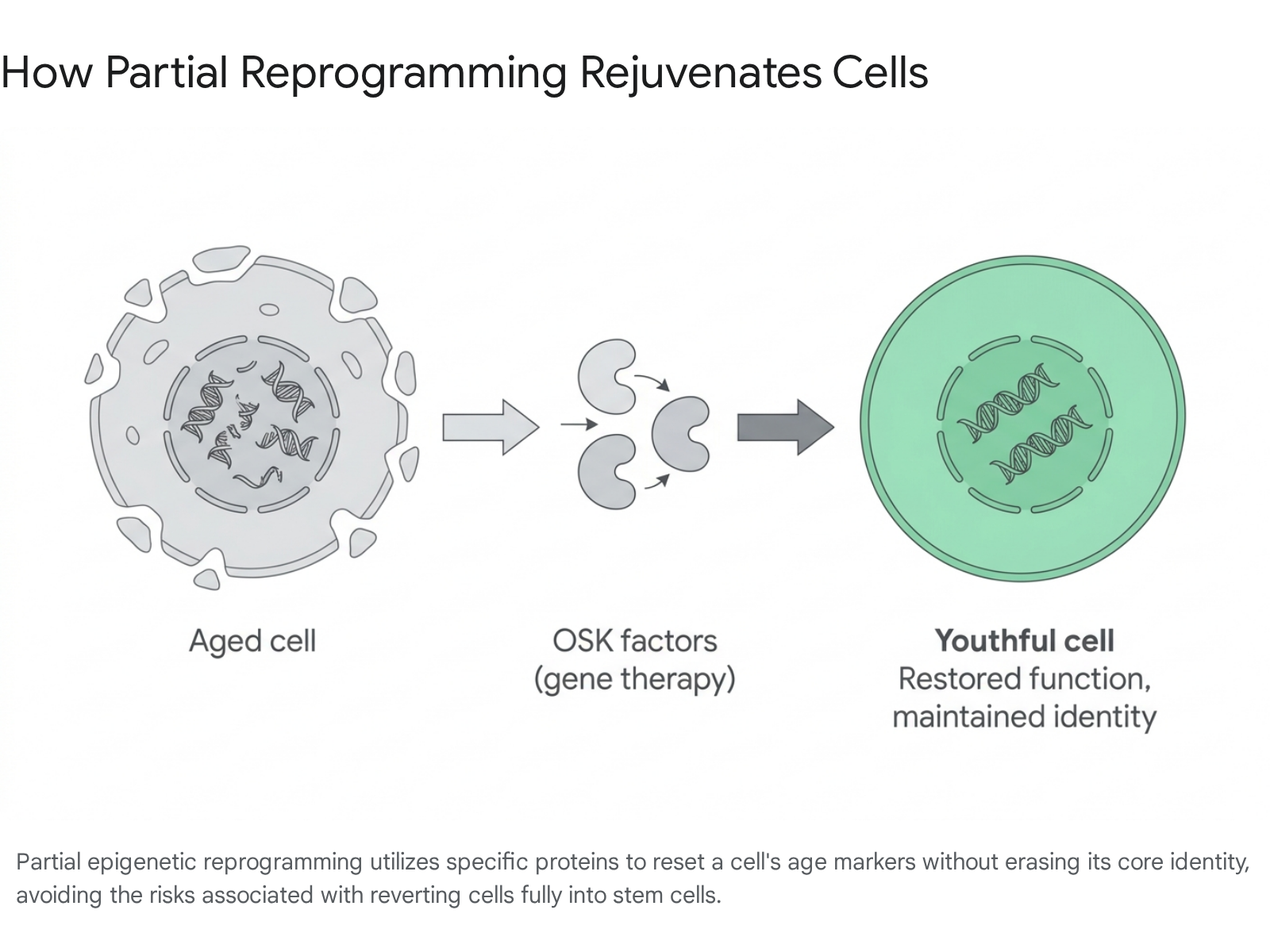
Perhaps the most radical and technologically complex scenario for 2040 is the clinical maturation of cellular reprogramming. Drawing on Nobel Prize-winning research, scientists discovered that exposing adult somatic cells to a specific cocktail of four proteins - known as Yamanaka factors (OCT-4, SOX-2, KLF-4, and c-Myc) - can revert them all the way back to a blank-slate, embryonic stem cell state 289. However, doing this inside a living human body is exceedingly dangerous; as cells lose their original identity, they can rapidly form teratomas (tumors) 9.
The vital breakthrough for longevity medicine is partial epigenetic reprogramming. By delivering a modified cocktail (usually OSK, omitting the oncogenic c-Myc factor) for a strictly limited duration, scientists can reset the epigenetic code - the chemical marks that dictate how DNA is turned on and off - to a more youthful state 28930. This restores youthful cellular function and resilience without forcing the cell to lose its original identity 28930.
2026: The First Human Trials
As of 2026, partial reprogramming has moved firmly from the realm of science fiction into serious biomedical inquiry, backed by unprecedented capital. Companies like Altos Labs launched with a record-breaking $3 billion to map cellular resilience, while Retro Biosciences secured $180 million from prominent tech investors to push reprogramming therapies toward the clinic 28931.
The most immediate and concrete proof-of-concept is currently playing out in ophthalmology. Life Biosciences recently received FDA clearance to begin the first-ever human clinical trial of a cellular reprogramming technology 930. The trial utilizes an AAV viral vector gene therapy to deliver OSK factors to retinal ganglion cells, aiming to treat age-related vision loss caused by open-angle glaucoma and non-arteritic anterior ischemic optic neuropathy (NAION) 93031. Crucially, the therapy, ER-100, is activated systemically by a safety switch: an oral dose of the antibiotic doxycycline. When patients take the pill, the gene therapy turns on; when they stop, it turns off, allowing for a precise eight-week reprogramming window 930. Preclinical data in non-human primates demonstrated that ER-100 successfully restored broken epigenomes and improved electrical signals in the optic nerve without causing tumors 931.
Simultaneously, competitors are exploring alternate delivery mechanisms. Turn Biotechnologies is utilizing mRNA delivery - similar to the technology used in COVID-19 vaccines - to deliver reprogramming factors for skin rejuvenation and osteoarthritis 31. This approach is technically safer than viral vectors because mRNA is temporary and does not permanently integrate into or alter the patient's DNA, allowing the therapy to be dosed like a traditional drug 31.
While whole-body, systemic cellular rejuvenation remains highly unlikely in the near term due to safety concerns, by 2040, the localized cellular rejuvenation of specific organs (e.g., the optic nerve, skin tissue, or ex-vivo organs treated on a machine prior to transplant) may become a routine reality 931.
Scenario 5: Precision mTOR Inhibition (Rapamycin) Proves Safe
Rapamycin, originally discovered in the soil of Easter Island (Rapa Nui) and developed as an immunosuppressant for organ transplant patients, has become one of the most rigorously studied and debated compounds in the longevity field 3233.
Rapamycin functions by inhibiting the mTOR (mechanistic target of rapamycin) pathway, a central biological regulator of cellular growth, protein synthesis, and metabolism 323334. When mTOR is chronically activated - as it tends to be in modern, high-calorie lifestyles - cellular senescence accelerates, and autophagy (the body's internal cellular cleanup and recycling system) declines, leading to metabolic dysfunction 32. Conversely, intermittent mTOR inhibition triggers a protective, stress-resistant cellular state. In animal models, rapamycin acts as a calorie restriction mimetic, consistently yielding a 10% to 25% extension in lifespan across multiple species 3234.
Translating these results to humans has historically been constrained by fears of immunosuppression and metabolic dysregulation, side effects well-documented in transplant patients taking high, daily doses of the drug 3234. However, clinical data maturing in 2026 is presenting a clearer picture of how low, intermittent dosing can capture the anti-aging benefits while mitigating the risks.
The PEARL Trial and Evolving Off-Label Data
The crowdfunded PEARL (Participatory Evaluation of Aging with Rapamycin for Longevity) trial, which tracked 114 relatively healthy participants over 48 weeks, published its findings revealing that weekly rapamycin administration (at 5mg and 10mg doses) was generally safe, with adverse events mirroring the placebo group 323335. While the efficacy results were mixed - women in the higher-dose group experienced significant improvements in lean muscle mass and reduced self-reported pain, while broad physical function metrics for the overall cohort remained largely unchanged - the trial provided the crucial baseline safety data the field required 33.
Simultaneously, a landmark 2026 observational study from the Mayo Clinic tracking 1,200 older adults using off-label low-dose rapamycin revealed a 23% reduction in all-cause mortality over a four-year follow-up period compared to age-matched controls 32. While observational data cannot prove causation, the signal strongly correlates with preclinical models.
As dose-finding studies continue to establish the exact pharmacokinetics required to hit biological targets without triggering immunosuppression, by 2040, precision mTOR inhibitors (rapalogs) are likely to be standard prophylactic treatments utilized to preserve metabolic and immune resilience in middle-aged populations 343536.
Summary of Major Longevity Avenues in Clinical Development
| Therapeutic Avenue | Primary Mechanism of Action | Lead Focus / Prominent Candidates | Clinical Status (as of 2026) |
|---|---|---|---|
| AI Drug Discovery | Computational modeling to identify novel biological targets and design optimal molecules. | Insilico Medicine, Gero, Chai Discovery | 173+ programs in trials; heavy weighting in Phase I with unprecedented 80-90% success rates 911. |
| Metabolic Repurposing | Modulating nutrient sensing, mitochondrial function, and systemic inflammation. | GLP-1 RAs (Semaglutide), Biguanides (Metformin) | Widely approved for specific diseases; massive TAME and VITAL-H trials underway for broad aging metrics 14720. |
| Targeted Senolytics | Selectively disabling pro-survival networks to induce apoptosis in toxic, pro-inflammatory senescent cells. | Dasatinib + Quercetin (D+Q), Fisetin | 45+ active trials; human proof-of-biology established in targeted diseases like IPF and kidney disease 82526. |
| Cellular Reprogramming | Delivering transcription factors to reset the epigenome to a youthful state without inducing pluripotency. | OSK gene therapy, mRNA delivery (Life Biosciences, Turn Bio) | First-in-human Phase I trials beginning; initial focus strictly on localized tissue like the optic nerve and skin 93031. |
| Precision mTOR Inhibition | Downregulating the mTOR pathway to trigger autophagy, mimicking the effects of calorie restriction. | Rapamycin (Sirolimus), Everolimus | Proven generally safe in healthy adults at intermittent low doses; widespread off-label use while academic trials refine optimal dosing 323334. |
The Demographic Reality: Why We Need Healthspan by 2040
As these five scientific scenarios mature, their inevitable collision with global demographic realities by 2040 will trigger profound socioeconomic consequences. The global population is aging at a historic and accelerating rate, driven by a global decline in fertility and historical improvements in medicine.
The proportion of the global population aged over 60 is expected to rise from roughly 14% today to 20% by 2050 13. In the European Union, the shift is even more dramatic, with estimates suggesting that nearly 30% of the population will be aged 65 and over by mid-century 3738. According to the United Nations Population Division, while global life expectancy at birth has risen to 71 years globally, developed regions are projected to see life expectancy approach 90 years by 2100 10.
Global life expectancy rankings will also shift dramatically over the next two decades. According to comprehensive analyses of demographic trends published in The Lancet by the Institute for Health Metrics and Evaluation, Spain is projected to overtake Japan for the highest life expectancy in the world by 2040, driven largely by the benefits of the Mediterranean diet and robust healthcare systems 40414243.
| Country | 2016 Global Rank | 2016 Average Life Expectancy | 2040 Projected Rank | 2040 Projected Life Expectancy |
|---|---|---|---|---|
| Spain | 4th | 82.9 years | 1st | 85.8 years 4142 |
| Japan | 1st | 83.7 years | 2nd | 85.7 years 4142 |
| Singapore | 3rd | 83.3 years | 3rd | 85.4 years 42 |
| China | 68th | 76.3 years | 39th | 81.9 years 4142 |
| United States | 43rd | 78.7 years | 64th | 79.8 years 4142 |
Japan serves as the leading indicator for the demographic crises awaiting the developed world. The country is facing a severe "2040 Problem." By 2040, members of Japan's second baby boom (the "employment ice age" generation) will reach age 65, pushing the senior population past 35% 4445. Furthermore, government projections indicate that by 2040, 25% of women and 21% of men over sixty-five in Japan will be living completely alone - a population roughly equivalent to the entire country of Austria 44. This inverted population pyramid severely strains the tax base, escalates healthcare costs, and results in acute labor shortages, forcing Japan to heavily invest in automation, robotics, and advanced biotech to maintain its economy 44.
Economic Ripple Effects on Pensions and Retirement
Living longer is inherently more expensive. The traditional societal model designed in the mid-20th century - working until age 65 and retiring for a brief 5 to 10 years - is structurally collapsing as populations are forced to fund retirements lasting 25 to 30 years 1147.
The old-age dependency ratio - the number of people of pensionable age for every 1,000 working-age people - is soaring. In the UK, it is projected to increase from 280 in 2020 to 341 by 2045, meaning every 1,000 workers will be supporting significantly more retirees 48. To remain solvent, public pay-as-you-go pension systems face the immediate risk of insolvency without significant, often unpopular reform 11. To combat this, retirement ages are inevitably being pushed higher; the Centre for Future Studies forecasts the UK state pension age may reach 69 by 2041, forcing Millennials and Generation Z to severely adjust their retirement aspirations 48.
The financial burden is immense. An extension of retirement by just two years requires single retirees in the UK to save an estimated additional £67,200 for a comfortable lifestyle 48. This places an unprecedented strain on the "sandwich generation," who find themselves financially supporting both their children and their aging parents simultaneously 48.
Consequently, longevity technologies that improve healthspan are not merely medical luxuries - they are macroeconomic necessities. If therapies can delay the onset of frailty, Alzheimer's, and cardiovascular disease, older adults can remain in the workforce longer, maintaining their independence and mitigating the crushing fiscal strain on shrinking tax bases and overwhelmed long-term care facilities 3812.
Global Equity and the Threat of "Longevity Apartheid"
The most pressing ethical concern regarding longevity breakthroughs in 2040 is equitable access. The global wellness economy has ballooned to over $6 trillion, with the longevity-focused market forecast to reach over $610 billion 50. However, the distribution of these technologies and the capital funding them is heavily skewed.
Current investment patterns indicate a severe geographic and socioeconomic concentration. Approximately 70% of global longevity investment is concentrated in wealthy countries possessing advanced capital infrastructure, despite these nations housing only 16.9% of the global elderly population 51. If unregulated, the translation of advanced interventions - such as personalized gene therapies and specialized senolytics - could create a system of "longevity apartheid," where biological age and healthspan become the ultimate markers of global socioeconomic stratification 51.
Pricing and Regulatory Friction
The cost of these therapeutics remains a massive friction point. Even repurposed drugs like GLP-1 agonists carry massive price tags that threaten the sustainability of health insurance systems. While the U.S. government negotiated Medicare caps of $245 per month (with a $50 patient copay) for specific indications starting in 2026, cash-pay patients using direct-to-consumer platforms still face costs of roughly $350 to $500 per month, and commercial insurance rates remain high 525313. The sheer popularity of these drugs is already driving up the cost of health insurance premiums across the board, forcing intense debates regarding cost-effectiveness and broad societal scaling 1355.
Furthermore, regulatory environments will deeply influence market access and equitable distribution. For instance, the FDA's regulatory back-and-forth regarding NMN (Nicotinamide mononucleotide, a popular NAD+ boosting supplement) highlights the chaos of longevity regulation. The FDA excluded NMN from being classified as a dietary supplement in 2022 due to prior drug investigations, only to reverse its stance and reinstate its New Dietary Ingredient (NDI) status in December 2025 following fierce industry lawsuits 561458. However, while legal in the US, NMN remains heavily restricted under Novel Food rules in Europe, creating a stark regulatory divide 56.
Without aggressive public-private partnerships, tiered international pricing models, scaled manufacturing, and a continued focus on the foundational social determinants of health (SDOH) - such as nutrition, clean air, and housing - the longevity breakthroughs of 2040 may remain confined to wealthy enclaves. This would only serve to widen the staggering 19-year gap in life expectancy that already exists between high- and low-income countries today 51156061.
Bottom line
By 2040, the pursuit of human longevity will definitively transition from generalized life extension to precise, AI-accelerated therapies aimed at compressing morbidity and extending healthspan. Breakthroughs in metabolic drug repurposing (GLP-1s, metformin), targeted senolytics, precise mTOR inhibition, and partial cellular reprogramming will provide clinicians with a robust, regulated toolkit to manage and delay biological aging. However, it remains highly uncertain whether global healthcare systems and fragmented regulatory bodies can equitably distribute these advanced, often expensive therapies to prevent a deep socioeconomic divide in healthy life expectancy.