What FDA Approval of Deramiocel Means for Duchenne Families
If approved by the FDA, deramiocel would become the first cell therapy to specifically target the heart failure and upper-limb decline associated with advanced Duchenne muscular dystrophy (DMD). For families and caregivers, this mutation-agnostic, quarterly intravenous infusion offers a novel way to preserve function for older, non-ambulatory patients. However, accessing the therapy will require navigating specialized care centers, significant out-of-pocket travel costs, and complex insurance prior authorization processes.
The Evolving Reality of Duchenne Muscular Dystrophy
Duchenne muscular dystrophy is a severe, progressive, and fatal neuromuscular disease 12. Caused by an X-linked genetic mutation, it is almost exclusive to males, occurring in approximately 1 in every 3,500 live male births 13. In the United States, an estimated 15,000 boys and young men are currently living with the disease 13.
The disorder is rooted in a mutation of the DMD gene, which prevents the body from producing functional dystrophin 14. Dystrophin is an essential structural protein that acts like a shock absorber for muscle cells 15. Without it, the normal mechanical stress of everyday movement causes microscopic tears in the muscle cell membranes.
The Cascade of Inflammation and Fibrosis
When muscle cells are continually injured, the body's immune system responds. In a healthy body, immune cells clear out damage and promote healing 46. In a body with Duchenne, the continuous lack of dystrophin leads to a relentless cycle of muscle breakdown 4. This triggers a chronic, aggressive inflammatory cascade 24.
Over time, the body is unable to keep up with the damage. Dead muscle cells are replaced by non-contractile fibrofatty scar tissue - a process known as fibrosis 14. This fibrotic scarring is what ultimately drives the progressive muscle dysfunction, motor function loss, and eventual organ failure that characterizes the disease 4.
Typically, boys with Duchenne are diagnosed between the ages of 3 and 5 3. The initial focus is on skeletal muscle weakness, which usually begins in the proximal muscles near the body's core before spreading to the extremities 7. As the disease advances, most patients lose the ability to walk independently and become reliant on power wheelchairs by their early teenage years 18.
The Hidden Crisis: Duchenne Cardiomyopathy
While much of the historical focus in Duchenne research has been on preserving walking ability, the landscape is shifting. Improvements in the standard of care - particularly the aggressive use of corticosteroids and advances in respiratory support - mean that patients are living longer 910.
However, this extended lifespan has brought a new challenge to the forefront: the heart is also a muscle, and it desperately relies on dystrophin 1011.
Because the heart never stops beating, it is highly susceptible to the same cycle of mechanical stress, injury, inflammation, and scarring that destroys skeletal muscles 4. Approximately 25% of patients with Duchenne will develop signs of cardiomyopathy (heart muscle disease) by the age of 6, and 59% will show signs by the age of 10 3. As scar tissue accumulates in the myocardium (the muscular wall of the heart), the heart becomes stiff and weak, forcing it to work increasingly harder to pump blood 110.
Eventually, this cardiomyopathy leads to heart failure. Today, heart failure is the leading cause of mortality among young men with Duchenne muscular dystrophy 1211.
Despite this reality, there are currently no FDA-approved therapies specifically designed to treat Duchenne cardiomyopathy 312. Traditional heart failure medications, such as ACE inhibitors and beta-blockers, are used off-label as the standard of care to manage symptoms, but they do not stop the underlying fibrotic destruction of the heart tissue 313. This is the precise clinical gap that deramiocel aims to fill.
What Is Deramiocel?
Deramiocel, also known in clinical literature as CAP-1002, is an investigational allogeneic cell therapy developed by Capricor Therapeutics 312. It is currently in late-stage regulatory review with the U.S. Food and Drug Administration (FDA) seeking full approval for the treatment of Duchenne muscular dystrophy 14.
Unlike gene therapies that attempt to deliver a functional version of the dystrophin gene, or exon-skipping drugs that try to patch the genetic code, deramiocel takes an entirely different approach. It does not alter the patient's DNA or attempt to replace the missing dystrophin protein 5. Instead, it aims to alter the body's devastating immune response to the muscle damage 416.
Cardiosphere-Derived Cells (CDCs)
The therapy consists of allogeneic cardiosphere-derived cells (CDCs). "Allogeneic" means that the cells are sourced from a healthy human donor, rather than harvested from the patient's own body 2317. CDCs are a rare, unique population of stromal cells isolated from transplant-qualified human heart tissue 615.
The technology was first discovered in 2007 by Dr. Eduardo Marbán at Johns Hopkins Hospital, where it was originally investigated as a potential regenerative therapy to heal the heart after a myocardial infarction (heart attack) 415. In those early clinical trials, researchers noted that CDCs were remarkably effective at reducing fibrotic scar size in infarcted hearts 4.
Recognizing that Duchenne cardiomyopathy is also driven by relentless scarring, researchers began testing CDCs in animal models of Duchenne, specifically the mdx mouse model, which mimics the disease's cardiac and skeletal dysfunction 4. The results showed that the cells improved global cardiac function and exercise capacity, leading to human clinical trials 415.
The Mechanism of Action: Exosomes and Macrophages
When deramiocel is administered into a patient's bloodstream, the CDCs do not permanently engraft, meaning they do not physically turn into new heart muscle 13. Instead, they act as microscopic pharmaceutical factories.
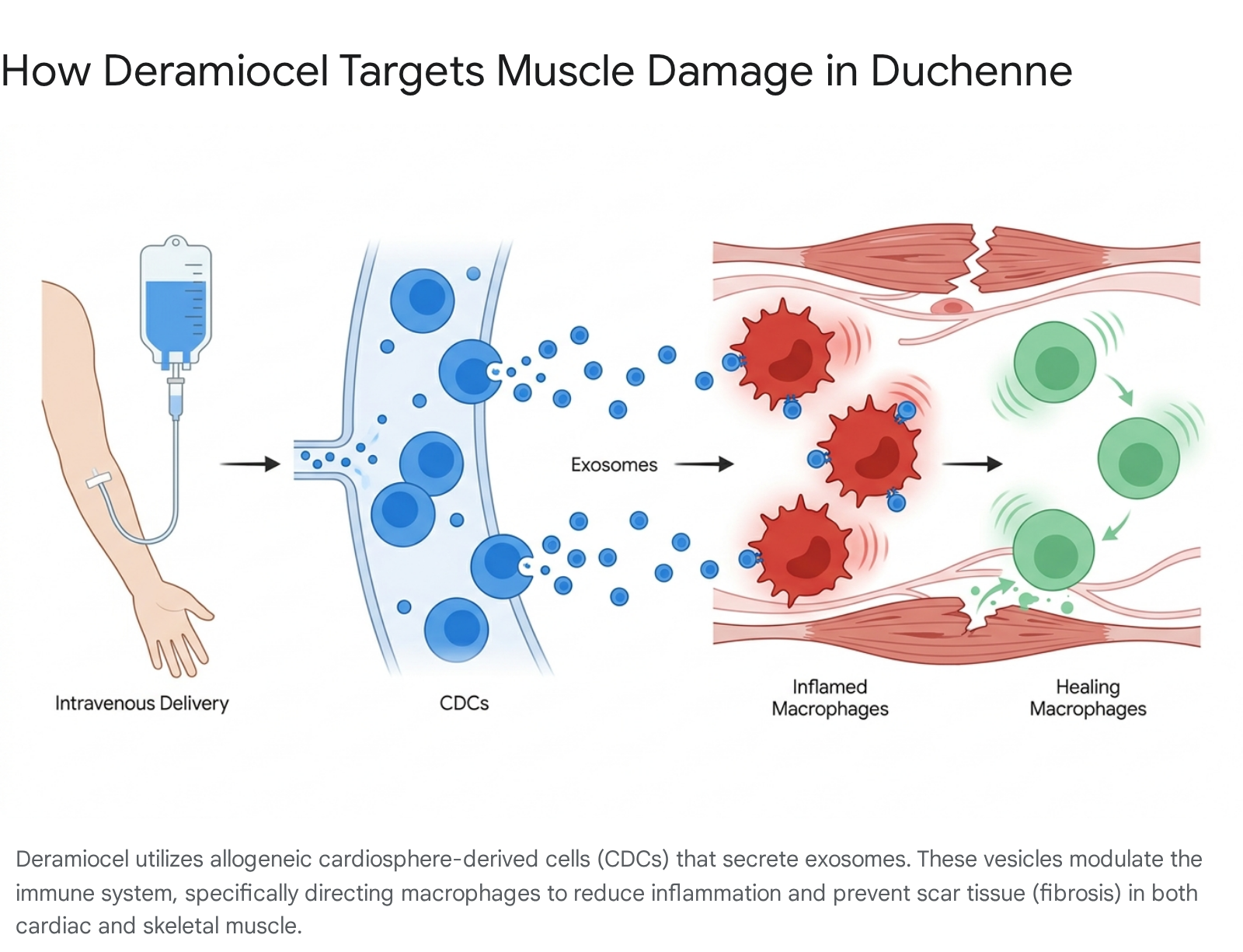
Once in the body, the CDCs secrete massive amounts of extracellular vesicles known as exosomes 2615. These tiny particles carry a payload of proteins, lipids, and RNA 11. The exosomes travel through the body and are taken up by the patient's immune cells - most notably, macrophages 615.
Macrophages are a type of white blood cell that act as the body's cleanup crew. In a Duchenne patient, macrophages are chronically "angry," triggering intense inflammation as they attempt to clear out the constant muscle damage 46. Deramiocel's exosomes essentially reprogram these macrophages, shifting their expression profile from a destructive, pro-inflammatory phenotype to a healing, anti-fibrotic phenotype 611.
By cooling off the chronic inflammation and halting the fibrotic scarring process, deramiocel creates a microenvironment that preserves the remaining functional muscle and encourages natural tissue repair 41116. Because this mechanism targets the downstream consequences of the disease rather than the specific genetic spelling mistake, deramiocel is considered "mutation-agnostic" 310. It has the potential to benefit patients regardless of which specific exon is deleted or mutated in their DNA.
How Deramiocel Compares to Current Standards of Care
To understand the potential impact of deramiocel on the Duchenne community, it is essential to view it in the context of the existing treatment landscape. Duchenne care has historically been defined by a few key classes of drugs, each with significant limitations.
Corticosteroids: The Double-Edged Sword
For decades, the foundational standard of care for Duchenne has been pharmacological corticosteroid therapy 79. Drugs like prednisone and deflazacort (Emflaza) are potent anti-inflammatories that help delay the loss of ambulation, preserve respiratory function, and reduce the risk of severe scoliosis 81620. More recently, the FDA approved vamorolone (Agamree), a "dissociative corticosteroid" designed to retain anti-inflammatory benefits with potentially fewer side effects 721.
Corticosteroids are generally recommended for patients beginning around age 4 to 8, before physical decline accelerates 716. However, their long-term use is fraught with devastating side effects. Patients often suffer from severe weight gain, stunted linear growth, bone density loss resulting in frequent fractures, cataracts, and significant behavioral issues 7920. Furthermore, while steroids slow the progression of muscle weakness, they cannot stop the inevitable cardiac scarring 810.
Exon-Skipping Therapies: Mutation-Specific Interventions
In recent years, the FDA has approved several exon-skipping therapies, including eteplirsen (Exondys 51), golodirsen (Vyondys 53), casimersen (Amondys 45), and viltolarsen (Viltepso) 316. These drugs use antisense oligonucleotides to act like a genetic patch, forcing the body's cellular machinery to skip over the faulty section of the DMD gene 516. This allows the production of a truncated, partially functional form of dystrophin 16.
However, exon-skipping is highly exclusive. A patient must have a specific genetic mutation to qualify. For example, Exondys 51 is only applicable to the roughly 13% of Duchenne patients with a mutation amenable to exon 51 skipping 16. Vyondys 53 applies to only about 8% of the population 16. Furthermore, these drugs require burdensome weekly intravenous infusions 1622, and clinical experts still express uncertainty regarding their long-term impact on functional outcomes, as much of the data relies on early surrogate endpoints rather than robust functional gains 22.
Gene Therapy: The Elevidys Revolution
The most high-profile advancement in Duchenne treatment is Elevidys (delandistrogene moxeparvovec-rokl), an adeno-associated virus (AAV) gene therapy developed by Sarepta Therapeutics 17. In June 2024, the FDA expanded its approval for Elevidys to include both ambulatory and non-ambulatory individuals aged 4 and older 1819.
Elevidys works by delivering an engineered, shortened version of the dystrophin gene (micro-dystrophin) directly into the patient's cells 17. While the clinical potential is profound, Elevidys comes with strict limitations. First, because it uses a viral vector to deliver the gene, patients who naturally possess pre-existing antibodies to the AAVrh74 virus are ineligible 19. Second, patients with deletions in exon 8 and/or 9 are strictly contraindicated due to severe safety risks 1819.
Safety remains a significant concern with viral gene therapies; tragic cases of acute liver failure have occurred in trials 2021. Finally, Elevidys is a one-time-only treatment, carrying a wholesale acquisition cost (WAC) of $3.2 million, making it one of the most expensive drugs in the world 22.
Comparing the Options
| Therapy Category | Example Drugs | Target Population | Mechanism of Action | Delivery | Primary Limitations |
|---|---|---|---|---|---|
| Corticosteroids | Prednisone, Deflazacort, Vamorolone | All ages; mutation-agnostic 821 | Broad systemic immunosuppression to slow muscle damage 9 | Daily oral tablet or liquid 721 | Severe side effects: weight gain, bone loss, stunted growth, behavioral issues 7. |
| Exon-Skipping | Exondys 51, Vyondys 53, Amondys 45 | Specific genetic cohorts (e.g., Exon 51, 53) 16 | Splicing RNA to allow production of truncated dystrophin 516 | Weekly IV infusion 1622 | High logistical burden (weekly IV); only applicable to small sub-populations; debated long-term functional efficacy 1622. |
| Gene Therapy | Elevidys | Ages 4+; excluded for Exon 8/9 deletions or AAV antibodies 1819 | Delivers a micro-dystrophin gene via an AAV viral vector 17 | Single, one-time IV infusion 22 | $3.2M cost; risk of acute liver failure; one-time only; unproven in severe late-stage disease 202122. |
| Cell Therapy | Deramiocel (CAP-1002) | Mutation-agnostic; heavily studied in older, non-ambulatory patients 31323 | Reprograms macrophages to reduce inflammation and cardiac fibrosis 411 | Quarterly (every 3 months) IV infusion 323 | Currently unapproved; requires regional travel 4x/year; requires pre-medication for potential hypersensitivity 321. |
If deramiocel achieves FDA approval, it is not viewed as a replacement for these existing therapies. Instead, Capricor has positioned deramiocel as a complementary treatment 315. Because it targets the downstream inflammation and scarring rather than the genetic defect, deramiocel could theoretically be used alongside corticosteroids, exon-skippers, or even after gene therapy, offering a synergistic approach to managing the disease 315.
The Clinical Evidence: Focusing on the Non-Ambulatory
A recurring frustration in the Duchenne community is the design of clinical trials. The FDA historically prefers endpoints related to ambulation, such as the North Star Ambulatory Assessment (NSAA) or the 6-minute walk test 22. As a result, companies are incentivized to test their drugs on young boys (ages 4 to 8) who are still walking. Older patients, who have already lost ambulation and are experiencing respiratory and cardiac decline, are frequently excluded from trials and denied access to new innovations 62131.
Capricor took a different path. The company specifically designed its pivotal trials - HOPE-2 and HOPE-3 - to include non-ambulatory patients and those in the late stages of the disease, directly addressing a massive unmet clinical need 631. The average age of participants in the Phase 3 HOPE-3 trial was approximately 15 years old, a demographic highly vulnerable to cardiac complications 2332.
The HOPE-2 Trial: A Proof of Concept
The clinical foundation for deramiocel was established in the Phase 2 HOPE-2 clinical trial. Published in prestigious medical journals like The Lancet, HOPE-2 was a randomized, double-blind, placebo-controlled study evaluating the safety and efficacy of intravenous deramiocel 324.
The trial demonstrated that in a non-ambulatory population, deramiocel stabilized skeletal muscle function to the point where disease progression was attenuated by 71% over the first 12 months 1334. Following the main trial, participants were invited to enter the HOPE-2 Open Label Extension (OLE). Data presented at recent Muscular Dystrophy Association (MDA) and Parent Project Muscular Dystrophy (PPMD) conferences highlighted that after 36 to 48 months of continuous treatment, patients maintained the therapeutic benefit in both cardiac and skeletal muscle function, proving the therapy's durability 342536.
HOPE-3: Hitting the Endpoints
To secure FDA approval, Capricor launched HOPE-3, a larger Phase 3, multicenter, randomized, double-blind, placebo-controlled trial across 20 U.S. clinical sites 23. The trial enrolled 106 boys and young men, all of whom were on a stable background regimen of corticosteroids 2332. Over 75% of the participants already had a clinical diagnosis of cardiomyopathy 23.
Patients were randomly assigned to receive either 150 million cells of deramiocel or a placebo via intravenous infusion every three months for one year 23. The trial was unblinded in late 2025, and the results were widely celebrated within the scientific and advocacy communities 2337.
Deramiocel met both its primary endpoint and its key secondary endpoints with statistical significance 23.
Preserving Upper Limb Function: For non-ambulatory boys, preserving arm and hand strength is the difference between independence and total reliance on caregivers. It dictates whether a patient can feed themselves, drive a power wheelchair, or use a phone 3638. This is measured using the Performance of Upper Limb (PUL v2.0) assessment 2426.
In HOPE-3, patients treated with deramiocel showed a 54% slowing of disease progression in their PUL v2.0 scores compared to the placebo group at 12 months (p=0.029) 3224. A secondary measure, the Duchenne Video Assessment (DVA), which tracks real-world movements at home, showed an 83% slowing of disease progression in practical tasks, such as bringing food to the mouth 527.
Attenuating Cardiac Decline: The most highly anticipated data surrounded the heart. Cardiac function was measured centrally via MRI to determine the Left Ventricular Ejection Fraction (LVEF) - the percentage of blood leaving the heart each time it contracts 2324.
Across the entire treatment group, deramiocel was associated with a 91% slowing of the decline in LVEF over 12 months (p=0.041) 3224.
Even more striking were the results for patients who entered the trial with pre-existing cardiomyopathy. In this specific subgroup, deramiocel didn't just slow the decline; it resulted in a 3.3 percentage-point improvement in LVEF compared to the placebo group. This corresponds to greater than 100% attenuation of the expected cardiac decline (p=0.017) 27.
Biomarkers of Healing: Late Gadolinium Enhancement
The clinical functional scores were backed up by physical changes in the heart tissue itself. Using contrast-enhanced cardiac MRIs, researchers evaluated late gadolinium enhancement (LGE) 2741. LGE is a validated biomarker for myocardial fibrosis; essentially, it lights up the scar tissue in the heart 27.
The presence of LGE is strongly associated with progressive cardiac dysfunction, arrhythmias, and heart failure risk in Duchenne 27. The HOPE-3 data revealed a statistically significant reduction in fibrotic segments in patients treated with deramiocel versus placebo (p=0.022), corresponding to a three-segment treatment difference at 12 months 27. Furthermore, blood tests showed significant reductions in creatine kinase (CK-MB), an enzyme that indicates cardiac muscle damage 24.
Taken together, these results confirm that deramiocel is actively reducing inflammation, preventing new scar tissue, and allowing the heart to maintain its structural integrity 1327.
The Regulatory Rollercoaster
Despite the promising science, the path to FDA approval has been unpredictable. The regulatory journey of deramiocel illustrates the complex tension between the FDA's mandate for rigorous efficacy data and the patient community's desperate need for timely access to treatments.
The July 2025 Complete Response Letter
In late 2024, Capricor submitted a rolling Biologics License Application (BLA) to the FDA based primarily on the Phase 2 HOPE-2 data, an open-label extension, and comparisons to natural history datasets provided by Duchenne advocacy groups 121324.
Initially, the FDA granted Priority Review, signaling the urgency of the condition 12. However, the process derailed in mid-2025. An anticipated FDA Advisory Committee (AdComm) meeting was abruptly canceled 2025. Shortly after, in July 2025, the FDA issued a Complete Response Letter (CRL) 142026.
A CRL is effectively an agency rejection. In the letter, the FDA stated that the BLA did not meet the requirements for "substantial evidence of efficacy" based solely on the Phase 2 data 2442. The agency argued that the HOPE-2 trial was originally designed to evaluate skeletal neuromuscular function rather than cardiomyopathy, making it an inadequate pivotal study for a cardiac-specific label 28. Capricor pushed back, noting that the FDA itself had encouraged the company to focus the BLA on cardiomyopathy during informal meetings in 2024, and pointing out that the statistical models used were valid 28.
Re-aligning with the FDA
Following the CRL, Capricor held a crucial Type A meeting with the FDA to establish a path forward 26. During this meeting, the FDA agreed to exercise "regulatory flexibility" and stated that the ongoing, larger HOPE-3 trial could serve as the required confirmatory study 26. The FDA agreed that the new data could be submitted within the framework of the existing BLA, maintaining PUL v2.0 as the primary endpoint and LVEF as a key secondary endpoint 26.
When the HOPE-3 trial met all its endpoints in late 2025, Capricor rapidly compiled the clinical study reports 1123. In February 2026, the company submitted the massive data package to the FDA 1144.
The 2026 PDUFA Date
On March 10, 2026, Capricor announced a major breakthrough: the FDA officially lifted the CRL and resumed its review of the deramiocel BLA, classifying it as a Class 2 resubmission 1442.
The FDA established a new Prescription Drug User Fee Act (PDUFA) target action date of August 22, 2026 1429. This is the date by which the agency is legally expected to announce its final decision on whether to approve deramiocel for commercial use.
If approved, the therapy would not only enter the market but would likely qualify Capricor for a Rare Pediatric Disease Priority Review Voucher (PRV) 11442. PRVs can be sold to other pharmaceutical companies (often for around $100 million), providing a massive influx of non-dilutive capital that Capricor could use to scale up manufacturing and launch the drug nationwide 1031.
What Approval Means for Families: The Logistics of Care
While scientists debate p-values and executives track PDUFA dates, Duchenne families live in the logistical reality of disease management. If the FDA approves deramiocel in August 2026, what will this treatment actually look like for a patient?
The Infusion Experience
Unlike complex gene therapies or autologous CAR-T cell therapies (which require drawing the patient's blood, engineering it in a lab, and reinfusing it), deramiocel is an allogeneic, "off-the-shelf" product 31617. It is manufactured centrally at Capricor's GMP facility in San Diego, frozen, and shipped to clinics 2930.
The therapy is administered via intravenous (IV) infusion once every three months (four times a year) 323. For boys whose veins have been damaged by years of medical procedures, it is notable that the infusion can be delivered via a simple butterfly needle; an implanted surgical port is not strictly required 10.
In terms of safety, the treatment is generally well-tolerated. Out of over 800 infusions performed in clinical trials, there have been no severe new safety signals 331. However, because the cells are foreign to the body, allergic (hypersensitivity) reactions can occur. In the trials, reactions such as fever, rash, or changes in blood pressure were occasionally reported 316. These are typically managed by administering pre-medication (like antihistamines) before the infusion or by temporarily slowing the infusion rate 31621.
Finding a Specialized Care Center
Deramiocel cannot be administered at a neighborhood pharmacy or a standard pediatrician's office. Because it requires specialized handling and cardiac monitoring, families will need to travel to a designated infusion center or a major academic hospital 324950.
In the United States, Duchenne care is heavily centralized. Families often rely on the network of Certified Duchenne Care Centers (CDCCs) established by the Parent Project Muscular Dystrophy (PPMD), or one of the roughly 150 Muscular Dystrophy Association (MDA) Care Centers 3334. While these centers provide world-class, multidisciplinary care, their geographic distribution is uneven, often requiring families to travel across state lines 333435.
The Hidden Financial Burden on Caregivers
Even if insurance completely covers the price of the drug, the physical act of getting to a quarterly infusion introduces a massive, often invisible financial burden on families. Caregiving for a patient with advanced Duchenne is already an incredibly expensive endeavor 10.
The Baseline Cost of Accessibility
As Duchenne progresses and patients lose ambulation, the physical environment must be drastically altered. A recent survey by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) quantified this burden 5436.
The study found that families caring for someone with Duchenne face average out-of-pocket expenses totaling $78,303 over a five-year period simply to modify their homes and vehicles 5436. The largest single expense is purchasing or heavily modifying a handicap-accessible van, which averages nearly $48,000 5436. Modifications to home entrances and bathrooms account for another $30,000 5436. In addition, families spend an average of $14,071 out-of-pocket on medical equipment, primarily highly specialized power wheelchairs 5436.
The Price of Medical Travel
Adding quarterly medical travel to this baseline is daunting. Traveling with a non-ambulatory Duchenne patient requires immense planning. Airlines have a notoriously poor record of handling power wheelchairs; in 2019 alone, airlines reported breaking or damaging over 10,000 wheelchairs and scooters .
If flying is too risky, families must drive. This requires reliable, accessible vehicles and careful route planning to ensure hotels have genuinely accessible roll-in showers and beds at a safe transfer height 57.
Research into other quarterly cell therapies (such as CAR-T for cancer) highlights the severe financial toxicity of medical travel. Direct travel costs, including specialized lodging, gas, and hospital meals, can quickly drain a family's savings 583738.
Lost Income and Caregiver Exhaustion
The most profound hidden cost is lost income. Taking days off work every three months for travel, infusion, and observation periods puts employment at risk.
In the UK, research by the Anthony Nolan charity found that households undergoing cell therapy treatments lost an average of £30,000 (roughly $38,000 USD) in income because caregivers had to reduce their working hours or take unpaid leave 58. In the US, the ISPOR survey noted that as a Duchenne patient's upper-limb function declines, the need for professional, round-the-clock caregiving skyrockets 38. Annualized costs for professional care jump from roughly $2,500 for a patient with full arm mobility to over $11,000 for a patient with moderate-to-severe impairment 38.
If deramiocel proves successful in the real world at preserving upper-limb function as it did in the HOPE-3 trial, it could theoretically save families thousands of dollars in long-term caregiving costs 3638. However, surviving the immediate logistical reality of getting the therapy will require robust financial support programs, which Capricor's new commercial leadership team will be tasked with building prior to the 2026 launch 3161.
Navigating the Insurance Maze
Before a single drop of deramiocel reaches a patient, the family's neurologist will have to wage war with insurance companies. Cell and gene therapies carry eye-watering price tags 3262. While Capricor has not released official pricing, analysts project it will be priced similarly to existing exon-skipping drugs, which often run hundreds of thousands of dollars annually 3163.
The Prior Authorization Battle
Health plans and pharmacy benefit managers (PBMs) view these therapies as massive financial liabilities. A recent survey showed that 85% of health plans expect cell and gene therapies to create major financial challenges in the coming years 32. Consequently, insurers employ aggressive utilization management tactics 39.
To get deramiocel, patients will almost certainly require prior authorization 6240. Insurers will demand extensive documentation proving the patient matches the exact clinical profile approved by the FDA 5041. This will likely involve submitting recent cardiac MRIs to prove the status of their Left Ventricular Ejection Fraction (LVEF), genetic test results confirming their DMD mutation, and clinical notes proving they have already tried standard-of-care corticosteroids (a process known as step therapy) 165041.
If a patient's clinical profile slightly deviates from the FDA label, the initial claim will be denied. The patient's neurologist will then have to file a series of appeals, potentially culminating in an external board review 49. Families are advised to work closely with dedicated case managers provided by the drug manufacturer to navigate this bureaucracy 49.
Reimbursement Realities: Inpatient vs. Outpatient
Where the drug is administered will dictate how it is billed, which heavily influences whether a hospital is willing to provide it.
If deramiocel is administered while a patient is admitted to a hospital (inpatient), many state Medicaid programs and commercial insurers use a bundled payment system known as Diagnosis-Related Groups (DRGs) 6267. Under a DRG, the hospital receives a single, flat fee for the entire hospital stay, regardless of the individual services provided. Because the cost of deramiocel will vastly exceed standard DRG payouts, hospitals could lose hundreds of thousands of dollars on the procedure 62. This financial disincentive can make hospital administrators reluctant to offer the therapy.
To solve this, specialized therapies are increasingly being administered in dedicated outpatient infusion clinics 6742. In the outpatient setting, the drug can be billed separately under the patient's medical benefit (using specific J-codes) rather than bundled into a hospital stay, allowing the facility to recoup the high cost of the drug 496243.
Furthermore, to manage costs, insurers are beginning to explore Value-Based Purchasing (VBP) agreements 6270. Under these contracts, the drug manufacturer must refund a portion of the cost to the insurance company if the therapy fails to stabilize the patient's heart function as promised in the clinical trials 62.
Bottom line
For families living with the devastating reality of advanced Duchenne, FDA approval of deramiocel would mark a monumental shift, providing the first therapy explicitly proven to target the cardiac fibrosis that ultimately takes patients' lives. The clinical data strongly supports its ability to preserve heart function and upper-limb mobility in older, non-ambulatory young men who have aged out of other trials. However, the true success of this therapy will depend not just on FDA clearance in August 2026, but on whether the healthcare system can dismantle the crushing logistical, financial, and insurance barriers that stand between the patient and the infusion chair.