Science of Near-Death Experiences and Consciousness
The study of near-death experiences occupies a highly complex intersection of neurobiology, clinical psychiatry, and the philosophy of mind. Historically relegated to the domains of theology, folklore, and parapsychology, the phenomenon has undergone rigorous empirical and neuroscientific scrutiny over the past five decades. Driven by continuous advancements in cardiopulmonary resuscitation and neuro-intensive care, an increasing number of individuals survive clinical death. A significant subset of these survivors brings back structured, lucid, and profoundly transformative memories of their time in a borderline state of viability. Contemporary epidemiological estimates and random population polling suggest that approximately ten to twenty percent of cardiac arrest survivors report an anomalous conscious episode during resuscitation, representing millions of individuals globally 1223.
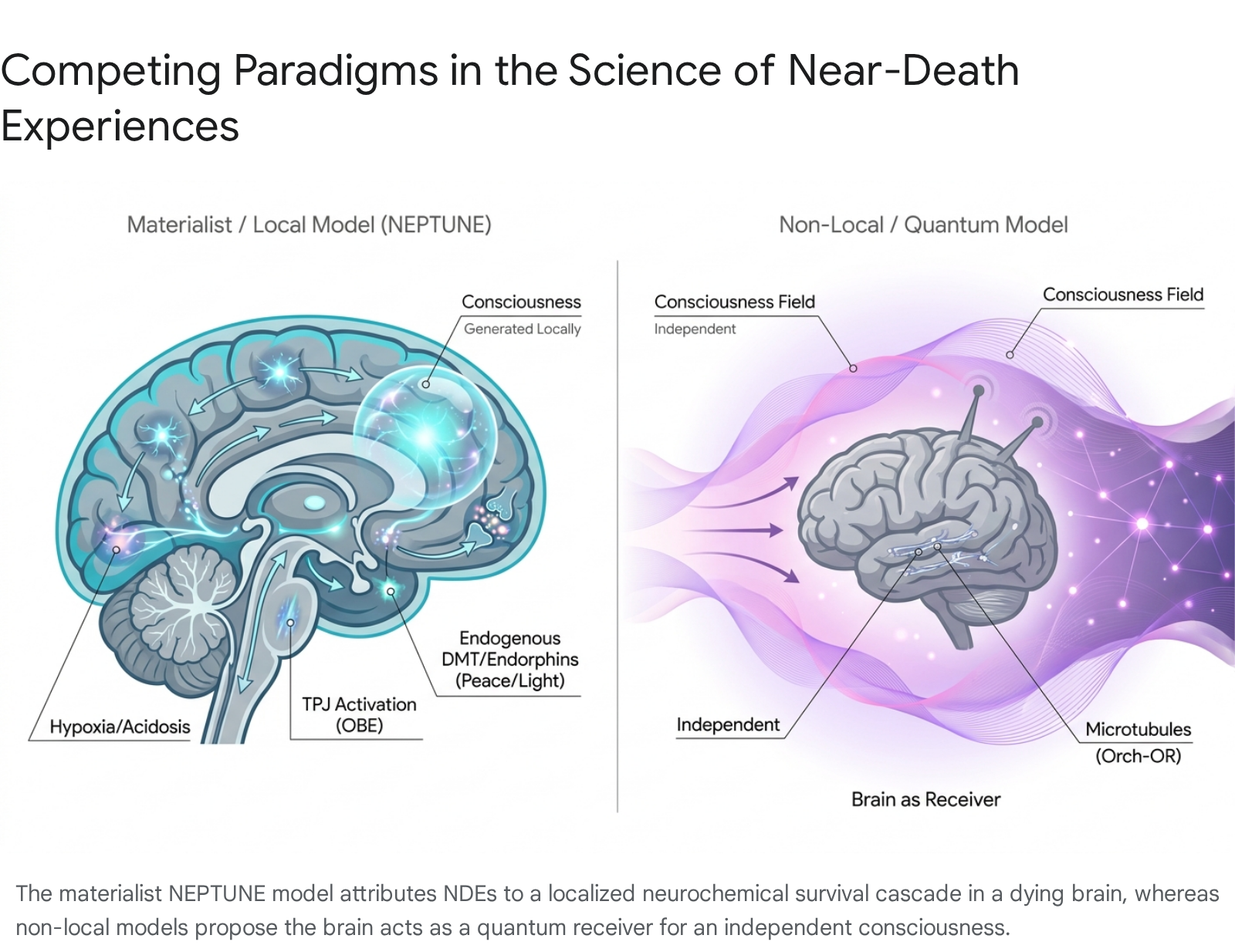
The central scientific debate regarding these phenomena revolves around the fundamental nature of consciousness itself. Prevailing materialist and neurocentric paradigms hypothesize that these experiences are extraordinarily complex hallucinations generated by a dying, hypoxic brain undergoing massive neurochemical and electrophysiological shifts 45. Conversely, an emerging body of anomalous data - including instances of apparent veridical perception during clinical brain inactivity, paradoxical lucidity in advanced dementia, and robust cross-cultural consistencies - has led some researchers to propose non-local models of consciousness. In these alternative frameworks, the brain is theorized to act not as the sole generator of conscious experience, but as a biological receiver or filter, implying that consciousness may persist independently of cortical function 687. This report exhaustively analyzes the science of these episodes, evaluating the psychometric frameworks used to measure them, their cross-cultural phenomenology, the specific neurophysiological mechanisms proposed to explain them, and the recent theoretical models that attempt to resolve the hard problem of consciousness.
Clinical Classifications of Death and Resuscitation
To scientifically investigate anomalous consciousness during a physiological crisis, researchers must first navigate the precise definitions of human death. The ambiguity surrounding the exact moment of death creates significant methodological challenges, as death is increasingly understood not as a singular, instantaneous event, but as a biological process 10812. Medical and legal frameworks generally divide this process into distinct categories, which are critical for establishing the temporal mapping of any reported cognitive activity.
Clinical death is defined by the cessation of cardiopulmonary function - specifically, when the heart stops pumping blood and spontaneous respiration ceases. Clinical death is a medical emergency, but it is potentially reversible if cardiopulmonary resuscitation and advanced life support are initiated immediately. During clinical death, the brain is rapidly deprived of oxygen, leading to cerebral ischemia. Within ten to twenty seconds of cardiopulmonary cessation, standard electroencephalogram monitoring typically flatlines, indicating a cessation of the organized cortical electrical activity generally associated with higher cognitive function and conscious awareness 10910.
If clinical death is not reversed, the organism progresses toward brain death. This state is a legally and medically recognized diagnosis indicating the irreversible cessation of all functions of the entire brain, including the brain stem. Brain death is considered equivalent to the legal and biological death of the individual, even if cardiopulmonary function is maintained artificially via mechanical ventilation and pharmaceutical interventions 1081211. The final stage, biological death, refers to the gradual, irreversible cellular necrosis of multiple organ systems following prolonged ischemia, representing the complete dissolution of the integrated biological organism 1212.
The vast majority of scientific research into anomalous end-of-life consciousness focuses on individuals who have survived clinical death (most notably through cardiac arrest resuscitation) but did not reach the threshold of irreversible brain death. The core scientific paradox lies in the observation that patients routinely report hyper-lucid, structured cognitive and sensory experiences during a clinical window when cortical activity is theoretically insufficient to sustain conscious awareness 61013.
Psychometric Measurement of Anomalous Experiences
Early research in this domain relied heavily on anecdotal collection and qualitative categorization. Pioneering efforts in the 1970s identified recurring motifs such as the sensation of traveling through a tunnel, emerging into a bright light, experiencing a separation from the physical body, and encountering deceased relatives or spiritual figures 218. To transition the field from qualitative observation to quantitative, reproducible science, standardized psychometric instruments were developed to objectively measure and validate subjective reports.
The Greyson Near-Death Experience Scale
The most widely adopted psychometric instrument in the field is the Greyson Scale, developed by psychiatrist Bruce Greyson in 1983. The scale comprises sixteen specific questions, each scored from zero to two, where zero indicates the absence of a feature, one indicates a mild or uncertain presence, and two indicates a definitive, strong presence. A total score of seven or higher out of a possible thirty-two points is the standardized clinical criterion for identifying a genuine episode, effectively differentiating it from organic brain syndromes, non-specific stress responses, and standard dreams or hallucinations 1141516. The mean score among large criterion groups of profound experiencers frequently rests at fifteen 17.
The Greyson Scale evaluates the depth of an experience across four distinct phenomenological components. The cognitive component measures severe alterations in thought processes, assessing whether the subject experienced time distortion (such as time speeding up or slowing down), unnaturally accelerated thoughts, a sudden sense of universal understanding, and the occurrence of a panoramic life review where past deeds and intentions are rapidly evaluated 1415. The affective component assesses profound emotional elements, requiring the subject to quantify feelings of overwhelming peace, joy, a sense of cosmic harmony or unity with the universe, and encounters with a brilliant, unconditional light 1415.
The paranormal component evaluates heightened sensory vividness and apparent extrasensory perception. This includes the classic out-of-body sensation where the self feels entirely separated from the physical form, as well as an awareness of remote events occurring elsewhere, and precognitive visions of the future 1415. Finally, the transcendental component measures encounters with unearthly realms. It queries the subject on whether they entered a mystical or extraterrestrial environment, encountered mystical beings or presences, saw deceased or religious spirits, and whether they perceived a definitive border or point of no return that they were not permitted to cross 141517. Decades of subsequent Rasch rating-scale analyses have established that the total score of this scale fits a unidimensional model, indicating that the scale successfully measures a single, cohesive clinical phenomenon with interval-scaling properties 15.
Alternative Scales and Memory Characteristics
While the Greyson Scale remains the fundamental benchmark for research, subsequent psychometric efforts have sought to address its clinical limitations. A primary criticism of the original scale is its failure to capture distressing, nightmarish, or "hellish" experiences, which account for approximately fourteen percent of all reports. To quantify the phenomenon in a more complete manner, researchers introduced the Near-Death Experience Content (NDE-C) scale, a twenty-item tool that incorporates negative emotional spectrums and provides a more granular five-factor structure covering relevant dimensions 15.
Furthermore, the subjective nature of these experiences poses challenges for empirical validation, leading to the development of the vNDE (verified Near-Death Experience) evidential strength scale in 2025. Created using the Delphi Method through iterative consensus among experts, this eight-item scale rigorously assesses the degree of third-person verification of anomalous information reported by the patient. The vNDE scale evaluates the experiencer's medical state, the impossibility of standard sensory explanations, and the precise number of verified versus erroneous perceptions, allowing researchers to categorize cases into distinct quartiles of evidential strength 23.
To determine whether these episodes are encoded in the brain similarly to hallucinations, researchers utilize the Memory Characteristics Questionnaire (MCQ). Studies deploying the MCQ compare the phenomenological quality of these end-of-life memories against memories of real, physical events and imagined events such as dreams. Findings consistently report that anomalous end-of-life memories contain significantly more detailed, sensory-rich features than memories of both real and imagined events, and completely lack the chaotic, rapidly fading nature of standard hallucinations. Researchers interpret these findings as evidence that the brain encodes these episodes as hyper-real phenomena, suggesting they are structurally distinct from standard metabolic hallucinations 41825.
Cross-Cultural Phenomenology
A major focal point in the literature is determining whether these anomalous experiences represent a universal neurobiological mechanism or a culturally constructed narrative. Early sociologists of religion frequently operated under a cultural source theory, proposing that all anomalous spiritual experiences are generated entirely by a subject's cultural, linguistic, and religious background, serving specific social functions. Conversely, the experiential source theory argues that the core neurological or spiritual event is a universal human phenomenon that precedes culture. Under this theory, the fundamental experience is identical worldwide, but is subsequently interpreted and articulated through local religious and societal frameworks upon the subject's resuscitation 192021.
Western and Asian Variations
Extensive comparative studies highlight both robust similarities and distinct divergences between reports originating in the West and those documented in Asia. While the sensation of leaving the physical body and encountering otherworldly beings are broadly consistent across borders, the specific iconography of the transition phase and the afterlife environment varies significantly depending on the local theology 22302324.
In North America and Europe, the experience is frequently characterized by a rapid transit through a dark, enclosed space - often described as a tunnel - toward a being of brilliant, unconditional light. This is typically accompanied by a rapid, panoramic life review and emotional reunions with deceased family members and recognizable religious figures 223023. However, research into Japanese populations reveals a stark absence of the tunnel motif and the panoramic life review. Instead, Japanese experiencers commonly describe traversing beautiful, terrestrial-like gardens or encountering a river that serves as the definitive point of no return. Furthermore, the light perceived in Japanese accounts is reported to be highly impersonal, lacking the anthropomorphic, divine, or loving attributes frequently assigned to the light in Western accounts 3023.
Reports from India and Thailand demonstrate further cultural stylization, heavily influenced by Hindu and Buddhist eschatology. Indian accounts rarely feature the panoramic life review in the Western sense, where the individual subjectively evaluates their own actions. Instead, they often feature a bureaucratic judgment motif involving spiritual clerks consulting a literal "book of deeds." Encounters with Yama, the traditional lord of death, are highly prevalent in both Indian and Thai accounts. A highly unique phenomenon documented exclusively in these regions is the "mistaken identity" motif. In these narratives, the experiencer is told by spiritual clerks that a divine administrative error has occurred, the wrong person was brought to the afterlife, and the subject is subsequently commanded to return to their physical body 3024.
Indigenous and Traditional Contexts
Research into indigenous and traditional cultures reveals that anomalous end-of-life experiences exist globally but are heavily modulated by local survival mechanisms, societal taboos, and ancient burial practices. A wide-ranging anthropological survey of African traditional religions suggests that historical accounts of these experiences are comparatively rare in indigenous African societies. This scarcity is attributed to precipitous burial practices that limited the opportunity for natural resuscitation, a prevalent cultural fear of ancestral spirits, and a shamanistic focus on spirit possession. In environments where anomalous spiritual experiences are often associated with dangerous sorcery or malevolent possession, individuals were likely reluctant to share their experiences. Nevertheless, isolated cases recorded among the Kongo and Basuto peoples of Central and Southern Africa demonstrate that when these events do occur, they feature the universal core elements: leaving the physical body, journeying to an afterlife realm, and encountering definitive boundaries 25262736.
Among Native American populations, historical records predating extensive colonial and Christian influence confirm the profound presence of these phenomena. Accounts recorded by early explorers, such as John Smith in 1623, alongside the later autobiographical records of Black Elk of the Oglala Sioux and Geronimo of the Chiricahua Apache, illustrate deeply naturalistic interpretations of the afterlife. Native American accounts frequently merge the near-death state with shamanic initiation themes, where the experiencer travels to the "village of the dead" - often observing abundant game, tamed wildlife, and lush nature rather than abstract light - and returns to the physical world with healing knowledge or a spiritual mandate. This narrative of dying, acquiring spiritual authority, and returning to guide the tribe is deeply embedded in indigenous religious revitalization movements 282930. Additional cross-cultural analyses of Maori accounts from New Zealand further support this dual reality: the phenomenology features universal out-of-body components, but the specific entities encountered strictly conform to prevailing Maori beliefs about the ancestral afterlife 313242.
The following table summarizes the key phenomenological differences across major cultural and regional groups:
| Culture / Region | Key Features Present | Key Features Absent or Rare | Associated Mythological Tropes |
|---|---|---|---|
| Western / European | Dark tunnel transit, brilliant being of light, panoramic life review, deceased relatives. | Bureaucratic judgment by clerks, "Mistaken identity" motifs. | Christian/Abrahamic deities, angels, "Being of Light". |
| Japanese | Beautiful gardens, rivers acting as boundaries, impersonal non-anthropomorphic light. | Tunnel sensation, panoramic subjective life review. | Pure Land Buddhist imagery, terrestrial landscapes. |
| Indian & Thai | Bureaucratic reading of deeds, out-of-body state, encounters with deities. | Tunnel sensation, life review (Western style of subjective self-evaluation). | Yama (God of Death), "Mistaken Identity" clerical errors. |
| Indigenous African | Journey to afterlife realms, spiritual beings, encountering firm boundaries. | High prevalence (historically suppressed by cultural taboos). | Ancestral spirits, shamanic initiation motifs, sorcery taboos. |
| Native American | Village of the dead, abundant nature and game, acquisition of shamanic mandate. | Christian theological judgment, abstract domains of pure light (pre-colonial). | Spirit guides, naturalistic spirit realms, revitalization mandates. |
The robust consistency of the out-of-body state and the encounter with an otherworldly boundary across these highly diverse populations provides strong evidence for an underlying universal trigger. Simultaneously, the vast differences in the aesthetic details of the realms and the entities encountered confirm the profound influence of post-experience cultural filtering and linguistic interpretation 24273242.
Neurophysiological Explanations
The sustained effort to map these subjective experiences to specific neurophysiological mechanisms has generated decades of hypotheses and debate. Materialist science posits that the rich phenomenology of the experience can be entirely explained by the aberrant firing of neural networks under extreme metabolic stress, driven by a predictable cascade of physiological fail-safes as the brain attempts to survive clinical death.
Electroencephalographic Surges in the Dying Brain
Historically, standard medical doctrine held that consciousness is extinguished simultaneously with the cessation of cortical electrical activity, which occurs rapidly following cardiac arrest. However, recent continuous electroencephalographic (EEG) studies have severely disrupted this assumption by identifying highly organized, high-frequency brain activity in the peri-arrest period.
In 2023, a landmark study published in the Proceedings of the National Academy of Sciences (PNAS) analyzed the continuous EEG and electrocardiogram signals of four comatose, dying patients immediately before and after the clinical withdrawal of ventilatory support. The researchers found that the resulting global hypoxia unexpectedly stimulated a massive, rapid surge of gamma-wave activity (ranging from 25 to 150 Hz) in two of the four patients. This activity was not chaotic electrical noise; the researchers observed a surge of cross-frequency coupling between the phases of slower alpha and beta oscillations and the amplitudes of the high-frequency gamma oscillations. Furthermore, this functional connectivity was distinctly localized within the temporo-parieto-occipital (TPO) junctions - a posterior cortical area postulated by prominent neurological frameworks, such as the Integrated Information Theory, to be the critical "hot zone" for conscious processing and sensory integration. This localized activity also exhibited directed global connectivity to the contralateral prefrontal areas 33344535.
These human findings directly mirrored previous preclinical animal models conducted in 2013, which demonstrated a transient surge of highly synchronous, global gamma oscillations in the first thirty seconds following experimentally induced cardiac and respiratory arrest in rats. The presence of this organized, high-frequency neurophysiological activity, coupled with cross-frequency coupling, suggests that the mammalian brain possesses the capacity to generate neural correlates of heightened conscious processing paradoxically near death 93436. Materialist researchers hypothesize that this highly aroused electrical state could account for the vivid, hyper-real phenomenological traits reported by survivors. However, critics caution against drawing definitive conclusions, noting that these gamma surges occurred in patients whose hearts were still beating, and because the patients died, none survived to report an actual conscious experience, leaving the correlation between this specific EEG surge and subjective end-of-life phenomenology strictly theoretical 45484950.
Blood Gases and the Endogenous Neurochemical Cascade
The neurochemical hypothesis posits that the intense emotional, visual, and transcendent components of the experience are directly mediated by the massive liberation of endogenous neurotransmitters and peptides during the physiological crisis of dying.
The role of blood gas abnormalities, specifically hypoxia (oxygen deprivation) and hypercarbia (elevated carbon dioxide levels), has been extensively studied. A clinical study of fifty-two cardiac arrest survivors in Maribor, Slovenia, found that the eleven patients who reported a near-death experience upon resuscitation had significantly higher levels of carbon dioxide in their bloodstream and expired breath upon admission to the intensive care unit compared to non-experiencers. Some neurological models suggest that hypercarbia acts analogously to classical hallucinogens, triggering vivid internal visual processing and contributing to the sensation of traversing a tunnel 451.
Alongside blood gas alterations, the profound sense of peace, joy, and the total lack of pain routinely reported during these episodes has been attributed to a stress-induced release of endogenous opioids, particularly beta-endorphins. During moments of extreme physical trauma, the brain releases massive quantities of endorphins which act on limbic structures, such as the amygdala and hippocampus, to produce profound euphoria, analgesia, and psychological detachment, buffering the organism against the terror of death 4373839.
The most heavily debated neurochemical theory centers on endogenous N,N-Dimethyltryptamine (DMT). The striking phenomenological overlap between anomalous end-of-life episodes and the experiences induced by serotonergic psychedelics has led to the hypothesis that endogenous DMT is synthesized and released in large quantities by the dying brain, possibly by the pineal gland. In 2023, researchers conducted a systematic qualitative comparison between a subject's clinically documented near-death experience and their subsequent experience with 5-MeO-DMT, a highly potent psychedelic. The analysis demonstrated profound qualitative similarities, particularly regarding mystical-type experiences, the perception of brilliant light, and the sensation of ego dissolution 4056.
This theoretical link received substantial experimental validation in 2024 through a comprehensive study published on bioRxiv. Researchers utilized high-density EEG and mass spectrometry to analyze the brains of adult rats, providing the first definitive measurements of endogenous DMT in the medial prefrontal and somatosensory cortices at levels comparable to baseline serotonin and dopamine during normal wakefulness. When exogenous DMT was administered intravenously, it induced dose-dependent increases in serotonin and dopamine while simultaneously causing a massive reduction in low-frequency EEG spectral power and a highly significant increase in medium and high gamma bands. This artificially induced functional connectivity across the gamma bands perfectly matched the spontaneous EEG signatures observed in the dying human brains during the PNAS studies, strongly suggesting a shared physiological mechanism of action and supporting a functional role for endogenous DMT in mediating end-of-life consciousness 574142.
Temporal Lobe Epilepsy and Seizure Mechanisms
Other researchers seek the origins of these experiences in structural or functional anomalies of specific brain networks, rather than systemic blood gas or neurochemical changes. Temporal lobe epilepsy (TLE) is characterized by partial seizures originating in the hippocampus and amygdala. Patients with TLE frequently experience complex auras featuring intense déjà vu, time distortion, profound emotions (euphoria or fear), auditory and visual hallucinations, and autoscopic phenomena - the perception of observing one's own body from an external perspective 604362.
Because these symptoms strongly parallel the phenomenology of end-of-life experiences, researchers have investigated the temporal lobes of survivors. A seminal 2004 study by Britton and Bootzin analyzed fifty-five individuals who had reported profound experiences during life-threatening events. The researchers found that these individuals exhibited significantly greater temporal lobe epileptiform EEG activity compared to age-matched controls, with the activity predominantly lateralized to the left hemisphere. Furthermore, the experiencers reported significantly more baseline temporal lobe epileptic symptoms in their daily lives. Rather than indicating a destructive pathology, this altered temporal lobe functioning was not associated with post-traumatic stress disorder, dissociation, or substance abuse; instead, it was strongly associated with positive psychological coping styles and altered sleep physiology. These findings suggest that individuals who report anomalous consciousness during resuscitation may possess an underlying, non-pathological neurophysiological predisposition to altered states of consciousness, rendering them more susceptible to profound experiences during a crisis 604445.
The REM Sleep Intrusion Hypothesis
An alternative physiological explanation relies on the mechanisms of the brain's arousal system, specifically the intrusion of Rapid Eye Movement (REM) sleep into waking consciousness. Promoted extensively by neurologist Kevin Nelson, this hypothesis suggests that the severe physiological crisis of dying triggers a defensive blending of conscious states, where the mechanisms that generate dreams and sleep paralysis are inappropriately activated while the subject is awake or semi-conscious 464748.
During normal REM sleep, the brain is highly active, vivid visual dreaming occurs, and the brainstem sends signals to the spinal cord to induce atonia (temporary muscle paralysis) to prevent the acting out of dreams. Nelson's studies demonstrated that individuals who have had near-death experiences report a lifetime prevalence of REM intrusion - such as sleep paralysis, hypnagogic (falling asleep) hallucinations, and hypnopompic (waking up) hallucinations - that is roughly 2.5 to 2.85 times higher than that of matched control subjects. Proponents of this theory argue that the out-of-body sensation is a direct manifestation of REM-related temporoparietal activity, and the visual hallucinations of deceased relatives are essentially hyper-lucid dreams generated by an arousal system predisposed to REM intrusion under conditions of peril 3464950.
However, the REM intrusion hypothesis has faced severe scientific critique. Critics point out that anomalous end-of-life experiences frequently occur under conditions of general anesthesia, a pharmacological state that actively suppresses and inhibits REM sleep mechanisms. Furthermore, critics argue that the chaotic, bizarre, and rapidly fading nature of normal dreams and hypnagogic hallucinations contrasts sharply with the hyper-real, highly structured, logical, and permanently memorable narratives characteristic of true near-death episodes. Finally, the finding that many experiencers exhibited increased REM intrusion after their life-threatening event suggests that altered sleep architecture may be a consequence, rather than the cause, of the profound psychological transformation 185051.
Integrative Materialist Frameworks and Critiques
In an attempt to synthesize the disparate physiological data into a cohesive neurobiological narrative, neuroscientists have recently introduced comprehensive, unifying models. These attempts have subsequently sparked intense academic debate regarding their true explanatory power and their treatment of anomalous clinical data.
The NEPTUNE Model
In early 2025, a multinational team of researchers published a highly influential integrative framework in Nature Reviews Neurology titled the NEPTUNE model, an acronym for Neurophysiological Evolutionary Psychological Theory Understanding Near-death Experience. Formulated by analyzing empirical data from animal studies, psychedelic research, and clinical observations of the dying brain, the NEPTUNE model posits that these end-of-life experiences are fundamentally an evolutionary defense mechanism. The authors suggest that the experience is a complex, psychologically immersive human extension of thanatosis - the evolutionary biological strategy of feigning death to evade predators 37525354.
According to the NEPTUNE model, when the human body perceives an imminent, unavoidable physical threat resulting in cardiovascular collapse, a predictable physiological cascade is triggered. Blood oxygen levels drop precipitously while carbon dioxide spikes, leading to profound cerebral acidosis. This metabolic crisis initiates a massive release of endogenous neurotransmitters, including serotonin, dopamine, endorphins, and possibly DMT. This neurochemical flood hyper-excites key brain regions before they shut down. Specifically, the abnormal activation of the temporoparietal junction (TPJ) generates the out-of-body sensation, while the neurotransmitter surge produces the intense visual hallucinations, the overwhelming sense of peace, and the profound feelings of hyper-reality. By linking respiratory collapse to specific regional brain activations, the NEPTUNE model attempts to definitively ground the phenomenon in localized, neurocentric biology, dismissing non-local consciousness theories entirely 5375455.
Critiques of the Localized Brain Model
The publication of the NEPTUNE model was met with immediate, sweeping critiques from veteran researchers in the field, most notably Dr. Bruce Greyson and Dr. Marieta Pehlivanova of the University of Virginia. In late 2025, they published a rigorous, point-by-point rebuttal in the journal Psychology of Consciousness, systematically dismantling the argument that these episodes are mere biological malfunctions 484976.
Greyson and Pehlivanova argued that the NEPTUNE model achieves its comprehensive nature by selectively ignoring decades of robust empirical data that contradicts localized neurophysiology. The critique focused on several catastrophic failures in the materialist argument. First, they addressed the hypoxia paradox. While NEPTUNE claims low oxygen triggers the experience, clinical data demonstrates that patients reporting these episodes often possess normal or even higher blood oxygen levels - and lower carbon dioxide levels - than comparison patients who report nothing. Furthermore, true hypoxia reliably produces confusion, severe disorientation, amnesia, and fragmented agitation in patients. This directly contradicts the hyper-lucid, highly structured, cognitively complex, and permanently memorable nature of anomalous end-of-life episodes 484956.
Second, the critique dismantled the reliance on temporal lobe seizures and temporoparietal junction stimulation. While temporal lobe epilepsy does produce hallucinations, epileptic patients universally describe their seizures as frightening, bizarre, and fragmented; a comparative study of one hundred epilepsy patients found zero instances of experiences matching the serene, narrative consistency of a near-death episode. Similarly, while laboratory electrical stimulation of the TPJ can induce illusory bodily distortions - such as sensing a "shadow person" or feeling physically displaced - it has never successfully produced the accurate, 360-degree environmental perception reported in classic out-of-body states 485678.
Finally, the most critical flaw identified in the NEPTUNE model - and materialist models generally - is their complete inability to account for Apparent Veridical Perception (AVP). Dying patients with flatlined EEGs and no respiratory function have routinely reported highly specific events, complex conversations, and hidden medical details (such as the serial numbers of surgical instruments) that occurred during their resuscitation, which are later verified by medical staff. Endorphin releases and temporal lobe spasms, the critics argue, cannot logically impart accurate, veridical visual data to a clinically dead visual cortex. By ignoring AVP and encounters with deceased relatives unknown to be dead, the NEPTUNE model fails to explain the most perplexing and defining characteristics of the phenomenon 25484956.
Prospective Clinical Studies on Resuscitation Awareness
Recognizing the limitations of retrospective, anecdotal data, researchers have sought to move the field toward prospective, objective clinical testing within hospital environments. The most significant efforts in this direction are the AWARE (AWAreness during REsuscitation) investigations, spearheaded by Dr. Sam Parnia.
The AWARE I and AWARE II Investigations
AWARE I, published in 2014 in the journal Resuscitation, established a multi-center protocol across Europe and North America to test for conscious awareness and veridical out-of-body perception during cardiac arrest. The study utilized innovative experimental methods, placing distinct images on shelves visible only from an elevated vantage point near the ceiling in resuscitation rooms, aiming to objectively test claims of floating above the body. While the study confirmed that consciousness could persist during cardiac arrest, the sample size of survivors who had out-of-body experiences in the specifically rigged rooms was too small to validate the hidden targets 137980.
Building on these findings, AWARE II (published in 2023) represented an unprecedented escalation in methodological rigor. A twenty-five-site, in-hospital study evaluated 567 cardiac arrest patients between 2017 and 2020. To test for veridical perception, AWARE II incorporated independent audio-visual testing. Headphones were placed on patients undergoing CPR, transmitting specific audio cues (the names of three fruits: apple, pear, banana) while a tablet projected randomly stored images to test both implicit and explicit learning. Simultaneously, researchers utilized cerebral oximetry (rSO2) to measure brain oxygenation and continuous real-time EEG to monitor brain function during the arrests 57825884.
The survival statistics highlight the severe difficulty of this research: of the 567 patients, only 53 (9.3%) survived to discharge, and 28 were clinically capable of completing the extensive interviews. Of those 28 survivors, 11 patients (39.3%) reported memories or perceptions suggestive of consciousness. The researchers classified these reports into four categories of Recalled Experience of Death (RED): CPR-induced consciousness, post-resuscitation experiences, dream-like experiences, and transcendent recalled experiences of death 578285.
While nobody correctly identified the hidden visual images (unsurprising given that only six patients reported a full transcendental experience), one patient successfully identified the auditory stimulus administered during CPR. Most remarkably, despite marked cerebral ischemia - with mean regional oxygen saturation at just 43% - the continuous EEG monitoring detected normal cortical activity, including delta, theta, and alpha waves, emerging as late as 35 to 60 minutes into the CPR effort 5784.
The AWARE II researchers concluded that consciousness, external awareness, and internal cognitive processes can indeed occur during prolonged cardiac arrest. The paradoxical emergence of normal EEG patterns during severe ischemia suggests that the dying brain may undergo a process of disinhibition, activating dormant neural networks that facilitate heightened lucidity precisely when standard executive function is offline 13805759.
Theoretical Models of Non-Local Consciousness
The persistent failure of purely physicalist theories - such as the Integrated Information Theory and Global Neuronal Workspace - to adequately explain the genesis of complex subjective experience during periods of severe brain inactivity has fueled a paradigm shift. Increasingly, researchers are turning toward non-local theories of consciousness to explain the anomalies documented in NDE research 6735.
The Receiver Paradigm
In physicalist models, consciousness is viewed as an emergent property of neuro-computational activity; the brain is a factory that manufactures the mind. In non-local frameworks, consciousness is posited as a fundamental property of the universe, akin to electromagnetism or gravity. The brain, under this paradigm, functions not as a generator, but as a highly sophisticated biological transceiver - a television set or antenna that tunes into, filters, and localizes a vast, non-local field of consciousness 22687.
Under the "receiver" paradigm, clinical death damages the physical receiver (the brain), but the broadcast signal (consciousness) remains entirely intact and, in fact, expands. Because the biological filter is removed, the consciousness is temporarily untethered, allowing for the perception of a wider reality. This model elegantly and effectively accounts for the continuity of memory, the paradoxical hyper-lucidity, and the occurrence of veridical out-of-body perceptions during flatline conditions, as the observing self is no longer restricted by the sensory limitations of the biological cortex 81087.
Quantum Mechanics and the Orch-OR Theory
The mechanics of how a physical brain might interact with a non-local consciousness field are highly speculative, but increasingly intersect with quantum physics. The most prominent theory in this domain is the Orchestrated Objective Reduction (Orch-OR) theory, developed jointly by Nobel laureate physicist Roger Penrose and anesthesiologist Stuart Hameroff 8889.
Orch-OR suggests that consciousness does not arise from the standard chemical synaptic connections between neurons, but rather from quantum state reductions occurring at a much deeper, sub-cellular level within microtubules - tiny, hollow structural proteins that form the cytoskeleton of brain neurons. Because quantum mechanics allows for phenomena like entanglement and superposition (where particles can be linked and exist in multiple states across vast distances), Orch-OR provides a theoretical mathematical framework for how consciousness could persist non-locally and survive the biological death of the physical body 78889.
Historically, physicists criticized Orch-OR by arguing that the warm, wet environment of the human brain would immediately destroy fragile quantum states, which usually require absolute zero temperatures to function in laboratory computers. However, in August 2024, a groundbreaking study published in the peer-reviewed journal eNeuro provided major biological evidence supporting the theory. Researchers at Wellesley College administered isoflurane (a general anesthetic) to rats. They discovered that when they simultaneously administered drugs that specifically stabilized the microtubules inside the rats' neurons, the rats remained conscious significantly longer under the anesthesia. By demonstrating that microtubule stability directly mediates the threshold of conscious awareness, the study revived the Orch-OR theory and strengthened the case that the brain's fundamental interface with consciousness operates on the level of quantum mechanics, leaving the door open for non-local survival 8889.
Conclusions
The scientific investigation of near-death experiences demonstrates that the human mind is capable of maintaining profound clarity, emotional depth, and complex narrative structure at the exact moment that supporting biological systems undergo catastrophic failure. While comprehensive materialist frameworks, such as the NEPTUNE model, have successfully mapped the neurochemical and electrophysiological correlates of the dying process - identifying gamma wave surges, endogenous DMT release, and temporal lobe volatility - they consistently fail to explain the most critical anomalies of the phenomenon. The hyper-lucidity, long-term transformational aftereffects, and verified instances of apparent veridical perception documented during periods of profound cerebral ischemia defy reductionist categorization.
As sophisticated clinical studies like AWARE II push the boundaries of real-time cerebral monitoring during cardiac arrest, and as advanced theories like Orch-OR begin to bridge the gap between neurobiology and quantum mechanics, anomalous end-of-life consciousness remains the ultimate frontier challenging the standard biological model of the mind. The persistence of structured awareness in the absence of cortical function mandates a fundamental expansion of scientific paradigms, suggesting that consciousness may not merely be a product of the brain, but a fundamental feature of the universe intricately interacting with it.