Talk Therapy vs Somatic Therapy: What's the Difference
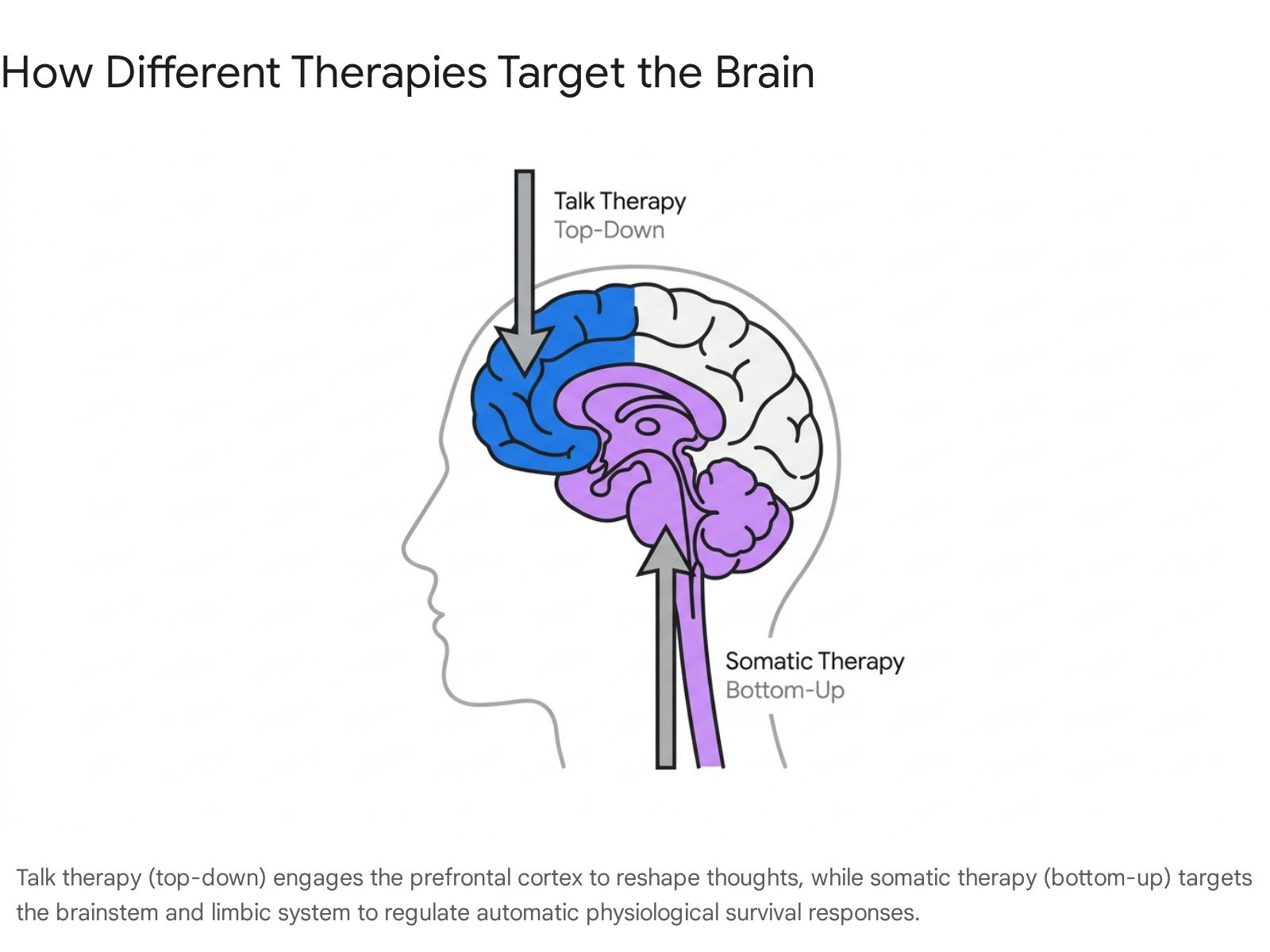
Talk therapy is a "top-down" approach that uses language and cognitive reframing to help you understand your emotions, process memories, and change your behaviors. Somatic therapy is a "bottom-up" approach that focuses directly on physical sensations to help your autonomic nervous system release stored trauma and chronic stress. While traditional talk therapy excels at building intellectual insight, somatic therapy is often necessary when the body continues to react to triggers that the logical mind already understands.
For decades, the cultural default for treating mental health struggles has been a comfortable chair and a guided conversation. Traditional psychotherapy - commonly referred to as talk therapy - has a vast, proven track record for treating conditions ranging from general anxiety to severe depression 1. However, a growing number of patients and clinicians are recognizing a frustrating plateau: you can cognitively understand exactly why you have a panic attack, or logically realize that a past event is over, yet still feel your chest tighten and your heart race when triggered 23.
This disconnect between intellectual insight and physical reactivity has fueled the rapid rise of somatic therapy 34. Rather than relying solely on narrative and logic, somatic approaches invite the physical body into the healing process. To decide whether a cognitive approach, a body-based approach, or a blend of both is right for you, it is essential to understand the science of how humans process distress, what actually happens in these sessions, and what the latest clinical research reveals about their effectiveness.
The Brain's Staircase: Top-Down vs. Bottom-Up Processing
To grasp the fundamental difference between talk therapy and somatic therapy, clinical psychologists often rely on a neurological model known as "top-down" versus "bottom-up" processing 256. You can visualize the human brain as a three-story staircase:
- The First Stair (Brainstem): This is your "survival brain," often referred to as the reptilian brain. It is the oldest, most primitive part of the nervous system. It handles automatic functions like heart rate, breathing, and temperature regulation. Crucially, it initiates immediate fight, flight, or freeze responses to danger before you even have time to consciously think about what is happening 25.
- The Second Stair (Limbic System): This is your "emotional brain." This middle layer processes emotions, memories, and unconscious threat detection 57.
- The Top Stair (Prefrontal Cortex): This is your "thinking brain." This highly evolved outer layer is responsible for logic, language, reasoning, planning, and narrative meaning-making 57.
What Is Top-Down Processing?
Traditional talk therapies - such as Cognitive Behavioral Therapy (CBT), Dialectical Behavior Therapy (DBT), Psychoanalysis, and Acceptance and Commitment Therapy (ACT) - are top-down approaches 12. They start at the top of the staircase.
The premise of top-down therapy is that by using the prefrontal cortex to analyze your life narrative, challenge cognitive distortions, and build new coping skills, you can eventually send calming signals down to the emotional and survival centers of the brain 52. Essentially, top-down therapy operates on the theory: If we change your thoughts and beliefs, we can eventually change how your body feels and reacts 5.
What Is Bottom-Up Processing?
Somatic therapy - which encompasses modalities like Somatic Experiencing (SE), Sensorimotor Psychotherapy, and the Hakomi Method - is a bottom-up approach 23. The word "somatic" originates from the Greek word soma, meaning "body" 24114.
Research shows that trauma and chronic stress frequently knock the prefrontal cortex "offline," rendering logic and language temporarily inaccessible during a triggering event 5. Because trauma is often stored as fragmented physical sensations and survival energy in the nervous system rather than as coherent narrative stories, bottom-up therapies bypass the top stair entirely 52.
Bottom-up therapy operates on the theory: If we regulate your body's physiological response and create a visceral sense of physical safety, your mind will naturally follow, allowing your thoughts and emotions to shift 5.
The Window of Tolerance: The Science of Nervous System Regulation
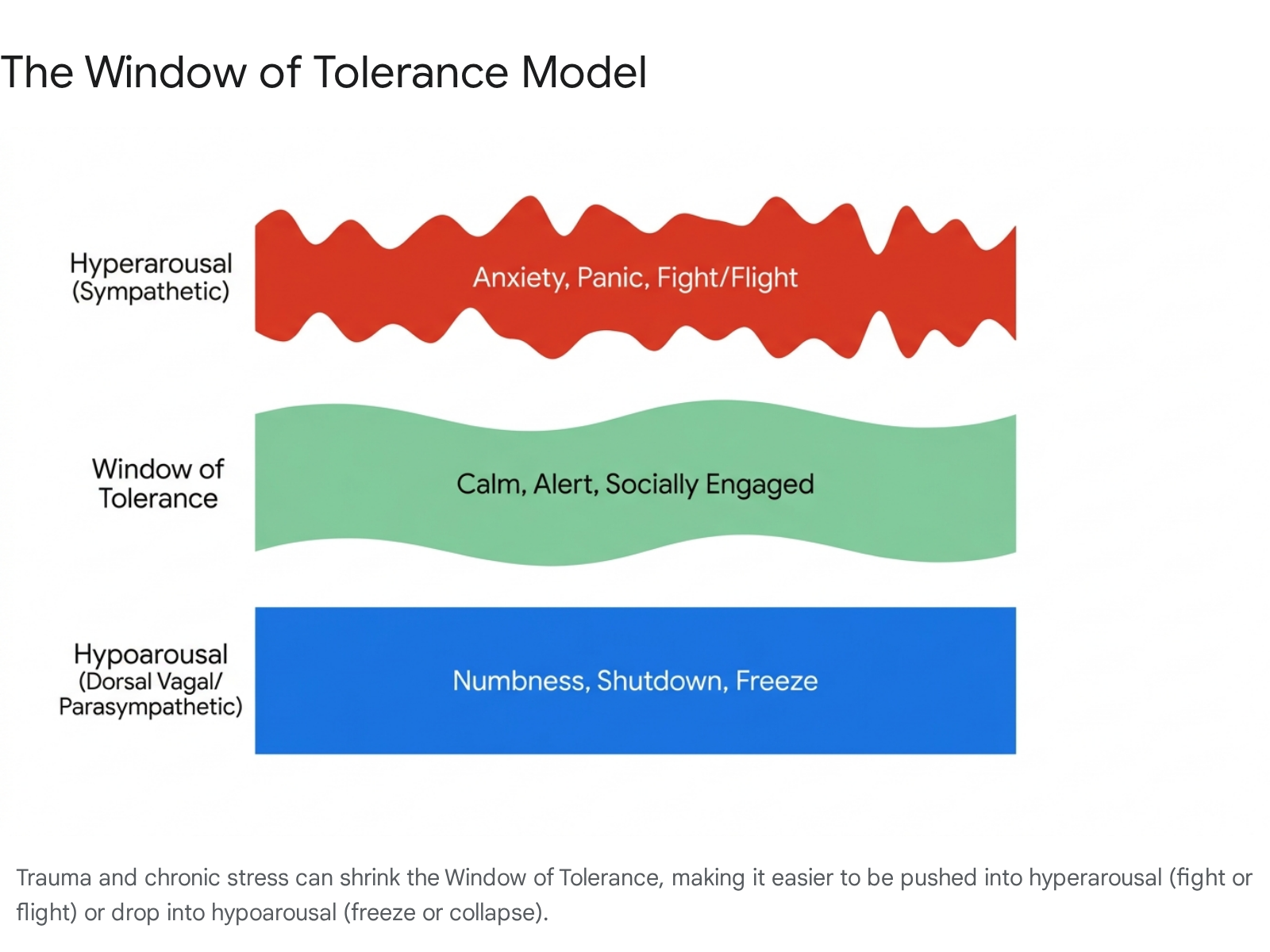
To fully understand why somatic therapy is necessary for certain individuals, it helps to understand a clinical concept coined by psychiatrist Dr. Dan Siegel: The Window of Tolerance 131415.
Imagine your nervous system as a river. When you are floating down the middle, the water is relatively calm. This is your Window of Tolerance - the optimal zone of arousal where your sympathetic and parasympathetic nervous systems are in balance. In this zone, you can think clearly, process emotions healthily, engage socially, and manage everyday stressors without losing your cool 131415.
Shrinking the Window
When a person experiences severe adversity, ongoing burnout, or acute trauma, this window of tolerance can shrink 145. Minor stressors that once felt manageable now push the individual entirely out of their optimal zone into one of two extreme autonomic states:
- Hyperarousal (Too much arousal): The sympathetic nervous system initiates a massive fight-or-flight response. The body is flooded with excessive survival energy, manifesting as panic, hypervigilance, irritability, an elevated heart rate, and the inability to relax 15517.
- Hypoarousal (Too little arousal): The dorsal vagal parasympathetic system initiates a freeze, flop, or collapse response. The nervous system becomes so overwhelmed that it simply shuts down. This manifests as emotional numbness, dissociation, a flat affect, chronic exhaustion, and feeling disconnected from your own body 1551718.
If you try to process severe psychological pain while stuck in a state of hyperarousal or hypoarousal, traditional talk therapy can occasionally backfire, leading to re-traumatization. As trauma expert Dr. Peter Levine often points out, you cannot effectively process cognitive thoughts if your bodily alarms are screaming that you are standing in front of a tiger 6. Somatic therapy's primary objective is to physically expand your Window of Tolerance so that you can safely process your life experiences without panicking or shutting down 1517.
Inside the Room: Comparing the Experience
While both therapeutic approaches aim to reduce distress and improve daily functioning, the actual experience of sitting in a practitioner's office (or on a telehealth call) feels vastly different depending on the modality you choose.
| Feature | Traditional Talk Therapy (e.g., CBT) | Somatic Therapy (e.g., Somatic Experiencing) |
|---|---|---|
| Primary Focus | Thoughts, beliefs, emotional narratives, and behavioral patterns 119. | The mind-body connection, physical sensations, and autonomic nervous system regulation 319. |
| Starting Point | Language, memory recall, and cognitive framing (Top-Down) 22. | Posture, breath, tension, and visceral bodily sensations (Bottom-Up) 22. |
| Typical Techniques | Cognitive restructuring, behavioral activation, exposure, homework assignments 1621. | Breathwork, grounding, tracking sensations, pendulation, titration 31922. |
| Goal of Session | Insight, behavioral change, meaning-making, and symptom reduction 12324. | Nervous system coherence, discharging "stuck" survival energy, and restoring physical safety 323. |
| Best Suited For | Anxiety, depression, phobias, building coping skills, and relationship issues 12. | Complex trauma, PTSD, bodily dissociation, chronic pain, and feeling "stuck" despite prior therapy 157. |
Anatomy of a Talk Therapy Session
Cognitive Behavioral Therapy (CBT) is one of the most widely researched and heavily structured forms of talk therapy, typically lasting between 8 to 20 sessions 26. A standard CBT session is a collaborative, goal-oriented conversation divided into predictable, distinct phases:
- Check-In and Mood Assessment: The therapist begins with a brief mood check, sometimes using a standardized self-report questionnaire (like the PHQ-9 for depression or GAD-7 for anxiety) to objectively track your progress over time 68.
- Bridge and Agenda Setting: You and the therapist briefly review the most important takeaways from the previous session. Then, you collaboratively set an agenda of specific, current problems you want to tackle during the hour 62128.
- Homework Review: Skill acquisition is what sets CBT apart from unstructured "venting." The therapist will review the homework assigned in the previous session - such as a thought log where you tracked negative automatic thoughts during the week - to see what you learned 218.
- Agenda Execution (Cognitive Restructuring): You discuss a difficult situation on the agenda. The therapist helps you identify cognitive distortions (e.g., catastrophizing, assuming the worst) and challenges you to reframe those thoughts by examining the objective evidence for and against them 22126.
- Actionable Takeaways: The session concludes with a final summary and a new homework assignment, allowing you to practice the skills you just learned in the real world 621.
Anatomy of a Somatic Therapy Session
Somatic therapy sessions - whether utilizing Somatic Experiencing, the Hakomi Method, or Sensorimotor Psychotherapy - are generally less rigidly structured. They are highly fluid and paced entirely by the capacity of the client's nervous system.
Instead of staying locked in continuous dialogue about the past, a somatic therapist will routinely pause the conversation to draw your attention to your present-moment physical experience 324. A session relies heavily on the following core mechanics:
Tracking
Tracking involves inviting you to notice and describe internal physical sensations (interoception) without judgment. Instead of asking "How did that make you feel emotionally?", the therapist might ask, "When you talk about that difficult meeting, what do you notice happening in your chest or your jaw right now?" 3242930. The goal is to build awareness of the body's language.
Resourcing
Before approaching any difficult traumatic material, the therapist helps you identify a "resource." A resource can be internal (a memory of feeling powerful, a visualization of a safe place) or external (the feeling of your feet firmly planted on the floor, the weight of a blanket). Connecting with this resource brings a visceral feeling of deep safety, grounding, and strength to the body, serving as an anchor 39.
Titration
Trauma is clinically defined as an event that occurred "too much, too fast, too soon" for the nervous system to handle. Titration is the antidote to this overwhelm. It involves engaging with distressing memories or physical tension in microscopic, highly controlled doses 29932. You might only touch upon the stress for a few seconds before deliberately backing away. This prevents emotional flooding and ensures the nervous system can actually process the event rather than just surviving it again.
Pendulation
Coined by Dr. Peter Levine, pendulation is the act of consciously shifting your attention back and forth - like a pendulum - between a sensation of distress (e.g., a tight knot in the stomach) and a resourced state of safety (e.g., the warmth in your hands) 293210. This oscillation teaches a dysregulated nervous system that it is not permanently stuck in danger, restoring the natural rhythm of expansion and contraction 91034.
Discharge
As the body begins to feel safe and the nervous system exits the fight-or-flight state, it may attempt to release the "survival energy" it trapped during the original trauma. This release, known as discharge, can look like spontaneous trembling, shaking, crying, deep yawning, or a sudden, profound exhalation 2226.
The Scientific Evidence: What the Research Says
If you are evaluating treatments for trauma, depression, or chronic stress, you are likely wondering which modality the broader medical and scientific community formally endorses. The answer is nuanced, depending largely on how "evidence-based" is defined by major health institutions.
The Stance of the American Psychological Association (APA)
Traditional talk therapies have a massive, decades-long head start in empirical research. According to the APA's updated 2025 Clinical Practice Guideline for the Treatment of PTSD in Adults, top-down cognitive approaches - specifically Prolonged Exposure (PE), Cognitive Processing Therapy (CPT), and Trauma-Focused CBT (TF-CBT) - carry the strongest, highest-tier evidence recommendations 111213. These therapies have been subjected to countless large-scale, randomized controlled trials (RCTs) proving they significantly reduce PTSD symptoms 11.
Presently, purely somatic approaches do not hold this top-tier clinical guideline recommendation from the APA. The primary reason is that the sheer volume of massive-scale RCTs for somatic therapy does not yet match the decades of data compiled for CBT 123839.
However, the field is evolving. The APA recently released parallel professional practice guidelines for Working with Adults with Complex Trauma Histories (often referred to as C-PTSD). Complex trauma stems from repeated, chronic interpersonal trauma (such as childhood abuse) rather than a single event. These new guidelines emphasize that treatment must go beyond simple symptom reduction and cognitive processing. They advocate for a phase-based approach that prioritizes nervous system stabilization, physical safety, and addressing the profound somatic and dissociative symptoms that accompany complex trauma 131441.
The Challenge of Measuring the Body
The lack of top-tier institutional endorsement for somatic therapy does not mean it is ineffective; rather, it reflects a structural challenge in how psychological research is conducted 38.
Top-down therapies like CBT are highly manualized. A therapist follows a strict, step-by-step protocol that looks nearly identical for every patient. This makes it incredibly easy to test in a rigorous laboratory setting. Conversely, somatic therapy is inherently fluid, intuitive, and highly individualized to the micro-movements of a patient's nervous system on any given day. This makes it genuinely difficult to standardize for clinical trials 263815.
Despite these hurdles, the empirical evidence base for somatic therapy is growing rapidly and showing highly promising outcomes: * Significant Effect Sizes: A 2021 scoping review of Somatic Experiencing found large, statistically significant effect sizes (Cohen's d > 0.8) for reducing both PTSD and depression symptoms 73816. * High Remission Rates: One controlled trial demonstrated that 44.1% of participants no longer met the clinical criteria for PTSD after completing somatic therapy. Nearly half of the participants moved from a clinical diagnosis to full symptom remission 38. * Dramatically Lower Dropout Rates: This is arguably the most crucial metric. Recent 2024 and 2025 research indicates that 30% to 50% of patients do not achieve remission with gold-standard cognitive exposure therapies. Furthermore, dropout rates in real-world settings can reach up to 50% because the process of verbally recounting horrific trauma is simply too overwhelming for the nervous system 11. Somatic therapies, which do not require patients to verbally narrate the worst moments of their lives, show significantly lower attrition rates 11. * Cultural Acceptability: Studies conducted in urban safety-net clinics show high acceptability of somatic therapy among diverse, low-income populations who had previously dropped out of or felt alienated by traditional exposure-based talk therapies 111517.
The current consensus among trauma specialists is that somatic therapy is deeply "evidence-informed" and increasingly validated by modern neuroscience, even as it continues to climb the ladder of formal institutional RCT guidelines 3839.
Emerging Biological Adjuncts
The recognition that trauma is fundamentally a biological injury to the nervous system has spurred National Institute of Mental Health (NIMH) clinical trials exploring medical ways to assist bottom-up processing. Interventions like Transcranial Magnetic Stimulation (TMS), Amygdala-EEG neurofeedback, and Stellate Ganglion Blocks (SGB) are being rigorously tested to physically calm the brain's fear circuitry 1118194720. Furthermore, psychedelic-assisted therapies (utilizing MDMA or psilocybin) are currently navigating FDA trials. These compounds appear to reduce amygdala reactivity, artificially expanding the patient's Window of Tolerance so they can process somatic trauma without the overwhelming fear response that usually shuts down therapeutic progress 1847.
Somatic Therapy vs. Somatic Symptom Disorder
When exploring this topic, readers often encounter the term "Somatic Symptom Disorder" (SSD), which sounds similar to somatic therapy but refers to a distinct clinical challenge.
Somatic Symptom Disorder is a mental health condition characterized by an extreme, disproportionate focus on physical symptoms - such as severe pain, chronic fatigue, or digestive issues - that cause major emotional distress and problems functioning 4950. The physical pain is entirely real, but medical doctors often cannot find a biological or structural cause for it 50.
Often, SSD is linked to a psychological trait called alexithymia - the inability to recognize, identify, or describe one's own emotions 5021. When a person cannot mentally process profound emotional distress, the brain may translate that psychological pain into a physical, somatic experience 50. Somatic therapy is frequently used to treat SSD. By teaching patients to track their bodily sensations and safely connect them to underlying emotions, somatic therapy helps resolve the psychological root of the unexplained physical pain 4921.
Global Roots: The Ancient Origins of Embodied Healing
While terms like "Somatic Experiencing" and "Sensorimotor Psychotherapy" were coined, trademarked, and popularized by Western psychologists in the late 20th century, the foundational mechanisms of somatic therapy are anything but new 235222.
Modern somatic practitioners are increasingly pushing to "decolonize" wellness, explicitly acknowledging that many body-based systems were appropriated by the West, stripped of their community and spiritual contexts, and repackaged as clinical innovations 52225423. The truth is, Indigenous, African, and Asian cultures have understood the mind-body connection for millennia.
African and Caribbean Traditions
Traditions like Haitian Vodou, Cuban Santería, and various West African healing ceremonies (such as those led by Yoruba Babalawos) have long utilized rhythmic drumming, chanting, and trance dance to move suppressed emotional energy through the body 225424. The fundamental belief in these cultures that illness is a holistic disruption to be collectively discharged maps flawlessly onto modern somatic principles of nervous system regulation and physical release 5424.
Asian Traditions
India's 5,000-year-old Ayurvedic medical system utilizes Pranayama (breath control) to regulate the nervous system - a practice identical to modern somatic breathwork 5457. Traditional Chinese Medicine (TCM) and practices like Qigong and Tai Chi have historically viewed emotional pain as life force energy (Qi) blocked in specific organs. These systems utilize slow, intentional movements and acupressure to dissolve trauma, predating Western psychology's recognition of the mind-body link by thousands of years 5457.
Indigenous American Traditions
For generations, Indigenous cultures have recognized that trauma lives in the physical body, the community, and the land. Embodied practices, grief rituals, and community healing circles treat physical and psychological suffering holistically 522225. Reclaiming these traditional somatic practices is increasingly viewed not just as a path to wellness, but as a vital act of cultural restoration and resilience against historical trauma 2326.
How to Choose: Bridging the Gap
When deciding between talk therapy and somatic therapy, the good news is that it rarely has to be an "either/or" choice. In fact, clinical consensus strongly suggests that the most profound, lasting healing happens when top-down and bottom-up approaches are integrated 27760.
The brain and the body operate on a bidirectional highway. Top-down therapies give you the language to understand your life, build boundaries, and consciously change destructive habits. Bottom-up therapies give your nervous system the stability and physical safety required to actually implement those cognitive changes without collapsing into panic 5760.
You might lean toward starting with Talk Therapy if: * You are dealing with specific behavioral patterns or cognitive distortions you want to change 119. * You are facing mild-to-moderate anxiety, depression, or a specific life transition 127. * You find structured problem-solving, logic, and cognitive reframing comforting and effective 2127. * You do not have severe, complex trauma or a history of feeling highly dissociated from your body 27.
You might lean toward starting with Somatic Therapy if: * You have spent years in talk therapy analyzing your issues ("I know exactly why I'm like this") but still experience the exact same physical anxiety and startle responses 3247. * You have a history of complex, developmental, or early childhood trauma 256. * You frequently feel disconnected, numb, or "floating outside" of your own body 57. * Traditional talk therapy triggers severe panic attacks or feels completely overwhelming, leading you to abandon treatment 617.
Many modern, trauma-informed therapists utilize a phased, integrative approach. They begin with bottom-up somatic techniques to stabilize the nervous system and build a baseline of physical safety. Once the client's Window of Tolerance is sufficiently expanded, the therapist gradually introduces top-down cognitive work to consolidate those insights, build resilience, and reshape the client's personal narrative 5760.
Bottom line
Talk therapy primarily relies on the thinking brain to alter emotional and behavioral patterns, making it highly effective for developing logical insight, building coping strategies, and reframing negative narratives. Conversely, somatic therapy addresses the physical imprints of stress and trauma, utilizing bottom-up techniques like breathwork, titration, and sensation tracking to regulate the autonomic nervous system. While traditional talk therapies like CBT hold the lion's share of top-tier clinical backing, somatic therapy is rapidly gaining empirical support as a powerful, highly tolerable alternative for those whose trauma lives stubbornly in the body. Ultimately, the most comprehensive healing occurs when both modalities are combined, allowing the mind to understand the past while the body safely releases it.