Causes and Risks of Anxiety-Induced Chest Pain
Chest pain is one of the most frequent chief complaints among patients presenting to emergency departments and primary care settings globally, accounting for a massive allocation of healthcare resources 123. While immediate clinical evaluation inherently prioritizes fatal etiologies such as acute coronary syndrome (ACS) or pulmonary embolism, accelerated diagnostic pathways reveal that up to 70% to 80% of these presentations are ultimately classified as non-cardiac chest pain (NCCP) 245. Within the NCCP cohort, psychological distress - specifically generalized anxiety disorder (GAD), panic disorder, and somatoform conditions - accounts for a substantial proportion of cases 67.
The sensation of a heavy chest or chest tightness during episodes of acute anxiety often precipitates significant patient distress due to its phenomenological overlap with ischemic cardiac events 46. Understanding the mechanisms of anxiety-induced chest pain requires an exhaustive examination of autonomic nervous system dysregulation, visceral hypersensitivity, and the complex bidirectional signaling of the gut-brain axis. Furthermore, determining the prognostic danger of anxiety-induced chest pain necessitates a nuanced bifurcation: while acutely benign in the context of immediate mortality, chronic untreated anxiety and NCCP carry profound long-term prognostic implications, including elevated incidence of major adverse cardiovascular events (MACE) and severe degradation of health-related quality of life 48910.
Autonomic Nervous System Dysregulation
The primary physiological driver of anxiety-induced chest tightness is the dysregulation of the autonomic nervous system, specifically the hyperactivation of the sympathetic nervous system coupled with the withdrawal of parasympathetic tone 1112. When the brain's threat-detection centers, such as the amygdala, perceive psychological stress or anxiety, they initiate a rapid systemic stress response 1113.
Sympathetic Overactivation and Musculoskeletal Tension
The activation of the sympathetic-adrenal-medullary (SAM) axis results in the systemic release of stress hormones, prominently cortisol, epinephrine, and norepinephrine 812. These circulating catecholamines bind to adrenergic receptors across the body, leading to immediate cardiovascular, respiratory, and musculoskeletal alterations. Physiologically, this manifests as tachycardia (increased heart rate), peripheral and cutaneous vasoconstriction, and elevated blood pressure - all evolutionary adaptations designed to optimize the organism for immediate physical exertion 812.
In the context of the thoracic cavity, sympathetic activation induces severe, involuntary contractions of the intercostal muscles and the diaphragm 1214. Because the individual is not engaging in actual physical combat or flight, this persistent muscular tension is sustained without release. The sustained contraction of the chest wall musculature is frequently interpreted by the patient's sensory cortex as a crushing weight, a restrictive band across the thorax, or generalized tightness 14. Prolonged exposure to elevated cortisol levels further exacerbates musculoskeletal tension and delays recovery from localized muscle fatigue, perpetuating the sensation of chest wall pain 12.
Hyperventilation and Respiratory Mechanics
Concomitant with musculoskeletal tension, acute anxiety triggers distinct alterations in respiratory mechanics. The sympathetic response induces bronchodilation and a shift toward rapid, shallow breathing patterns, often localized to the upper chest rather than utilizing the diaphragm 14. This hyperventilation rapidly disrupts the homeostatic balance of oxygen and carbon dioxide in the bloodstream.
The excessive exhalation of carbon dioxide leads to hypocapnia, which in turn causes respiratory alkalosis (an elevation in blood pH) 14. The alkaline shift in blood pH alters calcium ion binding to albumin, transiently reducing the level of ionized calcium in the blood. This acute hypocalcemia increases peripheral nerve excitability, leading to tetany (involuntary muscle cramps), dizziness, and paresthesia (tingling sensations, commonly in the extremities or around the mouth) 14. Crucially, while the patient experiences profound breathlessness and chest restriction, clinical pulse oximetry typically reveals normal or supranormal oxygen saturation levels (above 95%), as the lungs are functioning optimally and gas exchange remains unobstructed 14.
The Modulatory Role of the Vagus Nerve
The vagus nerve (cranial nerve X) is the longest and most complex cranial nerve, serving as the primary structural component of the parasympathetic nervous system 11. It operates as a bi-directional communication highway, with up to 80% of its fibers being afferent (carrying sensory information from the internal organs to the nucleus tractus solitarius in the brainstem) and 20% being efferent (transmitting motor signals from the brain to the organs) 111516.
Under baseline conditions, the efferent vagal fibers exert a continuous, calming inhibitory influence on the heart's pacemaker (the sinoatrial node), slowing the resting heart rate and promoting heart rate variability (HRV) 1517. High vagal tone is strongly associated with emotional resilience, homeostasis, and cardiovascular health 1518. Conversely, chronic anxiety and panic disorders are characterized by low vagal tone and parasympathetic withdrawal, leaving the sympathetic nervous system unchecked 15.
Recent psychoneuroimmunology research highlights the vagus nerve's role in the inflammatory reflex 13. Severe or prolonged psychological stress can trigger an overproduction of pro-inflammatory cytokines, such as interleukins (IL-6), interferons, and tumor necrosis factor-alpha (TNF-α), in both the body and the central nervous system 1317. These cytokines can interfere with the synthesis and regulation of key neurotransmitters like dopamine and serotonin, directly exacerbating depressive and anxious phenotypes 13. By connecting the brain to the immune system, vagal dysfunction ensures that anxiety is not solely a psychological phenomenon but a systemic inflammatory state that physically manifests as chest discomfort, fatigue, and heightened pain perception 131619.
Visceral Hypersensitivity and Neural Pathways
Beyond superficial muscular tension, anxiety-induced chest pain is heavily mediated by central and peripheral neural pathways, specifically through the phenomenon of visceral hypersensitivity. Visceral hypersensitivity is characterized by a lowered pain threshold in the internal organs, where normally benign physiological processes or mild spasms are perceived as acutely painful 2021. This mechanism is a hallmark of disorders of gut-brain interaction (DGBIs), which frequently co-occur with anxiety 1920.
Peripheral Sensitization and Molecular Mediators
Most abdominal and lower thoracic pain signaling originates from nociceptors known as visceral primary afferent nerves, which have pseudo-unipolar axons connecting the internal organs to the spinal cord 19. Pathological triggers such as psychological stress, low-grade mucosal inflammation, or microbial dysbiosis can sensitize these nerves 1920. This sensitization activates "silent nociceptors" - afferent fibers that are normally unresponsive but become highly reactive in the presence of inflammatory mediators 20.
The molecular mechanisms governing this peripheral sensitization involve critical mediators such as prostaglandins, neuropeptides, and specific ion channels. Emerging evidence points to the upregulation of transient receptor potential vanilloid 1 (TRPV1) and acid-sensing ion channels (ASICs) in patients experiencing functional visceral pain 20. Furthermore, stress-induced alterations in non-coding RNA (ncRNA) expression and impaired integrity of the gastrointestinal mucosal barrier exacerbate this hypersensitivity, allowing luminal contents to further irritate the nerve endings 1220.
Central Sensitization and Viscerosomatic Convergence
The localization of visceral pain is notoriously imprecise due to the relatively sparse innervation of internal organs compared to somatic structures 19. The mechanism underpinning the diffuse, radiating nature of anxiety-related chest pain is viscerosomatic convergence 2022.
Afferent nociceptive signals originating from visceral structures (such as the esophagus) and somatic signals from the chest wall muscles travel along separate primary sensory neurons. However, these divergent neurons converge onto the exact same second-order projection neurons in the dorsal horn of the spinal cord, particularly at the C3 - T5 spinal segments 22. When psychological stress triggers minor esophageal spasms or increased gastric pressure, the resulting afferent signals are transmitted to the somatosensory cortex 422. Because the brain is more accustomed to processing somatic pain from the body's surface, it frequently misinterprets the visceral signal as originating from the chest wall or heart, leading to classic referred pain patterns 22. Functional MRI studies during episodes of referred pain have demonstrated increased activation in the secondary somatosensory cortices and the insular region, confirming the central nervous system's role in this misattribution 22.
Prolonged psychological distress leads to central sensitization, a state of hyperexcitability within the central nervous system where spinal cord neurons receiving continuous input become amplified 192022. Consequently, the threshold for pain perception drops, and minor fluctuations in heart rate or respiratory effort are amplified into alarming, painful stimuli 19.
Differential Diagnosis of Chest Tightness
Because the clinical presentation of anxiety-induced chest tightness heavily mimics potentially fatal conditions, accurate differential diagnosis is the cornerstone of emergency and primary care triage 2324. Healthcare providers must systematically rule out ischemic, pulmonary, and functional respiratory mimics before attributing chest pain solely to a psychiatric origin 2526.
Acute Coronary Syndrome and Triage Protocols
The foremost concern in any patient presenting with chest tightness is Acute Coronary Syndrome (ACS), an umbrella term encompassing unstable angina, non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI) 2627. ACS occurs when atherosclerosis, plaque erosion, or rupture leads to thrombosis, acutely restricting myocardial blood flow 2628.
The 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guidelines for the Management of Patients With Acute Coronary Syndromes mandate an immediate, aggressive approach to undifferentiated chest pain 27293031. The guidelines emphasize rapid identification through early 12-lead electrocardiograms (ECGs) and serial high-sensitivity cardiac troponin testing 2327. If a patient presents with a STEMI, immediate reperfusion therapy via primary percutaneous coronary intervention (PCI) is required, targeting a first-medical-contact to device time of less than 90 minutes 2427. Regional systems of care utilizing prehospital catheterization laboratory activation and single-call transfer protocols are recommended to meet these strict timelines 27. If PCI is unavailable within 120 minutes, fibrinolytic therapy must be administered within 30 minutes of arrival 24. The 2025 guidelines also strongly recommend the use of intravascular imaging to guide complex PCI procedures and prioritize radial (wrist) access over femoral (groin) access to minimize bleeding complications 2631.
Patients with ACS require potent pharmacological intervention, including dual antiplatelet therapy (DAPT) - typically aspirin combined with a P2Y12 inhibitor such as ticagrelor or prasugrel - to prevent further thrombotic events 262932. The 2025 guidelines have updated recommendations for DAPT duration, noting that while standard therapy lasts at least 12 months, strategies such as transitioning to P2Y12 monotherapy or de-escalating to clopidogrel after one month can mitigate bleeding risks in populations with lower ischemic risk 262931. High-intensity statin therapy is universally recommended; furthermore, for patients with LDL cholesterol ≥ 70 mg/dL despite maximal statins, the addition of non-statin lipid-lowering agents (such as ezetimibe, PCSK9 inhibitors, or bempedoic acid) is indicated to stabilize plaque and reduce major adverse cardiovascular events 2631. In rare but severe cases complicated by cardiogenic shock, the 2025 guidelines recognize the cautious, highly selected use of microaxial flow pumps over routine intra-aortic balloon pump (IABP) insertion, balancing survival benefits against the risks of vascular injury and bleeding 262931.
Accelerated Diagnostic Pathways
Because of the severe mortality risks associated with missing an ACS diagnosis, emergency departments utilize accelerated diagnostic pathways (ADPs) to safely rule out cardiac ischemia in patients who may simply be experiencing anxiety 333435.
Two of the most validated clinical decision aids are the HEART Pathway (History, ECG, Age, Risk factors, and Troponin) and the Emergency Department Assessment of Chest pain Score (EDACS) 333436. The HEART score quantifies the short-term risk of a patient experiencing a MACE within six weeks. A HEART score of 0 to 3 classifies a patient as low-risk, indicating a probability of MACE of less than 3% (often ~0.4% to 2.5% in major validation studies) 3334.
Comparative studies demonstrate nuanced differences between these pathways. In large cohort validations, the HEART Pathway exhibited a higher sensitivity for MACE (98.4%) compared to EDACS (94.2%), yielding a superior negative predictive value of 99.6% versus 99.0% 3336. However, the HEART score is slightly less specific, classifying only 38.4% of patients as safe for early discharge, compared to EDACS which safely classifies up to 58.1% of patients as low-risk 33.
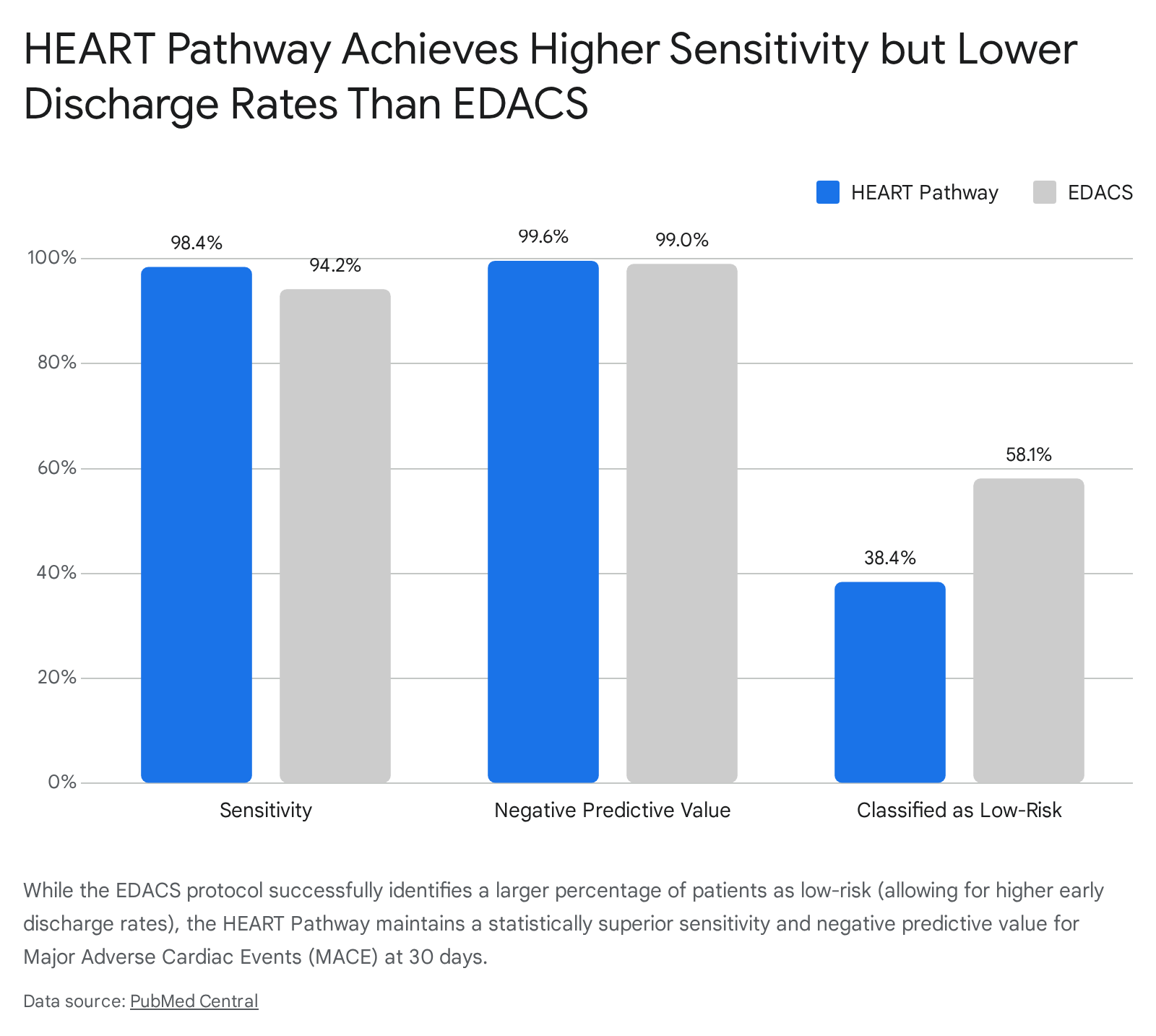
By integrating serial troponin testing at 0 and 3 hours, the HEART Pathway provides emergency physicians with the confidence to discharge anxious patients safely without exposing them to unnecessary, costly, and potentially harmful invasive cardiac testing 3435.
Chest Tightness Variant Asthma
A frequently overlooked respiratory mimic of anxiety-induced chest tightness is Chest Tightness Variant Asthma (CTVA) 3738. Classic asthma presents with a triad of symptoms: wheezing, shortness of breath, and coughing, which are caused by eosinophilic inflammation, excessive mucus production, and reversible airway obstruction 1439. However, it is a significant clinical pitfall to assume asthma is absent solely because wheezing is not detected on physical examination 2540.
CTVA is an atypical phenotype of asthma where chest tightness is the sole or predominant clinical manifestation 373841. The pathophysiology of CTVA involves the activation of bronchial C-fibers and rapidly adapting stretch receptors in the lungs; these neural impulses are transmitted via the vagus nerve to the cerebral cortex, where they are interpreted as chest tightness 38. Patients with CTVA often exhibit normal baseline pulmonary ventilation function, making the condition notoriously difficult to diagnose 4142. Epidemiological data indicate that CTVA is highly prevalent in school-aged children compared to adolescents, with significant comorbidities including allergic rhinitis, eczema, and elevated total IgE levels (>60 kU/L) 43.
Diagnostic Criteria for Chest Tightness Variant Asthma
To definitively separate CTVA from anxiety-induced chest tightness, objective spirometry is mandatory in all patients over five years of age 2526. A clinical history of symptoms that worsen at night or early morning, or are triggered by allergens and cold air, should prompt pulmonary function testing 2637. A confirmed diagnosis of CTVA requires demonstrating reversible airflow limitation, defined precisely as an improvement in Forced Expiratory Volume in one second (FEV1) of ≥12% and ≥200 mL following the administration of an inhaled rapid-acting bronchodilator (such as salbutamol) 25263744.
If baseline spirometry is normal but clinical suspicion remains high, a bronchoprovocation test (e.g., methacholine challenge) demonstrating asymptomatic bronchial hyperresponsiveness serves as the gold standard for diagnosis 254145. Furthermore, elevated Fractional Exhaled Nitric Oxide (FeNO) - with diagnostic thresholds of >20 ppb in children and >35 ppb or >50 ppb in adults depending on regional guidelines - combined with evidence of small airway dysfunction can significantly enhance diagnostic accuracy 4344.
Crucially, while asthma and anxiety are distinct etiologies, they frequently coexist 1439. The stress of chronic airway inflammation can induce anxiety, and conversely, the rapid breathing of an anxiety attack can hyper-expose airways to physical triggers, precipitating a genuine asthma exacerbation 14. Therefore, empirical trials of bronchodilators or inhaled corticosteroids (ICS) may be required to differentiate the components of the patient's discomfort 2637.
| Clinical Feature | Anxiety-Induced Chest Tightness | Chest Tightness Variant Asthma (CTVA) | Acute Coronary Syndrome (ACS) |
|---|---|---|---|
| Primary Symptom Pattern | Rapid, shallow breathing; feeling unable to draw a full breath (inspiratory difficulty) 1446. | Chest tightness as the sole symptom; typical wheeze absent. Sensation of a constricting band 143738. | Crushing, heavy, or squeezing pressure. May radiate to the jaw, neck, left arm, or back 2228. |
| Temporal Triggers | Triggered by emotional stress, panic, or specific phobias. Can occur at any time 1439. | Worse at night or early morning. Triggered by cold air, exercise, or allergens 263744. | Triggered by physical exertion or emotional stress. Unstable angina may occur at rest 26. |
| Objective Diagnostic Findings | Normal spirometry; normal O2 saturation (often >95%); normal ECG and negative cardiac troponins 1434. | FEV1 improvement ≥12% and ≥200 mL post-bronchodilator; positive methacholine challenge 2526. | Ischemic ECG changes (ST-elevation or depression); elevated high-sensitivity cardiac troponins 2327. |
| Response to Treatment | No response to bronchodilators or nitrates. Responds to anxiolytics, pacing, or vagal nerve stimulation 141548. | Rapid resolution (10-15 minutes) following inhaled bronchodilators or corticosteroids 142637. | May respond to sublingual nitroglycerin. Requires antiplatelet therapy and potential PCI revascularization 2429. |
Long-Term Prognostic Implications and Cardiovascular Risk
When addressing whether anxiety-induced chest tightness is dangerous, the answer depends entirely on the temporal horizon. In the acute setting, once life-threatening conditions like ACS and pulmonary embolism have been ruled out via rigorous emergency department protocols, an isolated anxiety-induced panic attack is not medically fatal. However, declaring NCCP benign is a clinical oversimplification that ignores robust epidemiological evidence regarding the long-term sequelae of chronic anxiety 469.
Non-Cardiac Chest Pain and Quality of Life
The persistence of NCCP despite medical reassurance represents a significant clinical challenge. Epidemiological studies demonstrate that the reduction in health-related quality of life for patients with NCCP is equivalent to, and occasionally worse than, the impairment seen in patients with confirmed ischemic cardiac chest pain 4647. Patients frequently harbor profound cardiophobia - a lingering fear that an underlying cardiac condition was missed - leading to cyclical hypervigilance toward normal cardiopulmonary sensations 479.
This hypervigilance breeds a high rate of psychiatric comorbidity. Studies indicate that up to 79% of patients with esophageal-origin NCCP exhibit concurrent psychological disorders 7. Across the broader NCCP population, major depressive disorder is present in roughly 23% of cases, and anxiety disorders (panic disorder and GAD) are observed in 11% to 50% of patients 6748. In pediatric and adolescent cohorts presenting with NCCP, diagnostic screenings identify psychiatric conditions in nearly 40% of patients, with GAD and attention-deficit/hyperactivity disorder (ADHD) being the most prevalent 49. This psychological burden translates into severe socioeconomic consequences, including elevated rates of unemployment, frequent work absenteeism, and recurrent, resource-intensive emergency department visits 45.
Anxiety as a Predictor of Cardiovascular Events
More alarmingly, recent long-term cardiovascular research has dismantled the paradigm that anxiety is entirely devoid of organic risk. Large-scale meta-analyses encompassing cohort studies of hundreds of thousands of patients have established that clinical anxiety and depressive symptoms are independent predictors of future cardiovascular morbidity 81050.
Robust meta-analyses have found that anxiety disorders are associated with a 26% to 41% increased risk of incident coronary heart disease and a 48% to 71% elevated risk of stroke 810. Furthermore, in patients who have already experienced an acute myocardial infarction (AMI) or undergone percutaneous coronary intervention (PCI), the development of post-procedural anxiety significantly worsens long-term prognosis 89. Post-AMI anxiety disorders affect 20% to 40% of patients and are notably more prevalent in women (OR = 1.8); if left untreated, this anxiety leads to a documented 47% increase in readmission rates (HR = 1.47) and a 31% increase in recurrent cardiovascular events (HR = 1.31) 948.
However, long-term mortality data present a complex picture. The Berlin Anxiety Trial (BAT) and SPIRR-CAD study, which tracked 180 coronary heart disease patients over a 12-year follow-up, surprisingly found that low levels of anxiety were associated with higher all-cause mortality (58.7%) compared to the highest anxiety quartile (14%) 50. Researchers hypothesize that while severe anxiety drives short-term MACE through sympathetic overload, a complete lack of anxiety may reflect maladaptive denial or poor coping mechanisms, leading to medical non-adherence in the long term 50.
The pathophysiology linking high anxiety to organic heart disease remains multifaceted. Chronic SAM axis activation subjects the cardiovascular system to sustained hypertension, increased myocardial oxygen demand, and endothelial shear stress 812. Simultaneously, the reduction in heart rate variability associated with vagal withdrawal increases vulnerability to fatal arrhythmias. The chronic inflammatory state mediated by the vagus nerve's failure to inhibit pro-inflammatory cytokines also accelerates atherosclerosis 813. Behavioral factors exacerbate these risks, as highly anxious patients frequently exhibit lower medication adherence and poorer engagement with cardiac rehabilitation programs 951.
Psychiatric Classification Systems
The diagnostic frameworks used by clinicians to codify anxiety-induced chest pain have evolved significantly, reflecting a deeper understanding of the mind-body interface. The two primary diagnostic manuals, the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) and the World Health Organization's International Classification of Diseases, 11th Revision (ICD-11), share core similarities but diverge in structural nuance 525354.
Diagnostic Frameworks in the DSM-5-TR
In both systems, acute chest pain is a hallmark criterion for diagnosing a Panic Attack, which acts as a building block for Panic Disorder 53. A notable structural change in the DSM-5 was the unlinking of Panic Disorder and Agoraphobia into two distinct, independently codable diagnoses, recognizing that severe panic attacks (and the resulting chest pain) frequently occur without agoraphobic avoidance 53. Furthermore, the DSM-5 allows "panic attack" to be listed as a specifier applicable across all other mental disorders 53.
When anxiety-induced chest pain becomes a chronic, persistent fixation, diagnostic classification shifts toward somatic disorders. The DSM-5 eliminated the older diagnosis of "Hypochondriasis" because it was perceived as pejorative and overly broad 5253. It was replaced by two distinct categories: Somatic Symptom Disorder (applied when the patient actually experiences severe, distressing somatic symptoms, such as chronic chest pain, accompanied by disproportionate anxiety regarding the symptom) and Illness Anxiety Disorder (applied when physical symptoms are absent or trivial, but the patient remains paralyzed by the fear of acquiring a severe disease like a heart attack) 5253.
Structural Divergence in the ICD-11
The ICD-11 maintains a slightly different architectural approach. It retains Hypochondriasis but classifies it under obsessive-compulsive and related disorders, emphasizing the repetitive, intrusive nature of health-related fears rather than the somatic symptoms themselves 52. Furthermore, the ICD-11 introduced a purely dimensional model for personality disorders, stripping away specific categories (like Borderline Personality Disorder) in favor of trait domain assessments, whereas the DSM-5-TR preserved the categorical approach alongside a secondary dimensional model 54.
Despite these differences, studies assessing the concordance between the DSM-5 and ICD-11 criteria for stress-related disorders (such as PTSD) show moderate to strong agreement. In cohorts of military veterans, Cohen's kappa values ranged from 0.65 to 0.83, indicating that while prevalence rates may slightly differ (DSM-5 algorithms tend to diagnose slightly higher rates due to requiring four symptom clusters versus the ICD-11's three), the core identification of pathological anxiety remains consistent 55.
Evidence-Based Interventions for Non-Cardiac Chest Pain
Recognizing that reassurance alone is insufficient to alter the trajectory of anxiety-induced NCCP, modern clinical practice increasingly relies on targeted psychological and neurophysiological interventions 14.
Cognitive Behavioral Therapy and Digital Interventions
Cognitive Behavioral Therapy (CBT) remains the gold standard psychological intervention for NCCP 756. CBT for chest pain focuses on restructuring maladaptive cognitive patterns - specifically the catastrophic misinterpretation of normal somatic sensations (e.g., perceiving a benign esophageal spasm as an impending myocardial infarction) 7. Therapy incorporates exposure techniques, graded physical activity, and breathing retraining to extinguish hypervigilance and reduce cardiophobia 75657.
A Cochrane review of 17 randomized controlled trials encompassing over 1,000 participants demonstrated that CBT significantly reduces the frequency and severity of chest pain episodes in the short term (up to three months) while decreasing healthcare utilization 56. The PACER trial (Patient-Centered Treatment of Anxiety after Low-Risk Chest Pain in the Emergency Room) demonstrated that both standard therapist-administered CBT and peer-supported internet-based CBT (iCBT) significantly improved anxiety and quality of life in low-risk chest pain patients 1.
Recent clinical trials have confirmed the long-term efficacy of iCBT. Patients undergoing six weeks of web-based iCBT showed substantial improvements in health-related quality of life and reductions in cardiac anxiety at a 12-month follow-up compared to treatment as usual 5758. Sub-group analyses indicated that patients presenting with co-occurring depressive symptoms at baseline experienced the most profound differential treatment effects, underscoring the critical need for psychiatric screening utilizing tools like the Hospital Anxiety and Depression Scale (HADS) prior to discharge from chest pain units 758. Conversely, brief, single-session psychological interventions have shown limited efficacy in reducing ED re-presentations, highlighting the necessity of sustained, structured therapeutic engagement 159.
Transcutaneous and Implantable Vagus Nerve Stimulation
Neuromodulation via Vagus Nerve Stimulation (VNS) has emerged as a promising therapy for mitigating the physiological manifestation of anxiety 151660. Initially approved by the FDA for treatment-resistant epilepsy and depression using surgically implanted cervical devices, VNS leverages the vagus nerve's parasympathetic capacity to restore autonomic balance 176061.
Recent advancements have focused on transcutaneous auricular Vagus Nerve Stimulation (taVNS), a non-invasive alternative that stimulates the auricular branch of the vagus nerve via the ear 1518. By avoiding the direct stimulation of cervical efferent fibers near the cardiac branch (which is why implanted VNS is typically applied only to the left side to prevent bradycardia), taVNS safely modulates neuromodulators like acetylcholine and norepinephrine without causing adverse cardiac events 1562. Clinical and preclinical systematic reviews encompassing over 100 studies indicate that taVNS enhances cognitive performance, improves extinction learning (a crucial component for treating PTSD and anxiety), and suppresses systemic inflammation by normalizing pro-inflammatory cytokines 151718. While results in major depressive disorder remain mixed, the application of taVNS for anxiety-induced visceral hypersensitivity represents a critical frontier in non-pharmacological management 1662.
Neuromodulation via the Mammalian Dive Reflex
For acute management of severe anxiety and panic-induced chest pain, patients can manually leverage an evolutionary biological mechanism known as the Mammalian Dive Reflex (MDR) 6366.
The MDR is a powerful, hardwired survival reflex shared by aquatic and terrestrial mammals, designed to optimize respiration and conserve oxygen when submerged in cold water 63. When the face is exposed to cold water - specifically targeting the distribution of the trigeminal nerves situated below the eyes and above the cheekbones - afferent signals are sent directly to the brainstem 6366.
This cold-water stimulation overrides higher-order cognitive panic circuits and directly triggers the efferent fibers of the vagus nerve 6664.
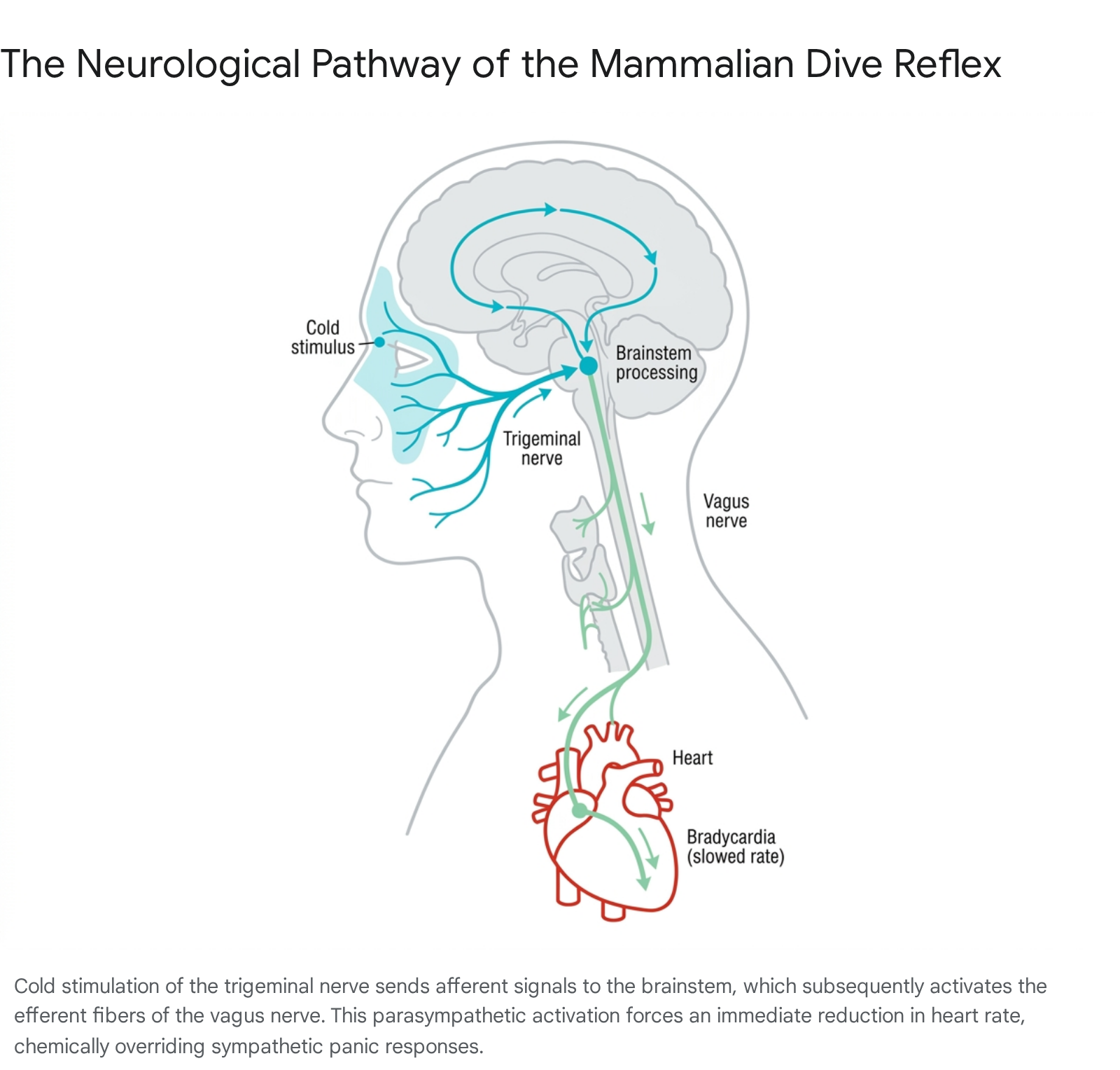
The resulting parasympathetic surge induces profound, immediate physiological changes. First, it induces severe bradycardia, dropping the heart rate rapidly - sometimes by up to 15% to 25% within seconds - countering the sympathetic tachycardia that drives the sensation of panic 486364. Second, it causes peripheral vasoconstriction, actively shunting blood away from the extremities and non-essential organs to preserve oxygen for the heart and brain 63. Finally, the reflex naturally induces apnea (breath-holding), which halts the hyperventilation cycle responsible for respiratory alkalosis and chest tightness .
Clinical applications of the MDR involve filling a bowl with icy water and, while holding one's breath, submerging the face for 15 to 30 seconds 6664. Alternatively, applying a cold pack directly across the forehead and cheekbones while practicing slow, diaphragmatic breathing can adequately stimulate the trigeminal receptors 48. Because the neural response is entirely involuntary, the MDR bypasses the patient's inability to logically suppress an acute panic attack, serving as an immediate physiological reset button that rapidly alleviates chest tightness, slows the heart, and restores the autonomic nervous system to a manageable baseline 6664.