Rapamycin vs Metformin: What Human Longevity Trials Show
Human longevity trials indicate that while rapamycin demonstrates profound potential for immune rejuvenation and neuroprotection, it may blunt the beneficial adaptations of physical exercise. Metformin exhibits a safer, deeply established clinical profile with notable neuroprotective and epigenetic age-reversal effects in combination therapies, though recent meta-analyses suggest it lacks the absolute lifespan-extending power of rapamycin. Both remain strictly off-label for aging and require careful medical supervision as clinical guidelines continue to evolve.
The Biological Foundations of Gerotherapeutics
The pursuit of human life extension has largely transitioned from theoretical biology to actionable clinical pharmacology. Aging is increasingly understood not as an accumulation of random wear and tear, but as a heavily regulated biological process driven by specific cellular signaling pathways. As human life expectancy has increased, the gap between lifespan (total years lived) and healthspan (years lived free of chronic disease) has widened dramatically. The goal of modern geroscience is to bridge this gap by targeting the root molecular causes of aging.
Historically, the most robust and highly replicated method for extending healthspan and lifespan across species - from yeast to non-human primates - is dietary restriction 112. By reducing caloric intake without inducing malnutrition, organisms trigger deeply conserved evolutionary survival mechanisms. In a state of perceived nutrient scarcity, cellular metabolism shifts from a mode of active growth and proliferation into a protective "maintenance mode." This maintenance state prioritizes DNA repair, upregulates stress resistance, and initiates autophagy - a cellular recycling process that clears out damaged proteins, dysfunctional mitochondria, and toxic debris 145.
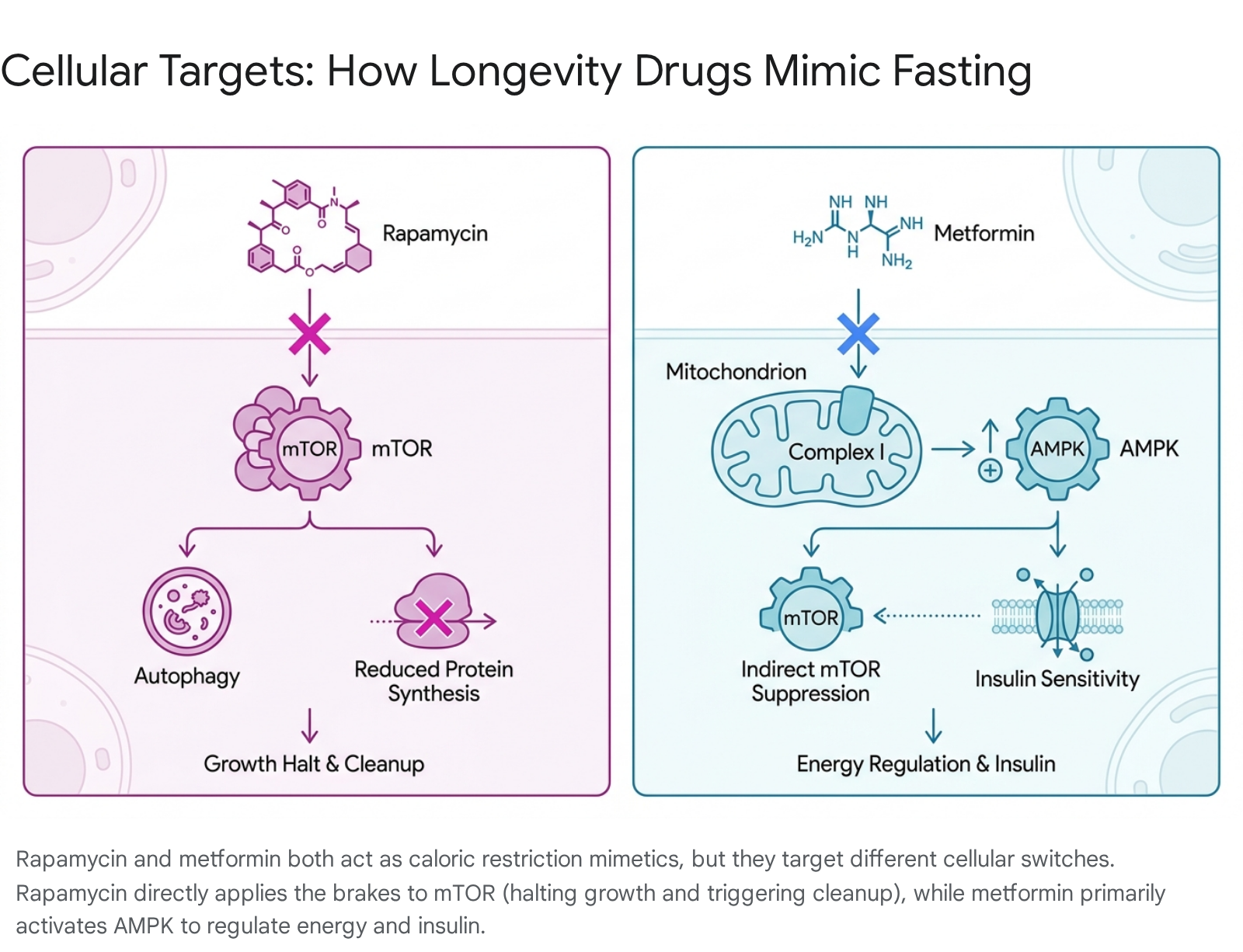
However, strict, long-term caloric restriction is exceptionally difficult for humans to maintain and can carry risks of frailty and immunosuppression. Consequently, the longevity field has focused intensely on identifying "caloric restriction mimetics" - pharmacological agents that chemically deceive the body's nutrient-sensing pathways into activating these longevity programs without requiring actual starvation 256. Today, two prescription drugs dominate this landscape: rapamycin and metformin. Though they are prescribed for vastly different conventional indications, both intersect intimately with the cellular machinery that governs aging.
Rapamycin: The Allosteric Brake on mTOR
Rapamycin (generic name sirolimus) is a macrolide compound first isolated in 1975 from a soil bacterium, Streptomyces hygroscopicus, found on Easter Island (Rapa Nui) 434. In conventional medicine, rapamycin is an FDA-approved immunosuppressant utilized primarily to prevent organ rejection in kidney transplant recipients and to coat coronary stents to prevent arterial re-narrowing 1910.
Its relevance to longevity stems from its specific molecular target, which was named after the drug itself: the mechanistic target of rapamycin (mTOR).
The Mechanics of mTOR Inhibition
mTOR is a central protein kinase that functions as a master metabolic switch, integrating signals from nutrients, insulin, and growth factors to regulate cell growth, proliferation, and survival 1411. It exists in two distinct functional complexes: mTORC1 and mTORC2.
In young, healthy organisms, mTOR signaling is highly dynamic, turning on to build tissue after a meal and turning off during fasting to allow for cellular repair. However, as organisms age, mTOR signaling tends to become chronically hyperactive. This continuous "on" state drives several hallmarks of aging. It prevents the initiation of autophagy, allowing damaged organelles to accumulate, and it drives the creation of senescent cells - cells that have stopped dividing but refuse to undergo apoptosis (programmed cell death) 14. Instead, these senescent cells secrete a toxic cocktail of inflammatory molecules known as the senescence-associated secretory phenotype (SASP), which damages surrounding healthy tissues 412.
Rapamycin acts by binding to an immunophilin protein (FKBP12), and this newly formed complex acts as a highly specific, allosteric inhibitor of mTORC1 13. By chemically forcing the mTORC1 brake pedal, rapamycin artificially mimics a state of nutrient deprivation. This intervention has proven to be the most reliably replicated pharmacological method for extending lifespan in mammalian models. Across dozens of independent laboratories, including the rigorous, multi-site Interventions Testing Program (ITP) funded by the NIH, rapamycin has consistently extended the median lifespan of genetically heterogeneous mice by 9% to 26%, even when administration begins late in life (the equivalent of a human starting the drug at age 60) 1414.
However, chronic high-dose rapamycin administration can eventually inhibit mTORC2, which is associated with detrimental metabolic side effects, including glucose intolerance, insulin resistance, and altered lipid profiles 1314. This has led longevity physicians to adopt intermittent, low-dose protocols (typically once weekly) to selectively target mTORC1 while sparing mTORC2 1415.
Metformin: The AMPK Activator and Metabolic Regulator
Metformin is fundamentally different in origin and mechanism. Derived from compounds found in the French lilac (Galega officinalis), metformin has been utilized clinically since the 1950s and was approved by the FDA in the 1990s as the first-line pharmacotherapy for type 2 diabetes 5618. Today, it is one of the most widely prescribed and extensively studied medications globally, boasting decades of long-term human safety data 1618.
While metformin has a well-established capacity to lower blood glucose, its exact mechanisms of action have proven surprisingly complex and multi-faceted, extending far beyond simple glycemic control.
Mitochondrial Complex I, AMPK, and the Brain-Gut Axis
For years, the primary consensus held that metformin acted primarily in the liver. At the cellular level, metformin mildly inhibits mitochondrial respiratory chain complex I 1197. This mild suppression of the cell's energy-producing machinery decreases the ratio of ATP to ADP, creating a localized energy deficit. This subtle cellular stress powerfully activates AMP-activated protein kinase (AMPK) 119.
AMPK acts as an evolutionary counterweight to mTOR. When AMPK detects low energy availability, it triggers a cascade of catabolic processes that improve insulin sensitivity, reduce hepatic glucose production, and lower systemic inflammation 11319. Crucially, the activation of AMPK by metformin also acts as an upstream inhibitor of mTORC1, effectively yielding some of the same downstream autophagic benefits as rapamycin, albeit less potently and through an indirect, metabolic pathway 119.
Recent research from 2024 to 2026 has radically expanded our understanding of metformin's mechanism, revealing that its geroprotective effects heavily involve the gut microbiome and the central nervous system. In the gastrointestinal tract, metformin alters the composition of the microbiota, specifically promoting the aggressive growth of Akkermansia muciniphila. This bacterial strain is highly associated with improved glucose tolerance, a fortified intestinal barrier, and increased secretion of Glucagon-like Peptide-1 (GLP-1) from intestinal L-cells 12.
Furthermore, groundbreaking 2026 data published in Science Advances demonstrated that metformin's metabolic benefits are highly dependent on neural signaling. Researchers discovered that metformin acts on a specific protein called Rap1, located in the ventromedial hypothalamus (VMH) of the brain. At clinically relevant, low doses, metformin activates a specific subset of neurons (SF1 neurons) entirely dependent on the presence of Rap1. When Rap1 was genetically removed from these neurons in mouse models, metformin completely lost its ability to regulate blood sugar, proving that the drug operates as a vital signaling agent across the brain-gut axis, responding to much lower drug concentrations in the brain than required in the liver or intestines 8.
The Preclinical Foundation: A Massive Meta-Analysis
Before evaluating the highly nuanced results of human clinical trials, it is necessary to establish the absolute baseline of preclinical data. A monumental meta-analysis published in Aging Cell in June 2025 by Ivimey-Cook et al. sought to resolve decades of conflicting animal data regarding these compounds 25.
The researchers compiled data from 167 published scientific papers, isolating 911 specific effect sizes across eight distinct non-human vertebrate species (ranging from fish to rhesus macaques, with the vast majority being mice and rats) 129. The primary goal was to compare the lifespan-extending efficacy of rapamycin and metformin against the gold standard of dietary restriction.
The meta-analysis delivered a definitive conclusion regarding absolute lifespan. The data showed that dietary restriction robustly and reliably extended both mean and median lifespan across vertebrate species 12. Crucially, rapamycin mirrored this success, producing a statistically significant lifespan extension that rivaled, and in some models exceeded, the benefits of dietary restriction 26. Furthermore, rapamycin's efficacy was consistent across both males and females, dispelling earlier concerns of severe sex-specific efficacy gaps 26.
In stark contrast, the meta-analysis concluded that metformin failed to produce a reliable, statistically significant extension of absolute lifespan in healthy vertebrates 126. While prior studies have shown metformin to be highly effective at extending the life of simpler invertebrates, such as the nematode C. elegans (by up to 50%), this geroprotective effect did not scale consistently into healthy, non-diabetic mammalian models 1610. The researchers cautioned that while metformin undoubtedly mitigates the morbidity of metabolic diseases, its capability to fundamentally alter the absolute lifespan ceiling of a healthy organism appears limited compared to the profound cellular reprogramming triggered by rapamycin 569.
Human Studies on Rapamycin: Progress and Paradoxes
With the preclinical superiority of rapamycin firmly established, translational geroscience has accelerated efforts to test the drug in human populations. Over the past decade, a wave of clinical data has emerged, attempting to define the parameters of off-label rapamycin use for healthy aging. The results highlight profound benefits in immunity and neuroprotection, alongside significant complexities regarding body composition and physical performance.
The PEARL Trial: Safety, Body Composition, and Dosing Complexities
Published in April 2025, the Participatory Evaluation of Aging with Rapamycin for Longevity (PEARL) trial represents a landmark achievement in the field. It was the first decentralized, double-blinded, randomized, placebo-controlled trial specifically designed to evaluate the long-term safety and efficacy of intermittent, low-dose rapamycin in healthy, normative-aging adults 41125. Crowdfunded with the support of Lifespan.io, the study enrolled 114 participants aged 50 to 85, who were randomized to receive a placebo, 5 mg, or 10 mg of compounded rapamycin once weekly for 48 weeks 32512.
The trial's primary endpoint was a reduction in visceral adiposity (visceral fat), a key marker of metabolic dysfunction and age-related decline. The study failed to meet this endpoint; there was no statistically significant change in visceral fat accumulation across any of the cohorts (ηp2=0.001, p=0.942) 1125. Furthermore, complex epigenetic aging clocks run on the participants showed no meaningful significant changes, failing to demonstrate a molecular age-reversal effect 1113.
However, the PEARL trial provided immense value in establishing a foundational safety profile. Over the course of the 48-week intervention, low-dose intermittent rapamycin was demonstrated to be highly tolerable. Reports of adverse and serious adverse events were statistically similar across both the rapamycin and placebo groups 112512. While minor gastrointestinal discomfort was reported slightly more frequently in the rapamycin arms, there was no spike in severe infections or immune challenges 1112.
The trial also uncovered intriguing, sex-specific secondary benefits. Women utilizing the 10 mg weekly dose demonstrated statistically significant improvements in lean tissue mass, alongside notable reductions in self-reported pain scores (ε2=0.168, p=0.015) 112528. Meanwhile, participants across both sexes in the 5 mg cohort reported significant improvements in generalized emotional well-being and overall health metrics 1112.
A critical caveat to the PEARL data emerged during the trial: pharmacokinetic testing revealed that the specifically compounded rapamycin capsules used in the study (chosen to match the appearance of the placebo) suffered from severe bioavailability issues. Blood concentrations measured 24 hours post-administration were approximately one-third of the expected levels seen in commercial rapamycin formulations (such as Pfizer's Rapamune) 1112. Consequently, the effective therapeutic dose received by the participants was drastically lower than intended, suggesting that future trials utilizing commercial formulations may yield more pronounced clinical effects.
Reversing Immunosenescence: The PROTECT Trials
One of the longest-standing medical dogmas regarding rapamycin is its role as an immunosuppressant. At high, daily trough levels required for transplant patients, rapamycin inhibits T-cell proliferation, intentionally suppressing the adaptive immune system to prevent organ rejection 41029.
However, geroscience has uncovered a powerful paradox: when administered intermittently at very low doses, rapamycin and its analogs (rapalogs) appear to aggressively rejuvenate the aging human immune system.
This paradigm shift is largely attributed to the seminal research of Dr. Joan Mannick. In 2014, Mannick published a randomized, observer-blind, placebo-controlled Phase 1 trial involving 218 healthy adults over the age of 65. The participants were given the rapamycin analog RAD001 (everolimus) for six weeks, followed by a two-week washout period, and were then administered the seasonal influenza vaccine 301415.
The results were unprecedented. The elderly cohorts receiving low-dose RAD001 (particularly the 0.5 mg daily or 5 mg weekly groups) exhibited a roughly 20% enhancement in their antibody response to the influenza vaccine compared to the placebo group 15. Blood analysis revealed the mechanism behind this rejuvenation: the mTOR inhibitor successfully reduced the percentage of CD4 and CD8 T-lymphocytes expressing the programmed death-1 (PD-1) receptor 1533. High PD-1 expression is a classic marker of T-cell "exhaustion" - a state where immune cells become sluggish and unresponsive due to age and chronic antigenic stimulation. By lowering PD-1, the rapalog effectively rescued these exhausted cells, restoring their functional capacity 301433.
Building on this success, Mannick spearheaded the PROTECT Phase 2a clinical trial in 2018. This expanded study shifted the clinical endpoint from surrogate vaccine responses to real-world disease incidence, tracking 264 elderly subjects to see if mTORC1 inhibition could reduce the actual rate of respiratory tract infections over a year 33. The trial demonstrated that low-dose mTOR inhibition successfully increased interferon-induced antiviral gene expression, providing a tangible reduction in laboratory-confirmed respiratory tract infections 293033. These trials proved that targeted, low-dose modulation of mTORC1 could safely counteract immunosenescence without triggering the dangerous metabolic side effects associated with mTORC2 suppression 33.
Neuroprotection and Alzheimer's Disease
As the global burden of neurodegenerative disease compounds, mTOR inhibition has emerged as a premier target for preserving brain architecture. The most compelling human data regarding rapamycin and brain health arrived in 2025 and 2026, centering on the ERAP (Evaluating Rapamycin Treatment in Alzheimer's Disease using Positron Emission Tomography) and REACH phase IIa pilot trials 341617.
These trials represent the critical translation of preclinical longevity data into the realm of human cognitive decline. Preclinical murine models of Alzheimer's disease previously demonstrated that rapamycin could reverse cognitive deficits, improve neurovascular coupling, and clear toxic amyloid-beta and tau protein aggregates via enhanced autophagy 161737.
In these early-stage human trials, cohorts of patients with early-stage Alzheimer's disease or amnestic mild cognitive impairment were administered an intermittent dose of 7 mg of oral rapamycin weekly for 26 weeks 1116.
In the natural trajectory of Alzheimer's disease, the brain experiences a progressive, localized failure to utilize glucose for energy, an effect distinctly visible on [18F]FDG-PET brain scans. Following six months of rapamycin therapy, researchers documented an extraordinary stabilization of cerebral glucose metabolism. Participants demonstrated no significant metabolic decline in prespecified high-risk cortical regions, including the posterior cingulate cortex, precuneus, and temporoparietal lobe 11. Exploratory analyses even identified localized metabolic increases in the putamen and anterior cingulate cortex, directly contradicting the expected hypometabolic decay characteristic of the disease 11.
Furthermore, a distinct 2025 study evaluating asymptomatic middle-aged individuals carrying two copies of the APOE4 gene - a genetic profile that increases Alzheimer's risk roughly 12-fold - found that just four weeks of rapamycin treatment significantly increased both cerebral blood flow and the physical volume of the hippocampus and caudate 37.
The ERAP trial also generated highly paradoxical, yet theoretically encouraging, biomarker data regarding cerebrospinal fluid (CSF). Typically, when neurologists see sharp spikes in structural proteins like total tau and neurofilament light chain (NfL) in the CSF, it indicates accelerated neuroaxonal damage and rapid brain cell death 11. Rapamycin treatment induced significant elevations in these exact proteins. However, concurrent structural MRI scans confirmed that the physical rate of brain atrophy had remained stable at approximately 1.2% over six months, noticeably lower than the expected 2% annualized decline associated with untreated Alzheimer's 11.
Researchers hypothesize that this uncoupling of fluid biomarkers from physical neurodegeneration suggests the protein surge was not a sign of acute toxicity, but rather an indicator of "secretory autophagy." The rapamycin was likely functioning exactly as intended - hyper-activating the cellular recycling machinery within the neurons, forcing them to violently flush out the accumulated toxic tau and amyloid proteins into the spinal fluid, thereby preserving the structural integrity of the brain 11.
The Exercise Paradox: Does Rapamycin Blunt Physical Gains?
While rapamycin exhibits profound capabilities for cellular cleanup and resting state rejuvenation, a significant clinical conflict has emerged regarding its interaction with physical exertion. Exercise remains the single most effective, evidence-based intervention for extending human healthspan 13. However, the physiological pathways required for exercise adaptation are in direct biological opposition to the mechanisms of rapamycin.
When a human engages in resistance training, the mechanical stress triggers an acute, massive spike in mTORC1 activity 39. This transient mTOR activation is the non-negotiable biological signal required to initiate muscle protein synthesis, drive hypertrophy, and repair micro-tears 40. By artificially clamping down on mTOR with a pharmacological inhibitor, physicians run the risk of inducing severe anabolic resistance, preventing the muscles from responding to the workout 13.
To test this "cycling hypothesis" - the idea that spacing the drug away from workouts could preserve adaptations - Dr. Brad Stanfield and an international team of researchers published a highly anticipated trial in the Journal of Cachexia, Sarcopenia and Muscle in April 2026 1340.
The trial tracked a cohort of sedentary older adults engaging in a supervised, 13-week resistance exercise program (three days per week). The experimental group received 6 mg of rapamycin once weekly, deliberately administered 24 hours after the final exercise session of the week to theoretically clear the drug from the system before the next workout 40.
The results indicated a clear interference effect. While both groups saw physical improvements from moving from a sedentary state to an active one, the older adults taking rapamycin gained measurably less strength and physical function compared to the placebo cohort . In the standardized 30-second chair-stand test - a vital clinical metric for lower-body strength and fall risk - the rapamycin group completed an average of two fewer repetitions than the placebo group 40. The rapamycin cohort also demonstrated higher instances of aches, fatigue, and lower self-rated physical well-being .
The researchers concluded that the 6 mg dose of rapamycin likely possessed a long enough biological half-life to linger in the tissues, chronically suppressing post-exercise mTOR activation and fundamentally blunting the human body's ability to undergo exercise-induced muscular adaptation 13.
Human Studies on Metformin: Deep Data and Epigenetic Reversal
While rapamycin commands the spotlight regarding absolute lifespan and targeted cellular therapies, metformin anchors the longevity field due to its unparalleled epidemiological history. Because the FDA approved metformin in 1995, geroscience benefits from analyzing millions of patient-years of data.
Observational Triumphs and the UKPDS
The longevity hypothesis for metformin originated from massive, retrospective population analyses, most notably the United Kingdom Prospective Diabetes Study (UKPDS) 1218. Epidemiologists uncovered a statistical anomaly: patients utilizing metformin to manage their type 2 diabetes were experiencing drastically lower rates of cardiovascular events, myocardial infarctions, and cancer mortality compared to diabetics managing their disease with insulin or sulfonylureas 121819.
More remarkably, subsequent analyses of large clinical practice databases revealed that in some cohorts, diabetic patients taking metformin exhibited longer survival rates than age-matched, non-diabetic, healthy controls 119. This suggested that metformin was conferring systemic physiological protections that extended beyond simple glycemic control.
However, observational data cannot prove causation. Diabetics take a multitude of medications, receive more frequent medical screening, and often implement strict lifestyle changes, all of which confound longevity statistics 519. To prove that metformin operates as a genuine geroprotector, researchers have established rigorous clinical trials targeting the biology of aging directly.
Transcriptomic Shifts: The MILES Trial
One of the earliest translational efforts was the Metformin in Longevity Study (MILES), a double-blind, placebo-controlled crossover clinical trial launched in 2014 1018. The trial aimed to investigate whether a daily dose of 1700 mg of metformin could alter the fundamental biology of aging in humans with impaired glucose tolerance 1018.
Instead of tracking decades of lifespan, researchers analyzed the transcriptomic signature of the participants. They extracted physical biopsies of skeletal muscle and adipose (fat) tissue and utilized RNA-Seq analysis to map the exact genes being expressed 18. The publication of the MILES data provided the first direct human evidence that metformin intervention actively modulates both metabolic and non-metabolic gene expression pathways, successfully shifting the biological "fingerprint" of the elderly tissues to more closely resemble the youthful gene expression profiles of healthy controls 101820.
Earning a Clinical Indication: The TAME Trial
The most ambitious project in the history of gerotherapeutics is currently underway: the Targeting Aging with Metformin (TAME) trial. Spearheaded by Dr. Nir Barzilai and coordinated by the Wake Forest University School of Medicine, TAME is a multi-site, double-blind, placebo-controlled trial designed to track 3,000 individuals between the ages of 65 and 79 over a six-year period 618.
TAME is revolutionary not because of the drug it utilizes, but because of its clinical endpoints. The trial is explicitly designed not to measure mortality independently, but rather to track a combined cluster of age-related morbidities: cardiovascular disease, cancer, cognitive decline, and mortality 56.
The primary goal of the TAME trial is regulatory rather than purely scientific. Currently, the FDA does not recognize "aging" as a disease; it only approves drugs for specific, isolated conditions 18. By proving that metformin can delay the onset of multiple, seemingly unrelated chronic diseases simultaneously, researchers hope to force the FDA to officially approve "aging" as a valid treatment indication 6. Earning this indication would trigger a paradigm shift, paving the way for pharmaceutical companies to aggressively fund and develop novel longevity compounds with a clear regulatory path to market 618.
While the trial design received FDA concurrence years ago, TAME has suffered from chronic, massive funding deficits because metformin is an off-patent, generic drug that costs pennies to manufacture, offering zero financial incentive for pharmaceutical investment 618. However, as of mid-2025, the trial is advancing under the operational umbrella of the Advanced Research Projects Agency for Health (ARPA-H), heavily supported by the American Federation for Aging Research (AFAR) 68.
Epigenetic Age Reversal: The TRIIM-X Trial
While metformin is often viewed as a mild, foundational geroprotector, it is currently a critical component of one of the most aggressive and successful age-reversal protocols in human history: the TRIIM (Thymus Regeneration, Immunorestoration, and Insulin Mitigation) trial family 444521.
The human thymus is a primary lymphoid organ essential for the maturation of T-cells. Beginning in puberty, the thymus undergoes profound involution, shrinking and replacing active immune tissue with fat, a process directly responsible for the catastrophic collapse of the immune system in old age (immunosenescence) 444521.
Led by Dr. Greg Fahy and Intervene Immune, the TRIIM protocol hypothesizes that thymus involution is not permanent. Prior animal data demonstrated that Recombinant Human Growth Hormone (hGH) possesses the unique ability to regenerate thymic tissue 4447. However, hGH therapy carries a massive risk: it is highly diabetogenic, inducing severe insulin resistance that accelerates aging 4447.
To counter this, the TRIIM protocol pairs hGH with two protective agents: DHEA (a hormone that protects against the diabetogenic effects) and metformin (to aggressively support insulin sensitivity and lower hepatic glucose) 4447.
The results of the initial one-year pilot trial were staggering. Not only did the participants experience the physical regeneration of their thymus glands accompanied by a resurgence of youthful immune function, but they also demonstrated a systemic reversal of biological aging 4748. Across four independent epigenetic DNA methylation clocks, the participants experienced an average biological age reversal of 2.5 years 47.
Crucially, researchers concluded that metformin was not merely a passive shield against insulin spikes in this protocol. As the expanded TRIIM-X trial (incorporating women and a wider age range) continues to yield data in 2025 and 2026, researchers note that metformin and DHEA exert profound, independent anti-aging effects that work synergistically with hGH to unwind the epigenetic markers of cellular decay 4445.
The 2024 Primate Breakthrough
While human epidemiological data is vast, controlled human lifespan studies take decades to mature. Therefore, the longevity community relies heavily on non-human primate models to simulate human outcomes. In late 2024, a landmark, exhaustive 40-month study published in the journal Cell provided the most compelling evidence to date for metformin's systemic anti-aging properties in higher mammals 225051.
Researchers administered daily, clinically relevant doses of metformin to elderly male cynomolgus macaques (aged 13 - 16 years, the equivalent of 40 - 50 human years) 2250. Utilizing highly advanced, multi-dimensional biological aging clocks (including pan-tissue transcriptomics, DNA methylomics, plasma proteomics, and single-cell aging assessments), the researchers mapped the drug's effect across 68 distinct biological parameters 225023.
The physiological improvements were systemic, mitigating periodontal bone loss, skin aging, and tissue degeneration in the lungs and liver 225123. However, the most explosive findings localized to the central nervous system. Metformin exerted an overwhelming neuroprotective effect, physically preserving the structural thickness of the frontal and parietal lobes - areas critical for higher-order cognitive function that inevitably atrophy with age 2251.
Cognitive testing confirmed that the macaques on metformin retained superior learning abilities, memory retention, and overall cognitive resilience 2251. When assessed via molecular aging clocks, the metformin cohort exhibited an astonishing 6-year regression in biological brain aging markers, effectively winding back the neurological clock by the equivalent of 15 to 18 human years 85023. This profound neurological rescue was determined to be mediated, in part, by metformin's activation of Nrf2, a master transcription factor that unleashes massive intracellular anti-oxidative defenses 2250.
Summary of Major Human Trials
| Trial / Study | Drug Used | Primary Endpoint / Focus | Key Findings & Current Status |
|---|---|---|---|
| PEARL 1112 | Rapamycin (5/10mg weekly) | Visceral adiposity; safety | Visceral fat endpoint missed. Safe over 48 weeks. Lean mass/pain improvements in women. |
| PROTECT 1533 | RAD001 (Rapalog) | Immunosenescence; vaccine response | 20% boost in flu vaccine response. Decreased exhausted PD-1 T-cells. Lowered infection rates. |
| ERAP / REACH 3416 | Rapamycin (7mg weekly) | Alzheimer's; FDG-PET glucose uptake | Stabilized brain glucose metabolism. Increased brain volume/blood flow in APOE4 carriers. |
| Stanfield 40 | Rapamycin (6mg weekly) | Resistance exercise adaptation | Blunted strength gains (chair-stand test) compared to placebo due to mTOR anabolic suppression. |
| MILES 1018 | Metformin (1700mg daily) | Gene expression in muscle/fat | Shifted transcriptomic markers in elderly tissues toward a more youthful profile. |
| TAME 6 | Metformin | Multimorbidity delay (aging indication) | Ongoing via ARPA-H. Targeting 3,000 subjects over 6 years. |
| TRIIM / TRIIM-X 4547 | Metformin + hGH + DHEA | Thymus regeneration; epigenetic age | 2.5-year reversal of epigenetic DNA clocks. Thymus regrowth. Metformin acts as metabolic shield and active geroprotector. |
Assessing the Clinical Risks and Off-Label Realities
The aggressive repurposing of these pharmaceuticals has led to widespread off-label use in specialized longevity clinics and biohacking communities. However, neither drug is FDA-approved for the treatment of aging, and both carry specific, clinically documented risks that demand rigorous physician oversight. In fact, major financial institutions like Swiss Re have begun drafting formal insurance guidelines strictly addressing the actuarial impact and risks of the exploding "longevity drug" market 53.
The Dangers of Unsupervised Rapamycin
While the PEARL trial demonstrated general tolerability at 5 to 10 mg weekly, unsupervised rapamycin use is fraught with biochemical hazards. In a detailed observational survey of 333 off-label rapamycin users, the most frequently reported adverse event was the development of painful aphthous ulcers (mouth sores/canker sores), indicating localized mucositis 11015.
More critically, mTOR operates heavily in glucose and lipid regulation. Even on intermittent dosing schedules, rapamycin has been documented to disrupt metabolic homeostasis, leading to elevated blood sugar, increased insulin resistance, and undesirable shifts in lipid profiles (elevated LDL cholesterol and triglycerides) 102425. While intermittent dosing is theorized to circumvent the severe immunosuppression seen in transplant patients, rapamycin users remain at an elevated risk for bacterial infections and delayed wound healing; longevity physicians universally recommend halting the drug immediately at the first sign of any significant illness or prior to surgery 410.
The Tolerability Profile of Metformin
Metformin benefits from an exceptionally deep safety history, yet it is not universally tolerated. The primary barrier to compliance is severe gastrointestinal distress; approximately 20% of users report nausea, cramping, and diarrhea upon initiation 1.
From a long-term longevity perspective, chronic metformin administration is highly correlated with the depletion of Vitamin B12, requiring active supplementation and monitoring to prevent hematological and neurological complications 112. In patients with impaired renal clearance (CKD), metformin carries a highly publicized, though exceptionally rare, risk of lactic acidosis - a life-threatening metabolic emergency 17.
Furthermore, mirroring the rapamycin exercise paradox, metformin has been clinically shown to blunt the physiological adaptations of aerobic cardiovascular training. A landmark 2019 study (Walton et al.) demonstrated that metformin physically reduced mitochondrial biogenesis in older adults engaged in aerobic exercise routines, limiting their peak cardiorespiratory fitness gains 1. This energy-limiting effect during intense exertion forces many longevity physicians to strategically pause metformin dosing on heavy training days 156.
The Synergy Hypothesis: Why Clinics Combine Both
Rather than viewing rapamycin and metformin as strict competitors, the modern vanguard of longevity medicine often approaches them as complementary therapies. Because they operate on opposing, yet interconnected, nutrient-sensing pathways, combining them theoretically maximizes cellular coverage 156.
A standard protocol utilized by prominent longevity physicians involves prescribing daily metformin to activate AMPK, establish robust insulin sensitivity, and maintain a constant, low-level suppression of systemic inflammation 1. To this baseline, physicians add a once-weekly "pulse" of low-dose rapamycin. This pulse acts as a precision strike, temporarily shutting down mTORC1 to trigger a deep wave of autophagy and cellular recycling, before clearing from the system quickly enough to avoid crushing the immune system or inducing severe insulin resistance 156.
This dual approach attempts to harvest the absolute lifespan-extending power and neural cleanup of rapamycin while relying on the metabolic shielding and deep historical safety data of metformin 157.
Bottom line
Human clinical trials over the last decade have dramatically advanced our understanding of gerotherapeutics. Rapamycin remains the most potent biological agent for absolute lifespan extension and deep cellular rejuvenation, showing profound clinical promise in reversing immune exhaustion and preserving brain architecture in early Alzheimer's disease. Metformin, conversely, lacks the brute-force lifespan extension seen in animal models but provides a deeply validated, safe foundation for metabolic regulation, with recent primate and human epigenetic trials highlighting its role in complex neuroprotection and age-reversal protocols. However, because both drugs harbor unique side effects - and notably exhibit the capacity to blunt the structural benefits of physical exercise - their off-label integration into a longevity regimen requires highly personalized, expert medical supervision.