Effects of breathwork on the nervous system
Introduction to Respiratory Neurophysiology
The voluntary manipulation of respiration - broadly categorized as breathwork - has transitioned from traditional esoteric practices into a subject of rigorous neurophysiological inquiry. While traditional modalities such as yogic Pranayama and Chinese Qigong have utilized breath control for millennia, contemporary clinical research has begun to isolate the specific mechanical, chemical, and neural pathways through which these practices influence the human nervous system 12. The integration of these techniques into clinical psychiatry, sports performance, and stress management has been accompanied by a surge of commercial interest, often leading to the conflation of established physiological mechanisms with pseudoscientific health claims.
The primary objective of current research is to separate empirical autonomic nervous system adaptations from the wellness theater that frequently surrounds the discipline. Respiration is unique among autonomic functions in that it is under dual control; it is governed involuntarily by brainstem pacemakers in the medulla oblongata to maintain blood gas homeostasis, yet it can be voluntarily overridden by the motor cortex 34. This conscious override provides a direct, accessible portal to modulate the autonomic nervous system, the hypothalamic-pituitary-adrenal axis, and central neurotransmitter concentrations.
To evaluate the efficacy of breathwork, it is necessary to examine the diverse methodologies employed - ranging from slow-paced diaphragmatic breathing to high-ventilation breath retention - and assess their respective impacts on cardiovascular hemodynamics, neurochemistry, and psychometric outcomes. Furthermore, a critical appraisal of the clinical trial data is required to identify the limits of these interventions, particularly concerning expectancy bias, methodological flaws, and the biological implausibility of certain commercial claims.
Autonomic Modulation and Cardiorespiratory Coupling
The foundation of breathwork's physiological efficacy lies in its ability to influence the autonomic nervous system through mechanical and neural feedback loops. The dynamic interplay between respiratory patterns and cardiovascular function is known as cardiorespiratory coupling, a process primarily mediated by the vagus nerve.
Vagal Tone and Respiratory Sinus Arrhythmia
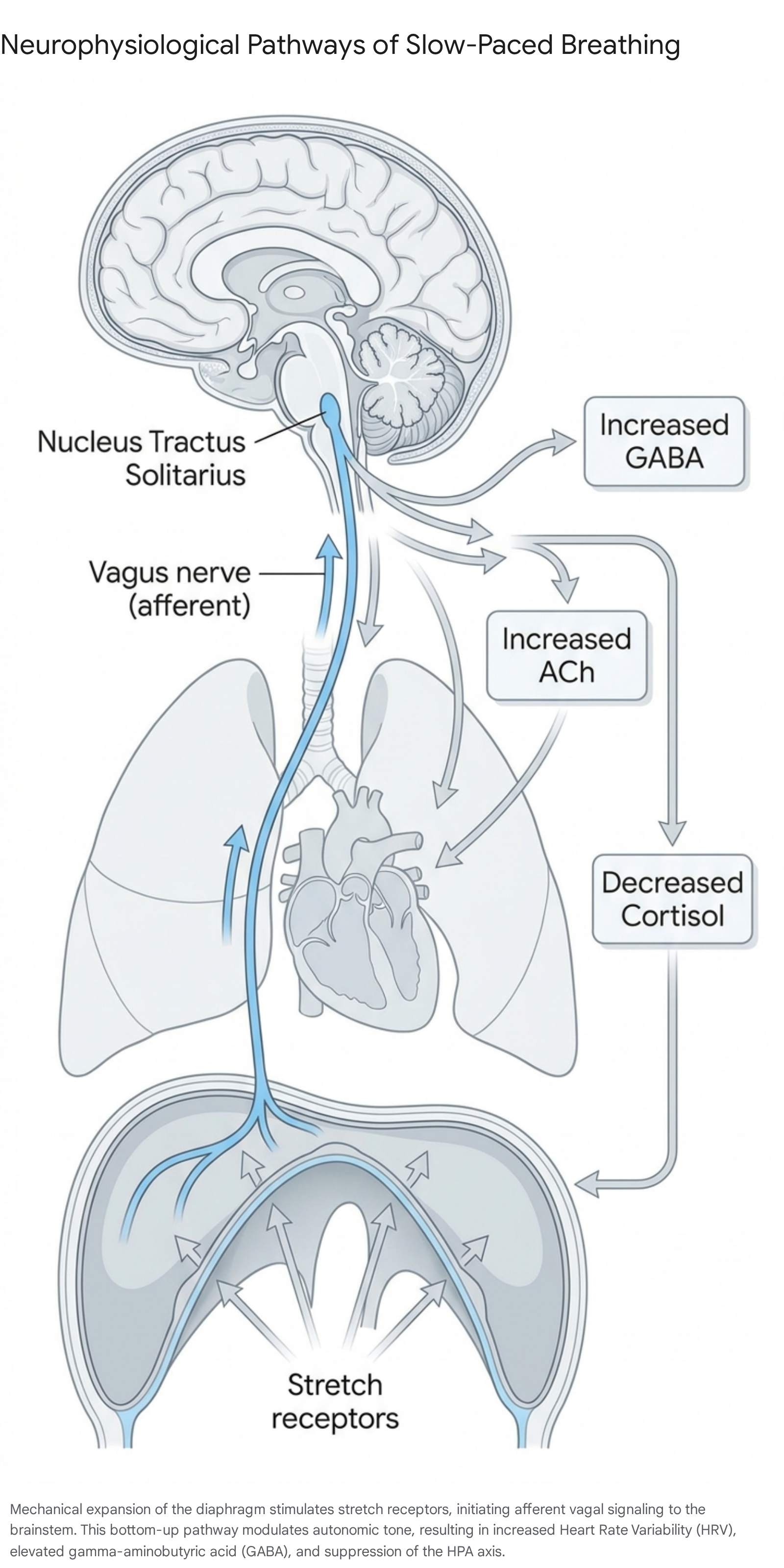
The vagus nerve, the tenth cranial nerve, serves as the primary conduit of the parasympathetic nervous system, extending from the brainstem to the visceral organs, including the heart, lungs, and digestive tract 4. Approximately 80% of vagal fibers are afferent, meaning they transmit sensory information from the body to the brain 5. Slow, diaphragmatic breathing capitalizes on this afferent pathway. As the diaphragm descends during a deep inhalation, pulmonary stretch receptors are activated. This mechanical expansion sends signals via the vagus nerve to the nucleus tractus solitarius in the brainstem, which subsequently relays information to higher-order cortical structures, including the prefrontal cortex and the amygdala 46.
A critical biomarker of this vagal modulation is Respiratory Sinus Arrhythmia, a phenomenon where the heart rate naturally fluctuates in synchrony with the respiratory cycle 37. During inhalation, parasympathetic influence is momentarily inhibited, leading to a slight increase in heart rate to optimize pulmonary blood flow. During exhalation, vagal efferent activity resumes, releasing acetylcholine at the sinoatrial node and slowing the heart rate 3.
Slow-paced breathwork techniques, particularly those practiced at a resonance frequency of approximately 5.5 to 6 breaths per minute, deliberately amplify Respiratory Sinus Arrhythmia. By extending the exhalation phase, practitioners maximize the duration of vagal dominance 8910. This sustained parasympathetic activation increases heart rate variability - specifically the high-frequency domain and time-domain indices such as the standard deviation of normal-to-normal intervals (SDNN) and the root mean square of successive differences (RMSSD) 311. Elevated heart rate variability is a widely accepted indicator of autonomic flexibility, cardiovascular health, and emotional resilience, contrasting sharply with the low variability typically observed in states of chronic stress, anxiety, and allostatic load 312.
The Chemistry of Respiration and the Bohr Effect
While the mechanical stretching of the diaphragm influences neural pathways, the chemical alterations in blood gases - specifically carbon dioxide (CO2) - exert profound effects on hemodynamics and tissue oxygenation. In popular wellness contexts, carbon dioxide is often misunderstood merely as a metabolic waste product to be expelled. However, in respiratory physiology, it acts as a critical metabolic regulator that dictates vascular tone and oxygen delivery 13.
The relationship between carbon dioxide and oxygen delivery is governed by the Bohr effect, a physiological principle stating that the affinity of hemoglobin for oxygen is inversely related to the concentration of carbon dioxide and blood acidity 1415. In individuals experiencing chronic stress or anxiety, a common physiological response is sub-clinical hyperventilation, or overbreathing. This chronic shallow, rapid breathing leads to hypocapnia, a condition characterized by depressed arterial carbon dioxide levels. According to the Bohr effect, when carbon dioxide levels fall, hemoglobin binds more tightly to oxygen, impairing its release into tissues and organs, including the brain 16. This localized cerebral hypoxia can induce feelings of dizziness, fatigue, and heightened anxiety, creating a negative feedback loop that perpetuates rapid breathing 916.
Specific breathwork techniques focus on improving carbon dioxide tolerance - the body's ability to withstand rising partial pressures of the gas without triggering a panic response or a reflexive urge to hyperventilate. Practices involving breath holds or prolonged, slow exhalations intentionally allow carbon dioxide to accumulate 9. Over time, these practices reset the chemoreceptors in the brainstem, which dictate the respiratory drive, to tolerate higher baseline levels 13. Enhanced carbon dioxide tolerance promotes vasodilation, optimal cerebral blood flow, and more efficient cellular oxygenation, which correlates with reduced baseline sympathetic arousal and improved cognitive focus under stress 1516.
Neurochemical and Endocrine Modulations
The modulation of the autonomic nervous system via slow-paced breathing generates cascading effects throughout the central nervous system and endocrine system. Clinical research has documented specific neurochemical alterations that occur during and after regulated breathwork practices, directly linking respiratory mechanics to emotional regulation and systemic health.
Gamma-Aminobutyric Acid and Cortical Inhibition
Slow-paced breathing has been repeatedly associated with shifts in central neurotransmitter concentrations. Of primary interest is the up-regulation of gamma-aminobutyric acid (GABA), the brain's principal inhibitory neurotransmitter. GABA is critical for dampening excessive neural excitability, particularly within the amygdala, the region associated with fear and threat detection 610. Magnetic resonance spectroscopy studies have demonstrated that mind-body interventions incorporating coherent breathing result in significant increases in thalamic GABA levels, which correlate directly with reductions in depressive symptoms 5. By increasing the inhibitory capacity of the medial prefrontal cortex over the amygdala, slow-paced breathing enhances the organism's capacity for emotional self-regulation and stress resilience 6.
Clinical trials evaluating major depressive disorder have utilized dose-finding models to measure this effect, randomizing patients to varying volumes of breath-focused mind-body programs. Findings consistently link the volume of breathwork to the magnitude of thalamic GABA increases, subsequently leading to decreased symptom severity 5. This neurochemical shift explains why respiratory interventions are highly effective in halting the runaway neural firing associated with panic and acute anxiety.
The Cholinergic Anti-Inflammatory Pathway
Simultaneously, vagal efferent activation drives the cholinergic anti-inflammatory pathway. Acetylcholine released from vagal nerve endings binds to alpha-7 nicotinic acetylcholine receptors on tissue macrophages. This binding inhibits the phosphorylation of the NF-κB signaling pathway, thereby suppressing the production of pro-inflammatory cytokines such as tumor necrosis factor-alpha and interleukin-6 1718.
This neuro-immune link suggests that regular breathwork practice not only addresses psychological distress but also mitigates systemic inflammation, a recognized co-factor in various psychiatric, autoimmune, and metabolic disorders. Clinical research demonstrates that decreases in these inflammatory factors are directly related to improvements in chronic fatigue and respiratory efficiency 17. The ability of voluntary breathing to interface with the immune system represents a significant intersection between conscious behavior and subconscious physiological defense mechanisms.
Nitric Oxide Production and Vascular Dynamics
Nasal breathing, particularly when combined with specific vocalizations or resistance, actively modulates nitric oxide production. Nitric oxide is a potent vasodilator produced by the paranasal sinuses. When air is inhaled through the nose, it is infused with nitric oxide before entering the lower respiratory tract, enhancing pulmonary oxygen uptake and facilitating systemic vasodilation 918.
Certain breathwork techniques drastically amplify this effect. For instance, the yogic practice of Bhramari pranayama - which involves a low-pitched humming sound during exhalation - causes vibrations in the nasal and laryngeal mucous membranes. Studies demonstrate that this humming can increase the production of free nitric oxide by up to 15-fold at rest 1819. The infusion of this molecule into the bloodstream modulates neurotransmitters like norepinephrine and serotonin while inducing significant drops in both systolic and diastolic blood pressure 1820. The subsequent vasodilation reduces the mechanical workload on the heart, making such practices highly relevant for hypertensive patients 21.
Hypothalamic-Pituitary-Adrenal Axis Regulation
In addition to neurotransmitter and immune modulation, slow-paced breathing interventions effectively down-regulate the hypothalamic-pituitary-adrenal axis, resulting in measurable decreases in salivary and serum cortisol levels 722. Chronic psychological stress causes the continuous release of corticotropin-releasing factor from the hypothalamus, leading to sustained glucocorticoid elevation. This continuous state of sympathetic readiness creates a heavy allostatic load, which damages tissue and impairs cognitive function over time 23.
By stimulating the vagus nerve and enhancing parasympathetic tone, breathwork minimizes the secretion of corticotropin-releasing factor, curtailing the downstream release of cortisol 2324. Regular practice has been shown to flatten the post-stress cortisol spike, accelerating the body's return to homeostasis 25. This endocrine regulation is a primary mechanism behind the consistent clinical findings that breathwork reduces perceived stress and mitigates the physiological wear-and-tear associated with modern environmental and psychological pressures.
Clinical Methodologies of Regulated Respiration
While the umbrella term "breathwork" implies a monolithic practice, specific techniques yield distinct physiological profiles. The landscape of respiratory interventions encompasses both ancient traditional practices and modern, clinically optimized protocols. Table 1 summarizes the mechanisms and evidence associated with widely practiced slow-paced modalities.
| Breathing Modality | Description and Technique | Primary Physiological Mechanism | Documented Clinical Outcomes |
|---|---|---|---|
| Coherent Breathing | Rhythmic breathing at a resonance frequency, typically 5.5 to 6 breaths per minute 322. | Maximizes Respiratory Sinus Arrhythmia; balances sympathovagal tone 326. | Increases HRV; significant reductions in baseline stress, depression, and anxiety 325. |
| Ujjayi Pranayama | Slow breathing with mild glottal constriction, creating airway resistance 226. | Increases intrathoracic pressure; stimulates carotid baroreceptors; enhances vagal tone 2627. | Significant reductions in perceived stress, tension, and heart rate; increases in subjective peacefulness 2628. |
| Bhramari Pranayama | Prolonged exhalation accompanied by a low-pitched humming sound 1419. | 15-fold increase in paranasal nitric oxide production; vagal stimulation via auricular branch 1819. | Pronounced reduction in blood pressure and cardiovascular hyper-reactivity; improved auditory reaction time 1920. |
| Nadi Shodhana | Alternate nostril breathing; inhaling and exhaling through one nostril at a time 230. | Modulates hemispheric dominance; slows respiratory rate; normalizes sympathovagal balance 2030. | Improvements in spatial memory, reductions in systolic and diastolic blood pressure 2029. |
| Box Breathing | Equal duration for inhalation, breath hold, exhalation, and post-exhalation hold (e.g., 4 seconds each) 3031. | Carbon dioxide tolerance accumulation during apnea phases; steady regulation of the respiratory pacemaker 1631. | Reductions in physiological arousal, lowered respiratory rate, enhanced focus, utility in tactical environments 93031. |
| 4-7-8 Breathing | Inhale for 4 seconds, hold for 7 seconds, exhale for 8 seconds 3233. | Extended exhalation maximizes vagal efferent activity; breath hold builds mild carbon dioxide tolerance 3233. | Rapid reduction in state anxiety, heart rate variability improvement, utility as a sleep aid 3233. |
High-Ventilation Breathwork and Hormetic Stress
In contrast to slow-paced modalities designed to up-regulate parasympathetic activity, high-ventilation breathwork with retention (HVBR) - popularized commercially as the Wim Hof Method and historically rooted in Tibetan Tummo - utilizes rapid overbreathing followed by voluntary breath holds at low lung volumes 3435. The physiological framework for this practice differs fundamentally from slow-paced breathing, operating on the principle of hormesis: the application of a brief, intense, and controlled stressor to provoke an adaptive, resilient response from the organism.
Acute Respiratory Alkalosis and Immune Responses
Rapid, deep hyperventilation drastically alters blood gas concentrations, expelling large volumes of carbon dioxide and inducing hypocapnia 3536. This rapid depletion of carbon dioxide disrupts the acid-base balance of the blood, resulting in acute respiratory alkalosis - a transient state in which the blood pH becomes abnormally alkaline 3637.
This extreme physiological shift triggers a robust sympathetic nervous system response. A landmark 2014 study by Kox et al. investigated the effects of this technique by injecting practitioners with an endotoxin (E. coli). The results demonstrated that the breathing intervention provoked a massive release of endogenous epinephrine, which subsequently modulated the innate immune response 3841. Participants utilizing the high-ventilation technique exhibited an increase in the anti-inflammatory cytokine interleukin-10 and a marked reduction in pro-inflammatory markers such as tumor necrosis factor-alpha, interleukin-6, and interleukin-8 3438. Additionally, the epinephrine surge caused leukocytosis, an acute increase in circulating white blood cells 3738.
These findings confirm that voluntary, high-intensity breathwork can directly interface with the sympathetic nervous system and exert top-down control over inflammatory pathways. This mechanism suggests potential, though highly specific, therapeutic applications for conditions characterized by excessive inflammation, provided the intervention is administered safely to avoid hyperventilation-induced syncope.
Efficacy Constraints in Randomized Controlled Trials
Despite the profound acute physiological changes induced by high-ventilation breathwork, clinical evidence regarding its long-term efficacy for mental health remains deeply contested. The intense sympathetic arousal provoked by the practice has raised questions regarding its suitability as a generalized, daily intervention for stress and anxiety.
A robust 2024 blinded, randomized controlled trial (NCT06064474) conducted by Fincham et al. provided critical insights into the psychological effects of high-ventilation breathwork 394041. The trial allocated 200 healthy adults to either a 3-week daily protocol of remote high-ventilation breathwork or an active placebo comparator consisting of paced breathing at 15 breaths per minute, a rate considered physiologically neutral 3942. To control for expectancy bias, the trial was concealed as a "fast breathwork" study, and participants in both groups reported equal levels of intervention credibility and expectancy of benefit 3941.
The results of the trial revealed a significant main effect of time (F = 13.0, p < 0.01), meaning both groups experienced reductions in subjective stress pre-to-post intervention. However, there was no significant group-by-time interaction (F(1,180) = 1.98, p = 0.16) and no main effect of group (F = 0.35, p = 0.55) 3940. Secondary outcomes for trait anxiety, depression, positive and negative affect, and sleep impairment mirrored this null finding, with no significant differences observed between the hyperventilation group and the neutral breathing group 3940.
These data indicate that brief, remote high-ventilation breathwork is not more efficacious at improving mental health outcomes than a well-designed, neutral breathing comparator 4041. The improvements observed in the intervention group were likely attributable to the placebo effect, the pause in daily routine, or non-specific behavioral factors rather than the specific physiological stress of hyperventilation. Consequently, while the technique reliably produces acute biochemical alterations, its superiority as a daily psychiatric intervention over milder forms of breathing is not supported by current rigorous evidence.
Evidence in Specific Clinical Populations
The clinical utility of breathwork extends beyond general stress reduction into the targeted management of specific psychiatric, cardiopulmonary, and musculoskeletal disorders. Evaluating the literature reveals varied effect sizes and distinct applications across disease states.
Psychiatric and Neurological Disorders
A comprehensive 2023 meta-analysis assessing the effect of breathwork on self-reported stress, anxiety, and depression yielded significant small-to-medium effect sizes favoring breathwork over non-breathwork control conditions (Hedges' g ranging from -0.32 to -0.40, p < 0.001) 25. Similarly, systematic reviews of traditional Indian breathwork (Pranayama) applied to patients with diagnosed mental disorders - including major depressive disorder, generalized anxiety disorder, and PTSD - found that the interventions significantly reduced post-intervention symptom severity compared to passive controls, with an overall standardized mean difference (SMD) of -0.27 in intention-to-treat samples and -0.35 in per-protocol samples 4344.
In adolescent populations, the impact appears even more pronounced. A 2025 systematic review and meta-analysis of 18 studies examining Pranayama's effectiveness on adolescent stress and anxiety reported a moderate-to-large effect size (SMD = -1.166) 4546. However, researchers noted that the certainty of this evidence remains very low due to serious concerns regarding the risk of bias, inconsistency, and methodological imprecision across the included trials 45.
Cardiopulmonary Disorders
Given the direct mechanical involvement of the respiratory system, breathwork is heavily researched in the context of cardiopulmonary rehabilitation. For patients with chronic obstructive pulmonary disease (COPD), specific patterns are utilized to manage dyspnea and improve exercise tolerance. Network meta-analyses of mind-body exercises indicate that practices incorporating controlled respiration, such as Qigong, are highly effective in reducing disease impact. Qigong was identified as the most effective exercise intervention for improving scores on the St. George's Respiratory Questionnaire, a validated tool for assessing health-related quality of life in COPD patients 17. Additionally, box breathing interventions have been shown to be 99.2% effective in normalizing breathing frequency in COPD patients, although they do not significantly alter resting oxygen saturation 31.
In the management of asthma, the Buteyko breathing technique is uniquely targeted. Asthma attacks are frequently exacerbated by hyperventilation, which depletes carbon dioxide and causes bronchoconstriction. The Buteyko method focuses on reducing tidal volume and respiratory rate to prevent overbreathing and normalize carbon dioxide levels 3347. Clinical studies indicate that patients practicing this technique achieve better control over their asthma symptoms and significantly reduce their reliance on inhaled corticosteroid therapy and bronchodilators, highlighting the clinical relevance of carbon dioxide tolerance training 47.
Musculoskeletal and Pain Syndromes
The intersection of autonomic regulation and pain perception has led to the adoption of breath-centric mind-body exercises for chronic pain management. A network meta-analysis of interventions for chronic non-specific neck pain (CNNP) demonstrated that practices like Qigong, Yoga, and Tai Chi significantly reduced functional disability, as measured by the Neck Disability Index, and lowered pain intensity on the Visual Analog Scale 4849.
Functional near-infrared spectroscopy studies examining these interventions reveal that structured breath and movement exercises enhance resting-state functional connectivity in the prefrontal cortex while decreasing activation in the visual cortex 49. This neuroplastic shift suggests that breathing practices modulate the top-down executive perception of pain. Furthermore, by down-regulating the sympathetic nervous system, these practices decrease systemic muscle tension, providing mechanical relief to cervical and lumbar musculoskeletal structures 2349.
Methodological Challenges in Breathwork Research
To accurately evaluate the literature surrounding breathwork, researchers must acknowledge the widespread methodological vulnerabilities within mind-body intervention trials. A primary structural issue is the inherent impossibility of blinding participants to a breathing intervention 485051. Because subjects are actively and consciously altering their respiration, they are acutely aware that they are receiving an active treatment.
When trials employ passive comparators - such as wait-list controls or standard care - the intervention group becomes highly susceptible to expectancy bias 4850. Participants entering a breathwork trial frequently carry preconceived beliefs about the efficacy of the practice, influenced by cultural narratives and pervasive media coverage 5253. This expectation can artificially inflate subjective, self-reported outcomes regarding pain, stress, and mood 4853. Open-label trials attempt to mitigate this by informing participants that both the active intervention and the comparator are evidence-based approaches, but the psychological bias often remains 51.
Furthermore, bias assessments using the Cochrane RoB 2.0 tool frequently identify moderate-to-high risks of bias in respiratory trials. The most common domains flagged for concern include deviations from intended interventions and bias in the measurement of the outcome, particularly when outcomes are exclusively reliant on self-reported psychometric questionnaires 434852. Recent systematic reviews utilizing the GRADE framework have concluded that the certainty of evidence for many respiratory interventions remains low to very low due to small sample sizes, high heterogeneity among trial designs, and inconsistent adherence tracking 4546.
To produce reliable data, future research must prioritize active, structurally equivalent placebos, mirror the rigorous design of the Fincham high-ventilation trial, and increasingly rely on objective physiological markers such as continuous ambulatory heart rate variability tracking, salivary cortisol assays, and neuroimaging to bypass the limitations of subjective self-reporting 73950.
Critical Appraisal of Wellness Industry Claims
The proliferation of breathwork in the commercial wellness industry has resulted in the aggressive marketing of techniques utilizing pseudoscientific rationales. Establishing the credibility of respiratory interventions requires a strict demarcation between empirical neurophysiology and wellness theater.
The Blood Alkalization Fallacy
A pervasive and biologically dangerous claim within certain segments of the wellness industry is that high-ventilation breathwork permanently alkalizes the blood, and that this alkaline state can cure diseases, neutralize toxins, and prevent cancer 545556. These assertions are rooted in long-debunked theories which posit that systemic acidity is the root cause of chronic illness and that dietary or respiratory interventions can permanently shift the body's pH to a therapeutic alkaline state 5560.
From a physiological standpoint, these claims are fundamentally flawed. The human body tightly regulates arterial blood pH within a narrow homeostatic range of 7.35 to 7.45; deviations beyond this range result in severe cellular dysfunction, protein denaturation, and potentially fatal consequences 3755. While it is true that hyperventilation causes acute respiratory alkalosis by rapidly offloading carbon dioxide, this state is strictly temporary and represents a deviation from, rather than an optimization of, homeostasis.
In response to respiratory alkalosis, the body immediately engages compensatory mechanisms. The kidneys decrease the excretion of hydrogen ions and increase the excretion of bicarbonate to pull the blood pH back down to the baseline 37. The highly alkaline urine occasionally observed by practitioners of hyperventilation techniques is merely evidence of normal renal compensation attempting to fix the acute imbalance, not an indication that the body's internal environment has been permanently upgraded 37. Claiming that breathwork can durably alter blood pH to cure disease demonstrates a profound misunderstanding of basic homeostatic mechanisms and crosses firmly into the territory of wellness theater 3755.
Commercialization and Contextual Efficacy
Further examples of wellness theater involve the hyper-commercialization of autonomic regulation. For example, consumer products such as functional fragrance mists are currently marketed to pair with specific micro-breathwork routines, claiming to provide rapid "nervous system infrastructure" 57. These products often cite the presence of compounds like linalool or cedrol, asserting that inhaling them alongside a vagal breath will directly modulate GABA receptors or lower cortisol at the source 57.
While it is true that olfactory receptors communicate with the limbic system, the aggressive packaging of these biological mechanisms as necessary consumer products exaggerates the clinical magnitude of the effect 57. The physiological reality is that breathwork alone, driven by mechanical diaphragmatic stretching and the manipulation of blood gases, is entirely sufficient to achieve the desired autonomic modulation. The addition of branded accessories or branded frameworks often serves to commodify a biological mechanism that is inherently free and autonomous.
Conclusion
The scientific investigation of breathwork reveals a robust physiological framework that substantiates its efficacy as an autonomic regulatory tool. The evidence overwhelmingly supports the utility of slow-paced, diaphragmatic breathing interventions. By leveraging cardiorespiratory coupling and the vagal afferent network, these practices reliably modulate heart rate variability, increase central GABAergic inhibition, and down-regulate the hypothalamic-pituitary-adrenal axis. Such mechanisms provide a sound biological rationale for the clinical improvements observed in patients suffering from anxiety, depression, chronic pain, and cardiopulmonary dysregulation.
Conversely, while high-ventilation techniques effectively harness hormetic stress to induce acute immune modulation and sympathetic arousal, claims regarding their long-term psychiatric superiority remain unsubstantiated by rigorous placebo-controlled trials. The intense hyperventilation produces measurable biochemical shifts, but these do not consistently translate into superior relief from psychological distress when compared to neutral breathing patterns. Furthermore, the commercial assertions that breathwork can permanently alkalize the blood to eradicate disease are biologically invalid and represent a clear distortion of respiratory physiology.
Ultimately, the clinical utility of breathwork does not require pseudoscientific embellishment. The empirical reality - that the deliberate modulation of respiratory rate can directly alter central nervous system function, improve vascular dynamics, and restore autonomic balance - cements breathwork as a highly effective, evidence-based intervention in the landscape of integrative medicine.