Continuous glucose monitoring for people without diabetes
Introduction
Continuous glucose monitoring (CGM) technology has fundamentally transformed the management of diabetes mellitus over the past two decades. Historically confined to patients with type 1 diabetes and, subsequently, individuals with insulin-dependent type 2 diabetes, the technology provides real-time, dynamic insights into interstitial glucose concentrations. By measuring glucose in the interstitial fluid rather than capillary blood, these biosensors offer a continuous pharmacokinetic curve, revealing the magnitude, duration, and frequency of glycemic excursions that episodic finger-prick testing inherently misses. However, a profound paradigm shift has materialized in recent years. Advancements in sensor miniaturization, prolonged wear times, and aggressive direct-to-consumer marketing have catapulted CGMs out of the exclusive domain of clinical endocrinology and into the mainstream wellness market.
By 2026, the use of CGMs by individuals without diabetes - a demographic traditionally classified as normoglycemic - has surged, driven by a growing cultural fascination with metabolic optimization, longevity, and quantified self-tracking 123. The target market is vast; in the United States alone, an estimated 260 million adults do not have a formal diabetes diagnosis, yet public interest in metabolic health has never been higher 1. This expansion into healthy populations has generated a highly polarized and complex discourse within the medical community. Proponents of this shift, heavily represented by longevity physicians, functional medicine practitioners, and digital health startups, argue that standard episodic testing (such as fasting plasma glucose and Hemoglobin A1c) fails to capture high glycemic variability, thereby missing the earliest physiological whispers of hyperinsulinemia and insulin resistance 567.
Conversely, traditional endocrinology bodies, including the American Diabetes Association (ADA) and the Endocrine Society, warn that the mass deployment of medical devices in healthy populations outpaces the peer-reviewed evidence. These organizations express concern over the lack of validated normative CGM metrics, the pervasive public misinterpretation of normal physiological post-prandial glucose excursions as pathological, and the potential for device-induced psychological morbidity, such as severe health anxiety and orthorexia nervosa 2345.
This exhaustive research report evaluates the utility, accuracy, and clinical evidence surrounding CGM use in people without diabetes. It delineates the profound regulatory shifts defining the 2024 to 2026 consumer market, notably the divergent pathways of the United States Food and Drug Administration (FDA) and European Conformity (CE) marking. Furthermore, it establishes the current scientific consensus on normative glycemic metrics, dissects the commercial claims of consumer health brands against independent peer-reviewed clinical trials, and provides a nuanced synthesis of the ongoing debate between proactive longevity medicine and evidence-based traditional endocrinology.
The Transatlantic Regulatory Divide: US FDA versus European CE Mark
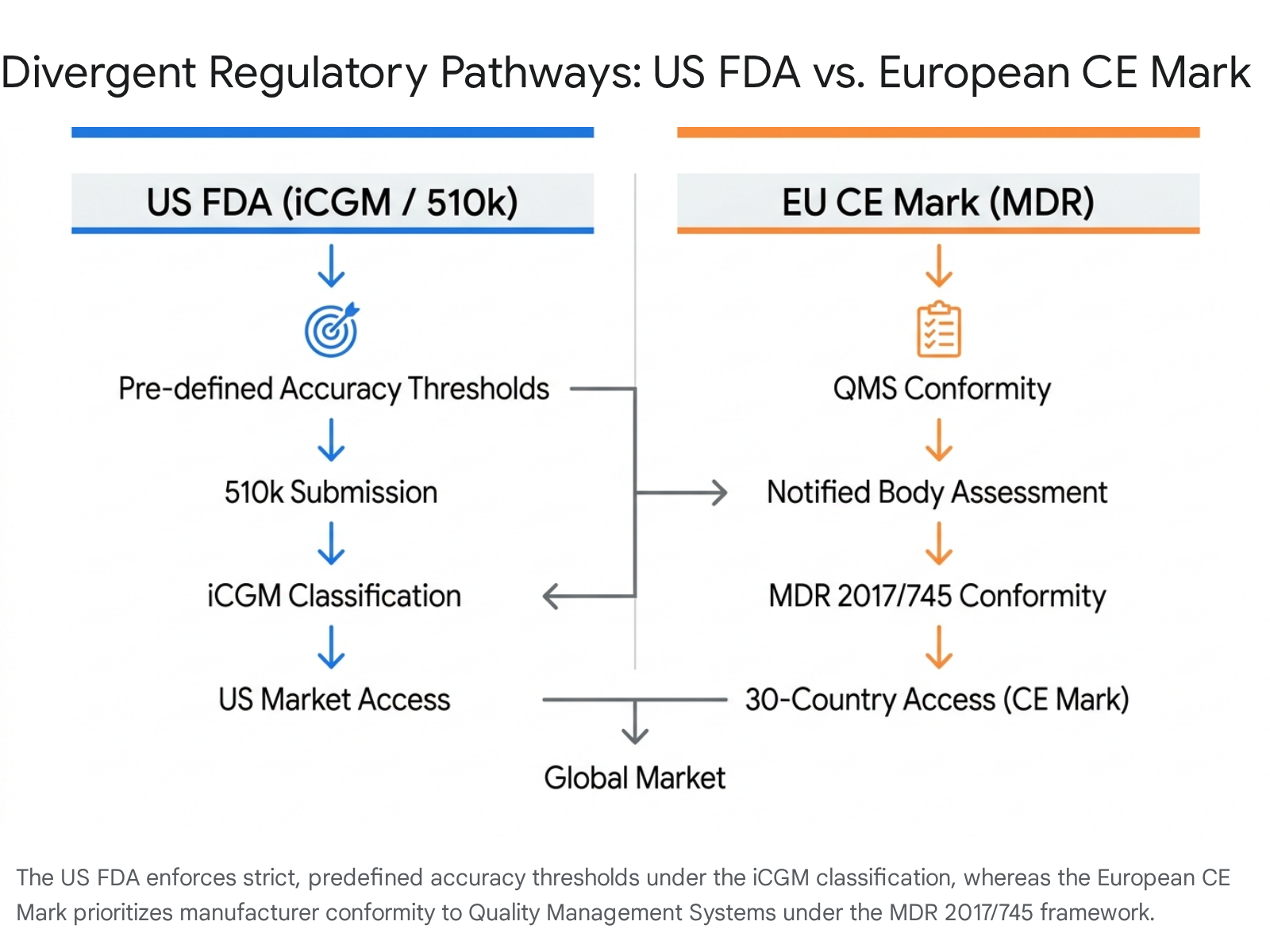
The regulation of continuous glucose monitors reflects distinct underlying philosophies regarding medical device safety, efficacy, and consumer access. A critical examination of the regulatory frameworks in the United States and the European Union reveals significant discrepancies in how device accuracy and clinical utility are validated, ultimately impacting the safety profiles of the biosensors reaching consumers.
The FDA iCGM Classification and Stringent Premarket Review
In the United States, the Food and Drug Administration (FDA) has historically maintained stringent oversight of CGM technology, classifying these devices as Class II or Class III medical devices requiring robust premarket clinical validation. The establishment of the integrated Continuous Glucose Monitor (iCGM) special controls pathway marked a watershed moment for the industry. The iCGM classification sets rigorous, predefined accuracy standards across the entire physiological glucose range. To achieve this designation, manufacturers must provide comprehensive data on Mean Absolute Relative Difference (MARD) - the industry standard for accuracy where a lower percentage indicates closer alignment with a laboratory blood reference - along with stringent assessments of alert performance and safety against interfering substances like acetaminophen or ascorbic acid 126.
The FDA 510(k) clearance process, which demands proof of "substantial equivalence" to a legally marketed predicate device, traditionally requires between three to six months for review. While clinical data is requested in only a minority of general 510(k) submissions, the iCGM standard uniquely enforces full-range clinical testing to ensure robust accuracy performance 121415. This rigorous premarket hurdle is designed to guarantee that devices utilized for critical medical decisions, such as insulin dosing, operate with minimal failure rates across diverse patient populations.
The European Union Medical Device Regulation (MDR) and Conformity Assessment
The European regulatory pathway stands in stark contrast to the FDA's heavily premarket-focused approach. In the European Union and the European Free Trade Association (EFTA) regions, medical devices must obtain a CE mark, which signifies conformity with the relevant European safety and performance regulations. Since May 2021, the applicable framework has been the Medical Device Regulation (MDR) 2017/745/EU, which superseded the older Medical Device Directive (MDD) originally established in 1993 126.
While the MDR significantly tightened the requirements for clinical evaluation and post-market surveillance compared to its predecessor, the CE marking process fundamentally remains a conformity assessment utilizing a Quality Management System (QMS). Manufacturers must demonstrate through Notified Body certification that their design and production processes meet EU safety requirements 614. However, unlike the FDA's iCGM pathway, the European framework has historically lacked universally mandated, predefined accuracy thresholds (such as a specific maximum MARD) that a CGM must achieve before initial market entry 12.
This divergence implies that in Europe, CE marking permits devices to reach the market without the exact same consistency of study requirements or rigid numerical accuracy thresholds enforced in the US. Critics point out that this flexibility can lead to discrepancies between the marketed indications and actual real-world performance. A 2023 review published in the journal Diabetes, Obesity and Metabolism highlighted that while FDA-approved indications tightly match available clinical data, CE marking indications in the EU can exhibit clinical discrepancies, potentially exposing users to devices that have not undergone full-range accuracy testing equivalent to the US iCGM standard 7.
Furthermore, the pathways dictate market speed and breadth. The CE marking process grants simultaneous access to 30 European Economic Area countries and relies heavily on robust post-market clinical follow-up plans. Consequently, devices like the Abbott Lingo achieved CE marking and were launched in the United Kingdom in 2023, a full year prior to their FDA OTC clearance in the United States 11415.
The 2024 Over-The-Counter Paradigm Shift
The regulatory and commercial landscape experienced a seismic shift in 2024 with the FDA's unprecedented clearance of over-the-counter (OTC) continuous glucose monitors. Specifically targeting adults aged 18 and older who do not use insulin, this move effectively birthed a new category of consumer-facing health management tools. In March 2024, Dexcom secured the first OTC clearance for the Dexcom Stelo Glucose Biosensor System 8910. Shortly thereafter, in June 2024, Abbott received OTC clearance for two distinct systems: the Libre Rio (targeted at non-insulin-using type 2 diabetics) and the Lingo (specifically marketed for health and wellness in individuals without diabetes) 111.
These OTC clearances required the manufacturers to demonstrate substantial equivalence to their prescription predicates while proving safety for lay users. Crucially, to mitigate the risk of unnecessary medical interventions and alarm fatigue in healthy users, the FDA required these devices to feature altered software architectures. Notably, neither the Dexcom Stelo nor the Abbott Lingo feature real-time alarms for imminent hypoglycemia - a critical safety feature in devices intended for insulin users, but a potential source of extreme anxiety for normoglycemic individuals who routinely experience asymptomatic physiological dips in interstitial glucose 101213.
The Dexcom Stelo Biosensor System
The Dexcom Stelo is structurally derived from the highly accurate Dexcom G7 biosensor but features proprietary firmware and software tailored for type 2 diabetics not on insulin and general health-conscious consumers. By eliminating the prescription barrier, Dexcom opened the market to an estimated 25 million non-insulin-dependent diabetics in the US, alongside millions of wellness-focused consumers, offering the device at an out-of-pocket subscription price of approximately $89 to $99 per month 914.
Technical specifications of the Stelo include an unprecedented 15-day sensor wear time (with a 12-hour grace period for seamless changeovers), a 30-minute warm-up period, and robust waterproofing 1324. A fundamental difference from its clinical counterpart is its data reporting cadence. While the Stelo sensor continually samples interstitial fluid, the software algorithm aggregates and updates the user's smartphone app only every 15 minutes. This is a deliberate reduction in data frequency compared to the G7's 5-minute updates, designed to smooth out minor physiological noise and reduce user hyper-fixation on minute-by-minute changes 2425. Furthermore, the Stelo restricts its measurable glucose reading range to 70 - 250 mg/dL, omitting the extreme pathological highs and lows (40 - 400 mg/dL) displayed by the G7 13. In independent real-world head-to-head testing evaluating MARD, the Stelo demonstrated a highly respectable 7.87%, confirming its reliability for non-critical metabolic trend monitoring 25.
The Abbott Lingo and Libre Rio
In response to Dexcom, Abbott structured a bifurcated OTC approach. The Libre Rio is explicitly intended for people ages 18 and older with type 2 diabetes who do not take insulin, maintaining a full measurement range of 40 - 400 mg/dL 11. Conversely, the Abbott Lingo positions itself purely as a health and wellness biowearable for the non-diabetic population.
The Lingo sensor offers a 14-day wear time and requires a 60-minute warm-up period 24. Unlike the Stelo, the Lingo app updates glucose readings every single minute, providing a highly granular, real-time curve of interstitial glucose. In independent MARD testing, the Lingo demonstrated an exceptional accuracy rate of approximately 6.36%, positioning it among the most precise sensors available outside of critical care 25.
Abbott differentiates the Lingo through proprietary software analytics, primarily the "Lingo Count." Rather than forcing novice users to interpret complex area-under-the-curve graphs, the Lingo Count acts as a daily composite metric that quantifies the magnitude and duration of glucose spikes. By gamifying the data, Abbott aims to simplify behavioral modifications, encouraging users to lower their daily Lingo Count through dietary adjustments, prioritizing protein, and engaging in post-prandial physical activity 2515. However, a notable limitation of the Lingo ecosystem compared to the Stelo is its closed architecture; as of 2026, the Stelo allows for relatively easy data sharing directly with healthcare providers, whereas the Lingo lacks native provider data-sharing capabilities, maintaining its status as a direct-to-consumer lifestyle product 2728.
Establishing Normative Glycemic Baselines in Healthy Populations
A primary clinical and epidemiological challenge in deploying CGMs to healthy populations is the historical lack of validated normative reference ranges. Because traditional glycemic targets were developed exclusively for diabetes management - specifically to prevent microvascular complications like retinopathy and macrovascular events like myocardial infarction - applying these rigid targets to healthy individuals is both scientifically inaccurate and clinically inappropriate.
The American Diabetes Association (ADA) generally recommends that individuals with diabetes maintain a Time in Range (TIR) between 70 - 180 mg/dL (3.9 - 10.0 mmol/L) for at least 70% of the day 1617. However, a healthy pancreas maintains far tighter, yet surprisingly dynamic, control. Recent multi-center prospective studies, utilizing latest-generation CGM devices in normoglycemic cohorts, have provided the vital benchmarking data required to accurately interpret consumer CGM readings.
The T1D Exchange and Contemporary Normative Data
A pivotal study published in the Journal of Clinical Endocrinology & Metabolism, leveraging data from the T1D Exchange Clinic Network, established foundational reference ranges for sensor glucose in healthy, non-diabetic children and adults (aged 7 to 80 years) using the Dexcom G6 1819. The results fundamentally dismantled several assumptions about healthy glucose metabolism.
In this healthy cohort of 153 participants, the mean average 24-hour glucose was remarkably consistent at 98 to 99 mg/dL across all age groups under 60 years. The median Time in Range (defined strictly as 70 to 140 mg/dL for non-diabetics) was 96%. However, the data definitively revealed that healthy individuals routinely experience brief excursions outside this narrow band. Participants spent a median of 2.1% of their day (approximately 30 minutes) with glucose levels exceeding 140 mg/dL, and a median of 1.1% of their day (approximately 15 minutes) with levels below 70 mg/dL 1819.
More recent independent evaluations emphasize the profound individuality of glycemic responses. A 2022 matched-pair analysis involving healthy participants found that individuals spent 90.6% of their time between 70 and 125 mg/dL, and 95.8% of their time between 70 and 140 mg/dL 20. Astonishingly, another analysis observed that 41% of healthy individuals experienced interstitial glucose levels below 70 mg/dL in a 24-hour period, with some healthy men spending up to 8.8% of their day (126 minutes) below 70 mg/dL without exhibiting any clinical symptoms of hypoglycemia 20.
This phenomenon underscores a critical physiological nuance: interstitial fluid glucose (measured by CGMs) is not perfectly identical to capillary blood glucose. Because glucose must diffuse from the vascular space into the interstitial fluid, there is an inherent physiological lag of 5 to 10 minutes. In states of rapid change, or during periods of physical compression (such as sleeping on the sensor, causing localized ischemia), interstitial glucose can drop artificially, leading to false "lows" that trigger unnecessary alarm if misinterpreted by a lay user 23435.
The Clinical Diagnostic Gap
Despite these emerging datasets, clinical interpretation of non-diabetic CGM data remains highly discordant. A 2025 survey of 18 expert clinicians analyzing potentially challenging CGM reports from individuals without diabetes revealed profound disagreement. While the clinicians reviewed cases where participants spent >2% of their time above 180 mg/dL (despite having normal HbA1c <5.7% and normal fasting glucose), there was no clear consensus on whether clinical follow-up was required. The interrater reliability was exceptionally poor (Fleiss Kappa = 0.36), highlighting that the medical establishment currently lacks universally accepted, evidence-based guidelines for identifying which subtle CGM anomalies in healthy individuals truly predict future progression to type 2 diabetes 5.
Summary of Normative Glucose Metrics
To synthesize the clinical findings from 2022 to 2026, the table below outlines the established normative CGM metrics for healthy, non-diabetic individuals compared to standard diabetic targets.
| Glycemic Metric | Target for Diabetes Management (ADA Standards) | Normative Range for Healthy Individuals (Clinical Evidence) |
|---|---|---|
| Fasting Glucose | 80 - 130 mg/dL | 75 - 95 mg/dL 20 |
| Mean 24-Hour Glucose | < 154 mg/dL | 94 - 102 mg/dL 1820 |
| Time in Range (70 - 140 mg/dL) | Not the primary evaluation metric | > 90% to 96% of the day 1820 |
| Time in Range (70 - 180 mg/dL) | > 70% of the day | > 99% of the day 1820 |
| Time Above 140 mg/dL | < 25% of the day | ~2% to 10% of the day (Represents normal physiological post-meal spikes) 3518 |
| Time Below 70 mg/dL | < 4% of the day | ~1% to 8.8% of the day (Frequently asymptomatic; influenced by interstitial lag and sleep compression) 1820 |
Post-Prandial Glycemic Excursions: Physiological Norms Versus Pathological Risk
A central tenet of the consumer CGM movement is the vilification of the post-prandial glucose "spike." Grey literature, wellness blogs, and aggressive direct-to-consumer marketing campaigns frequently assert that any rapid escalation in blood glucose causes immediate oxidative stress, systemic inflammation, vascular damage, and accelerated cellular aging 3621. Consequently, consumers are urged to flatten their glucose curves at all costs, often resorting to extreme carbohydrate restriction or fasting protocols.
However, a rigorous review of peer-reviewed endocrinology literature paints a vastly different picture, distinguishing sharply between pathological glycemic variability and normal homeostatic responses. While chronic hyperglycemia and sustained glycemic variability in patients with diabetes unquestionably lead to endothelial dysfunction, microvascular complications, and cardiovascular mortality, equating a transient, post-prandial glucose elevation in a healthy person to diabetic pathology is a profound mischaracterization of human physiology 222324.
The Physiological Carbohydrate Response
When a healthy individual consumes a carbohydrate-rich meal, glucose enters the bloodstream, prompting the pancreas to release insulin in a highly orchestrated, biphasic response. A rapid, transient rise in blood glucose - reaching peaks of 130 to 140 mg/dL, and occasionally higher depending on the glycemic load - is not a pathological failure of the system; it is the system working exactly as designed to process macronutrients 341.
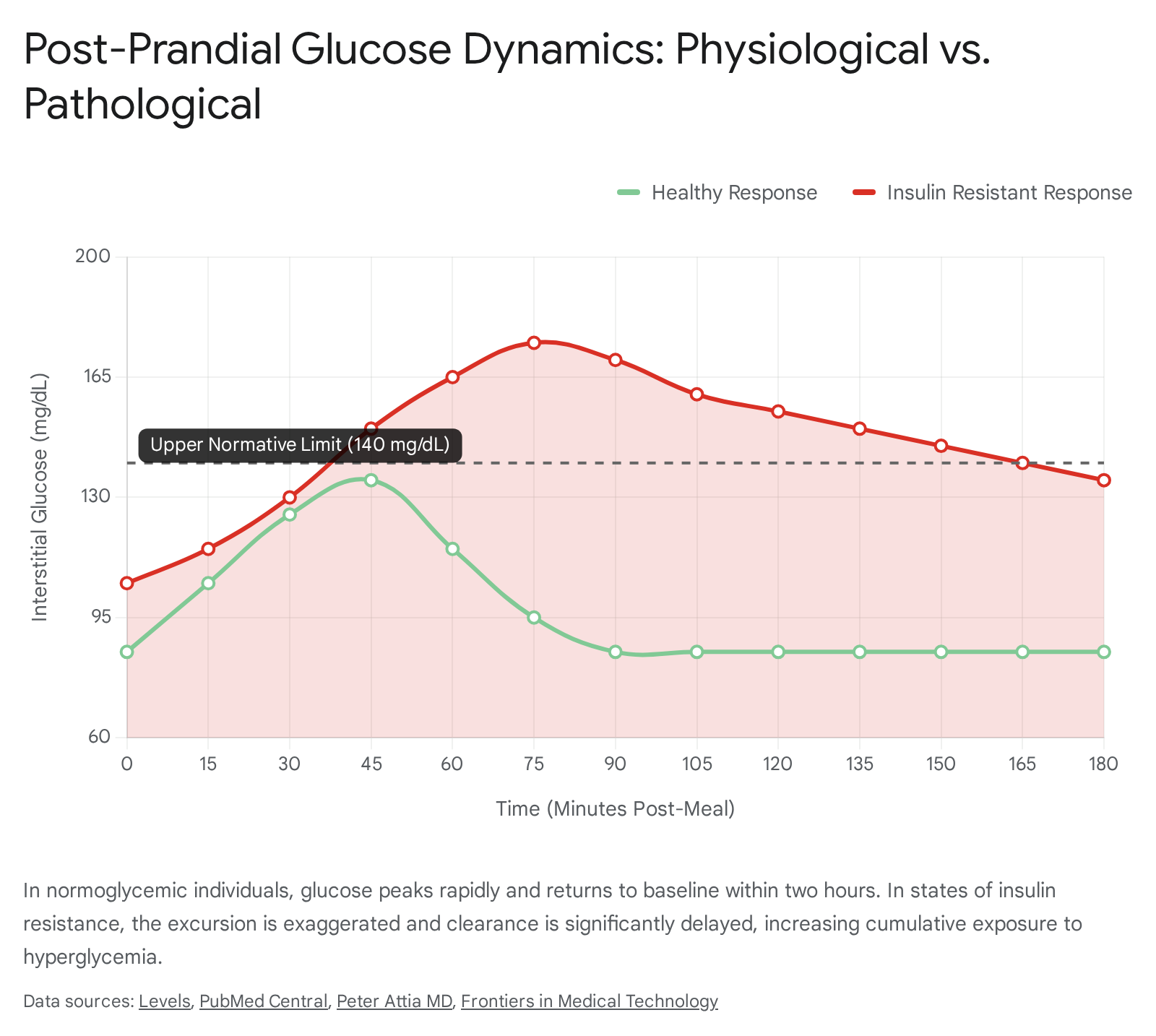
A comprehensive 2026 scoping review comparing claims in the grey literature with formal medical research found significant discrepancies regarding the danger of these spikes. Both domains agree that chronic glucose spikes and sustained high baseline glucose cause oxidative stress and endothelial dysfunction. However, the grey literature extensively extrapolates these findings to claim that acute, isolated spikes in normoglycemic individuals independently cause cancer, rapid aging, and severe mental health disorders. The peer-reviewed medical literature does not support the assertion that isolated acute spikes in people without diabetes drive these significant morbidity outcomes. Instead, the evidence overwhelmingly suggests that long-term, frequent, and sustained spikes - indicative of underlying hyperinsulinemia and developing insulin resistance - are the true drivers of cardiometabolic risk 362122.
Furthermore, healthy physiological responses inherently include glucose elevations triggered by mechanisms entirely separate from food intake. High-intensity exercise, acute psychological stress, and the "dawn phenomenon" (the natural early-morning release of cortisol and epinephrine) all stimulate hepatic gluconeogenesis and glycogenolysis, elevating blood glucose to provide immediate energy substrates. Penalizing a healthy user for a glucose spike during a rigorous cardiovascular workout or a stressful presentation represents a fundamental misunderstanding of human metabolism 22526.
Commercial Platforms and the Pursuit of Metabolic Optimization
The commercialization of CGMs for healthy users has given rise to sophisticated digital health platforms, most notably Levels and Nutrisense. These companies operate by pairing third-party CGM hardware (like the Dexcom G7 or FreeStyle Libre) with proprietary software ecosystems designed to analyze, score, and optimize dietary habits based on glycemic responses 14445.
These platforms have successfully democratized access to metabolic data, empowering users to undertake personalized "N=1" clinical trials to discover their unique responses to different macronutrients. For example, clinical studies by the Weizmann Institute have shown that two non-diabetic individuals can eat the exact same food - such as a banana versus a wheat cookie - and experience equal and opposite glycemic excursions based on their unique microbiome and insulin sensitivity 46. By visualizing this biofeedback, these platforms have popularized the concept of metabolic flexibility and provided an undeniable behavioral feedback loop that frequently drives users toward healthier, whole-food diets and increased physical activity 4647.
However, the specific glycemic targets promoted by these consumer brands often diverge significantly from established clinical consensus. By aggressively defining "optimal" glucose levels in their whitepapers and marketing materials, these platforms sometimes pathologize variations that the medical community considers entirely benign.
Evaluating the Consumer Targets
Levels, relying heavily on its interpretation of longevity and metabolic research, sets highly stringent "optimal" ranges for its users. For example, the platform advocates for a fasting glucose between 72 - 85 mg/dL, and recommends that post-meal glucose should ideally not exceed 110 mg/dL, with an increase of no more than 30 mg/dL from baseline 20.
While it is true that epidemiological data associates higher fasting glucose (even within the "normal" ADA range of 90-99 mg/dL) with increased long-term risks of cardiovascular disease and type 2 diabetes, the mandate to keep post-prandial spikes below 110 mg/dL is exceptionally rigid. As demonstrated by the T1D Exchange data, healthy, non-obese individuals routinely exceed 110 mg/dL after meals, occasionally reaching up to 140 mg/dL as a normal physiological response to digestion 1841.
The table below contrasts the commercial claims of consumer CGM platforms against the current peer-reviewed clinical evidence.
| Claim / Metric | Consumer CGM Brand Marketing (e.g., Levels, Nutrisense) | Independent Clinical Evidence & Physiology |
|---|---|---|
| Optimal Post-Meal Peak | Should remain < 110 mg/dL; a spike > 30 mg/dL from baseline is deemed suboptimal and indicative of poor metabolic fitness 20. | Transient peaks up to 140 mg/dL are entirely normal. Healthy individuals routinely exceed 110 mg/dL post-prandially without harm 31827. |
| Danger of Spikes | Frequent spikes above 140 - 160 mg/dL cause immediate cellular damage, acute inflammation, and rapid cellular aging 2021. | Acute spikes are physiological. Cellular damage and vascular risk stem from chronic hyperglycemia and sustained hyperinsulinemia, not transient dietary excursions 362124. |
| Hypoglycemia Threshold | Users are warned to keep levels strictly > 72 mg/dL to prevent epinephrine release and cardiovascular stress 20. | Up to 41% of healthy individuals experience asymptomatic dips below 70 mg/dL daily, often artifactual due to interstitial fluid lag or sleep compression 22035. |
| General Utility | Essential for everyone to achieve optimal metabolic fitness, enhance cognitive performance, and prevent chronic disease 746. | Excellent behavioral modification tool for diet awareness, but lacks long-term longitudinal data proving it alters hard mortality outcomes in strictly healthy cohorts 249. |
Proactive Longevity Medicine Versus Traditional Endocrinology
The integration of CGMs into the wellness sphere represents the flashpoint of a broader ideological battle within modern medicine: the proactive, preventative approach of longevity medicine versus the evidence-based, risk-stratified approach of traditional clinical endocrinology.
The Longevity Paradigm: Proactive Optimization
Prominent longevity advocates and researchers, such as Dr. Peter Attia and Dr. David Sinclair, view the continuous glucose monitor as an indispensable tool for extending human healthspan. Their core argument rests on the premise that traditional metabolic screening is critically flawed and reactive. They argue that episodic tests like Hemoglobin A1c (HbA1c) and fasting plasma glucose are lagging indicators; by the time these metrics register as officially "abnormal," the patient has likely harbored underlying hyperinsulinemia and progressive beta-cell dysfunction for a decade 567.
Dr. Attia points to the concept of "glucotypes" - a term popularized by a 2018 study by Hall and colleagues - which demonstrated that up to 25% of individuals classified as normoglycemic by standard clinical measures actually exhibit severe glucose variability, occasionally reaching pre-diabetic ranges (e.g., > 140 mg/dL for 15% of the day) 641. Attia frequently cites case studies of patients with "perfect" clinical labs (e.g., A1c of 5.1%) whose CGM data revealed an average glucose of 104 mg/dL, a standard deviation of 17 mg/dL, and multiple weekly excursions over 140 mg/dL. While traditional medicine ignores this, longevity physicians argue that this hidden volatility is a "canary in the coal mine." By wearing a CGM, a non-diabetic individual can identify specific dietary triggers, implement behavioral interventions, and flatten their glucose curve, thereby mitigating the hyperinsulinemia that drives atherosclerosis, neurodegeneration, and oncogenesis 56741. In this framework, the CGM is the ultimate preventative tool, operating under the philosophy that when it comes to average glucose and glucose variability, "lower is better" 56.
Traditional Endocrinology: The Risk of Over-Medicalization
Conversely, the traditional endocrinology establishment approaches CGM use in healthy individuals with profound caution, focusing on equitable resource allocation and evidence-based morbidity outcomes.
The 2025 and 2026 ADA Standards of Care represent monumental leaps for diabetes management. The updated guidelines recommend CGM use from the very onset of diagnosis for all individuals on insulin therapy, and vastly expand access to those on non-insulin therapies at risk for hypoglycemia. The guidelines also strongly endorse Automated Insulin Delivery (AID) systems, support the use of GLP-1 receptor agonists in type 1 diabetes for weight management, and provide specific perioperative glucose targets (100 - 180 mg/dL) for hospitalized patients 16502829.
However, amidst these sweeping technological endorsements, the ADA explicitly refrains from recommending CGM as a standard screening, diagnostic, or optimization tool for healthy, non-diabetic populations 2328. Endocrinologists emphasize that while reducing profound glycemic variability is paramount in diabetes, micromanaging the transient, normal fluctuations of a healthy pancreas yields unproven clinical benefits. A 2025 position statement from the Endocrine Society acknowledges the CGM as a potential "wellness tool" for low-risk individuals seeking behavioral feedback (e.g., observing the dampening effect of a post-meal walk on glucose). However, they strongly caution against making extreme dietary modifications based on short-term interstitial data 2417.
The medical establishment warns that the focus must remain on holistic health - physical activity, lean muscle mass preservation, and sustainable nutrition. Fixating on a singular metric ignores the broader metabolic picture, including lipid profiles, systemic inflammation, and cardiovascular fitness. As experts noted in a 2025 ADA debate, without longitudinal data proving that flattening the curve in healthy individuals reduces actual mortality or MACE (Major Adverse Cardiovascular Events), the widespread use of CGMs risks becoming a "disaster waiting to happen" characterized by over-medicalization, resource diversion, and widespread misinterpretation of biological data 30.
The Psychosocial Sequelae: Data Fatigue and Orthorexia Nervosa
Perhaps the most significant and under-discussed concern regarding the unregulated use of CGMs in healthy populations is the psychological toll. The democratization of high-fidelity biometric data inevitably brings the risk of obsessive tracking, leading to deleterious mental health outcomes that paradoxically degrade the user's overall well-being.
Data Fatigue and Alarm Burden
The continuous stream of data generated by a CGM can quickly overwhelm an individual. Qualitative studies assessing the uptake of digital health technologies consistently identify "data fatigue" and "alarm burden" as primary barriers to long-term adherence 353155. Healthy users, unaccustomed to evaluating biometric data, may become obsessively focused on interpreting every minor fluctuation, leading to heightened anxiety when values inevitably drift outside self-imposed optimal ranges.
Historically, prescription CGMs triggered "alarm fatigue" due to constant auditory warnings for predicted high or low glucose, resulting in sleep disturbances and device abandonment 3556. While the manufacturers of OTC devices (Stelo and Lingo) wisely removed the hypoglycemia alarms to mitigate this specific issue, the cognitive burden of constantly scanning and evaluating daily summary scores (like the Lingo Count) remains a significant psychological stressor. For perfectionist users, the pressure to achieve a "perfect" score daily transforms eating from a biological necessity into a stressful data-entry exercise 132535.
The Rise of Orthorexia Nervosa
The most alarming psychological consequence of CGM use in healthy populations is the exacerbation or induction of Orthorexia Nervosa (ON). While not yet formally recognized as a distinct diagnosis in the DSM-5, orthorexia is characterized by a pathological obsession with "clean" or "healthy" eating. Unlike anorexia nervosa, which centers on food restriction to achieve weight loss and body image alterations, orthorexia centers on the extreme fixation on the purity, sourcing, and physiological impact of food 23.
When a healthy individual pairs a predisposition for perfectionism with a continuous biofeedback device that provides immediate, negative reinforcement for eating a piece of fruit or a bowl of oatmeal (in the form of a red "spike" on a graph), the psychological conditioning can be devastating. Qualitative analyses of individuals scoring high on diagnostic instruments like the Bratman Orthorexia Test (BOT), the Dusseldorf Orthorexia Scale (DOS), and the Orthorexia Nervosa Scale (ORTO-R) reveal that extreme health anxiety drives them to impose rigid, monotonous dietary rules 232. Furthermore, studies utilizing the Short Health Anxiety Inventory (SHAI-18) and the Clinical Impairment Assessment (CIA) demonstrate that beliefs in health controllability independently predict ON symptomatology 3233.
These users systematically eliminate entire food groups - such as all complex carbohydrates, legumes, and fruits - simply because these foods elicit a natural physiological glucose response. This relentless pursuit of a flat glucose line can paradoxically ruin a user's physical health. The severe restriction of carbohydrates drastically alters the gut microbiome, reduces essential dietary fiber intake, and can lead to clinical malnutrition. Psychologically, the fear of "spiking" prevents these individuals from dining out, trying new foods, or participating in social events, leading to profound social isolation 23435. In these cases, the CGM transforms from an empowering biofeedback tool into a digital tyrant, enforcing a level of micromanagement that drastically diminishes the user's quality of life.
Conclusion
The evolution of Continuous Glucose Monitoring from a highly specialized diabetes management tool to an over-the-counter biowearable represents a watershed moment in digital health and consumer empowerment. The 2024 FDA clearances of the Dexcom Stelo and Abbott Lingo have successfully democratized access to metabolic data, empowering millions to peer inside their physiological black box. By bridging the gap between daily lifestyle choices - such as diet, exercise, and stress management - and immediate biochemical responses, CGMs hold immense potential as behavioral modification engines.
However, the application of this technology in normoglycemic populations is fraught with scientific, regulatory, and psychological complexities. The clinical evidence overwhelmingly supports the fact that healthy individuals naturally experience significant glycemic variability, including transient post-prandial spikes above 140 mg/dL and asymptomatic dips below 70 mg/dL. The commercial narrative, propagated by some digital health platforms, which pathologizes these normal physiological excursions and demands ultra-tight glycemic control, outpaces the current peer-reviewed evidence.
While longevity advocates correctly identify the utility of CGMs in uncovering hidden insulin resistance long before traditional metrics fail, the traditional endocrinology community provides a necessary, evidence-based counterweight. Medical professionals must rigorously distinguish between the chronic, systemic inflammation caused by sustained diabetic hyperglycemia and the normal, acute carbohydrate response of a healthy pancreas.
Ultimately, for the non-diabetic individual, the CGM is a profoundly powerful instrument of self-discovery, but it is not an infallible oracle of health. To maximize its utility and prevent the onset of data fatigue or orthorexia nervosa, the technology must be wielded with profound physiological context. Users and clinicians alike must interpret interstitial data not as a strict pass/fail examination of daily dietary virtue, but rather as one informative component of a holistic, balanced approach to long-term metabolic health.