Is Online Therapy as Effective as In-Person Therapy
Research consistently shows that online therapy is just as clinically effective as traditional in-person sessions for treating common mental health conditions like anxiety and depression. While virtual care offers unparalleled convenience and frequently results in higher program completion rates, face-to-face therapy retains distinct advantages for severe diagnoses and the interpretation of subtle nonverbal cues. The optimal choice ultimately depends on the specific therapeutic approach used, the severity of the clinical presentation, and the patient's individual comfort with digital communication.
The Global Shift to Tele-Mental Health
The delivery of psychological services underwent a permanent transformation following the global disruption of the COVID-19 pandemic. Prior to 2020, telepsychology was largely considered a niche service or a temporary stopgap. Today, the integration of digital technology into mental health services represents a foundational advancement in global health infrastructure.
According to the World Health Organization's (WHO) Mental Health Atlas 2024, mental health conditions affect more than one billion people worldwide, yet severe gaps in access and quality of care persist 1. Only 12% of countries currently meet all WHO criteria for the full integration of mental health into primary care, and a staggering 91% of people with depression globally do not receive minimally adequate treatment 1. In this context, the WHO has explicitly endorsed digital self-help tools and tele-mental health - now available in 63% of countries - as critical mechanisms for efficiently and affordably scaling care across geographic and socioeconomic boundaries 11.
The primary barrier to psychological care is rarely a lack of clinical efficacy but rather logistical friction. Traditional in-person therapy requires commute time, child care arrangements, schedule coordination, and the navigation of physical clinical spaces that can trigger stigma or anxiety 2. By removing these obstacles, online therapy has transitioned from an alternative option to a primary care pathway. However, as the digital landscape matures, clinicians and researchers have pivoted from asking whether online therapy works to investigating how it works, who it works best for, and which specific modalities are most effectively translated through a screen.
Establishing the Clinical Baseline: Is Online Therapy Effective?
The question of whether a digital interface dilutes the effectiveness of psychotherapy has been rigorously tested over the past several years. The scientific consensus is clear: for the vast majority of common mental health disorders, online therapy is not a lesser substitute but a clinical equivalent to in-person care 23.
The CMAJ Meta-Analysis on Cognitive Behavioral Therapy
One of the most definitive evaluations of digital efficacy was published in the Canadian Medical Association Journal (CMAJ) in March 2024. Researchers conducted an exhaustive systematic review and meta-analysis comparing therapist-guided remote Cognitive Behavioral Therapy (CBT) against traditional in-person CBT 456. The study analyzed 54 randomized controlled trials (RCTs) encompassing a total of 5,463 adult patients 5.
The remote interventions analyzed included videoconferencing, teleconferencing, and internet-delivered CBT programs supported by licensed practitioners 8. The researchers utilized the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to evaluate the certainty of the evidence. The results yielded moderate-certainty evidence demonstrating little to no statistical difference in the effectiveness of remote versus in-person CBT across all primary patient-important outcomes (Standardized Mean Difference [SMD] -0.02, 95% Confidence Interval -0.12 to 0.07) 567.
This equivalence was not limited to a single diagnosis. The researchers segmented the RCTs by clinical condition and found that the delivery medium did not alter the therapeutic outcome for an exceptionally broad spectrum of somatic and psychological disorders.
| Clinical Condition Category | Number of RCTs in Meta-Analysis | Comparative Effectiveness (Remote vs. In-Person) |
|---|---|---|
| Anxiety and Related Disorders | 17 | No significant difference 5 |
| Depressive and Mood Disorders | 14 | No significant difference 5 |
| Insomnia | 7 | No significant difference 5 |
| Chronic Pain or Fatigue Syndromes | 6 | No significant difference 5 |
| Body Image or Eating Disorders | 5 | No significant difference 5 |
| Tinnitus | 3 | No significant difference 5 |
These findings reinforce the WHO's designation of CBT as an essential health care intervention and confirm that remotely delivered, therapist-guided CBT can be deployed to facilitate massive expansions in evidence-based care without compromising clinical integrity 47.
Global Corroboration of Digital Efficacy
The clinical equivalence of online therapy is not restricted to Western health systems. A cross-sectional study conducted during the pandemic at a mental health clinic in the United Arab Emirates evaluated 49 clients who received psychotherapy in both online and in-person modalities. The researchers found that the clients' overall satisfaction levels did not significantly differ between the two formats, supporting the global viability of teletherapy 10.
Similarly, a 2025 parallel clinical trial in Yazd, Iran, investigated the effectiveness of positive-approach group counseling for women experiencing psychosexual complications following a benign complete abdominal hysterectomy. Sixty-six participants were randomly assigned to either online or face-to-face counseling for eight sessions. Both groups saw significant increases in their sexual intimacy scores by week twelve. Interestingly, the online counseling group demonstrated slightly higher efficacy in enhancing sexual intimacy (P = 0.043) compared to the face-to-face cohort, suggesting that the privacy and comfort of the home environment may facilitate deeper engagement when discussing highly sensitive physiological and relational challenges 8.
Synchronous vs. Asynchronous: The Video and Text Debate
As the definition of "online therapy" expands, it increasingly encompasses fundamentally different modes of communication. The two dominant paradigms are Video-Based Psychotherapy (VBP) - which relies on synchronous, live face-to-face interaction over a webcam - and Message-Based Psychotherapy (MBP) - which utilizes asynchronous text, audio, or video messages exchanged throughout the week via dedicated applications.
A critical question for modern mental health architecture is whether the asynchronous, text-heavy nature of MBP can rival the conversational fluidity of live video. A rigorous pragmatic sequential multiple-assignment randomized clinical trial (SMART), published in JAMA Network Open in October 2025, provided a definitive comparison 129.
The JAMA 2025 Depression Trial
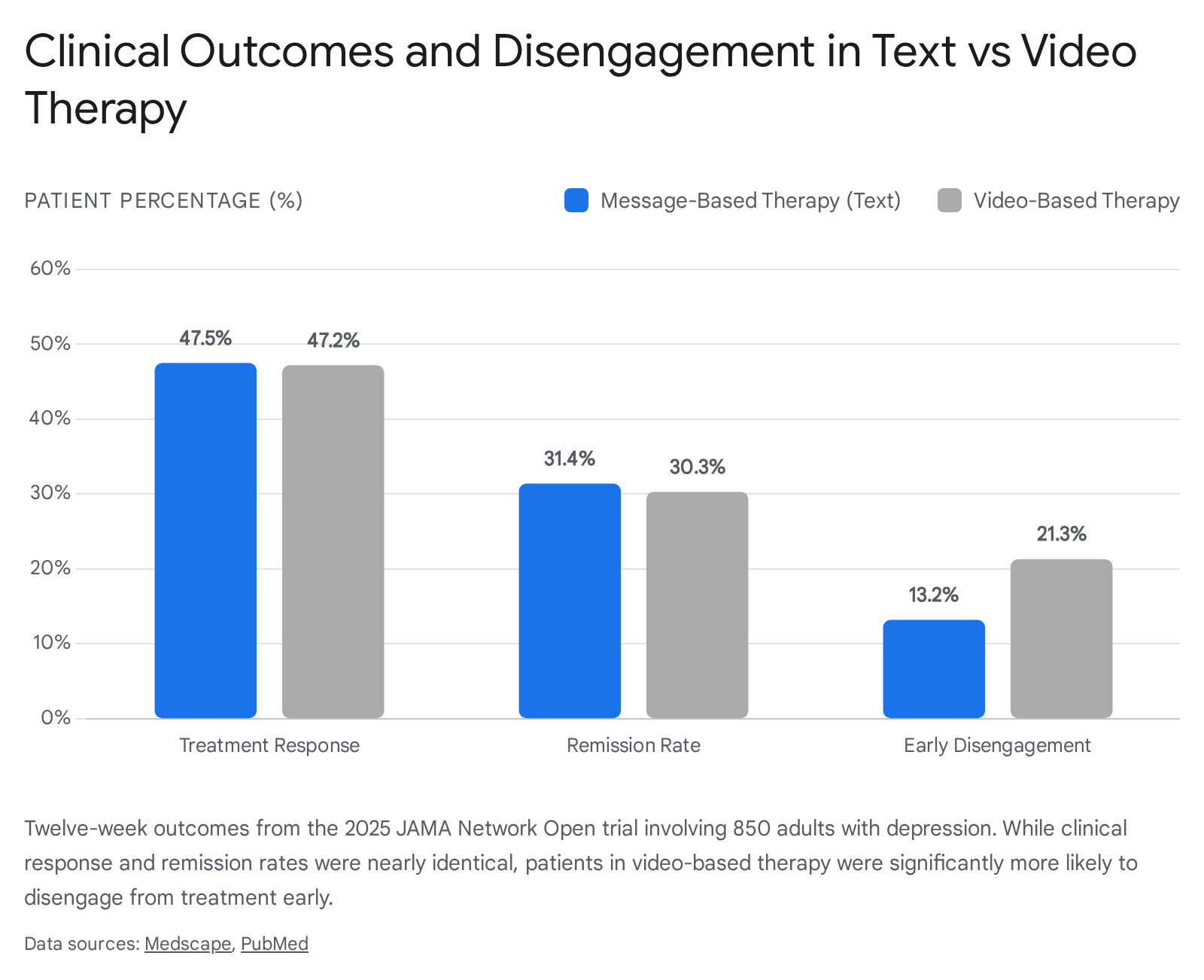
Researchers from the University of Washington School of Medicine partnered with Talkspace, a major commercial mental health platform, to evaluate 850 adults diagnosed with depression 1415. Participants were initially randomized to receive either weekly VBP or ongoing MBP for a 12-week period. To ensure rigorous clinical tracking, patients who did not respond to their assigned modality by week six were re-randomized to receive a combination of both therapies 12. Primary outcomes were measured using the nine-item Patient Health Questionnaire (PHQ-9) and standard social functioning metrics 1214.
The clinical outcomes challenged traditional assumptions regarding the necessity of real-time conversational therapy. By the end of the 12-week trial, there were no statistically significant differences in clinical improvement between the text-based and video-based cohorts 1210. The rate of clinical response (defined as a 50% or greater reduction in PHQ-9 symptom scores) was 47.5% for the MBP group and 47.2% for the VBP group 129. Similarly, the rates of total remission were virtually identical: 31.4% for text therapy versus 30.3% for video therapy 129.
Behavioral Discrepancies and Early Disengagement
While the end-stage clinical outcomes were equivalent, the delivery format significantly influenced how patients behaved during the treatment process.
The most glaring discrepancy was in patient retention. The study revealed that participants assigned to weekly live video sessions were significantly more likely to disengage and drop out of treatment within the first five weeks (21.3%) compared to those utilizing asynchronous messaging (13.2%) 1215.
Researchers hypothesized that message-based therapy offers greater operational flexibility, allowing patients to interact with their treatment on their own schedule rather than coordinating strict live appointment times, thereby reducing the friction that leads to dropout 141011.
Conversely, the data highlighted a distinct advantage for video therapy regarding initial rapport building. Among patients who were classified as nonresponders early in the trial, those in the VBP group reported a significantly stronger therapeutic alliance at week four compared to their MBP counterparts 1215. This suggests that while live video demands more scheduling commitment and causes higher early attrition, the real-time visual interaction fosters a more rapid interpersonal bond for patients who struggle to engage with the material.
The implications of this trial are vast. By demonstrating that asynchronous text can match live video in treating a leading cause of global disability, the research validates message-based care as a highly scalable, evidence-based alternative. The study authors explicitly recommended that broader insurance reimbursement for message-based platforms could drastically improve access to care for the millions of individuals who cannot accommodate live therapy appointments 911.
Modality Matters: How Different Therapy Styles Translate to the Screen
Psychotherapy is not a monolithic practice. It comprises dozens of distinct clinical modalities, each relying on different mechanisms of action. Consequently, the transition from the physical office to the digital screen impacts these approaches differently. Understanding how specific therapy styles fare online is crucial for setting accurate clinical expectations.
Cognitive Behavioral Therapy (CBT)
As demonstrated by the CMAJ meta-analysis, CBT adapts exceptionally well to digital environments. Because CBT is inherently highly structured, psychoeducational, and focused on practical skill-building, it does not rely exclusively on the nuanced physical presence of the therapist 312. The digital format actually enhances several core CBT components. Video platforms allow for seamless screen-sharing, enabling the therapist and client to collaboratively fill out digital thought records, review behavioral homework, and analyze cognitive distortions in real time 1913.
Furthermore, internet-based CBT (eCBT) empowers patients to access interactive self-help modules and multimedia materials between sessions, reinforcing the learning process 14. For these reasons, online CBT is widely considered the gold standard for digital efficacy 15.
Dialectical Behavior Therapy (DBT)
Dialectical Behavior Therapy was originally developed to treat borderline personality disorder (BPD) and severe emotional dysregulation. Standard comprehensive DBT is an intensive, resource-heavy treatment involving weekly individual therapy, weekly group skills training (focused on mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness), and between-session phone coaching 2316.
Given the severity of the symptoms it treats, the transition of DBT to an online format (e-DBT) was initially met with skepticism. However, recent systematic reviews have confirmed the efficacy and feasibility of internet-delivered DBT skills training 16. Studies show no significant differences in symptom reduction between online and in-person DBT groups; both formats produce large reductions in depression, anxiety, and general psychiatric symptoms 1625.
The most fascinating aspect of e-DBT research is the paradox it reveals between patient retention and patient satisfaction.
Standard in-person DBT is notorious for high attrition rates due to its demanding schedule and the emotional intensity of group work. However, online DBT has dramatically improved retention. A 2024 analysis observed a 69% completion rate for virtual DBT therapy compared to a mere 44% for in-person sessions 25. For emotionally sensitive individuals or those struggling with severe trauma, attending a group skills class from the physical safety of their own home mitigates nervous system overwhelm. It removes the anxiety associated with commuting, navigating a clinical waiting room, and engaging physically with a group of strangers 232526.
Despite higher completion rates, the digital barrier does extract a toll on subjective satisfaction. A 2026 pilot study assessing patients in a comprehensive outpatient DBT program found that 63% of participants opted for online groups, but those who attended in-person reported higher overall satisfaction with the therapy (a mean score of 53.5 compared to 49.2 for online participants) 17. Furthermore, 90% of in-person attendees felt the group directly helped them deal with their presenting problems, compared to 82.2% of online participants 17.
This data suggests a clear trade-off: in-person DBT fosters a richer sense of accountability, stronger group cohesion, and higher subjective satisfaction, but online DBT drastically lowers the barrier to entry and ensures that highly vulnerable patients actually finish the curriculum 2328.
| Factor | In-Person DBT | Online e-DBT |
|---|---|---|
| Clinical Efficacy | Highly Effective | Highly Effective (Comparable symptom reduction) |
| Completion Rates | Moderate to Low (~44%) | High (~69%) |
| Patient Satisfaction | Higher (Due to stronger group cohesion) | Slightly Lower (Due to digital distractions and isolation) |
| Primary Advantage | Controlled environment, non-verbal cues, peer accountability | Safety of home environment, scheduling flexibility, reduced social anxiety |
Psychodynamic Therapy
Psychodynamic therapy presents one of the most complex challenges for tele-mental health. Unlike the structured worksheets of CBT or the classroom-style skills training of DBT, psychodynamic therapy is a "depth psychology" approach. It explores unconscious processes, defense mechanisms, and early life experiences 18. A core component of this modality is the analysis of "transference" - how the patient redirects unconscious feelings about figures from their past onto the therapist.
Historically, psychodynamic practitioners have relied heavily on the physical environment of the consulting room. The silence, the shared physical space, the subtle shifts in posture, and the controlled isolation of the clinic are actively utilized as therapeutic tools 19. Consequently, the incorporation of online delivery into psychodynamic therapy has been controversial 19.
Despite theoretical reservations, the empirical data is highly promising. A systematic review and meta-analysis of randomized controlled trials evaluated the efficacy of Internet-delivered psychodynamic therapy (IPDT) 1820. The analysis involved 1,080 total participants and found small but significant effects favoring IPDT compared to inactive control conditions across main outcomes, including depression (g = 0.46) and anxiety (g = 0.20) 20. Crucially, the effects of IPDT were maintained or even increased during follow-up periods, suggesting that deep, lasting psychological restructuring can indeed occur over a digital connection 1820.
However, studies actively comparing online psychodynamic therapy directly to face-to-face psychodynamic therapy often reveal a preference for the physical room. A study evaluating university students during the COVID-19 pandemic found that while both online and face-to-face counseling effectively reduced psychological distress, the face-to-face interventions proved more robust at increasing overall life satisfaction and reducing a wider spectrum of psychopathological problems 15. Both patients and psychotherapists in these specific qualitative studies frequently reported that face-to-face psychodynamic therapy yielded slightly better relational results, citing the "artificiality" and "loss of presence" experienced via webcam 15.
Systemic and Family Psychotherapy
When treating complex relational dynamics, such as family therapy or couples counseling, the efficacy of the digital medium becomes more ambiguous. A 2025 systematic review and meta-analysis published in the Journal of Medical Internet Research attempted to synthesize evidence on the comparative efficacy of systemic psychotherapy delivered digitally versus face-to-face 21.
Analyzing trials involving youths with poor diabetic control, traumatic brain injuries, and parents of youths with anorexia nervosa, the researchers found massive heterogeneity in the data. Nonaggregated analyses of 56 distinct outcomes yielded highly mixed results: the digital modality was superior in 18% of outcomes, the face-to-face modality was superior in 5%, and the remaining 77% showed no clear superiority or equivalence 21. Furthermore, there were no significant differences in attrition or the number of sessions attended between the two formats 21. The researchers concluded that, at this stage, it is impossible to declare definitive superiority or equivalence for systemic psychotherapy delivered online, highlighting the need for more rigorous, large-scale trials in family-based interventions.
Emerging Youth Modalities: ACT and EMDR
The pediatric and adolescent mental health sectors have also aggressively expanded into teletherapy to combat staggering waitlists and rampant stigma 1433. Cutting-edge non-inferiority randomized controlled trials are currently underway to assess whether advanced modalities like Acceptance and Commitment Therapy (ACT) and Eye Movement Desensitization and Reprocessing (EMDR) can be effectively administered online to youths aged 12 to 18 14.
ACT, which utilizes structured mindfulness exercises, translates cleanly to an online format 13. EMDR, a trauma-focused therapy originally reliant on the therapist guiding the patient's eye movements manually, has been adapted using specialized digital software that provides bilateral visual and auditory stimulation via the patient's screen and headphones 1433. While definitive long-term data on virtual EMDR for youth is still pending, early protocols suggest that high willingness to participate in teletherapy combined with robust digital tools can make these specialized trauma treatments highly viable in non-acute settings 14.
Deconstructing the Digital Therapeutic Alliance
Regardless of the specific clinical modality, decades of psychotherapy research dictate that the single most robust predictor of treatment success is the "therapeutic alliance" (TA) 192223. Formally defined by psychologist Edward Bordin in 1979, the therapeutic alliance consists of three core components: mutual agreement on the goals of therapy, agreement on the tasks required to achieve those goals, and the affective emotional bond between the therapist and the patient 2324.
For years, skeptics argued that the inherent distance of a screen, the loss of direct eye contact, and the inability to share a physical space would irreparably damage this affective bond, rendering teletherapy cold and impersonal 2225. Extensive contemporary research unequivocally refutes this assumption.
Comparable Alliance Strength
A comprehensive meta-analysis of 34 studies evaluating teletherapy interventions confirmed a significant link between the therapeutic alliance and clinical outcomes (average effect size ≈ 0.15, p = .001) 22. A monumental 2024 noninferiority study involving nearly 1,000 clients revealed that individuals receiving teletherapy reported alliance quality commensurate with those engaged in face-to-face psychotherapy 22. Both patients and therapists rated their connections similarly, proving that the fundamental human bond central to psychological healing can develop just as effectively across digital networks 19.
The Disinhibition Effect and Attachment Styles
In certain psychological contexts, the digital medium actively accelerates the formation of trust. Psychologists attribute this to the "online disinhibition effect." The physical separation and perceived invisibility of a screen can drastically reduce social anxiety and relational pressure, prompting patients to reveal suppressed emotions, trauma, and vulnerabilities much faster than they would in the intimidating environment of a clinical office 2538.
A patient's underlying attachment style also plays a profound role in how they navigate the digital alliance. Patients with secure attachment patterns are generally more capable of engaging in self-exploration and collaborative understanding, regardless of the medium 23. Conversely, for patients with highly anxious or avoidant attachment styles, the screen acts as a protective buffer, allowing them to carefully calibrate their emotional exposure and retreat to the safety of their own physical environment the moment the session concludes 2623.
The Perception Gap: Clients vs. Therapists
An intriguing psychological phenomenon has emerged from the teletherapy data: a distinct "perception gap" regarding the quality of the virtual relationship. Studies consistently show that clients frequently rate their digital therapeutic connections much more positively than their therapists do 1915.
Therapists are rigorously trained to interpret micro-expressions, shifts in posture, and energetic changes in a controlled room. When restricted to a two-dimensional, chest-up view subject to audio lags and pixelation, clinicians often experience a profound sense of "loss of presence" 15. This sensory deprivation leads therapists to assume the alliance is weakening. Clients, however, are focused primarily on feeling heard, validated, and safely guided; if the therapist communicates effectively, the client perceives a robust, highly supportive bond, completely unaware of the therapist's internal technical anxieties 19.
Techniques for Engineering Virtual Rapport
Because the natural osmosis of shared physical space is absent, clinicians must actively engineer rapport through a screen. This requires the deliberate adaptation of nonverbal communication and therapeutic rhetoric.
Visual and Environmental Adjustments Therapists must compensate for the loss of full-body language by optimizing their visual frame. Best practices dictate adopting a "passport view" (framing the head, shoulders, and hands) to ensure gestures remain visible 26. Clinicians are trained to slightly exaggerate facial expressions and verbal affirmations (e.g., "I hear you," "Right") to ensure empathy pierces the digital divide 222640. Furthermore, because eye contact online requires looking directly into the camera lens rather than at the patient's face on the screen, therapists must constantly toggle their gaze to simulate genuine eye contact 27.
Crucially, therapists must verbally narrate off-screen actions. In a physical office, a client can see a therapist pick up a pen; online, looking down to take notes appears as disengagement. By explicitly stating, "I am looking down to write that important point in my notes," the therapist transforms a potential rupture into an act of validation 26.
The Power of Clinical Analogies To bridge the gap of physical abstraction, highly skilled tele-therapists rely heavily on vivid clinical analogies. Analogies serve as a shared linguistic bridge, transforming complex, invisible psychological concepts into grounded, relatable imagery 42.
For example, when a patient expresses fear that the therapist cannot handle the intensity of their trauma over a webcam, the therapist might reframe the relationship: "Think of me as a mechanic you call when you are stranded on the road. I might not be sitting in the passenger seat, but I can guide you precisely through the tools needed to fix your engine." 42. Similarly, to help a client tolerate emotional dysregulation, the therapist might say, "Emotions are like the weather. Rain clouds covering the sun does not mean the clouds are permanent. We just need to ride through the intensity until they pass." 42. These narrative devices foster a profound sense of shared understanding and emotional resonance, proving that linguistic connection easily transcends physical distance.
The AI Frontier: Establishing a "Digital Therapeutic Alliance"
The concept of the therapeutic alliance is currently undergoing a radical evolution, extending beyond human-to-human interaction entirely. Driven by the massive global shortage of psychiatric professionals, the mental health sector has seen a surge in fully automated, Artificial Intelligence (AI) powered chatbots designed to deliver psychological interventions 3828.
Initially, the idea that a human could form a healing bond with code seemed dystopian. However, human psychology is highly susceptible to the "ELIZA effect" - the unconscious tendency to attribute human-like empathy, understanding, and emotion to digital entities that mimic conversational rules 29.
Recent short-term longitudinal diary studies have investigated how users interact with prominent, commercially available mental health chatbots like Woebot and Wysa 30. The findings indicate that the "Digital Therapeutic Alliance" (DTA) is a very real phenomenon. In a study of 26 adult participants, 18 reported forming a "clear emotional bond" or a "light bond" with the chatbot over a four-week period 30.
The architecture of the DTA mirrors traditional human alliances but leverages unique digital advantages. Users reported that the absolute "humanness" of the conversational design, combined with the complete eradication of relational pressure, fostered deep engagement 38. Chatbots offer zero judgment, do not experience compassion fatigue, and are available instantaneously at 3:00 AM during a panic attack. While AI interventions lack the clinical intuition necessary to treat severe psychopathology or complex trauma, they are rapidly proving to be an effective, highly scalable, and emotionally resonant first line of defense for mild stress, anxiety, and daily emotional regulation 3031.
The Dark Side of Digital Delivery
While telehealth has revolutionized access, the wholesale transition of human communication to digital interfaces has unmasked significant systemic challenges. The most pressing of these is the physiological and psychological toll of technology overload.
Screen Fatigue and Patient Burnout
The effectiveness of online therapy is deeply entwined with a patient's overall digital diet. A recent systematic review analyzing data spanning the COVID-19 pandemic revealed that excessive recreational screen time is consistently linked to increased depression, heightened anxiety, severe stress, and systemic burnout in adults 47.
For individuals whose professional lives require eight to ten hours of intense video conferencing, the prospect of logging into an additional hour of virtual therapy can induce severe cognitive fatigue. Remote work and intense digitalization are heavily linked to eye pain, inattention, disrupted sleep quality, and mental exhaustion 3249. In these scenarios, the therapeutic medium actively conflicts with the patient's physiological limits. For these patients, replacing a screen-based session with an in-person appointment, an audio-only phone call, or asynchronous message-based therapy is often clinically necessary to prevent digital burnout from undermining therapeutic progress 1447.
Digital Compassion Fatigue in Providers
The burden of the digital interface is not borne by patients alone. The rapid transition to virtual care has birthed a novel occupational hazard for clinicians: Digital Compassion Fatigue (DCF) 33.
DCF is a specialized form of profound emotional exhaustion experienced by nurses, therapists, and social workers who provide empathic care exclusively through virtual platforms 33. According to a 2025 concept analysis utilizing Walker and Avant's rigorous theoretical model, DCF is characterized by six defining attributes: 1. Emotional numbing directly related to digital care. 2. Persistent emotional exhaustion following digital engagement. 3. Involuntary compassion withdrawal. 4. Severe cognitive overload caused by "screen-mediated empathy" (the immense neurological effort required to decode micro-expressions and project empathy through a restricted, two-dimensional video feed subject to latency). 5. Feelings of profound professional inefficacy. 6. A measurable decline in the quality of care and therapeutic presence 33.
The antecedents of DCF include prolonged digital caregiving, high emotional demands combined with technological glitches, and a lack of institutional support 33. When therapists are isolated in their homes, devoid of the natural energetic boundaries and peer support found in a shared clinical office, the emotional weight of trauma therapy compounds rapidly. Unrecognized DCF not only devastates provider well-being, leading to industry burnout, but it directly erodes the therapeutic alliance, resulting in reduced patient trust and poorer clinical outcomes 33.
Mitigating DCF requires healthcare organizations to implement strict limitations on consecutive virtual sessions, mandate adequate screen breaks, and provide specialized training in virtual empathy management to preserve the emotional core of the psychiatric workforce 3233.
Updating the Rulebook: Regulatory Evolution
As the empirical evidence cemented online therapy as a permanent fixture of modern healthcare, governing bodies recognized the urgent need to overhaul clinical frameworks. Regulatory structures built for the 20th-century physical clinic were entirely inadequate for the complexities of global, encrypted, digital care.
In August 2024, the American Psychological Association (APA) Council of Representatives formally approved a massive, comprehensive revision of the Guidelines for the Practice of Telepsychology 343536. Driven by rapid advancements in research, law, and post-pandemic clinical realities, the joint task force expanded the original 2013 document into 11 distinct, highly detailed guidelines designed to safeguard both practitioners and patients in the digital age 3738.
The 2024 revisions emphasize that telepsychology is not merely a translation of in-person skills, but a distinct competency requiring ongoing, specialized training 37.
| Key Area of 2024 APA Telepsychology Guidelines | Regulatory Focus |
|---|---|
| Technological Competence | Psychologists must actively maintain literacy in evolving platforms, recognizing how software architecture impacts clinical outcomes 37. |
| Data Security & Privacy | Strict mandates on end-to-end encryption, secure data transmission, and the ethical disposal of digital patient records 3738. |
| Interjurisdictional Practice | Clear frameworks for navigating the complex web of state and international licensing laws when a therapist and patient are geographically separated 3738. |
| Emergency Protocols | Mandates the establishment of localized crisis plans. If a remote patient becomes actively suicidal, the therapist must have predetermined contacts and procedures to intervene physically in the patient's jurisdiction 37. |
| Emerging Technologies | New guidelines explicitly addressing the ethical integration of AI, machine learning, and automated assessment tools into the therapeutic process 37. |
These updated guidelines serve as the operational bedrock for the future of the industry, ensuring that as therapy becomes increasingly digitized and globally distributed, the core tenets of ethical, safe, and highly competent psychological care remain inviolable.
Bottom line
The scientific evidence is overwhelmingly clear: online therapy is not a compromised alternative, but a highly effective clinical modality that matches the symptom reduction of in-person care for the vast majority of mental health conditions. While virtual platforms offer unprecedented accessibility, eliminate geographic barriers, and frequently result in higher program completion rates, they present unique physiological challenges such as digital fatigue and the loss of subtle environmental cues. Ultimately, the choice between digital and face-to-face therapy should not be based on a fear of reduced clinical efficacy, but rather on your personal lifestyle constraints, your diagnosis, and the specific environment in which you feel most secure to engage in deep emotional work.