Mechanisms and clinical trials of red light therapy
Introduction
Photobiomodulation (PBM), historically referred to in the literature as low-level laser therapy (LLLT) or cold laser therapy, represents a biomedical intervention utilizing non-ionizing optical radiation in the visible red and near-infrared (NIR) electromagnetic spectrum. The primary clinical objective of this modality is to elicit photophysical and photochemical events at the cellular level that subsequently promote tissue repair, reduce systemic and localized inflammation, and modulate nociception 1. The therapy was initially observed and developed in the 1960s, but it struggled for decades with clinical skepticism, frequently relegated to the periphery of conventional medicine due to an incomplete understanding of its exact intracellular mechanisms and highly variable clinical outcomes 21.
Over the past two decades, photobiomodulation has firmly transitioned from an empirical, observational modality to a deeply researched, evidence-based intervention 22. The accumulation of more than 5,000 peer-reviewed studies - including hundreds of randomized controlled trials (RCTs) - has systematically elucidated the intracellular signaling cascades triggered by targeted wavelengths, primarily located between 600 nm and 1100 nm 156. Despite this robust mechanistic validation in preclinical settings, the translation to human clinical application remains complex. Treatment outcomes are exceptionally sensitive to technical parameters such as wavelength, energy density (fluence), power density (irradiance), and the timing of the intervention 27. Furthermore, the aggressive commercialization of PBM devices in the wellness sector has outpaced the standardization of clinical protocols, leading to pervasive methodological heterogeneity and significant industry funding bias across the published literature 3.
This report systematically examines the biological mechanisms underpinning photobiomodulation, critically evaluates the clinical trial evidence across diverse medical and athletic applications, assesses the safety profile and physiological contraindications, and analyzes the structural challenges regarding dosimetry standardization and industry influence within the current body of research.
Biological Mechanisms of Action
The therapeutic physiological effects of photobiomodulation are strictly nonthermal. Unlike high-intensity surgical lasers designed to ablate, cut, or coagulate tissue through the generation of localized heat, PBM relies exclusively on the absorption of specific photons by endogenous photoacceptors 14. These photoacceptors are molecules containing chromophores capable of transducing optical light energy into biochemical signals, initiating a cascade of secondary cellular reactions 14.
Chromophore Absorption and Mitochondrial Bioenergetics
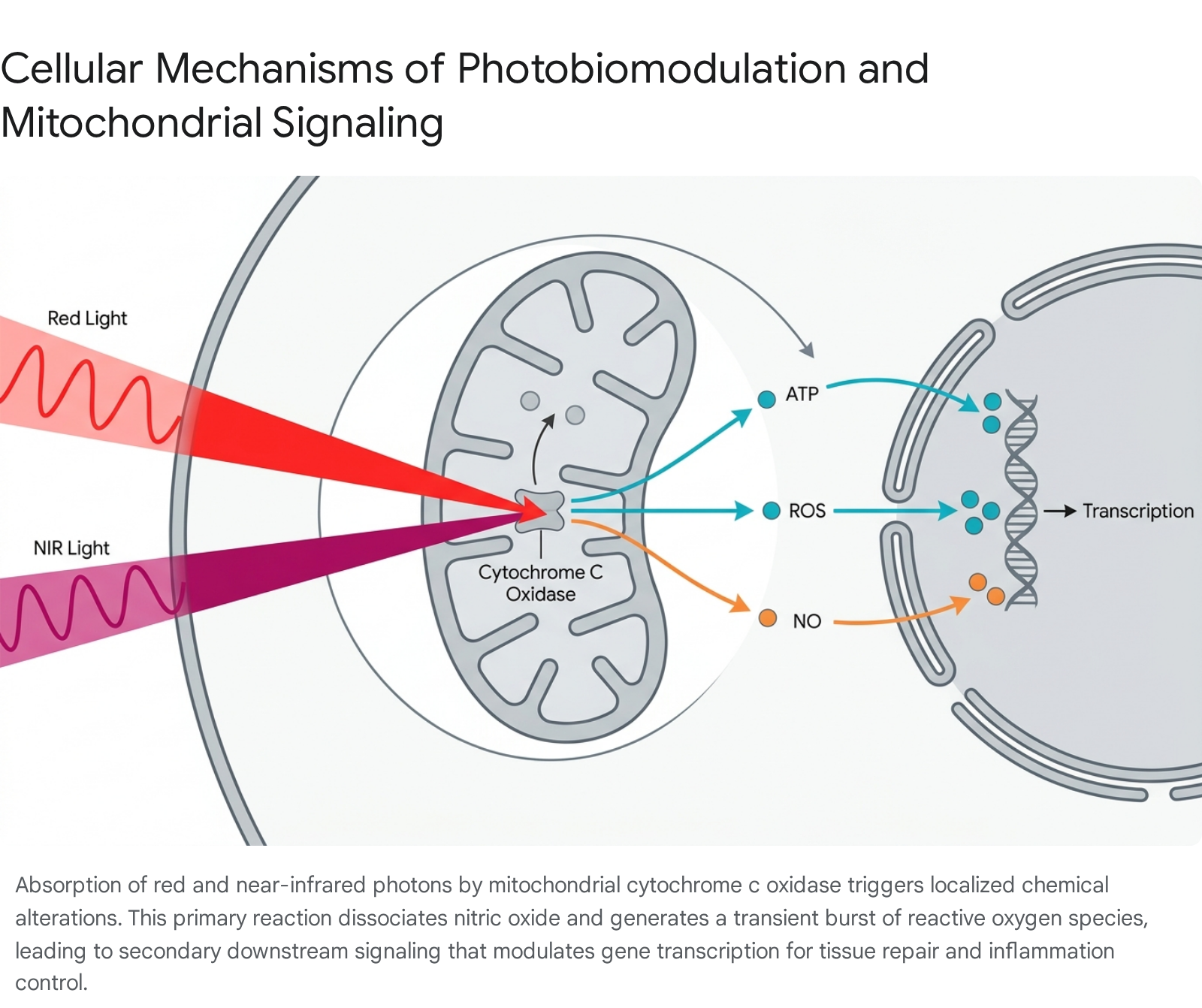
The primary and most extensively validated photoacceptor for red and near-infrared light in mammalian tissue is cytochrome c oxidase (CCO), also designated as Complex IV 410. Cytochrome c oxidase is the terminal enzyme in the mitochondrial electron transport chain, directly responsible for the reduction of oxygen to water - a vital and rate-limiting step in the synthesis of cellular adenosine triphosphate (ATP) 10.
Cytochrome c oxidase contains two distinct heme groups (heme $a$ and heme $a_3$) and four copper centers ($Cu_A$ and $Cu_B$) that actively participate in electron transfer. These metal centers exhibit distinct, inherent absorption spectra that directly match the red and near-infrared wavelengths utilized in clinical PBM protocols 10. When photons within these specific targeted ranges (typically 600 - 850 nm) penetrate human tissue and are absorbed by the CCO chromophores, the molecular and electronic structure of the enzyme is transiently altered 410.
A central biochemical event occurring during this primary photochemical reaction is the photodissociation of nitric oxide (NO). Under conditions of cellular stress, injury, or hypoxia, NO can competitively bind to the copper and heme centers of CCO, physically displacing oxygen and severely downregulating cellular respiration 110. Photon absorption provides the energy required to physically dissociate NO from the enzyme, restoring oxygen binding capacity and rapidly upregulating the efficiency of the electron transport chain 10. The immediate physiological consequence of this dissociation is a measurable, rapid surge in mitochondrial ATP synthesis, which provides depleted or damaged cells with the necessary bioenergetic resources to initiate systemic repair 2410.
Reactive Oxygen Species and Downstream Transcription
While chronically high levels of reactive oxygen species (ROS) induce oxidative stress, lipid peroxidation, and tissue damage, the highly localized, transient increase in ROS generated by PBM acts as a critical secondary signaling mechanism 10. The sudden increase in electron transport chain activity generated by photon absorption transiently elevates local ROS concentrations 10.
This temporary shift in cellular redox homeostasis acts as a highly effective hormetic stressor, triggering the activation of numerous redox-sensitive transcription factors situated in the cytosol 105. Key transcription factors acutely responsive to this cascade include Nuclear factor kappa B (NF-κB), which modulates the expression of hundreds of genes involved in cellular survival and the inflammatory response; Activator protein 1 (AP-1), which regulates gene expression in response to various environmental stimuli, influencing cellular proliferation and differentiation; and Hypoxia-inducible factor 1-alpha (HIF-1α), which promotes angiogenesis and structural cellular adaptation to hypoxic stress 10.
Once activated by the initial ROS burst, these transcription factors migrate to the cell nucleus, where they actively alter the expression of genes responsible for antioxidant defense mechanisms (including the upregulation of superoxide dismutase and glutathione peroxidase), structural tissue repair, and the modulation of both pro-inflammatory and anti-inflammatory cytokines 4105. Ultimately, this genetic modulation leads to secondary, macro-level physiological reactions including increased fibroblast proliferation, enhanced extracellular matrix production, optimized cellular migration, and improved local microcirculation 46.
The Temporal Sequence of Cellular Events
Recent advanced transcriptomic analyses have mapped the chronological sequence of cellular events following PBM exposure, revealing a highly dynamic and time-dependent biological response. Research utilizing human SH-SY5Y neuroblastoma cell lines exposed to 670 nm continuous-wave light revealed that PBM induces distinctly different intracellular transcriptomic profiles depending on the exact timeframe of measurement post-irradiation 78.
In the early phase (defined as up to 8 hours post-irradiation), the cellular response is heavily characterized by the statistical enrichment of molecular pathways related to active transcriptional regulation and acute cellular stress responses 78. Conversely, in the late phase (measured at 24 hours post-irradiation), the global transcriptomic profile demonstrates a physiological shift toward downstream pathways conventionally associated with cell death, apoptosis regulation, and DNA damage signaling 78. This temporal progression provides compelling support for the hypothesis that PBM functions essentially as a transient, low-level stressful stimulus. By briefly simulating oxidative stress and initiating early-phase transcription, PBM actively recruits and activates endogenous protective and reparative pathways, ultimately resulting in enhanced long-term cellular resilience and neuroprotection 78.
Dosimetry and the Biphasic Dose Response
A defining and often misunderstood characteristic of photobiomodulation is its strict adherence to the Arndt-Schulz law, which asserts that weak stimuli excite physiological activity, moderate stimuli favor it, strong stimuli retard it, and very strong stimuli arrest it entirely 7. In the specific context of PBM, this principle manifests as a sharp biphasic dose-response curve, meaning therapeutic benefits are heavily dependent on delivering a highly specific quantity of optical energy 210.
Wavelength Specificity and Tissue Penetration Profiles
The efficacy of PBM is fundamentally dependent on selecting the appropriate wavelength to reach the designated target tissue depth. Different wavelengths possess distinct optical penetration properties governed by the scattering and absorption coefficients of water, melanin, and hemoglobin present in human tissue 115.
| Wavelength Range | Spectrum Designation | Estimated Tissue Penetration Depth | Primary Clinical Applications |
|---|---|---|---|
| 630 - 680 nm | Visible Red Light | Superficial (1 - 5 mm). Absorbed primarily in the epidermis and dermis. | Wound healing, acne treatment, fine lines, skin rejuvenation, androgenetic alopecia (hair follicle stimulation). 151617 |
| 780 - 850 nm | Near-Infrared (NIR) | Deep (up to 5 cm). Penetrates through the cutaneous layers into underlying soft tissue. | Muscle recovery, tendinopathies, osteoarthritis, deep joint pain, fascial inflammation. 715 |
| 810 nm & 1064 nm | Deep Near-Infrared | Very Deep / Transcranial. Capable of penetrating the human cranium. | Traumatic brain injury, major depressive disorder, mild cognitive impairment, Parkinson's disease. 151819 |
Clinical protocols targeting highly superficial conditions, such as hair follicle stimulation in androgenetic alopecia, strictly utilize red wavelengths (typically 650 - 670 nm). Because the target stem cells reside only 2 - 5 mm below the scalp surface, the deeper penetration afforded by NIR is entirely unnecessary and may lead to unwanted systemic effects 717. Conversely, deep musculoskeletal applications routinely combine red and NIR wavelengths in a single array to target the entire cross-section of the affected anatomy simultaneously, ensuring photons reach deep capsular structures while also addressing superficial inflammation 715.
Fluence, Irradiance, and the Arndt-Schulz Curve
Accurate dosimetry in PBM relies on the calculation of fluence (also referred to as energy density), which is universally measured in Joules per square centimeter ($J/cm^2$). The core equation utilized in clinical settings is: $Fluence = Irradiance (W/cm^2) \times Time (seconds)$ 7.
Extensive clinical and preclinical data demonstrate that an energy dose between 3 and 50 $J/cm^2$ typically constitutes the effective therapeutic window for the vast majority of medical conditions 7. Doses falling significantly below this threshold (under 2 $J/cm^2$) provide insufficient cellular stimulation to yield measurable clinical outcomes, functioning effectively as a placebo 7. Conversely, arbitrarily escalating the energy dose does not yield linearly increasing clinical benefits. Doses exceeding 50 - 80 $J/cm^2$ begin to exhibit rapidly diminishing returns, and severe overdosing (exceeding 100 $J/cm^2$) triggers the Arndt-Schulz inhibitory effect 7. At this extreme threshold, the massive influx of optical light energy generates excessive and unmanageable ROS, physically reversing the therapeutic benefits, halting fibroblast proliferation, and potentially inducing unwanted cellular apoptosis 75.
This exceptionally narrow therapeutic index explains a vast majority of the conflicting or entirely negative results observed in the published literature. Clinical trials utilizing arbitrary dosing parameters that fall outside the optimal window consistently fail to demonstrate efficacy, underscoring the absolute necessity for standardized dosimetry 218.
Clinical Trial Evidence by Medical Application
The body of evidence evaluating photobiomodulation spans over 5,000 peer-reviewed studies and encompasses more than 700 randomized controlled trials evaluating dozens of discrete indications 57. The evidence base, however, remains highly heterogeneous, varying wildly in device specifications, treatment frequency, participant demographics, and methodological rigor 3.
Musculoskeletal Pain and Tendinopathies
Chronic musculoskeletal pain management is one of the most thoroughly investigated domains for PBM. A recent and comprehensive systematic review encompassing 53 clinical trials (representing approximately 2,800 patients) concluded that PBM consistently decreases mean visual analog scale (VAS) pain scores by roughly 32% (ranging from 28% to 40%) compared to sham interventions across conditions such as knee osteoarthritis, tendinopathies, and nonspecific low back pain 6. Similarly, standardized functional assessment scores (including the WOMAC, ODI, and NDI metrics) improved by 18 - 25% when PBM was integrated into the rehabilitation protocol 6.
To standardize these treatments, the World Association for Laser Therapy (WALT) produces condition-specific dosage recommendations based on continuous reviews of RCTs 20219.
| Target Condition | Wavelength Recommendation | Dose Recommendation (Joules per point) | Additional Clinical Parameters |
|---|---|---|---|
| Carpal Tunnel Syndrome | 780 - 820 nm | Minimum 4 Joules | Direct application to 2-3 points along the nerve path. 21 |
| Lateral Epicondylitis | 780 - 820 nm | 4 Joules | Maximum irradiance of 100 $mW/cm^2$ applied to 1-2 specific points. 21 |
| Achilles Tendinopathy | 780 - 820 nm | Minimum 8 Joules | Maximum irradiance of 100 $mW/cm^2$ applied to 2-3 specific points. 21 |
| Glenohumeral Joint Arthritis | 780 - 820 nm | Minimum 4 Joules | Applied across 2-4 points depending on joint circumference. 21 |
Despite these established guidelines, evidence certainty is not uniform across all musculoskeletal conditions. In the treatment of Patellofemoral Pain Syndrome (PFPS), for instance, meta-analyses incorporating eight RCTs (n=340) indicate a statistically significant reduction in pain (Standardized Mean Difference [SMD] = -0.83; 95% CI -1.40 to -0.27) when PBM is combined with conventional exercise 10. However, the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) evaluation for the certainty of this evidence was rated as "very low." This heavily downgraded rating was driven by severe methodological inconsistencies between the trials, a high risk of bias across five of the eight studies, and considerable imprecision in the reported effect estimates 1011.
Fibromyalgia and Systemic Pain Syndromes
PBM has gained significant attention in the management of Fibromyalgia syndrome, a highly complex condition characterized by central sensitization and widespread mitochondrial dysfunction 212. Clinical trials demonstrate significant, sustained reductions in tender point counts and overall pain intensity.
Interestingly, researchers have evaluated both localized laser applications directed onto specific trigger points and whole-body PBM beds. A triple-blinded, randomized controlled trial utilizing a NovoTHOR whole-body system (delivering 660 - 850 nm light globally at 25.2 $J/cm^2$) over 12 to 18 sessions produced large, durable reductions in pain scores, alongside significant improvements in the Fibromyalgia Impact Questionnaire (FIQR) from 63.2 down to 45.6 (p < 0.001) 212. Systematic reviews conclude that whole-body PBM yields superior and more sustained long-term benefits in functional capacity and psychological indices compared to localized treatments. This superiority is likely due to the systemic modulation of nociceptive pathways, a widespread reduction in systemic inflammation, and improved autonomic regulation across a broader vascular network 212. Localized treatments, however, remain effective; protocols incorporating static magnetic fields (PBMT-sMF) via the FibroLux system demonstrated dramatic localized VAS score decreases from 80.64 to 37.80 following three weeks of targeted 60 Joule applications 12.
Muscle Recovery and Athletic Performance
The application of PBM as an ergogenic and recovery tool is deeply documented, with the most pronounced physiological effects occurring when the therapy is strategically applied prior to strenuous exercise rather than solely post-exertion 2627.
A comprehensive meta-analysis of 15 RCTs evaluated the specific effects of PBM on skeletal muscle recovery. Despite significant variance in the chosen wavelengths and doses (commonly utilizing 10 to 50 Joules directed per targeted muscle group), pre-exercise PBM consistently improved maximum voluntary contraction (MVC), increased the total time required to reach physical exhaustion, and significantly decreased post-exercise systemic markers of muscle damage - primarily circulating creatine kinase (CK) and localized markers of oxidative stress 26.
However, moderating variables significantly influence the magnitude of this effect. Data suggests a pronounced divergence in efficacy based on the anatomical target; PBM yields a statistically stronger endurance response in upper limb resistance exercises compared to lower limb exercises, potentially due to differences in muscle belly depth and total tissue mass 28. Furthermore, gender and sport-specific biomechanics fundamentally alter outcomes. Meta-analyses note that while PBMT decreases CK levels robustly in professional volleyball players, the data is highly inconsistent when applied to professional football (soccer) players 27. This discrepancy suggests that the differing metabolic demands and anatomical muscle densities of these sports dictate whether the applied optical photon dose successfully penetrates to actively fatiguing deep muscle fibers 27.
Transcranial Photobiomodulation for Neurological Disorders
Transcranial Photobiomodulation (tPBM) represents a frontier application, involving the delivery of near-infrared light (810 - 1064 nm) directly through the cranium to target the cerebral cortex and deeper brain structures 519. Because only approximately 5% of incident light successfully penetrates the human skull and cerebrospinal fluid, achieving a meaningful cortical fluence requires high-density irradiance (50 - 250 $mW/cm^2$) applied in prolonged, direct-contact sessions (10 - 25 minutes) 719.
Clinical findings indicate that tPBM facilitates neuroprotection and neuroplasticity. By boosting cerebral metabolism and modulating endogenous opioids, tPBM directly targets the neuro-inflammatory cascades present in several psychiatric and degenerative conditions 29. * Major Depressive Disorder (MDD): A pilot trial (ELATED-2) testing tPBM with NIR light against sham treatments reported strong antidepressant properties, yielding a medium-to-large effect size (Cohen's d = 0.75 to 1.5) for the reduction of HAM-D17 depression scores, with excellent patient tolerability and zero serious adverse events reported 29. * Cognitive Impairment: RCTs targeting older adults diagnosed with Mild Cognitive Impairment (MCI) documented significant clinical improvements in Montreal Cognitive Assessment (MoCA) scores alongside elevated serum levels of brain-derived neurotrophic factor (BDNF), demonstrating a structural response to the therapy 25. * Post-COVID Sequelae: Double-blind, sham-controlled trials evaluating patients suffering from Post-COVID-19 Condition (PCC) "brain fog" found that 8 weeks of daily home-based tPBM targeting the brain's default mode network significantly improved composite cognitive scores and sustained attention tasks, pointing to a measurable reversal of prolonged neuroinflammation 30. * Parkinson's Disease: An 8-week double-blind RCT evaluating PBM combined with exercise for Parkinson's Disease (utilizing treatments directed at the head, neck, and abdomen) found that patients who continued the PBM therapy over extended periods demonstrated significant improvements in timed up-and-go motor outcomes compared to non-continuers, supporting the hypothesis of continuous neuroprotection 31.
Oncology Supportive Care and Neuropathy
Photobiomodulation is increasingly and successfully integrated into supportive cancer care to manage the severe, dose-limiting side effects of chemotherapy and ionizing radiation. The World Association for Photobiomodulation Therapy (WALT) and the Multinational Association of Supportive Care in Cancer (MASCC) have issued evidence-based consensus guidelines endorsing specific optical parameters for prophylactic and therapeutic use in oncology 323334.
A critical clinical application is the management of chemotherapy-induced peripheral neuropathy (CIPN). Chemotherapeutic agents frequently induce severe sensory and motor nerve dysfunction. In a randomized controlled trial (the NEUROLIGHT trial), 60 cancer patients undergoing 6 PBM sessions using either 6 $J/cm^2$ or 8 $J/cm^2$ fluences exhibited significant reductions in modified Total Neuropathy Scores (mTNS) and notable improvements in physical mobility. Interestingly, the lower 6 $J/cm^2$ dose proved statistically superior in soothing active nociception compared to the higher dose, again illustrating the biphasic dose-response curve 3513.
PBM has also demonstrated potent prophylactic efficacy against radiation-induced tissue injury, particularly radiodermatitis and oral mucositis. Pre-treatment of tissues with PBM actively upregulates antioxidant enzymes like superoxide dismutase, directly mitigating the acute DNA damage, massive ROS generation, and apoptotic signaling cascades triggered by ionizing radiation therapy 534.
Dermatology, Wound Healing, and Alopecia
While animal models consistently demonstrate profound acceleration of wound healing, human clinical trials in dermatology have produced highly mixed results, largely due to poor methodological controls. A rigorous meta-analysis evaluating PBM for perineal pain and soft tissue wound healing following episiotomy found no statistically significant superiority over control interventions (Mean Difference = 0.94; 95% CI -0.69 to 2.56; p = 0.26) 14. The GRADE certainty of this specific evidence was rated as "very low" due to massive clinical heterogeneity and imprecision, suggesting that human soft-tissue repair responses to PBM are easily confounded by variations in standard clinical care protocols and inadequate, poorly reported optical dosing 14. Other complex wounds, such as venous leg ulcers, are currently the subject of large-scale RCTs investigating the synergistic effects of combining PBM (using 6 Joules per emitter) with standard compression therapy, though definitive superiority remains under investigation 15.
Conversely, evidence for PBM in the treatment of Androgenetic Alopecia (AGA) is exceptionally robust and standardized. The mechanism diverges slightly from deep musculoskeletal applications; isolated red light (630 - 680 nm) increases ATP production specifically in follicular stem cells and dermal papilla cells, upregulating growth factors (IGF-1, VEGF) and shifting dormant telogen follicles back into the active anagen growth phase 1739. Because the target hair follicles sit superficially, merely 2 - 5 mm deep, very low fluences (1 - 4 $J/cm^2$) are entirely sufficient, and NIR wavelengths are generally unnecessary 1739. RCTs consistently record terminal hair count increases of 20 - 35% above baseline after 3 to 6 months of compliant use 17.
Ophthalmic Applications
A highly specialized application of PBM has emerged in the treatment of intermediate dry age-related macular degeneration (AMD). Utilizing dedicated hardware, specifically the Valeda Light Delivery System (which received FDA authorization in November 2024), ophthalmologists can deliver precise, low-intensity, multi-wavelength light (590 nm, 660 nm, and 850 nm) directly to the retinal tissue 161718.
In contrast to intravitreal injections of complement inhibitors, which only slow the progression of geographic atrophy in advanced stages, targeted retinal PBM has shown the unique potential to actually improve visual function in select patients 161718. The procedure is non-invasive, requires no dilating agents, and is performed in an office setting. Due to its clinical validation, specific Category III CPT codes (e.g., 0936T for a single session) have been established to standardize billing and reporting for this novel therapy 161718.
Equipment Variability and Regulatory Standards
The explosion of direct-to-consumer red light therapy panels has severely complicated the clinical landscape. A critical and widely documented discrepancy exists between the marketed specifications of consumer wellness devices and their verified optical outputs.
True clinical-grade devices are rigorously tested to IEC 60601 standards, dictating medical electrical equipment safety, photobiological risk management, and precise output consistency 4344. Conversely, many unregulated commercial panels massively inflate their output statistics to appear competitive. Independent testing utilizing calibrated optical meters at standard 6-inch treatment distances reveals that while high-end clinical beds deliver accurate irradiance (e.g., ~130 $mW/cm^2$), heavily marketed mid-tier consumer panels (such as Joovv and PlatinumLED) deliver 85 - 95 $mW/cm^2$. Most concerning, budget panels widely available online deliver as little as 28 $mW/cm^2$ despite claiming outputs exceeding 120 $mW/cm^2$ 4546.
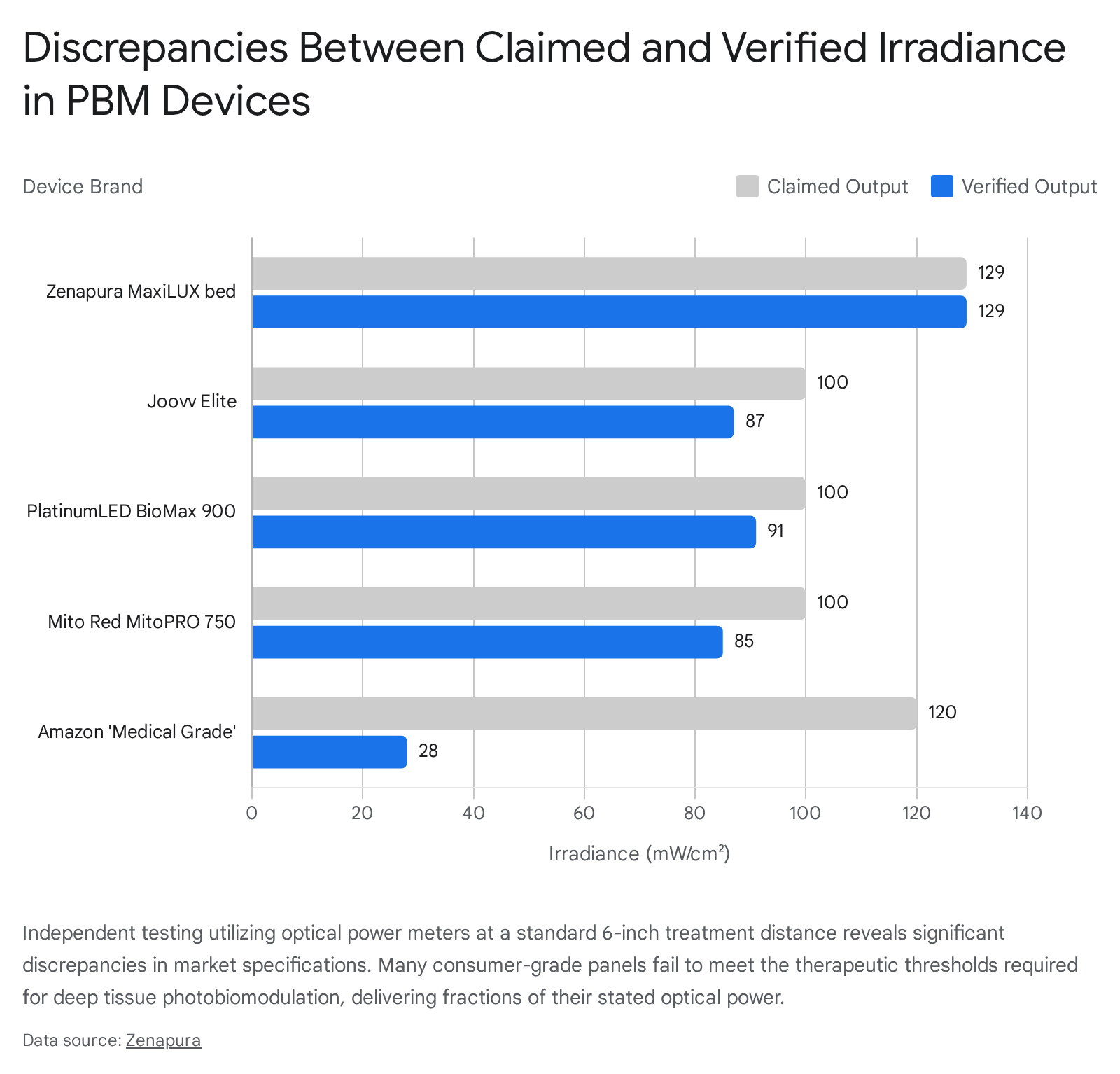
This severe optical deficit effectively renders budget devices sub-therapeutic for any deep tissue applications, resulting in purely placebo effects 46. Furthermore, consumer panels often emit higher levels of electromagnetic field (EMF) radiation due to unshielded components, which carries theoretical risks of exacerbating cellular inflammation and directly contravening the clinical goals of PBM 46. To navigate this, regulatory bodies like the EU Medical Device Regulation (MDR) rely on Annex XVI frameworks, clarifying that regulatory relevance and market access are determined by the intended therapeutic purpose and proven biological effect rather than the presence of LED technology alone 47.
Safety Profile and Contraindications
A defining feature of photobiomodulation is its exceptionally clean clinical safety profile. Across thousands of trials and tens of thousands of subjects, systematic reviews consistently confirm that adverse events are rare, mild, and uniformly transient 48. The most frequent adverse effects documented in RCTs include mild localized warmth, temporary erythema (redness) at the treatment site resulting from expected vasodilation, and occasional transient exacerbation of symptoms - representing a brief surge in localized inflammation before the long-term anti-inflammatory cascade takes effect 4849.
However, adherence to absolute and relative contraindications remains critical for clinical safety:
| Contraindication Category | Specific Condition | Clinical Rationale and Protocol |
|---|---|---|
| Absolute | Active Malignancies | PBM upregulates cellular metabolism, ATP synthesis, and proliferation. There is a theoretical risk that directing high-density light onto a malignant lesion could inadvertently accelerate tumor growth or metastasis. Explicit oncological clearance is required. 48505152 |
| Absolute | Unprotected Direct Ocular Exposure | Exposure to high-irradiance Class 3B lasers or powerful LED panels risks retinal thermal damage or phototoxicity. (Exceptions exist solely for FDA-authorized AMD treatments performed by ophthalmologists). 16484951 |
| Absolute | Photosensitive Conditions | Patients suffering from systemic lupus erythematosus, porphyria, or taking photosensitizing medications (tetracyclines, fluoroquinolones) risk severe phototoxic rashes. 48495051 |
| Relative | Recent Severe Burns | Fresh burns (within 24-48 hours) retain thermal energy; the mild heat generated by optical panels may worsen thermal damage. 4851 |
| Relative | Hyperthyroidism | Direct application over the thyroid gland is contraindicated to prevent overstimulation of glandular tissue. 4850 |
Methodological Limitations and Industry Bias
The greatest vulnerability in the current photobiomodulation research landscape is the prevalent and well-documented influence of industry sponsorship.
The Influence of Device Manufacturer Funding
As traditional federal research funding remains limited, many PBM investigators rely heavily on direct grants, equipment donations, and sponsorships from device manufacturers 1920. Systematic meta-research assessing industry sponsorship bias in medical literature indicates that trials funded by the medical device industry are significantly more likely to yield results favorable to the sponsor's product. A Cochrane systematic review analyzing this phenomenon calculated a risk ratio (RR) of 1.27 (95% CI: 1.17 to 1.37) for reporting favorable efficacy results, and an RR of 1.34 for drafting favorable overall conclusions in industry-sponsored trials compared to independently funded research 2156.
This bias rarely manifests through outright data fabrication. Instead, it occurs through subtle methodological choices during the trial design phase: selecting highly specific and unrepresentative patient populations, utilizing intentionally suboptimal dosing protocols for comparator sham groups (to guarantee the sponsor's device appears superior), and predominantly publishing only positive results while quietly withholding null or negative findings 205657. A recent meta-research study examining 285 systematic reviews in the PBM field found that only 45% had registered a priori protocols on platforms like PROSPERO. Of those that did register, nearly 72% failed to update their registry status post-publication, remaining classified as "ongoing" - strongly suggesting a high rate of selective reporting and the systemic abandonment of negative trials 3.
The Need for Standardized Reporting Frameworks
To combat this heterogeneity and lack of transparency, consensus efforts are pushing for the universal adoption of the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) statement. SPIRIT forces investigators to pre-define and rigorously document their clinical methodology, outcome measures, and statistical analysis plans before the trial even begins, preventing post-hoc data manipulation 22.
In PBM research specifically, investigators must adopt rigid standard reporting for optical parameters (often referred to as SPIRIT-PBM compliance). A clinical trial that merely states "red light was applied for 10 minutes" is scientifically useless and impossible to replicate. Exact specifications of wavelength, continuous versus pulsed wave operation (including specific Hertz frequency), irradiance, spot size, total Joules delivered, and exact beam geometry must be uniformly reported to ensure reproducibility and to mitigate the selective reporting of favorable operational parameters 3323.
Conclusion
Photobiomodulation is a biologically plausible, mechanistically highly complex, and increasingly clinically validated therapeutic modality. By deliberately leveraging the inherent absorption spectra of mitochondrial cytochrome c oxidase, targeted optical radiation can reliably upregulate cellular bioenergetics, modulate oxidative stress via localized ROS generation, and orchestrate systemic anti-inflammatory cascades through nuclear transcription factors. The body of clinical evidence robustly supports the utility of PBM in enhancing musculoskeletal recovery, managing specific chemotherapy-induced neuropathies, stimulating follicular hair growth, and offering neuroprotection in states of cognitive decline.
Nevertheless, the modality is strictly bound by unforgiving dosimetric constraints. The biphasic nature of the Arndt-Schulz curve demands absolute precision; deviations in irradiance or total fluence readily yield sub-therapeutic or entirely inhibitory outcomes. While the physiological safety profile of the intervention is remarkably benign across patient populations, the integrity of the clinical literature is frequently compromised by industry funding bias, selective reporting, and inadequate methodological standardization. Future advancements in photobiomodulation depend critically upon the widespread adoption of standardized dosing protocols (such as WALT recommendations), uncompromising transparency in conflict-of-interest reporting, and the deployment of large-scale, independently funded clinical trials designed specifically to isolate the optimal therapeutic parameters for discrete human pathologies.