How Often Should You Exercise to Live Longer
For optimal longevity, the scientific consensus indicates that adults should accumulate 150 to 300 minutes of moderate-to-vigorous physical activity per week, ideally structured around a foundation of Zone 2 aerobic training combined with two weekly sessions of resistance exercise. While the myth that extreme exercise volumes severely damage the heart has been refuted by recent mega-cohorts revealing an asymptotic mortality curve, exceeding 300 minutes weekly yields diminishing returns for pure lifespan extension. Ultimately, establishing consistent movement patterns that preserve lean muscle mass and cardiovascular efficiency offers the most profound biological defense against all-cause mortality.
The Architecture of an Active Lifespan: Weekend Warriors Versus Daily Gym-Goers
In contemporary society, physical activity profiles frequently bifurcate into distinct behavioral archetypes defined by the constraints of modern labor. On one end of the spectrum is the "weekend warrior" - a professional who remains largely sedentary from Monday to Friday due to occupational demands, only to engage in intense, prolonged bursts of physical exertion, such as a three-hour hike or back-to-back tennis matches, over a 48-hour period. On the other end is the "daily gym-goer," an individual who meticulously partitions their physical exertion into 45-minute daily sessions of structured cardiovascular and strength training. This behavioral dichotomy presents a complex physiological question: does the human body respond more favorably to the absolute cumulative volume of physical exertion, or to the daily consistency of the metabolic stimulus?
The pursuit of optimizing physical activity for longevity has evolved from broad public health recommendations into a nuanced science of precision medicine. Historically, exercise guidelines were generalized, focusing heavily on basic cardiovascular output without differentiating between the physiological adaptations induced by continuous versus intermittent metabolic stress. However, modern epidemiology, bolstered by accelerometer data and massive global cohorts spanning decades of observation, has provided unprecedented clarity on the dose-response relationship between human movement and mortality. Researchers have identified that physical activity interacts with human biology on a spectrum, governed by thresholds of minimum efficacy, optimal sweet spots, and definitive points of diminishing returns 123.
Recent data reveals that physical activity operates not merely as a mechanical stressor, but as a profound modulator of systemic biology. Contracting skeletal muscle acts as an endocrine organ, secreting signaling molecules that cross-talk with the brain, the cardiovascular system, and adipose tissue 12. Furthermore, geographically diverse studies from populations across the United States, Europe, and Asia demonstrate that the longevity premium associated with exercise is a universal human trait, though cultural and genetic variables influence the precise trajectory of these benefits 345. This report comprehensively evaluates the most current, top-tier scientific literature - prioritizing 2023 and 2024 umbrella reviews, mega-cohort studies, and meta-analyses - to decode the optimal exercise prescription for longevity.
Decoding the Metrics of Longevity
Before assessing specific exercise protocols, it is essential to define the standard metrics utilized in longevity research to quantify exertion, energy expenditure, and cardiovascular health. These abstract metrics form the foundation upon which epidemiological data is translated into actionable clinical advice.
The predominant metric for measuring exercise volume is the Metabolic Equivalent of Task (MET), typically expressed in MET-minutes or MET-hours per week. One MET represents the basal oxygen consumption of an individual at rest 4. Moderate physical activity (MPA), such as brisk walking or leisurely cycling, is generally classified at approximately 4 METs, while vigorous physical activity (VPA), such as running or competitive sports, operates at 8 METs or higher 4. The universally recognized baseline guideline for adults - 150 to 300 minutes of moderate exercise or 75 to 150 minutes of vigorous exercise per week - translates to an energy expenditure of approximately 500 to 1,000 MET-minutes per week 45. By converting duration and intensity into a singular MET-minute metric, researchers can accurately compare the longevity benefits of disparate activities, isolating the specific volume of metabolic work required to trigger systemic adaptations.
Beyond volume, maximal oxygen uptake (VO2 max) represents the peak capacity at which the heart, lungs, and muscles can effectively utilize oxygen during intense exercise. In contemporary preventive cardiology, VO2 max is widely considered the single strongest independent predictor of all-cause mortality, often superseding traditional risk factors such as smoking, hypertension, and hyperlipidemia 196. Observational data indicates that the risk of mortality for the least fit individuals (the bottom 20th percentile) is four-fold higher compared to extremely fit individuals 7. Furthermore, shifting from the lowest quartile of cardiorespiratory fitness to simply a below-average or average level yields the most dramatic reduction in mortality hazard 1. This metric is highly malleable through targeted cardiovascular training, specifically high-intensity interval training, which aggressively stimulates cardiac remodeling and mitochondrial proliferation 18.
While VO2 max represents peak capacity, Resting Heart Rate (RHR) serves as a continuous barometer of cardiovascular efficiency and autonomic nervous system balance. A healthy adult RHR typically ranges from 60 to 100 beats per minute (bpm), but optimal longevity is strongly associated with an RHR of 50 to 70 bpm 1. A comprehensive meta-analysis encompassing 46 studies demonstrated that an RHR consistently above 80 bpm significantly elevates the risk of all-cause mortality, with the hazard ratio increasing progressively for every 10 bpm increment 13. Conversely, individuals who maintain a stable or slightly declining RHR over their lifespan are 65% less likely to develop heart failure and 69% less likely to die from any cause 13. A lower RHR indicates that the myocardial tissue is robust and does not have to work as hard to maintain systemic perfusion, significantly reducing chronic mechanical stress on the vascular endothelium.
The Global Longevity Data Landscape
The profound impact of exercise on life expectancy is not an isolated phenomenon observed in specific demographics; it is a universally validated biological reality confirmed by some of the most extensive longitudinal studies in medical history.
The Copenhagen City Heart Study serves as a foundational pillar in this domain. This prospective population study tracked 17,589 healthy men and women aged 20 to 98 years over a maximum follow-up period of 35 years 3. The data revealed that joggers had an age-adjusted hazard ratio of death of 0.56 compared to non-joggers, corresponding to a massive survival increase of 6.2 years for men and 5.6 years for women 3. The baseline characteristics of the exercising cohort demonstrated lower body mass indices, lower resting heart rates, lower systolic blood pressure, and a significantly reduced incidence of diabetes 3.
Geographically diverse data further solidifies these findings. In China, the China Health and Retirement Longitudinal Study (CHARLS) evaluated 12,927 participants over the age of 50 4. The study categorized participants based on their Total Physical Activity (TPA), calculated by converting vigorous physical activity into equivalent moderate activity to achieve a standardized MET-minute score. Alarmingly, the data revealed that more than one-third of participants over the age of 50 never participated in any moderate or vigorous activity, highlighting a massive global deficit in physical movement 4. Similarly, cohort data regarding South Asian adults in the United States indicates that while they are as likely as White adults to engage in the baseline 150 to 300 MET-minutes per week of aerobic exercise, they are significantly less likely to reap the benefits of high-intensity exercise exceeding 300 MET-minutes, exposing a critical disparity in cardioprotective training intensity across populations 59.
In the United States, data from the Nurses' Health Study (encompassing nearly 80,000 participants) and the Health Professionals Follow-Up Study (44,000 participants) confirmed that achieving at least 30 minutes of moderate to vigorous physical activity daily extended life expectancy by 7 to 8 years 1. This massive accumulation of evidence from distinct global populations underscores that physical inactivity operates as an independent, primary driver of premature mortality, regardless of ethnic or geographic background.
The Minimum Effective Dose: Thresholds for Meaningful Protection
The foundational tier of the exercise-longevity spectrum is the minimum effective dose - the precise threshold where physical activity begins to generate statistically significant reductions in mortality compared to a completely sedentary baseline. The exercise-mortality curve is radically non-linear; the absolute steepest drop in mortality risk occurs in the transition from doing nothing to doing virtually anything 3.
For decades, public health messaging anchored heavily on the 150-minute weekly threshold, inadvertently creating a psychological barrier for chronically inactive populations who viewed the target as insurmountable. However, pooled data from six large cohorts encompassing 661,137 adults demonstrated that achieving just half of this recommendation - 75 minutes of moderate-intensity exercise per week, or roughly 11 minutes per day - yields a profound 20% reduction in all-cause mortality compared to inactivity 3. This initial investment captures the vast majority of the available longevity benefit.
The mechanics of this minimum effective dose are continually being refined. A 2022 study published in Nature Medicine utilizing accelerometer data from the UK Biobank identified that non-exercisers who engage in Vigorous Intermittent Lifestyle Physical Activity (VILPA) achieve massive survival benefits without ever stepping foot in a gym 9. Accumulating just three to four minutes of daily VILPA - such as sprinting up a flight of stairs or carrying heavy groceries, broken into one-to-two-minute bouts - is associated with an approximate 40% lower risk of all-cause and cancer-related mortality among individuals who otherwise do not exercise 9.
The widely propagated goal of 10,000 daily steps is similarly undergoing aggressive scientific recalibration. The 10,000-step metric originated not from physiological research, but from a 1965 Japanese marketing campaign for a commercial pedometer 3. Recent 2023 and 2024 umbrella reviews and meta-analyses have entirely redrawn the step-count thresholds. A meaningful protective threshold against cardiovascular disease and premature death begins as low as 3,100 to 4,000 steps per day 39. This establishes a highly accessible minimum effective dose for older adults, populations managing chronic morbidity, and those recovering from acute cardiovascular events.
While aerobic exercise targets systemic perfusion and mitochondrial health, resistance training is an absolute imperative for musculoskeletal longevity. As humans age, they experience a precipitous decline in muscle mass and power - a condition known as sarcopenia - driven by a blunted response to dietary protein (anabolic resistance) and a selective loss of fast-twitch Type II muscle fibers 810. A massive meta-analysis published in the British Journal of Sports Medicine revealed a J-shaped association for resistance training. The data established that a minimum effective dose of just 30 to 60 minutes of muscle-strengthening activity per week is associated with a 10% to 17% lower risk of all-cause mortality, alongside significant reductions in cardiovascular disease, total cancer incidence, and type 2 diabetes 16.
FAQ: Is More Exercise Always Better for a Long Life?
The narrative surrounding extreme physical exertion has historically been fraught with conflicting medical hypotheses. For years, the prevailing consensus in certain cardiology circles was governed by the "Extreme Exercise Hypothesis." This hypothesis suggested that the benefits of exercise existed on a strict U-shaped curve, positing that while moderate exercise protected the heart, extreme volumes of endurance training (e.g., marathons, ultramarathons, and Ironman triathlons exceeding 7 to 10 hours of intense cardio per week) caused cumulative cardiotoxicity. Proponents of the U-shaped curve warned that excessive volume increased the risk of myocardial fibrosis, coronary artery calcification, and potentially fatal arrhythmias 2.
However, an avalanche of rigorous 2023 and 2024 mega-cohort studies has systematically dismantled the U-shaped mortality curve in favor of an asymptotic, or "reverse J-shaped" and L-shaped, curve 711.
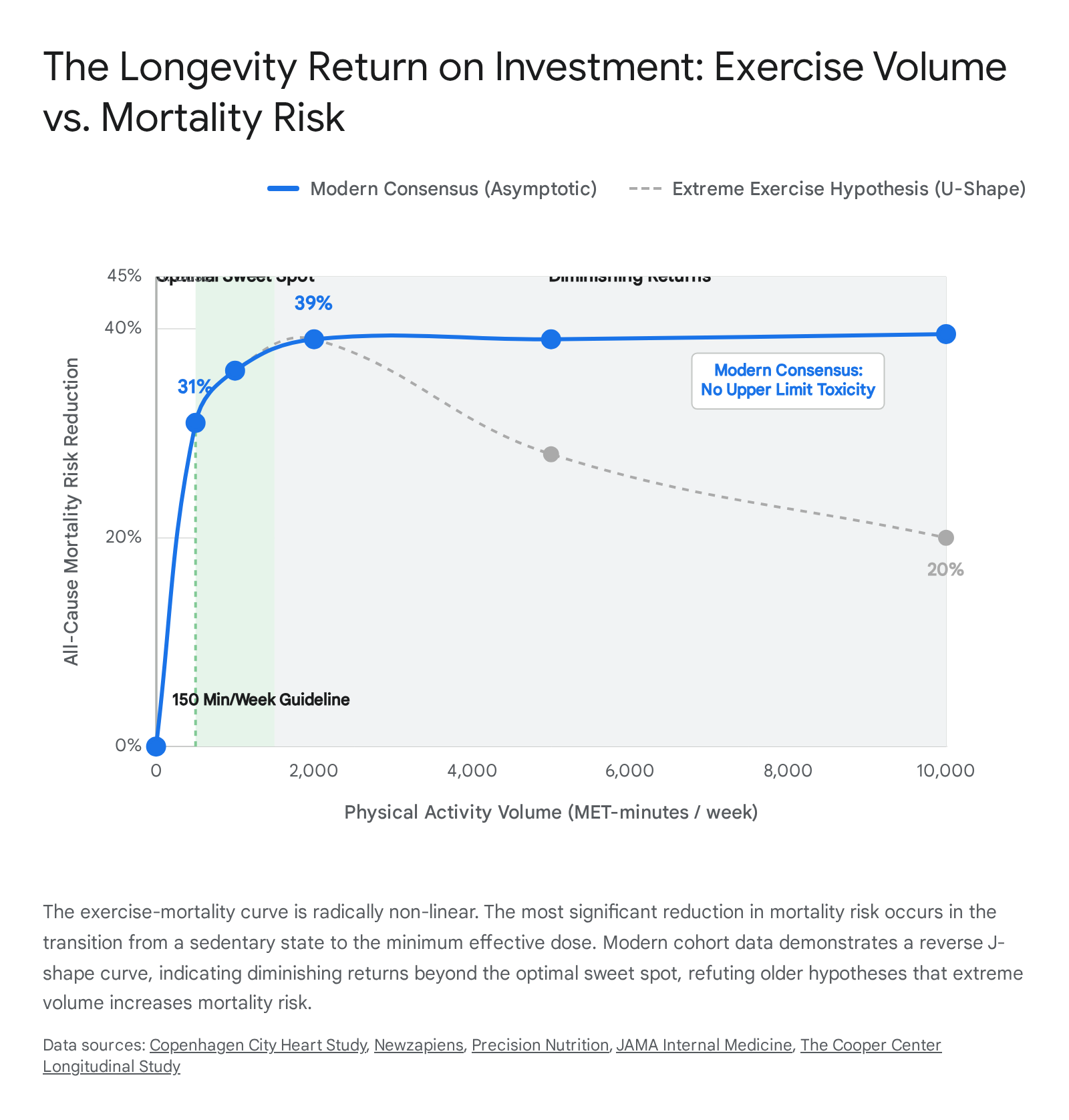
A landmark study published in Circulation, tracking 116,000 adults over 30 years, investigated the upper boundaries of physical activity. The researchers found no upper limit where exercise volume became objectively harmful regarding all-cause cardiovascular mortality 1. This was corroborated by another massive analysis of elite athletes engaging in extraordinary physical activity volumes (≥10,000 MET-minutes per week). Among these extreme exercisers, there was no observed increase in all-cause or cardiovascular mortality compared to those completing 3,000 MET-minutes per week; notably, none of the extraordinary volume athletes died of cardiovascular disease during the 10-year follow-up 6. Furthermore, a systematic review of 165,033 former elite athletes confirmed that those exposed to extreme, prolonged physiological stress actually lived longer and exhibited a lower incidence of cardiovascular disease than the general population 6.
Therefore, to definitively answer the question: more exercise is not inherently lethal, but it is not automatically "better" for extending the absolute limits of longevity.
Once an individual surpasses approximately 300 to 500 minutes of moderate-to-vigorous activity per week, they enter a profound zone of diminishing returns 13. Moving from 150 to 300 minutes yields a marginal 2% to 3% additional mortality reduction, and moving beyond 300 minutes yields virtually zero additional statistical lifespan extension 3. While the absolute upper limit of human tolerance remains contested within the highly specialized niche of extreme sports medicine - particularly regarding the elevated incidence of benign atrial fibrillation in older male endurance athletes engaging in lifelong marathon running 5 - the broader consensus confirms that exceeding public health guidelines is not fatal. It simply shifts the biological adaptation from "healthspan enhancement and disease prevention" to "elite athletic performance optimization," which are highly distinct physiological goals 618.
FAQ: Do Weekend Warriors Get the Same Benefits?
The modern reality of sedentary white-collar labor has given rise to the "weekend warrior" - individuals who compress their entire recommended 150 minutes of weekly moderate-to-vigorous activity into one or two highly concentrated sessions over the weekend. The physiological efficacy of this pattern, compared to the daily gym-goer, is a subject of intense scientific scrutiny and public interest.
From a strict mortality perspective, recent large-scale epidemiological data provides highly encouraging news. Analysis indicates that weekend warriors achieve remarkably similar reductions in all-cause and cardiovascular mortality compared to individuals who spread their exercise evenly throughout the week, provided the total weekly volume of metabolic effort is matched 1912. If the weekend warrior completes 150 minutes of intense hiking and cycling, their myocardium receives the necessary volumetric stimulus to drive critical adaptations in stroke volume, endothelial function, and vascular elasticity.
However, from a comprehensive metabolic and cardiometabolic standpoint, daily consistency holds a distinct and powerful physiological edge over sporadic intensity 3. The human body operates on continuous, highly sensitive metabolic cycles. Experimental studies demonstrate that uninterrupted sedentary behavior - sitting for 30 minutes or longer - acutely exacerbates postprandial cardiometabolic risk biomarkers. Prolonged sitting causes transient insulin resistance, impaired glucose tolerance, and drastically decreased vasodilatory function, as muscle lipoprotein lipase activity plummets during inactivity 131415.
Therefore, while the weekend warrior perfectly captures the macro-benefits of cardiovascular conditioning and avoids premature death, they remain highly vulnerable to the micro-damages of prolonged weekly sitting 1416. High cardiorespiratory fitness attenuates, but does not completely eliminate, the cardiometabolic risks associated with excessive daily sedentary time 9. Furthermore, daily exercise significantly influences Non-Exercise Activity Thermogenesis (NEAT) and helps regulate continuous circadian processes, making consistent, evenly distributed activity optimal for holistic healthspan and daily glycemic control, even if the ultimate mortality curves appear statistically similar 25.
FAQ: Zone 2 vs. Strength Training
The debate regarding the optimal modality of exercise for longevity has coalesced into a clear, evidence-based consensus: a bifurcated approach utilizing both low-intensity steady-state (Zone 2) cardio and progressive resistance training is absolutely essential. Neither modality can biologically replace the mechanisms of the other.
Zone 2 training is defined as steady, continuous exertion at a conversational pace, typically representing 60% to 70% of maximum heart rate. For longevity optimization, Zone 2 should comprise approximately 80% of an individual's cardiovascular routine 113. From a molecular perspective, Zone 2 is paramount because it exclusively targets and enhances mitochondrial density and function, driving mitochondrial biogenesis 118. Training in this specific zone maximizes the oxidative capacity of Type I (slow-twitch) muscle fibers and drastically improves the efficiency of lipid oxidation, training the body to utilize fat as a primary fuel source before relying on glucose 8. Furthermore, chronic Zone 2 training is the primary driver for lowering resting heart rate, increasing total blood volume, and driving vascular remodeling through capillarization, which collectively reduce the mechanical burden on the heart over decades 11317.
While Zone 2 builds the cardiovascular engine, strength training preserves the structural armor and acts as a profound metabolic sink. Resistance training independently reduces all-cause mortality risk by 10% to 17% 16. A 2025 study highlighted that regular resistance training can slow biological aging by nearly four years 1. As humans age, they succumb to sarcopenia and the infiltration of intramuscular adipose tissue (IMAT), which severely degrades muscle quality, strength, and insulin sensitivity 1810. Strength training directly combats this by stimulating muscle protein synthesis, reversing anabolic resistance, and preserving fast-twitch Type II fibers, which are the first to atrophy during the aging process 118.
Crucially, skeletal muscle is not merely a locomotive tissue; it is an active endocrine organ. During intense muscle contraction, the tissue secretes systemic signaling molecules known as myokines, such as irisin, Interleukin-6, and Metrnl 113. These myokines cross into the bloodstream, exerting profound anti-inflammatory, neuroprotective, and lipolytic effects throughout the body. Irisin, for example, is heavily linked to improved cognitive function and neurogenesis, while Metrnl improves glucose homeostasis and protects cardiac structure 1. Consequently, building muscle through resistance training is not merely about physical strength; it is about expanding the body's internal pharmacy to combat neurodegeneration and metabolic dysfunction.
The Optimal Sweet Spot and Sports Modalities
Moving beyond baseline disease prevention, the "optimal sweet spot" represents the precise volume and intensity of physical activity required to extract the absolute maximum physiological benefit for life extension. Mega-cohort data from the Harvard Alumni Health Study and subsequent 2023 meta-analyses suggest that the sweet spot for maximum mortality reduction resides strictly between 150 and 300 minutes of moderate aerobic activity, or 75 to 150 minutes of vigorous activity per week 1413. Within this tightly defined window, all-cause mortality is reduced by approximately 31% to 37% compared to entirely inactive populations 3.
For daily step counts, the optimal plateau for longevity occurs between 7,000 and 8,000 steps 925. Beyond 8,000 steps, the pure mortality benefits experience a sharp diminishing return. However, if the primary clinical goal is visceral fat reduction rather than simply extending baseline longevity, the optimal range shifts upward to 8,000 - 12,000 steps, heavily dependent on the introduction of deliberate intensity variations (such as incline walking, pace bursts, or zone 3 intervals) to continuously disrupt neuromuscular and metabolic optimization 25.
The specific modality of exercise performed within the optimal sweet spot profoundly influences the magnitude of life expectancy gains. The Copenhagen City Heart Study, a prospective population study following 8,577 adults for up to 25 years, evaluated the differential improvements in life expectancy associated with various sports. The findings were staggering: while all physical activity conferred an advantage over sedentary behavior, sports involving high social interaction and interval-based movement provided the greatest longevity gains.
Adjusted for multiple confounding variables including age, income, and education, the study found the following astonishing gains in life expectancy: * Tennis: +9.7 years * Badminton: +6.2 years * Soccer: +4.7 years * Cycling: +3.7 years * Swimming: +3.4 years * Jogging: +3.2 years * Health Club Activities (solitary gym workouts): +1.5 years 1919.
Researchers attribute this massive disparity to two interconnected biological and psychosocial factors. Physiologically, racket sports and soccer require intense interval bursts of high-intensity exertion utilizing large muscle groups and full-body movements in multiple planes of motion. This erratic, high-demand stimulation has proven superior for augmenting cardiorespiratory fitness and mitochondrial efficiency compared to steady-state continuous running 819. Psychologically, regular participation in highly interactive sports establishes a robust social support network. Belonging to a group that meets regularly promotes trust, commonality, and emotional well-being, directly counteracting the severe mortality risks associated with social isolation, loneliness, and chronic cortisol elevation 1919.
Contextualizing the "e572" Identifier in Exercise Literature
In bibliometric analyses, meta-research, and academic database queries concerning cardiovascular health and physical activity, the alphanumeric identifier "e572" frequently emerges. It is critical to clarify that "e572" does not refer to a specific biochemical marker, a genetic variant, or a clinical metric of fitness. Rather, it is the electronic pagination identifier for several highly cited, landmark medical publications that form the bedrock of current clinical guidelines regarding exercise, rehabilitation, and aging. Three specific papers share this pagination and are heavily relied upon in modern cardiology and gerontology:
1. The American Heart Journal (2011) - 162(4):571-584.e572 Authored by Lawler, Filion, and Eisenberg, this landmark systematic review and meta-analysis evaluated the efficacy of exercise-based cardiac rehabilitation following a myocardial infarction 202122. The study definitively proved that supervised exercise interventions post-heart attack reduce the hazard rate of all-cause mortality by a staggering 26% and cardiovascular mortality by similar margins 202123. The "e572" paper is a cornerstone of secondary prevention, proving that the cardiovascular benefits of physical activity remain incredibly potent even after severe cardiac damage has occurred, cementing exercise as a Class 1A medical intervention for cardiac cachexia and rehabilitation 2324.
2. The Gerontologist (2020) - 60(8):e572-e582 Authored by Copeland et al., this critical paper analyzed the intersection of sedentary behavior, aging trajectories, and interventions designed to promote physical activity in older adults 16252627. The findings contextualized how physical literacy and environmental factors influence healthspans, validating that interrupting sedentary behavior with even light-intensity activity mitigates severe cardiometabolic risks in elderly populations 162528.
3. Circulation (2019) - 140:e563-e595 (Referencing e572 specifically) The 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease utilizes the e572 pagination to outline clinical statements on lifestyle factors affecting cardiovascular risk 29. This specific section reinforces that achieving exercise recommendations is crucial for primary prevention and details the complex interplay between diet, exercise, and metabolic syndrome.
Together, these "e572" identified papers provide the scientific scaffolding that bridges primary longevity (preventing disease in healthy adults) with secondary longevity (rehabilitating the cardiovascular system and managing frailty in advanced age).
Translating Abstract Metrics into Actionable Weekly Routines
To optimize healthspan in the real world, abstract metrics like MET-minutes, relative hazard ratios, and mitochondrial biogenesis must be distilled into pragmatic, actionable schedules that accommodate varying levels of fitness and available time. The following routines synthesize the data on minimum doses, sweet spots, and optimal modalities.
Level 1: The Minimum Effective Dose (The Longevity Baseline) Target: ~500 MET-minutes/week. Designed for: Previously inactive individuals, those with extreme occupational time constraints, or populations managing chronic morbidity. * Daily Ambulation: Accumulate 3,100 to 4,000 steps daily 39. * Aerobic Base: 75 minutes of brisk walking or light cycling per week (e.g., roughly 11 minutes per day). This alone triggers a 20% reduction in all-cause mortality 3. * Incidental Intensity: Integrate 3 to 4 minutes of VILPA (Vigorous Intermittent Lifestyle Physical Activity) per day - such as taking the stairs briskly, carrying heavy groceries, or walking uphill to stimulate transient spikes in heart rate 9. * Strength: Two 15-minute sessions focusing on basic bodyweight movements (squats, modified push-ups) to engage major muscle groups and delay the onset of severe sarcopenia 16.
Level 2: The Longevity Sweet Spot (The Evidence-Based Ideal) Target: ~1,000 to 1,500 MET-minutes/week. Designed for: The general population seeking to absolutely maximize lifespan, neuromuscular health, and metabolic flexibility without transitioning into elite athletic training paradigms. * Daily Ambulation: Accumulate 7,000 to 8,000 steps 925. * Aerobic Base (Zone 2): 150 to 180 minutes per week of steady-state, conversational-pace cardio (e.g., three 50-minute sessions of cycling, brisk incline walking, or swimming). This forces the body to prioritize lipid oxidation 18. * Aerobic Peak (HIIT): One 20-minute session of High-Intensity Interval Training (e.g., 4x4 minute intervals at 90% max HR) to specifically boost VO2 max and increase capillary density 1. * Strength: Two 30- to 45-minute sessions of full-body resistance training lifting moderate to heavy weights. This stimulates muscle protein synthesis, increases bone mineral density, and triggers the release of neuroprotective myokines 2116. * Social/Interactive: Replace one standard cardio session with an interactive sport (tennis, badminton, or soccer) to gain the combined benefits of unpredictable interval training and the neurochemical rewards of deep social interaction 1919.
Thresholds of Longevity: Minimum, Optimal, and Diminishing Returns
The following table categorizes the physiological consensus across major longevity domains, mapping the minimum requirements against the optimal sweet spots and the distinct thresholds where diminishing returns occur.
| Biological Modality | Minimum Effective Dose (Baseline Protection) | Optimal Sweet Spot (Maximum Longevity ROI) | Diminishing Returns Threshold (Plateau) |
|---|---|---|---|
| Weekly Aerobic Volume | 75 mins moderate OR 37.5 mins vigorous 312. | 150 - 300 mins moderate OR 75 - 150 mins vigorous 412. | > 300 mins moderate OR > 150 mins vigorous (No added mortality benefit) 13. |
| Daily Step Count | 3,100 - 4,000 steps 39. | 7,000 - 8,000 steps (for mortality) 325. | > 8,000 - 10,000 steps (for mortality; fat loss may require intensity variation) 325. |
| Resistance Training | 30 - 60 mins total per week (across 1-2 sessions) 16. | 2 - 3 dedicated sessions per week targeting all major muscle groups 1239. | > 4 heavy sessions per week (Increases injury and systemic recovery risk without massive added longevity benefit) 239. |
| Cardiorespiratory (VO2 Max) | Moving out of the bottom 20th percentile (least fit) 7. | Top 25% for age and gender bracket 1. | Elite athletic VO2 max levels (Requires extreme volume training) 628. |
| Resting Heart Rate (RHR) | < 80 bpm (consistent baseline) 13. | 50 - 70 bpm (stable or slightly declining over time) 113. | < 40 bpm (Often seen in elite athletes, but unnecessary for general longevity) 1. |
Bottom Line
The scientific consensus on physical activity and longevity is unequivocal: the human body requires consistent, varied metabolic stimulus to delay cellular aging, prevent cardiovascular decay, and preserve neurological function across a lifespan. However, the pursuit of longevity is fundamentally different from the pursuit of elite athletic performance.
The vast majority of mortality reduction is achieved at surprisingly accessible thresholds. Transitioning from a completely sedentary state to merely 75 minutes of walking per week yields a massive 20% reduction in all-cause mortality, proving that any movement is profoundly better than none. To absolutely optimize lifespan, individuals should target the evidence-based sweet spot: 150 to 300 minutes of weekly activity, meticulously structured around an 80/20 split of steady Zone 2 aerobic work to build the mitochondrial base, supplemented by high-intensity intervals and anchored by two days of progressive resistance training to secrete protective myokines. While the persistent myth that extreme exercise inherently damages the heart has been largely debunked by modern mega-cohorts revealing an asymptotic mortality curve, pushing beyond 300 weekly minutes offers steeply diminishing returns for pure life extension. Ultimately, treating exercise as a daily, multifaceted hygiene practice - blending cardiovascular base building, muscular preservation, and socially engaging interval sports - remains the ultimate biological prescription for a long, highly functional life.