What the Science Says About Meditation and Mental Health
Research demonstrates that clinical mindfulness programs can physically alter brain structures, reduce anxiety, and prevent depressive relapses as effectively as some standard medications. However, the practice is not universally beneficial and can trigger adverse psychological effects in some individuals, meaning it requires careful, sometimes trauma-informed application rather than being treated as a harmless cure-all.
The Neuroscience of Mental Training
For decades, meditation was viewed through a purely spiritual or philosophical lens, largely disconnected from Western clinical practice. Today, it has entered the neuroscience mainstream, conceptualized as a rigorous form of mental training capable of inducing measurable neuroplasticity 1. The consensus across modern neuroimaging studies is that sustained mindfulness practice alters both the physical structure and the functional connectivity of the human brain, offering a biological explanation for its psychological benefits.
Remodeling the Cortex
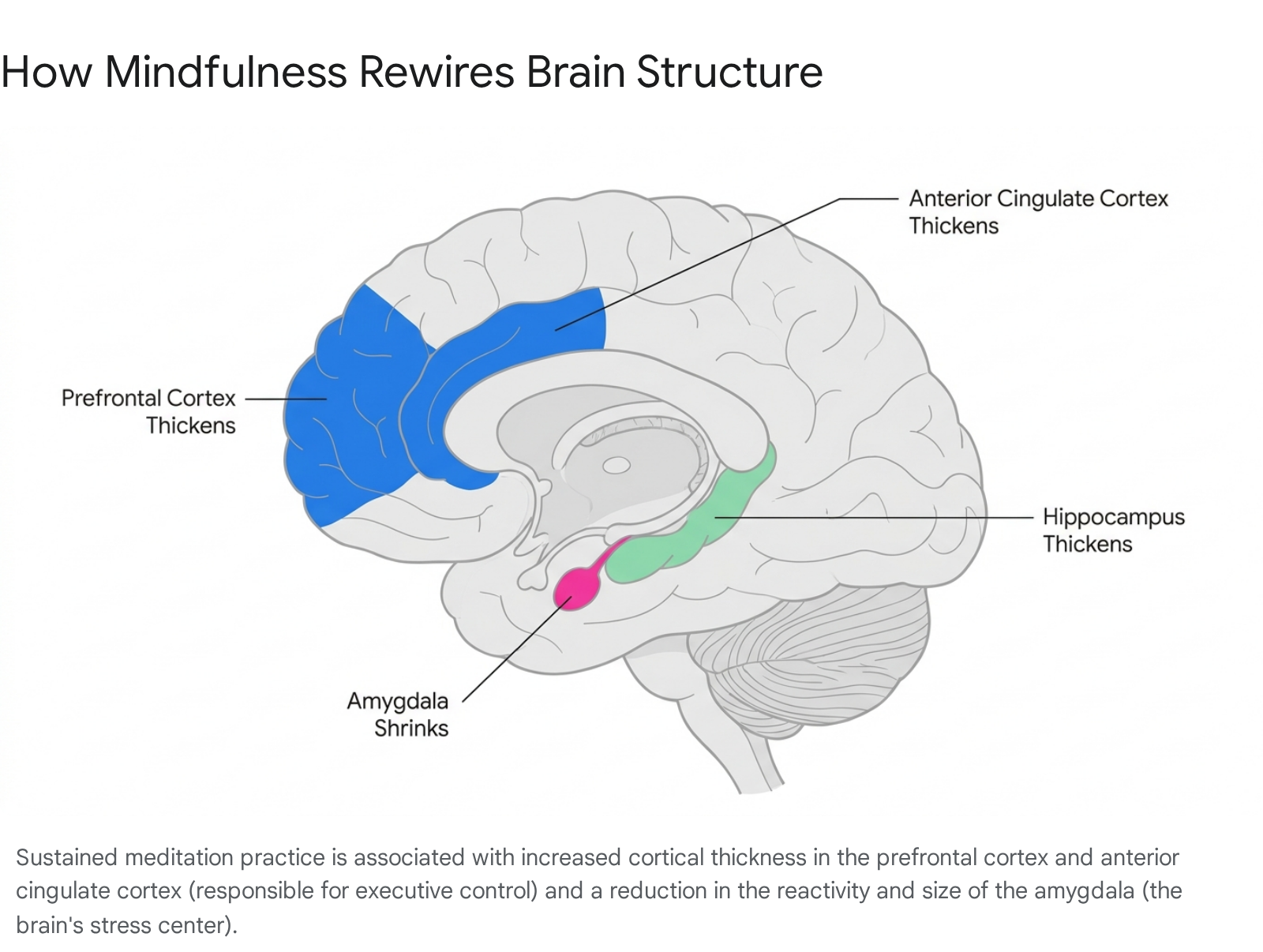
The most widely documented structural change resulting from meditation is an increase in cortical thickness, particularly in the prefrontal cortex and the anterior cingulate cortex 123. These areas are responsible for higher-order executive functions, including attention regulation, decision-making, and self-monitoring. By strengthening these regions, meditation enhances an individual's top-down regulatory control over their emotional responses, allowing them to process stressful stimuli with greater stability rather than pure reactivity 12.
Neuroimaging also reveals increased gray matter density in the hippocampus, a region critical for memory processing and emotional regulation, and the right insula, which is heavily involved in interoception, or the awareness of internal bodily sensations 234. Advanced practitioners demonstrate heightened gamma wave activity even outside of formal meditation sessions, suggesting that long-term practice creates durable, trait-level changes in how the brain processes emotional stimuli 4.
Downregulating the Amygdala
Conversely, mindfulness has been shown to downregulate the amygdala, the brain's primal fear and stress center 2. Research indicates that regular meditation not only reduces the physical size of the amygdala but also dampens its reactivity to psychological stress 12. This structural alteration correlates directly with reductions in self-reported anxiety and depression. When a practitioner encounters a stressful event, their brain relies more on the newly fortified prefrontal control regions and less on the reactive limbic system, resulting in a more measured behavioral response 1.
Quieting the Default Mode Network
A central focus of contemporary clinical research is the Default Mode Network, a large-scale brain network implicated in self-referential cognition, autobiographical memory, and mind-wandering 12. An overactive Default Mode Network is heavily associated with the kind of repetitive, negative rumination seen in clinical depression and anxiety disorders. Meta-analyses demonstrate that meditation consistently alters functional connectivity and reduces engagement in core hubs of this network, effectively interrupting the cycle of obsessive worry 12.
On a neurochemical level, mindfulness practices support these structural changes by altering the brain's chemical balance. Regular practitioners often show higher baseline levels of serotonin, which regulates mood, and gamma-aminobutyric acid, an inhibitory neurotransmitter that minimizes excess neural activity to reduce acute anxiety 2. Furthermore, meditation lowers blood concentrations of cortisol, the body's primary stress hormone, while boosting Brain-Derived Neurotrophic Factor, a protein vital for sustaining neuroplasticity and emotional resilience 2.
Clinical Gold Standards: MBSR and MBCT
The term "meditation" functions as a massive umbrella covering thousands of distinct cultural and spiritual techniques. However, in Western clinical literature and psychiatric trials, research heavily focuses on specific standardized, secularized programs designed for reproducible results.
Mindfulness-Based Stress Reduction
Developed by Jon Kabat-Zinn in 1979 at the University of Massachusetts Medical School, Mindfulness-Based Stress Reduction (MBSR) is the foundational evidence-based program 467. It was originally designed for the general public and patients suffering from chronic pain, aiming to reduce physical and psychological suffering by cultivating a non-judgmental awareness of the present moment 45.
The program requires a significant time commitment, structured as an eight-week experiential course. Participants attend weekly group sessions lasting two to two-and-a-half hours and are assigned roughly 45 minutes of daily home practice 46. The curriculum integrates sitting meditation, detailed body scans to improve interoception, and gentle hatha yoga 45. Meta-analyses of MBSR interventions show robust effectiveness in reducing general stress, improving sleep quality, and alleviating symptoms of anxiety in both clinical and non-clinical populations, such as nursing students and corporate employees 678.
Mindfulness-Based Cognitive Therapy
Building upon the framework of MBSR, Mindfulness-Based Cognitive Therapy (MBCT) was explicitly engineered as a clinical intervention to prevent depressive relapses in highly vulnerable populations 47. MBCT merges the core mindfulness techniques of MBSR with elements of traditional Cognitive Behavioral Therapy 477.
However, MBCT differs fundamentally from standard cognitive therapy. While traditional cognitive therapy attempts to challenge, analyze, and change negative belief patterns, MBCT teaches patients to change their fundamental relationship to their thoughts 477. Practitioners learn to view their negative thoughts and moods as transient mental events rather than absolute truths or core aspects of their identity 47.
Research indicates that while both programs are highly effective, they serve slightly different purposes. A recent systematic review highlights that MBCT produces larger effect sizes when targeting specific psychiatric vulnerabilities, particularly in preventing the recurrence of major depressive episodes 712. Conversely, MBSR remains more versatile for general stress reduction, burnout prevention, and chronic pain management 7.
The Efficacy of Digital Interventions
While standard clinical programs require roughly 30 minutes of practice six days a week, the modern mindfulness landscape is overwhelmingly dominated by digital smartphone applications. Digital mindfulness-based interventions overcome the financial, geographic, and scheduling barriers of in-person therapy, offering unprecedented accessibility 9.
App-Based Effectiveness and Dosage
Recent systematic reviews and meta-analyses of standalone digital interventions demonstrate that they do produce statistically significant improvements in sleep health and mental well-being. By reducing pre-sleep hyperarousal and daily worry, these apps can serve as effective introductory tools 1011. The average use among active app subscribers sits between 10 to 21 minutes per session, roughly three days a week - a drastically lower dosage than clinical programs 1116.
A compelling 2024 study involving 1,247 adults from 91 countries tested a purely app-based routine. The researchers found that just 10 minutes of daily mindfulness practice over 30 days led to a 19.2% greater reduction in depression and a 12.6% greater reduction in anxiety compared to an active control group 12. Crucially, these positive effects were largely maintained during a follow-up assessment a month after the structured training stopped, suggesting that massive time commitments are not strictly necessary to achieve baseline psychological benefits 12. Furthermore, longitudinal data on skill acquisition suggests that frequency matters more than duration; meditating for short intervals daily is more beneficial for neuroplasticity than a single, lengthy weekly session 13.
The Limitations of Digital Platforms
Despite these benefits, the scientific community expresses calibrated uncertainty regarding the long-term equivalence of apps compared to in-person training. The quality of evidence for digital interventions is frequently rated as "very low" due to significant publication bias, lack of active control groups, and reliance on unverified self-reporting 10.
Furthermore, digital meditation suffers from catastrophic attrition rates. Engagement data reveals that only about 4.7% of initial users continue to use digital meditation apps after 30 days, with the average lifetime use estimated at just one to four brief sessions 11. While apps successfully lower acute perceived stress, studies directly comparing online adaptations to in-person training suggest that face-to-face instruction leads to significantly higher overall life satisfaction 8916. This discrepancy is likely due to the social support, community accountability, and direct feedback from trained instructors that digital platforms currently cannot replicate 8916.
| Feature | Mindfulness-Based Stress Reduction (MBSR) | Mindfulness-Based Cognitive Therapy (MBCT) | Digital Mindfulness Apps |
|---|---|---|---|
| Primary Focus | General stress reduction, chronic pain, and overall well-being 47. | Preventing depressive relapse and managing severe anxiety 47. | Accessible, daily stress management and sleep improvement 1011. |
| Format | 8-week in-person/group program; ~45 mins daily practice 46. | 8-week in-person/group program; integrates CBT principles 467. | Self-guided mobile apps; heavily gamified 911. |
| Average Dose | High (2-2.5 hours weekly instruction + daily home practice) 6. | High (2-2.5 hours weekly instruction + daily home practice) 6. | Low (10-21 minutes per session, ~3 days a week) 11. |
| Best Suited For | Non-clinical populations, healthcare workers, chronic pain patients 678. | Patients with a history of recurrent major depressive disorder 47. | Beginners seeking convenience; individuals with mild-to-moderate stress 911. |
Meditation vs. Medication: The Clinical Evidence
One of the most heavily scrutinized questions in psychiatric research is whether meditation can stand toe-to-toe with pharmacological treatments. While the placebo response rate in depression hovers around 35 percent, standard antidepressant medications achieve a response rate of roughly 50 percent 19. Against this backdrop, the scientific consensus regarding clinical mindfulness is surprisingly robust: for certain specific conditions, rigorous meditation programs are essentially equivalent to first-line medications.
Evidence for Anxiety Disorders
Anxiety disorders, which affect an estimated 301 million people globally, are typically treated with selective serotonin reuptake inhibitors, commonly known as SSRIs 520. However, many patients hesitate to begin pharmacological treatment due to a well-documented profile of side effects, including insomnia, nausea, sexual dysfunction, and fatigue, or the risk of dependency associated with short-term benzodiazepine use 520.
A landmark clinical trial published in the journal JAMA Network Open directly compared an eight-week MBSR program against a standard daily dose of escitalopram, a common SSRI, for patients diagnosed with agoraphobia, panic disorder, generalized anxiety disorder, and social anxiety disorder 520. The researchers found that MBSR was just as effective as the antidepressant in alleviating anxiety symptoms by the end of the study period 520. While the medication demonstrated a slightly faster initial onset of relief, the final clinical outcome for emotional regulation and overall stress reduction was statistically comparable, positioning clinical mindfulness as a highly viable alternative for patients seeking non-pharmaceutical options 520.
Preventing Depressive Relapse
Similar equivalency results have been found in the treatment of major depression. A massive study conducted by researchers at Oxford University tested whether MBCT could effectively replace maintenance antidepressants for patients who had experienced at least three previous episodes of major depression 2114.
The trial was carefully structured: half the participants continued their standard maintenance medication, while the other half safely tapered off their drugs under medical supervision while completing an eight-week MBCT course 21. Over a two-year longitudinal follow-up, the researchers found no substantial statistical difference in the rates of depressive relapse between the two groups 2114. The cognitive therapy program was found to be just as effective as the pharmaceuticals at keeping recurrent depression at bay 2114.
Despite these highly promising findings, psychiatric experts strictly caution that meditation is not a replacement for intensive therapy or medication in the acute stages of severe, debilitating psychiatric illness. Rather, it has proven itself as a highly effective maintenance tool for preventing relapse and a primary intervention for mild-to-moderate anxiety and depressive symptoms 191524.
The Hidden Risks: Adverse Psychological Effects
Because mindfulness is widely marketed across the internet and corporate wellness sectors as a universal relaxation tool, it carries a public halo of absolute safety. However, a growing body of systematic reviews posits that meditation can have severe, detrimental effects on mental health, even for practitioners with absolutely no prior psychiatric history 252627.
The Prevalence of Negative Outcomes
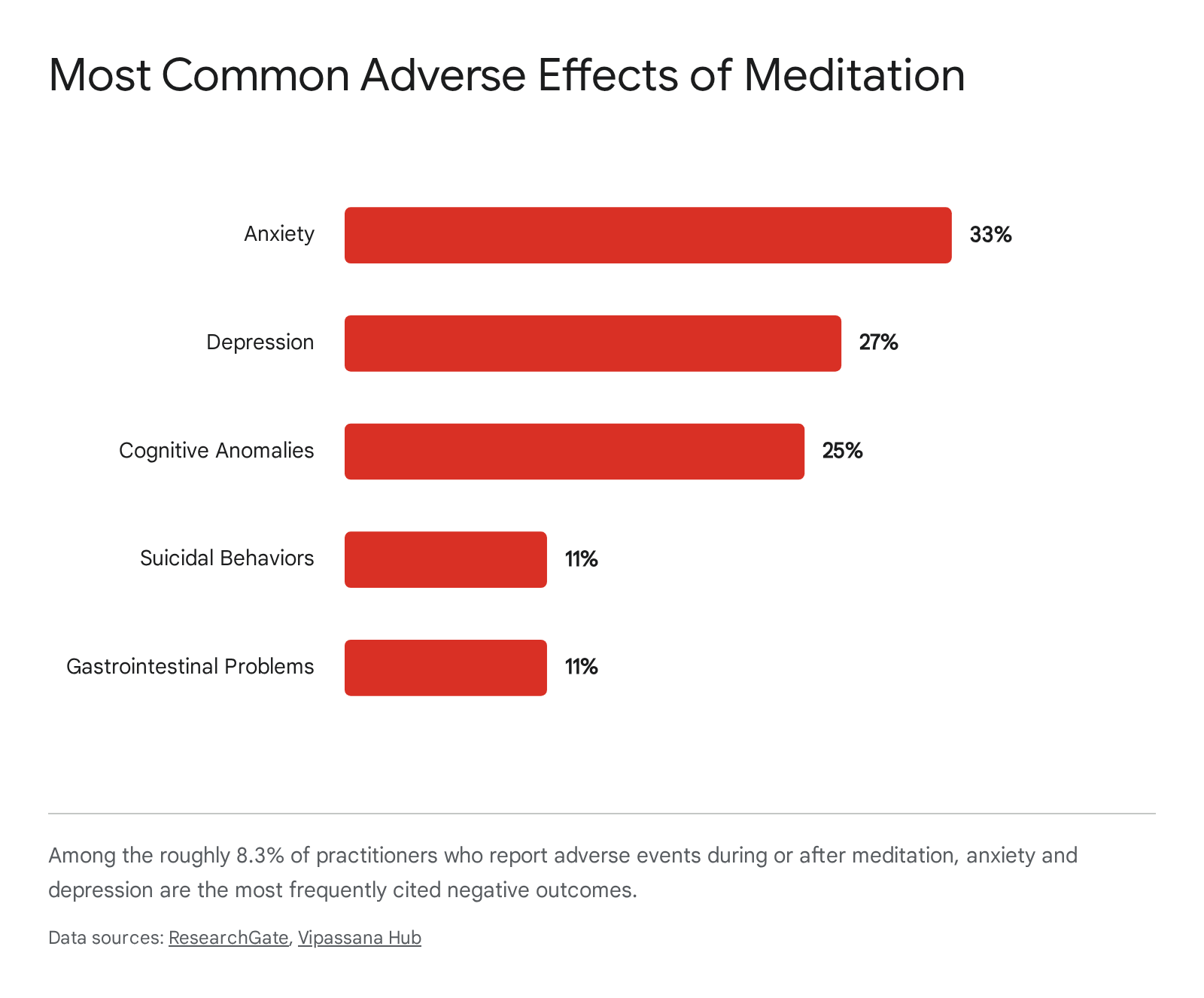
A sweeping systematic review led by researchers at Coventry University analyzed 83 distinct studies to investigate the frequency of meditation-related adverse events 2526. The researchers discovered that approximately 8.3 percent of practitioners report experiencing negative side effects during or after meditation 252616. This rate is notably similar to the estimated prevalence of negative outcomes reported by patients undergoing standard psychological therapies 1617.
The most common adverse effects documented in the literature include severe anxiety, which accounts for 33 percent of reported events, followed by sudden depressive episodes at 27 percent 252616. Additionally, a quarter of practitioners who experience negative effects report cognitive anomalies, which can include derealization, a distorted or terrifying dissolution of the sense of self, and even hallucinations 25262716. Less common but highly severe outcomes include gastrointestinal distress and the onset of suicidal ideation, each reported in about 11 percent of adverse cases 2526.
Mechanisms of Harm
These adverse effects often occur because standard meditation instruction directs students to stay intimately present with physical discomfort or emotional distress for extended periods 30. By systematically quieting the distractions of daily living, which often serve as necessary cognitive coping mechanisms, meditation can cause implicit, unprocessed traumatic memories to rush into conscious awareness like water from a broken dam 2718.
Furthermore, deeply concentrated states of mind can inadvertently trigger psychological dissociation. If a practitioner frequently feels as though they are hovering, detached from reality, or unnaturally distant from their own thoughts during practice, they may be utilizing meditation as a subtle defense mechanism to escape overwhelming emotions rather than processing them 24.
The Necessity of Trauma-Informed Mindfulness
The empirical recognition of these adverse effects has catalyzed a critical evolution in the field: the development of trauma-informed mindfulness. Pioneering quantitative research into meditation-related adverse effects has thoroughly challenged the traditional "no pain, no gain" mentality of intensive meditation retreats 32. Clinical evidence now clearly indicates that for individuals with histories of complex trauma, post-traumatic stress disorder, or adverse childhood experiences, standard meditative practices can inadvertently exacerbate traumatic stress 3219.
Modifying Traditional Instructions
Trauma-informed mindfulness fundamentally shifts the objective of the practice. The primary goal is no longer the mastery of absolute physical stillness or the achievement of a deep Zen-like state, but rather the cultivation of psychological safety, physical choice, and nervous system self-regulation 3234.
Certain traditional instructions are now explicitly flagged as potentially contraindicated for trauma survivors. For instance, instructing a class to sit perfectly still with their eyes tightly closed can immediately trigger somatic flashbacks of being trapped or held down for survivors of physical abuse 3234. By removing the ability to move, the instructor unknowingly eliminates the primary biological mechanism the nervous system uses to discharge stress energy 32. Similarly, intensely focusing on the breath - the most ubiquitous meditation anchor - can induce severe panic in practitioners who associate breath restriction with past traumatic events 3032.
Grounding and Pacing Techniques
To mitigate these risks, trauma-informed instructors deploy highly modified frameworks. Practitioners are given explicit permission to meditate with their eyes open, to shift postures frequently, or to pace the room if sitting induces anxiety 18343536. If internal bodily sensations become overwhelming, the focus is immediately redirected outward to safe, external anchors, such as noticing the specific texture of the floor beneath their feet, identifying ambient sounds, or even mindfully eating a small snack to ground the brain in the present physical reality 343620.
Most importantly, practitioners are taught the vital skill of applying the "brakes." If a session triggers a dissociative state or a flood of unbearable emotion, the practitioner is encouraged to stop the practice immediately, engage in self-soothing touch, or step out of the room 2430. This empowers the individual to maintain absolute autonomy over their exposure to distressing internal stimuli, ensuring that the intervention remains therapeutic rather than re-traumatizing.
Cultural Nuance: Eastern Roots vs. Western Clinical Models
Mindfulness did not originate in a sterile clinical laboratory; its roots stretch back thousands of years to ancient Eastern contemplative traditions, predominantly within Buddhism 221. In its original Southeast Asian context, mindfulness is not a standalone technique. It is merely one tenet of the Noble Eightfold Path - a comprehensive ethical, moral, and philosophical framework deeply concerned with community service, moral behavior, and spiritual enlightenment 2223.
The Secularization and "McMindfulness" Debate
When Asian culture and philosophy began gaining widespread traction in the West following World War II, mindfulness underwent a massive process of secularization to make it palatable for Western clinical and corporate environments 2224. Teachings regarding community obligation, compassion, and spiritual liberation were largely stripped away. In their place, Western adaptations inserted a hyper-focus on individual self-improvement, workplace productivity, and isolated stress reduction 2223.
This rigorous secularization allowed mindfulness to be studied objectively in government-funded clinical trials, ultimately proving its medical efficacy. However, it has also sparked a fierce, ongoing academic debate. Critics derisively refer to this stripped-down, commodified version of the practice as "McMindfulness" 42. Religious scholars, anthropologists, and some cross-cultural psychologists argue that by divorcing mindfulness from its foundational ethical framework, it has been reduced to a mere coping mechanism. Instead of addressing the systemic causes of modern distress, they argue, corporate mindfulness merely trains employees to be more compliant and less emotionally reactive to toxic environments 42.
The Importance of Cultural Adaptation
Interestingly, the exportation of Western clinical mindfulness models back to Asian cultures has exposed the limitations of a one-size-fits-all psychological approach. Medical professionals in Asia sometimes report confusion when attempting to apply strictly Western, secularized mindfulness protocols in their clinical settings, as the concepts feel unnaturally divorced from the cultural context that surrounds their patients daily 42.
Recent research underscores the critical importance of cultural adaptation. A 2024 meta-analysis examined the comparative impacts of the standard Western Mindfulness-Acceptance-Commitment (MAC) approach against a culturally adapted Chinese model known as Mindfulness-Acceptance-Insight-Commitment (MAIC) 2526. The culturally adapted MAIC model specifically reintegrated Eastern contextual elements, most notably the concept of philosophical "Insight." The results were striking: the culturally adapted model yielded substantially larger effect sizes across the board, significantly outperforming the Western model in improving both overall mindfulness and psychological flexibility among Chinese practitioners 2526. This strongly suggests that while the biological mechanisms of neuroplasticity are universal, the philosophical framework delivering the intervention matters deeply. Mindfulness is most effective when it aligns cohesively with the preexisting cultural and moral values of the practitioner 2627.
Global Guidelines and Institutional Perspectives
Given the robust evidence supporting both its efficacy and its potential risks, major health institutions worldwide have begun issuing formal guidance on the integration of mindfulness into public health strategies.
In the United States, the National Center for Complementary and Integrative Health advises that while mindfulness is effective for anxiety, depression, and PTSD, it should not be used to replace conventional care or to postpone seeing a healthcare provider for acute medical problems 17. They emphasize that patients should proactively inquire about the specific trauma training and clinical experience of their meditation instructors 17.
Internationally, governments are formally embedding mindfulness into national health policies. In 2023, Singapore's Ministry of Health launched a National Mental Health and Well-being Strategy, officially promoting mindfulness as a primary tool for mental wellness 462829. Furthermore, Singapore's Tripartite Advisory on Mental Well-being at Workplaces specifically encourages employers to integrate mindfulness training to mitigate work-related stress, alongside establishing formal peer support systems 4630.
Similarly, the Indian Council of Medical Research has explored the integration of ancient Eastern practices with modern clinical validation, supporting the rigorous evaluation of mindfulness-based interventions to address growing concerns like adolescent substance abuse, insomnia, and chronic stress 5031. Across the globe, the institutional consensus is clear: when applied with clinical rigor and cultural sensitivity, mindfulness represents a highly scalable, evidence-based pillar of modern psychiatric care.
Bottom line
The scientific evidence robustly supports clinical mindfulness programs as powerful interventions for anxiety, depression, and chronic stress. By fundamentally altering brain structure and functional connectivity, standardized programs can perform on par with standard antidepressants in maintaining remission for certain psychiatric conditions. However, meditation is not a risk-free panacea; the documented reality of adverse psychological effects necessitates a trauma-informed approach, ensuring that the practice is carefully adapted to the emotional safety and cultural background of the individual.