Jaw muscle tension and stress
Introduction to Bruxism and Masticatory Hyperactivity
The sensation of chronic jaw tightness is the primary clinical manifestation of masticatory muscle hyperactivity, a complex physiological condition broadly encapsulated by the term bruxism, along with its associated structural consequence, temporomandibular disorders (TMD). For decades, the biomedical understanding of bruxism was constrained by definitions that rigidly classified it either as a localized dental pathology or exclusively as a sleep disorder. The term itself, derived from the earlier description "la bruxomanie" by Pietkiewicz in 1907 and formally introduced as "bruxism" by Frohman in 1931, has undergone extensive semantic and clinical evolution 12.
Recent international consensus initiatives have fundamentally shifted this diagnostic paradigm. In a landmark 2024 closed workshop convened during the General Session & Exhibition of the International Association for Dental, Oral and Craniofacial Research (IADR), a consortium of global bruxism experts updated the diagnostic definitions to reflect contemporary physiological evidence 34. The resulting 2025 consensus report explicitly removes the historical addendum "in otherwise healthy individuals" to avoid clinical confusion, and it officially recognizes bruxism not as an inherent disorder or pathology, but as a specific motor behavior 4567.
This motor behavior is divided into two distinct circadian manifestations based on the time of occurrence. Sleep bruxism is defined as masticatory muscle activity during sleep that is characterized as rhythmic (phasic) or non-rhythmic (tonic) 567. It is not classified as a movement disorder or a sleep disorder in itself, although it frequently co-occurs with conditions such as obstructive sleep apnea 27. Awake bruxism is defined as masticatory muscle activity during wakefulness characterized by repetitive or sustained tooth contact and by bracing or thrusting of the mandible 356.
Crucially, the consensus emphasizes that bruxism is a behavior that can act as a risk factor for negative clinical consequences, a neutral factor, or even a protective factor 5. For example, sleep bruxism may aid in maintaining upper airway patency in individuals with sleep apnea, stimulate salivation to neutralize gastroesophageal reflux, and potentially exert positive effects on cognitive function during sleep 259. However, when the frequency and intensity of this motor behavior exceed an individual's physiological adaptive capacity, it transitions from a benign motor habit into a pathophysiological state 7. This state results in the chronic jaw tightness, muscular fatigue, and pain reported by patients.
The etiology of this masticatory hyperactivity is highly multifactorial, encompassing genetic predisposition, central nervous system mechanisms, and autonomic nervous system fluctuations 78. Despite this complexity, clinical research consistently identifies psychosocial stress, trait anxiety, and emotional dysregulation as the primary drivers of awake bruxism and major contributing factors to sleep bruxism 9101112. To understand why the jaw is consistently tight in the presence of psychological stress, it is necessary to examine the specific neuroanatomical pathways, autonomic nervous system responses, and localized hemodynamic shifts that tightly couple emotional arousal to the masticatory system.
Neurobiological Architecture of Stress-Induced Tension
The correlation between psychological stress and masseter overactivity is mediated by complex central nervous system circuitry that translates emotional distress into physical motor output. Recent neurobiological studies utilizing animal models of chronic restraint stress have elucidated the specific brainstem and limbic system pathways responsible for this phenomenon, proving that jaw tension is a direct neurological reflex to psychological strain.
The Amygdala-Brainstem Axis and Motor Excitation
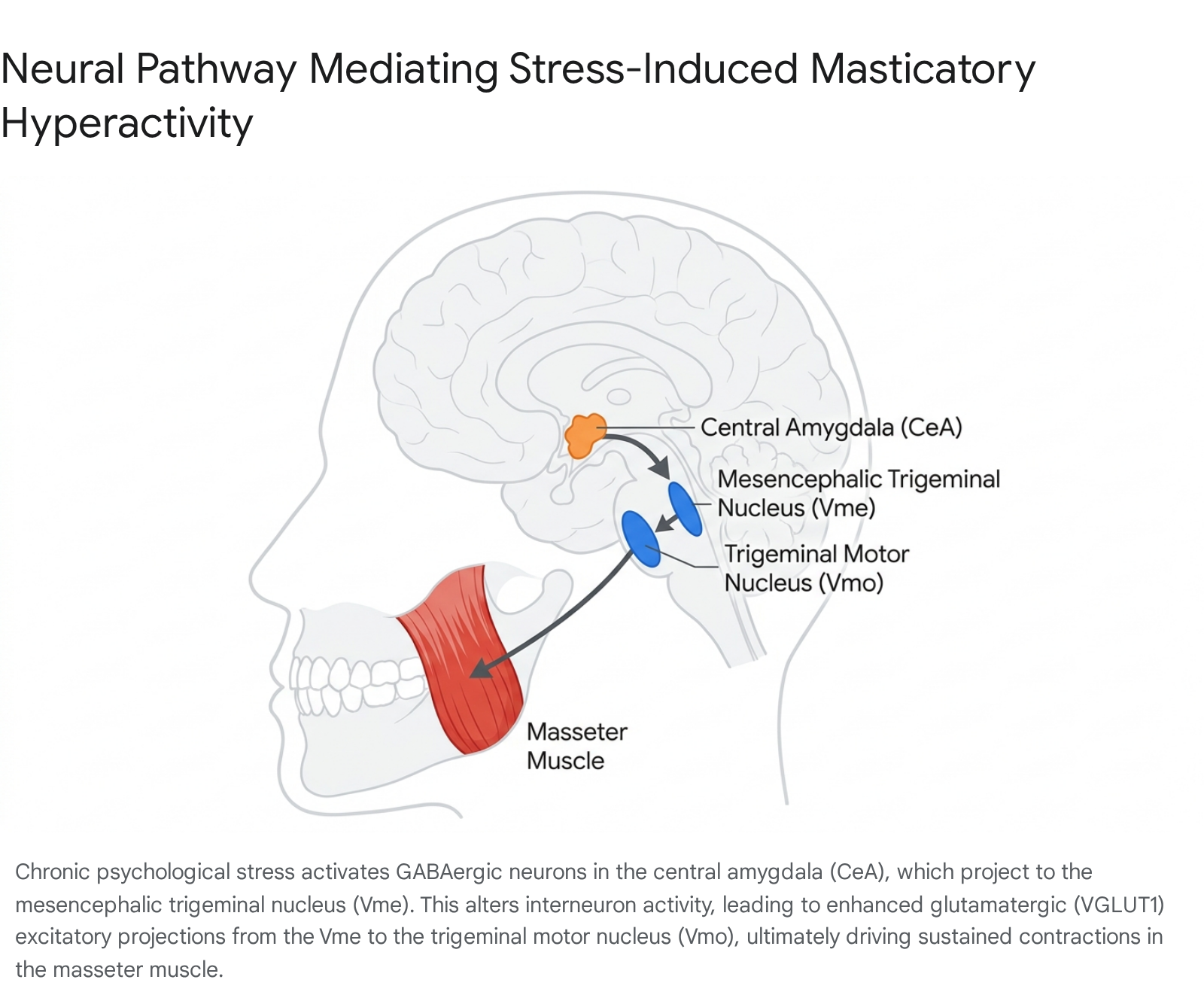
The central amygdala is a primary limbic structure responsible for processing stress-induced emotions and anxiety-related behaviors 13. Research indicates that the central amygdala projects directly to the mesencephalic trigeminal nucleus, a structure located in the brainstem that acts as the primary afferent center for masticatory proprioception 13141516. The mesencephalic trigeminal nucleus is highly unique because it contains primary sensory neurons within the central nervous system itself, and it plays a critical role in oral-motor coordination by projecting directly to the trigeminal motor nucleus, which provides the actual motor innervation to the jaw-closing muscles, including the masseter and temporalis 1416.
Under conditions of chronic stress, there is a marked activation of GABAergic neurons within the central amygdala. Tracing studies combined with immunofluorescence staining have revealed that these GABAergic projections terminate on interneurons within the mesencephalic trigeminal nucleus 13. The stress-induced alteration of these inhibitory signals paradoxically enhances the electrophysiological excitability of the primary pseudounipolar excitatory neurons in the mesencephalic trigeminal nucleus 131417.
Once these neurons become hyperexcitable due to chronic stress, they increase their output to the trigeminal motor nucleus via vesicular glutamate transporter 1-positive glutamatergic projections 141516. The enhanced glutamatergic excitatory neurotransmission from the mesencephalic trigeminal nucleus to the trigeminal motor nucleus directly drives the overactivity of the masseter muscle. Experimental models subjecting mice to chronic restraint stress for fourteen days demonstrated that stress not only elevates the expression of vesicular glutamate transporter 1 in the trigeminal motor nucleus but also upregulates choline acetyltransferase, leading to sustained masticatory muscle contractions analogous to human teeth clenching and bruxism 141516. When researchers experimentally suppressed the GABAergic projections from the central amygdala to the mesencephalic trigeminal nucleus via optogenetics, or administered targeted short hairpin RNA into the mesencephalic trigeminal nucleus, the stress-induced masseter hyperactivity was significantly attenuated, confirming this specific neural circuit as a primary driver of stress-induced jaw tension 131416.
Autonomic Arousal and Noradrenergic Pathways
In addition to direct somatomotor excitation, psychological stress profoundly influences the autonomic nervous system, triggering a cascade of physiological changes associated with heightened arousal. Noradrenergic neurotransmission in the brainstem is closely coupled with changes in muscle activity across the sleep-wake cycle, with noradrenaline acting as a key excitatory neuromodulator that reinforces arousal-related stimuli on motoneurons to drive movement 18.
During wakefulness, both endogenous glutamatergic and noradrenergic drives at the trigeminal motor pool are elevated, resulting in heightened motor activity and muscle tone 18. The perfusion of specific neuropharmacological agents into the trigeminal motor nucleus demonstrates that alpha-1 noradrenoceptor activation increases motoneuron responsiveness to excitatory glutamate receptor-mediated inputs during natural behavior 18. Conversely, entry into sleep, particularly rapid eye movement sleep, is normally characterized by an absence of endogenous alpha-1 noradrenoceptor activity, leading to a profound suppression of masseter muscle tone 18.
However, in individuals with sleep bruxism, periodic autonomic micro-arousals disrupt this physiological suppression. These arousals lead to transient spikes in noradrenergic drive, which subsequently cause rhythmic or non-rhythmic masticatory muscle contractions despite the individual remaining asleep 1819. This mechanism explains why stress - which raises the baseline tone of the sympathetic nervous system and increases the frequency of sleep arousals - directly correlates with the severity of nighttime teeth grinding.
Hemodynamic and Vascular Responses in Masticatory Muscles
The vascular response of the head and jaw muscles to sympathetic arousal differs significantly from the well-documented responses of limb muscles, providing further insight into why the jaw feels chronically tight. During acute mental stress tasks, systemic sympathetic nervous system activity increases, leading to a predictable rise in arterial blood pressure, heart rate, and overall cardiac output 2021. In typical skeletal muscles in the limbs, this sympathetic arousal generally induces marked vasoconstriction to redirect blood flow to vital organs.
However, studies utilizing near-infrared spectroscopy to measure tissue oxygenation and hemoglobin indices have demonstrated that the temporalis and masseter muscles do not exhibit a vasoconstrictive response to mental stress 2021. When healthy subjects were exposed to a randomized series of stressors - including cold pressor tests, mental arithmetic tests, apnea, and isometric handgrip exercises - tissue oxygenation indices significantly increased in both the masseter and temporalis muscles 202122. This suggests an increase in local muscle blood flow and vasodilation.
This specific sympathetic control of the head muscles is theorized to be an evolutionary adaptation related to the involvement of the jaw in aggressive or defensive reactions, physiologically preparing the masticatory muscles for immediate and sustained action during a threat 202122. While electromyographic activity in the temporalis muscle tends to increase sharply alongside sympathetic nervous activity during mental stress, the masseter muscle often shows profound and persistent hemodynamic changes without exhibiting large, continuous spikes in integrated electromyographic activity 172324. The persistent increase in tissue oxygenation and altered hemodynamics in the masseter muscle during long-lasting mental stress implies that the jaw muscles are uniquely and continuously metabolically engaged by psychological strain, providing a foundation for the etiology of stress-associated jaw muscle fatigue and dysfunction 172324.
Clinical Distinctions: Awake Bruxism, Sleep Bruxism, and Temporomandibular Disorders
While patients commonly report the generalized symptom of a tight jaw, clinical diagnosis requires distinguishing between three distinct but frequently overlapping phenomena: awake bruxism, sleep bruxism, and temporomandibular disorders. These entities share common clinical manifestations - such as masticatory muscle pain, restricted jaw mobility, and tension headaches - but they possess different etiologies, pathophysiological mechanisms, and required management protocols.
Awake Bruxism Phenotype
Awake bruxism is predominantly characterized by muscle bracing, sustained tooth contact, and jaw thrusting, rather than the loud, rhythmic grinding commonly associated with nighttime events 12. The introduction of ecological momentary assessment strategies, utilizing smartphone technologies to collect data on the frequency of muscle activities reported by individuals in their natural environment, has reshaped clinical understanding 12. These assessments reveal that true forceful teeth clenching and grinding during the day are much less frequent than previously believed; instead, sustained muscle bracing and light tooth contact are the primary behaviors 512. Awake bruxism is heavily correlated with individual psychological traits, specifically perceived stress, trait anxiety, and concentration, acting as a subconscious coping mechanism for emotional dysregulation 122528.
Sleep Bruxism Phenotype
Sleep bruxism is classified as a behavior characterized by rhythmic (phasic) or non-rhythmic (tonic) masticatory muscle activity during sleep 5710. It is strongly associated with sleep architecture variations, autonomic arousals, and respiratory conditions such as obstructive sleep apnea 7192627. Additionally, sleep bruxism is frequently triggered or exacerbated by the use of certain medications, particularly selective serotonin reuptake inhibitors used for depression and anxiety, as well as by the consumption of substances such as alcohol, tobacco, and caffeine 2627. Unlike awake bruxers, patients with sleep bruxism are typically entirely unconscious of the behavior and rely on reports from sleep partners regarding grinding noises or the presentation of morning symptoms such as severe tooth wear and jaw stiffness 2528.
Temporomandibular Disorders
Temporomandibular disorders are not a behavior, but an umbrella term for a structural and functional pathology affecting the temporomandibular joint, the masticatory muscles, or both 92531. The condition encompasses internal derangements (such as articular disc displacement), degenerative joint disease (osteoarthritis), and myofascial pain 9312829. While bruxism involves motor activity, temporomandibular disorders involve structural dysfunction and chronic pain. The two are inextricably linked; bruxism is considered a major risk factor for the development of temporomandibular disorders 92730. The sustained mechanical overload from chronic bruxism can result in joint inflammation, cartilage wear, and muscle spasms, culminating in the sharp joint pain, earaches, and restricted mouth opening characteristic of clinical temporomandibular pathology 9252831.
| Clinical Feature | Awake Bruxism | Sleep Bruxism | Temporomandibular Disorders (TMD) |
|---|---|---|---|
| Classification | Motor Behavior 3631 | Motor Behavior 3631 | Musculoskeletal / Neuromuscular Disorder 92531 |
| Primary Muscle Activity | Sustained muscle bracing, resting tooth contact, jaw thrusting 512 | Rhythmic (phasic) grinding, non-rhythmic (tonic) clenching 5726 | Variable; often involves chronic myofascial spasms or reflex splinting 313032 |
| Primary Drivers / Etiology | Psychosocial stress, trait anxiety, concentration, emotional dysregulation 122526 | Autonomic micro-arousals, sleep apnea, genetics, SSRIs, substance use 7192627 | Mechanical overload, joint trauma, malocclusion, prolonged bruxism, arthritis 9253133 |
| Hallmark Symptoms | Daytime muscle fatigue, tension headaches, indentations on tongue/cheeks 2528 | Partner reports of grinding sounds, severe tooth wear/fractures, morning jaw stiffness 192528 | Jaw clicking/popping, restricted mouth opening (lockjaw), sharp joint pain, earaches 252831 |
| Patient Awareness | Often subconsciously used as a coping mechanism; patient may be prompted to notice it 28 | Unconscious; patient is typically unaware until informed by a partner or dentist 2528 | Highly aware due to localized pain, functional restriction, or joint noise 2531 |
Global Epidemiology of Bruxism and Temporomandibular Disorders
The prevalence of bruxism and its structural consequences represent a significant global public health concern, with substantial variations based on geography, demographic factors, and ambient societal stress levels.
Population Prevalence of Circadian Manifestations
A comprehensive 2024 meta-analysis encompassing data extracted from 30 studies and 37,680 participants across multiple continents estimated the pooled global prevalence of bruxism (combining sleep and awake states) at 22.22%, with a 95% confidence interval ranging from 19.59% to 25.11% 1333435. When disaggregated by circadian manifestation, the global prevalence of awake bruxism is estimated at 23%, slightly higher than the global prevalence of sleep bruxism at 21% 13436. Notably, when occurrence is based strictly on objective polysomnography rather than self-reporting, the estimated prevalence of sleep bruxism rises significantly to 43% 13436.
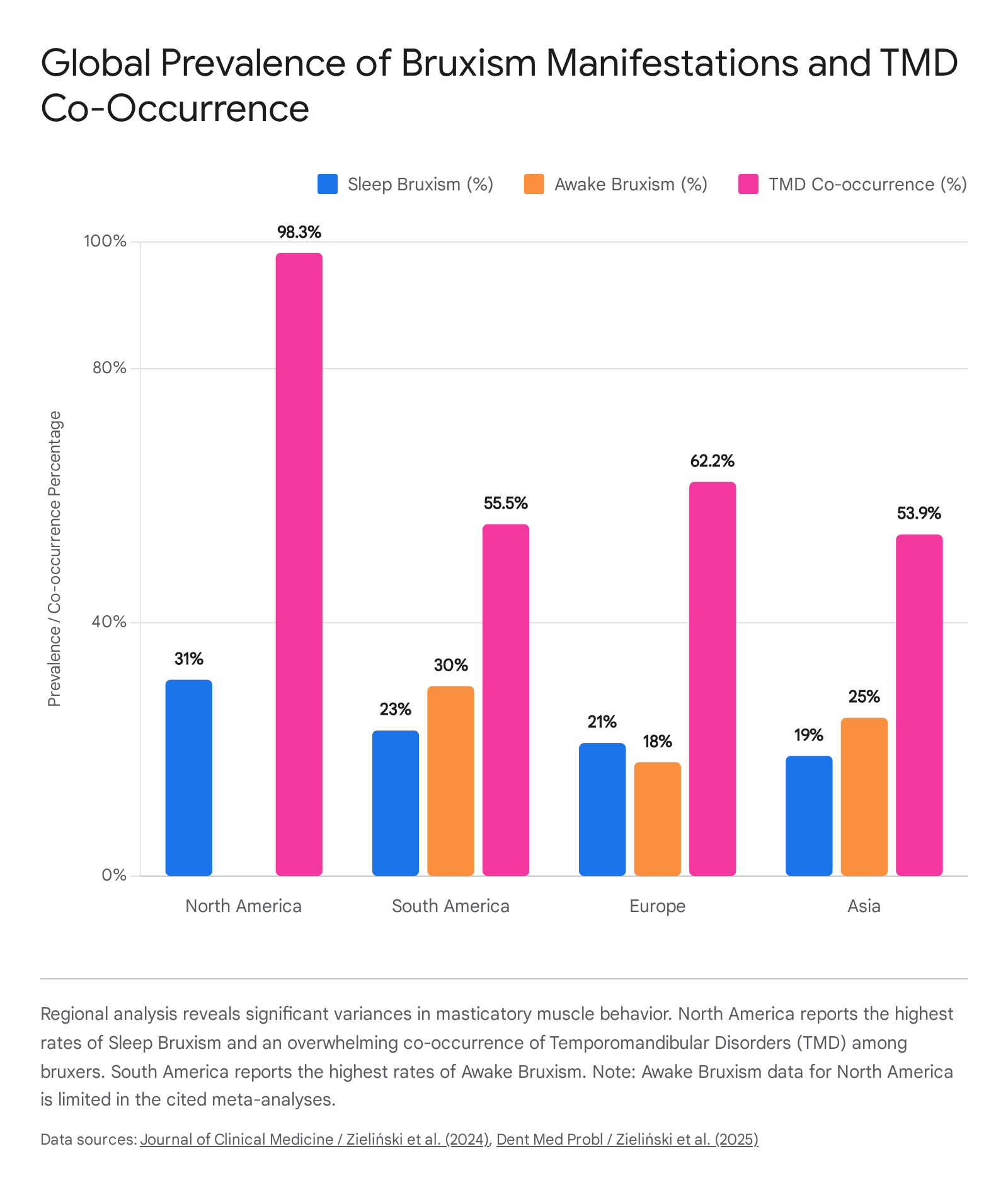
Geographical variations in bruxism prevalence are striking and suggest complex interactions between cultural environmental factors, diagnostic criteria, and population stress levels. North America exhibits the highest prevalence of sleep bruxism at 31%, followed by South America at 23%, Europe at 21%, and Asia at 19% 13436. Conversely, the prevalence of awake bruxism is highest in South America at 30%, followed by Asia at 25% and Europe at 18% 13436.
Co-occurrence of Bruxism and Temporomandibular Disorders
The co-occurrence of bruxism and temporomandibular disorders further highlights the profound clinical burden of masticatory hyperactivity. A 2025 meta-regression analysis found that the global co-occurrence of bruxism and temporomandibular disorders is approximately 17% in the general population 333537. However, among individuals already diagnosed with bruxism, the overall prevalence of comorbid temporomandibular disorders escalates dramatically to 63.5% 333537.
Regional disparities in this comorbidity are severe. In North America, a staggering 98.3% of bruxism patients present with concurrent temporomandibular disorder symptoms 333537. This prevalence drops to 62.2% in Europe, 55.5% in South America, and 53.9% in Asia 37.
Demographic factors also heavily influence susceptibility to these conditions. Female populations are significantly more vulnerable; statistical analyses reveal that for every 1% increase in the proportion of female participants in a study sample, the probability of bruxism and temporomandibular disorder co-occurrence rises by 4.4%, underscoring a distinct gender vulnerability to stress-induced masticatory dysfunction 333537. This vulnerability is further supported by studies demonstrating that stress significantly reduces burst frequency and wave peak values in the masseter muscle of males, while females and highly anxious individuals exhibit increased integral muscle activity with rising stress 38.
Pandemic-Induced Exacerbation of Masticatory Hyperactivity
The intrinsic link between psychological stress and jaw tension was heavily illuminated during the COVID-19 pandemic, which acted as an unprecedented global natural experiment on mass psychogenic stress.
During the pandemic, dental practices and organizations such as the American Dental Association reported a dramatic surge in stress-related oral health conditions, a phenomenon colloquially termed "COVID clenching" 433940. By late 2020, 59.4% of surveyed dentists noted an increased prevalence of bruxism among their patients, alongside a 53.4% increase in chipped and cracked teeth, and a 53% rise in temporomandibular joint disorder symptoms 433940. By 2021, over 70% of dentists reported an increase in patients experiencing teeth grinding and clenching conditions 43.
This surge was driven by profound disruptions in psychological homeostasis. Factors such as social isolation, health anxieties, and economic instability generated massive systemic stress, increasing the secretion of stress-related hormones and exacerbating emotional disorders 39. Furthermore, the loss of structured routines - blurring the lines between the home and the workplace - fostered environments ripe for passive, continuous anxiety 39. This psychological distress resulted in increased occurrences of daytime muscle bracing and an exacerbation of nocturnal grinding events 433941. Studies evaluating the psychological status of populations during this period found that nearly 50% of subjects reported increased bruxism, and up to 36% reported an increase in actual temporomandibular joint pain 39. The persistence of these elevated baseline prevalence rates into subsequent years demonstrates that once stress-induced masticatory hyperactivities are established, they often require active, targeted intervention to resolve 114041.
Diagnostic Frameworks and Clinical Assessment Protocols
Proper management of jaw tension requires accurate assessment, which is frequently complicated by the fact that many patients are entirely unaware of their bruxing habits, particularly during sleep. To standardize clinical research and practice, the international consensus established a diagnostic grading system to determine the validity of a bruxism diagnosis: * Possible Bruxism: This diagnosis is based solely on a positive patient self-report, often captured via questionnaires or clinical history regarding perceived teeth grinding or jaw clenching 63141. * Probable Bruxism: This diagnosis is based on positive clinical inspection, with or without a concurrent positive self-report. Pathognomonic clinical signs include observing excessive tooth wear facets on chewing surfaces, hypertrophy of the masseter or temporalis muscles, indentations on the tongue or buccal mucosa, or temporomandibular joint crepitus 64248. * Definite Bruxism: This definitive diagnosis requires positive instrumental assessment. For sleep bruxism, this traditionally mandates video-polysomnography combined with electromyography. For awake bruxism, a definite diagnosis relies on ambulatory electromyographic recordings taken during the day 63041.
Given the logistical and financial constraints of polysomnography, the clinical field is increasingly relying on standardized assessment tools such as the Standardized Tool for the Assessment of Bruxism and ecological momentary assessment via smartphone applications 712. Ecological momentary assessment prompts patients at random intervals during the day to record the current state of their jaw muscles, providing a highly accurate, real-time picture of awake bruxism frequencies without the recall bias inherent to traditional retrospective questionnaires 12.
Evidence-Based Management and Therapeutic Interventions
Management of masticatory muscle tension relies on a tiered, multidisciplinary approach. Because bruxism is a motor behavior regulated by the central nervous system and influenced heavily by psychosocial factors, treatments aimed solely at the teeth or the temporomandibular joint without addressing the underlying neuromuscular and psychological drivers are often incomplete. Clinical consensus dictates that if bruxism is asymptomatic, it does not strictly require treatment; however, when it results in chronic jaw tension, pain, or structural damage, intervention is mandatory 57.
Cognitive Behavioral Therapy and Psychosocial Management
Given that anxiety and emotional stress are primary etiologies for awake bruxism and major contributors to sleep bruxism, psychosocial interventions are considered first-line conservative therapies 112949.
Cognitive behavioral therapy aims to restructure maladaptive thought patterns, reduce trait anxiety, and equip patients with functional stress-coping mechanisms 434445. A 2024 meta-analysis evaluating the efficacy of cognitive behavioral therapy in managing temporomandibular disorders and bruxism reviewed data from numerous randomized controlled trials. The analysis found that psychological interventions significantly improved pain metrics, reduced jaw function impairment from 55% to 20%, and decreased overall catastrophizing and anxiety levels 434445. Cognitive behavioral therapy is highly effective at improving a patient's proprioceptive awareness of oral parafunctional habits; by training patients to notice when they are subconsciously bracing their jaw or clenching during stressful tasks, they can actively command the muscles to relax, thereby breaking the cycle of sustained awake bruxism 4943.
In modern practice, cognitive behavioral therapy is frequently combined with biofeedback therapy. Biofeedback utilizes surface electromyography sensors placed on the masseter or temporalis muscles. When the sensors detect muscle activity exceeding a certain threshold, the device alerts the patient via auditory, visual, or vibratory stimuli 191048. Over several weekly sessions, patients learn to consciously modulate their autonomic and motor responses to stress. Studies show that biofeedback combined with cognitive behavioral therapy yields an approximate 45% reduction in pain intensity and disability, an efficacy rate comparable to traditional occlusal splints but with the added benefit of addressing the root behavioral cause 43. Furthermore, integrating psychological therapies with physical therapy interventions - such as supervised jaw stretching, postural correction, and manual trigger point massage - provides immediate symptomatic relief for the musculature while the behavioral therapy addresses the long-term central nervous system triggers 294849.
Occlusal Splint Therapy: Mechanisms and Misconceptions
Occlusal splint therapy - encompassing devices known as night guards, bite plates, or stabilization splints - remains the most widely prescribed dental intervention for managing jaw tension, bruxism, and temporomandibular disorders 424647. A hard, full-coverage acrylic stabilization splint acts as a physical barrier between the maxillary and mandibular dental arches.
The primary clinical benefit of an occlusal splint is the rational redistribution of occlusal forces across the dentition and the protection of the teeth and prosthetic restorations from severe mechanical wear, fractures, and trauma 19464849. In cases of myogenous temporomandibular disorders, splints provide an artificial, balanced occlusal platform that temporarily alters proprioceptive feedback to the brain, frequently inducing relaxation in the masseter and temporalis muscles and providing significant short-term pain relief and improved mouth opening 485750.
However, there is a pervasive misconception in both clinical practice and public understanding that an occlusal splint "cures" or stops the physiological act of bruxism 4951. Current neurophysiological evidence indicates that occlusal splints do not eliminate the central motor commands driving bruxism. While the initial insertion of a new splint often results in a transient decrease in electromyographic muscle activity during sleep, this effect is largely due to the novelty of a foreign object altering the oral environment. After approximately two weeks of continuous use, neuroplastic adaptation occurs, and the frequency and intensity of sleep bruxism episodes typically return to their original baseline levels 424649. In some patients, poorly designed or generic splints can actually exacerbate muscle tension by destabilizing the jaw or reducing the necessary freeway space between the dental arches, worsening the structural symptoms 4251.
Optimal splint design is critical for therapeutic success. Recent literature indicates that flat, hard stabilization splints with a moderate thickness of 3 to 5 mm in the molar region provide the most optimal balance of joint decompression and muscle relaxation for the majority of patients 2832. Splints with a thickness of 2 mm or less are generally insufficient for addressing joint components in early-stage internal derangements, while splints thicker than 6 mm frequently cause patient discomfort and reduced compliance 28. Furthermore, soft thermoplastic splints - while sometimes preferred by patients for immediate comfort - are generally contraindicated for chronic bruxers. The resilient material can paradoxically stimulate the urge to chew or clench, potentially increasing masseter electromyographic activity rather than decreasing it 3252.
Crucially, occlusal splints are strictly contraindicated for patients whose sleep bruxism is secondary to obstructive sleep apnea. A traditional occlusal splint may inadvertently cause the mandible to drop backward during sleep, further narrowing the upper airway and severely exacerbating apneic events 1953. In patients presenting with both sleep bruxism and obstructive sleep apnea, a mandibular advancement device is the required intervention; this specialized oral appliance pulls the lower jaw forward to maintain airway patency, addressing the primary respiratory disorder while simultaneously reducing bruxism motor activity 1953.
Pharmacological Interventions and Neuromodulation
When conservative behavioral therapies and occlusal appliances fail to manage severe jaw tension and pain, pharmacological interventions may be integrated into the treatment plan.
For acute flare-ups of masticatory muscle spasm, short courses of muscle relaxants or non-steroidal anti-inflammatory drugs are appropriate for immediate symptomatic relief 114247. For chronic, refractory cases heavily influenced by stress and altered pain processing, neuromodulatory medications are considered. Low-dose tricyclic antidepressants, such as Amitriptyline, are often utilized as first-line pharmacologic agents for chronic orofacial pain, owing to their ability to modulate descending pain pathways and improve sleep architecture 42. Anticonvulsants like Gabapentin may also be employed for their neuropathic pain-relieving properties 42. While benzodiazepines like Clonazepam significantly reduce the bruxism index by suppressing central motor output, their high risk for dependency and tolerance strictly limits their use to very short-term applications under close medical supervision 942.
In recent years, the intramuscular injection of Botulinum Toxin Type A (commonly referred to as Botox) into the masseter and temporalis muscles has emerged as a highly effective intervention for severe, treatment-resistant bruxism and masticatory hypertrophy 9192947. Botulinum toxin acts by temporarily inhibiting the release of acetylcholine at the neuromuscular junction, inducing a localized, reversible muscle paralysis. While these injections do not address the central psychological stress or alter the frequency of central motor events driving sleep bruxism, they significantly decrease the physical strength of the jaw muscle contractions 19. By chemically weakening the masseter, the toxin dramatically reduces the mechanical force applied to the teeth and the temporomandibular joint, providing profound relief from chronic jaw tightness, functional limitations, and tension headaches for approximately three to six months per treatment cycle 1947. Additionally, complementary therapies such as low-level laser therapy (photobiomodulation) are increasingly utilized as non-invasive alternatives to reduce localized muscle activity and alleviate pain associated with temporomandibular disorders 294748.
Conclusion
Chronic jaw tightness is rarely an isolated biomechanical issue; rather, it is a complex behavioral and physiological manifestation of psychological stress. The central nervous system pathways linking the emotional processing centers of the amygdala directly to the motor nuclei controlling the jaw dictate that the masticatory system is exceptionally vulnerable to psychosocial strain. As demonstrated by the unprecedented surge in bruxism during the COVID-19 pandemic, ambient anxiety and psychological distress readily translate into sustained awake muscle bracing and rhythmic nocturnal grinding.
Effectively managing this tension requires moving beyond the misconception that dental splints provide a complete cure for the behavior itself. While correctly fabricated occlusal appliances are essential for protecting the dentition and temporarily unloading the temporomandibular joint, long-term resolution requires addressing the underlying neurological and psychological drivers. A multidisciplinary approach that integrates cognitive behavioral therapy to restructure stress responses, biofeedback to build proprioceptive awareness, physical therapy for localized muscle relief, and, when necessary, targeted pharmacotherapy or neuromodulation, offers the most comprehensive pathway to alleviating stress-induced masticatory hyperactivity.