What Is Cognitive Behavioral Therapy and Who Benefits Most
Cognitive behavioral therapy (CBT) is a structured, goal-oriented psychological treatment that helps individuals identify and change unhelpful thinking and behavioral patterns. The core premise is that psychological distress is often driven by deeply ingrained, faulty ways of processing the world around us. By actively challenging these cognitive distortions and practicing new coping skills, patients can achieve long-lasting relief from conditions ranging from depression and anxiety to chronic insomnia and pain.
The Core Philosophy: Thoughts, Feelings, and Behaviors
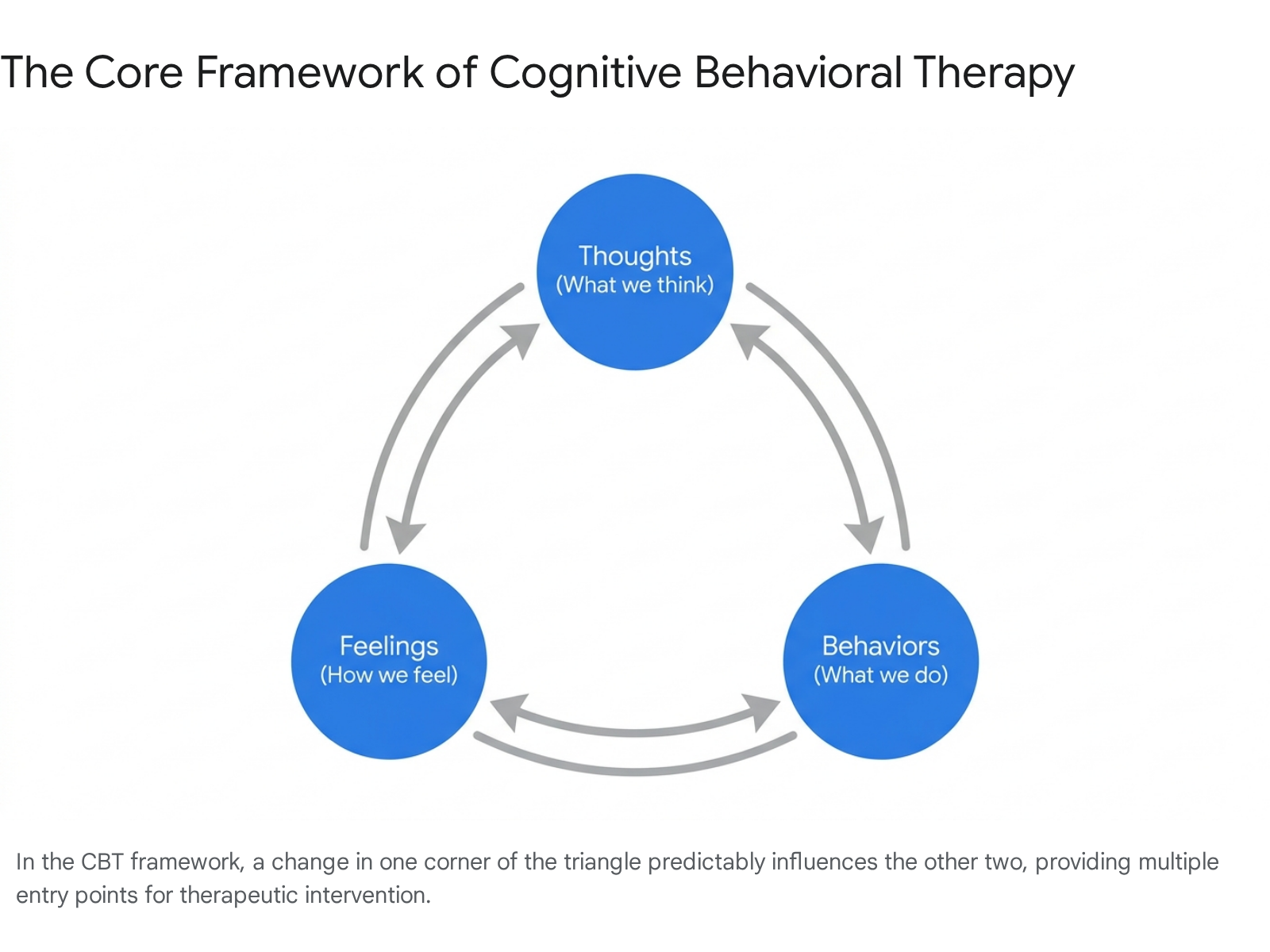
At its core, cognitive behavioral therapy is built on a deceptively simple premise: our thoughts, our feelings, and our behaviors are entirely interconnected 123.
Originating in the 1960s through the work of Dr. Aaron T. Beck, the therapy posits that psychological distress is not merely the result of a chemical imbalance or a traumatic past, but is actively maintained by how we process information in the present moment 45. In this framework, it is rarely a specific event itself that causes emotional turmoil; rather, it is the fundamental meaning we attach to that event 26.
To understand this, consider a scenario where you wave at a colleague across the street and they do not wave back. The objective event is entirely neutral. However, if your automatic thought is, "They are angry with me and are deliberately ignoring me," your resulting emotion will likely be anxiety or profound sadness. Your subsequent behavior might involve withdrawing from that colleague or avoiding them at the office. CBT works to intercept that automatic thought by asking you to evaluate the objective evidence. Perhaps the colleague simply did not have their glasses on, or was deeply distracted by a phone call 67. By restructuring the thought to be more realistic, the emotional distress dissipates, and the maladaptive behavior - in this case, social withdrawal - is prevented 68.
Unlike traditional psychoanalysis, which frequently attempts to unearth repressed childhood memories or subconscious drives over the course of years, CBT is firmly anchored in the "here and now" 29. While a skilled CBT therapist will certainly acknowledge how past events shaped your foundational worldview, the practical work of the therapy centers on identifying how those beliefs are malfunctioning in your present day-to-day life, and how to actively correct them using actionable skills 11011.
Schemas and Core Beliefs
To understand why people have such vastly different automatic reactions to the same events, CBT utilizes the concept of "schemas." Schemas are deep-seated core beliefs and personal rules for processing information, typically shaped by childhood influences and formative life experiences 9. A person who experienced early rejection might develop an unrelenting schema that dictates, "I am fundamentally unlovable."
These core beliefs act as an invisible lens through which all incoming information is filtered. If a person with a "failure schema" receives a performance review containing nine positive remarks and one piece of constructive criticism, their cognitive filter will discount the positive feedback entirely and magnify the single critique as absolute proof of their incompetence 612. CBT aims to gently bring these rigid, subconscious schemas to the surface so they can be examined and ultimately dismantled 2.
The Mechanics of Cognitive Restructuring
To achieve this paradigm shift, therapists utilize highly specific, structured tools. The most ubiquitous of these is the "thought record." A thought record is a cognitive-behavioral worksheet that patients use to document an activating event, their unfiltered automatic thoughts, the resulting emotions, and the cognitive distortions at play 61314.
Common cognitive distortions identified in these records include: * Catastrophizing: Automatically assuming the absolute worst-case scenario will materialize from a minor setback 25. * All-or-Nothing Thinking: Viewing situations in extreme black and white categories, where anything less than perfection is deemed a total failure 5. * Mind-Reading: Assuming you know exactly what others are thinking or feeling toward you, usually negatively, without any concrete evidence 615. * Over-generalization: Creating a sweeping universal rule from a single isolated negative experience 26.
Once these distortions are identified on the thought record, the patient is asked to act as a detective. They must put their own thoughts "on trial." They are required to gather objective evidence that supports the negative thought, and simultaneously compile evidence that contradicts it 1315. Through this rigorous exercise, patients learn to develop alternative, balanced perspectives that are grounded in reality rather than fear or assumption. Over time, this active cognitive restructuring literally rewires habitual thought patterns, allowing patients to regulate their own emotions and eventually become their own therapists 111.
Debunking Pervasive Myths About CBT
Despite being the most heavily researched psychotherapy in the world - recommended by the National Institute for Health and Care Excellence (NICE) in the UK and the American Psychiatric Association (APA) - CBT is frequently misunderstood by the general public 71213. These misconceptions often prevent people from seeking a highly effective treatment, as they assume the therapy is superficial or overly rigid.
The "Positive Thinking" Misconception
Many critics incorrectly assume CBT asks patients to put on rose-colored glasses, repeat self-affirmations, and ignore the harsh realities of life. This myth can be traced back to a conflation between CBT and mid-century self-help movements, such as Norman Vincent Peale's "The Power of Positive Thinking" 14. In reality, CBT does not advocate for relentless positive thinking; it advocates for realistic and accurate thinking 715.
Thinking purely positively has pitfalls equal to thinking purely negatively 7. If a patient makes a genuine mistake at work, CBT does not teach them to suppress their regret or tell themselves "I am perfect." Instead, it helps them challenge the catastrophic leap to "I am going to be fired and I am a total failure," replacing it with a balanced, evidence-based thought like, "I made a mistake on this project, but my overall track record is strong, and I can take immediate steps to rectify the error" 715. The goal is to see the glass not as half-full or half-empty, but to accurately measure the volume of water it currently holds.
The Role of the Past
Because CBT focuses heavily on present-day symptom relief, a common myth is that therapists coldly dismiss a patient's history. While a CBT therapist will not spend years exclusively analyzing childhood dynamics or interpreting dreams, they absolutely recognize that past experiences shape your current behaviors and thoughts 91021.
Exploring historical contexts provides critical insights for understanding mood disorders 10. Understanding how a past trauma created a present-day defense mechanism is an essential part of formulating a CBT treatment plan 211. The distinction is simply that CBT pivots quickly toward building coping strategies for the present, rather than dwelling indefinitely on the historical root cause. As one clinical analogy suggests, CBT is like being a good driver: you travel safely to your destination while regularly checking your rearview mirror, but you do not stare into it 21.
The Illusion of the Quick Fix
CBT is generally a short-term, time-limited therapy, usually lasting between 6 and 20 sessions depending on the complexity of the condition 39. Because of this brevity compared to open-ended talk therapy, some view it as a superficial band-aid that only offers a temporary reprieve. However, CBT is not a quick fix that requires passive participation. It is a highly active, demanding therapy that requires deep commitment and regular practice between sessions 1011. The skills learned are designed to provide permanent, long-term resilience against future stressors, making it a sustainable behavioral shift rather than a temporary emotional release 10.
The Anatomy of a CBT Session
If you sit down for a traditional psychoanalysis session, the hour might be unstructured, allowing your mind to wander wherever it chooses, guided only by free association. CBT is the exact opposite. It is highly structured, collaborative, and deliberately organized to maximize limited clinical time 91216. This structure ensures that both the therapist and the patient are aligned on the goals and that tangible progress is tracked week by week 1516.
Structured Efficiency and Agenda Setting
A standard 50-minute CBT session generally follows a predictable, evidence-based roadmap:
- Check-in and Homework Review (10-15 Minutes): The session begins with a brief review of the patient's current mood and an in-depth review of the "homework" assigned in the previous session. The therapist provides positive reinforcement, explores any challenges encountered, and helps integrate any insights gained during the week 1617.
- Collaborative Agenda Setting (5 Minutes): The therapist and patient collaboratively decide which specific, actionable problems they will tackle during that hour. This ensures the session remains entirely goal-oriented and prevents the conversation from drifting into unproductive venting 1216.
- Working the Agenda (20-30 Minutes): This is the core of the session. The therapist helps the patient examine the specific issues placed on the agenda. This might involve teaching a new emotional regulation skill, challenging a specific cognitive distortion using Socratic questioning, or preparing for a behavioral experiment 151617.
- Assigning New Homework (5-10 Minutes): The session transitions toward planning the work for the upcoming week. The therapist and patient collaboratively design a new homework assignment that directly relates to the skills practiced during the session 1617.
- Summary and Feedback (5 Minutes): The therapist summarizes the key takeaways and asks for the patient's explicit feedback on what was helpful, what was confusing, or if the therapist misunderstood anything. This fosters a strong, egalitarian therapeutic alliance 1617.
The Critical Role of Homework (The 168 Hours Concept)
In CBT, the therapy hour is merely a training ground; the actual healing and neurological rewiring happen in the real world. Therapists often remind patients that there are 168 hours in a week, and only one of those hours is spent in the clinic 12. Therefore, homework is non-negotiable and is considered the primary engine of therapeutic change.
Homework assignments are highly practical and tailored to the patient's specific presentation. For someone struggling with major depression, homework might involve "behavioral activation." Depression often strips away motivation, leading to severe inactivity, which in turn deepens the depression. A therapist might ask the patient to schedule specific, small activities - ranging from taking a shower to calling a friend - designed to generate a sense of mastery or pleasure, thereby systematically breaking the cycle of lethargy 5815.
For a patient with an anxiety disorder, homework might involve a "behavioral experiment." If a patient with social anxiety holds the catastrophic belief that "If I speak up in a meeting, everyone will think I am stupid," the therapist will assign them the task of intentionally asking a question in a low-stakes meeting. The patient then observes the actual outcome, directly testing their distorted belief against reality 516.
Who Does CBT Help Most? Target Conditions and Efficacy
CBT has been subjected to hundreds of randomized controlled trials (RCTs) and comprehensive meta-analyses, earning it the reputation as the benchmark for psychological intervention. While it is versatile, its efficacy shines most brightly in specific clinical domains.
Major and Subclinical Depression
CBT is incredibly effective for mood disorders. A massive 2024 systematic review and meta-analysis of 409 trials involving over 52,700 patients confirmed that CBT has moderate to large effects in reducing overall depression severity compared to usual care or waitlist control groups (Hedge's g = 0.79) 18.
Crucially, CBT is also highly effective in treating subclinical depression - intervening before mild depressive symptoms fully crystallize into a Major Depressive Disorder (MDD). A 2025 meta-analysis examining 5,877 participants found that CBT yielded a large significant improvement in subclinical depressive symptoms at post-assessment (g = -0.89) and maintained a moderate effect at long-term follow-up (g = -0.56) 19. Perhaps most importantly, CBT demonstrated profound preventive efficacy: individuals receiving CBT for subclinical symptoms significantly reduced their risk of transitioning to major depression 19. Demographic analyses within this data revealed that the intervention was particularly effective for adults aged 18 - 60 (g = -0.63) and in female-majority cohorts, with notably robust effect sizes observed in Asian populations (g = -1.13) compared to European cohorts 19.
Anxiety Disorders and Delivery Modalities
For anxiety disorders, particularly Social Anxiety Disorder (SAD) and Generalized Anxiety Disorder (GAD), CBT is widely considered a first-line treatment. Because anxiety is driven by avoidance behaviors and catastrophic predictions, CBT's emphasis on gradual exposure and cognitive reappraisal directly targets the root mechanisms of the pathology 15.
Recent data synthesized in 2024 evaluated how different delivery modalities impact the effectiveness of CBT for social anxiety. The analysis indicated that all forms of CBT are highly efficacious, but there are nuanced differences in effect sizes depending on how the therapy is administered.
| CBT Modality | Description | Effect Size (Hedge's g) | Clinical Context & Moderators |
|---|---|---|---|
| Individually-Administered (ICBT) | One-on-one sessions with a therapist 2021. | 0.95 (Large) | Strongest research base; widely recommended as a first-line approach. Older patient ages are associated with slightly smaller effect sizes 20. |
| Remotely-Delivered (RCBT) | Internet-delivered CBT, bibliotherapy, or app-based interventions 2021. | 0.90 (Large) | Highly effective, but guidance matters. Clinician-guided RCBT shows a significantly larger effect (g = 1.08) than purely self-guided platforms (g = 0.60) 20. |
| Group-Based (GCBT) | Therapy conducted in a group setting with peers facing similar challenges 2021. | 0.71 (Medium) | Slightly less clinically effective than individual formats, potentially due to reduced personalized therapist time or lower participant acceptability 20. |
Despite these statistical variations, the overall finding is that ICBT, GCBT, and RCBT do not differ significantly enough to rule any out; they can be delivered with equal confidence based on client preference and healthcare resources 20.
Chronic Insomnia (CBT-I)
One of the most striking triumphs of the cognitive-behavioral model is in the realm of sleep medicine. Cognitive Behavioral Therapy for Insomnia (CBT-I) has emerged as the definitive first-line treatment for chronic insomnia, vastly outperforming prescription sleep medications in the long term 2822.
While sleeping pills (such as benzodiazepines or "Z-drugs") may induce sleep faster in the short term, they are fraught with complications. They disrupt natural sleep architecture (often suppressing deep wave and REM sleep), carry high risks of physical dependency, and almost inevitably result in severe rebound insomnia the moment the medication is stopped 2822.
In stark contrast, meta-analyses reveal that CBT-I fundamentally changes what the brain has learned about sleep 28. By utilizing specific behavioral techniques - such as sleep restriction (limiting time in bed to consolidate sleep drive) and stimulus control (re-associating the bed solely with sleep rather than wakeful anxiety) - alongside cognitive restructuring regarding sleep anxiety, CBT-I produces highly durable results 2823. Patients treated with CBT-I continue to see improvements in their sleep quality and a reduction in sleep onset latency 6, 12, and even 24 months after the therapy concludes. The effects do not merely persist; they often deepen over time as the behavioral changes consolidate, making CBT-I significantly superior to pharmacotherapy for chronic, learned sleeplessness 28. This superiority extends to digitally delivered CBT-I (dCBT-I), which network meta-analyses show has the highest probability of being the most effective intervention compared to both face-to-face therapy and medication, offering a highly scalable solution for global sleep health 2324.
Chronic Pain Management
While psychological therapy cannot magically erase physiological tissue damage or cure structural spinal issues, CBT is heavily utilized to help patients manage chronic musculoskeletal conditions, such as lower back pain. Chronic pain frequently co-occurs with profound psychological distress; the relentless physical sensation causes depression and anxiety, which in turn amplifies the subjective neurological experience of the pain, creating a debilitating feedback loop 2526.
Recent systematic reviews and meta-analyses (2023 - 2026) clarify exactly what CBT does - and does not do - for chronic pain patients. The data shows that CBT may not drastically reduce the objective, physiological measurement of "pain intensity" compared to usual care 2526. However, it significantly reduces "pain catastrophizing" - the overwhelming psychological feeling that the pain is unbearable, endless, and will ruin one's life entirely 2527. Furthermore, CBT successfully improves functional disability, increases social participation, and significantly alleviates the comorbid depression and anxiety that accompany long-term pain conditions 25262728. By decoupling the physical sensation of pain from the emotional suffering attached to it, CBT allows chronic pain patients to reclaim their mobility and quality of life, even if the underlying physiological pain remains present. When combined with physical exercise, the multidisciplinary approach yields even stronger improvements in functional status 29.
Comparing CBT to Alternative Treatments
A frequent and critical question for patients entering the mental health system is whether to pursue CBT, psychiatric medication (such as SSRIs or SNRIs), or a more traditional, exploratory talk therapy like psychodynamic psychotherapy. The clinical data reveals that each modality has distinct strengths, mechanisms of action, and operational timelines.
CBT versus Antidepressant Medications
When comparing CBT to second-generation antidepressants for major depressive disorder, short-term remission and response rates are virtually identical. Neither treatment is inherently superior in the first few months of acute intervention 183730. However, a major divergence occurs when examining the durability of the treatment once it ends.
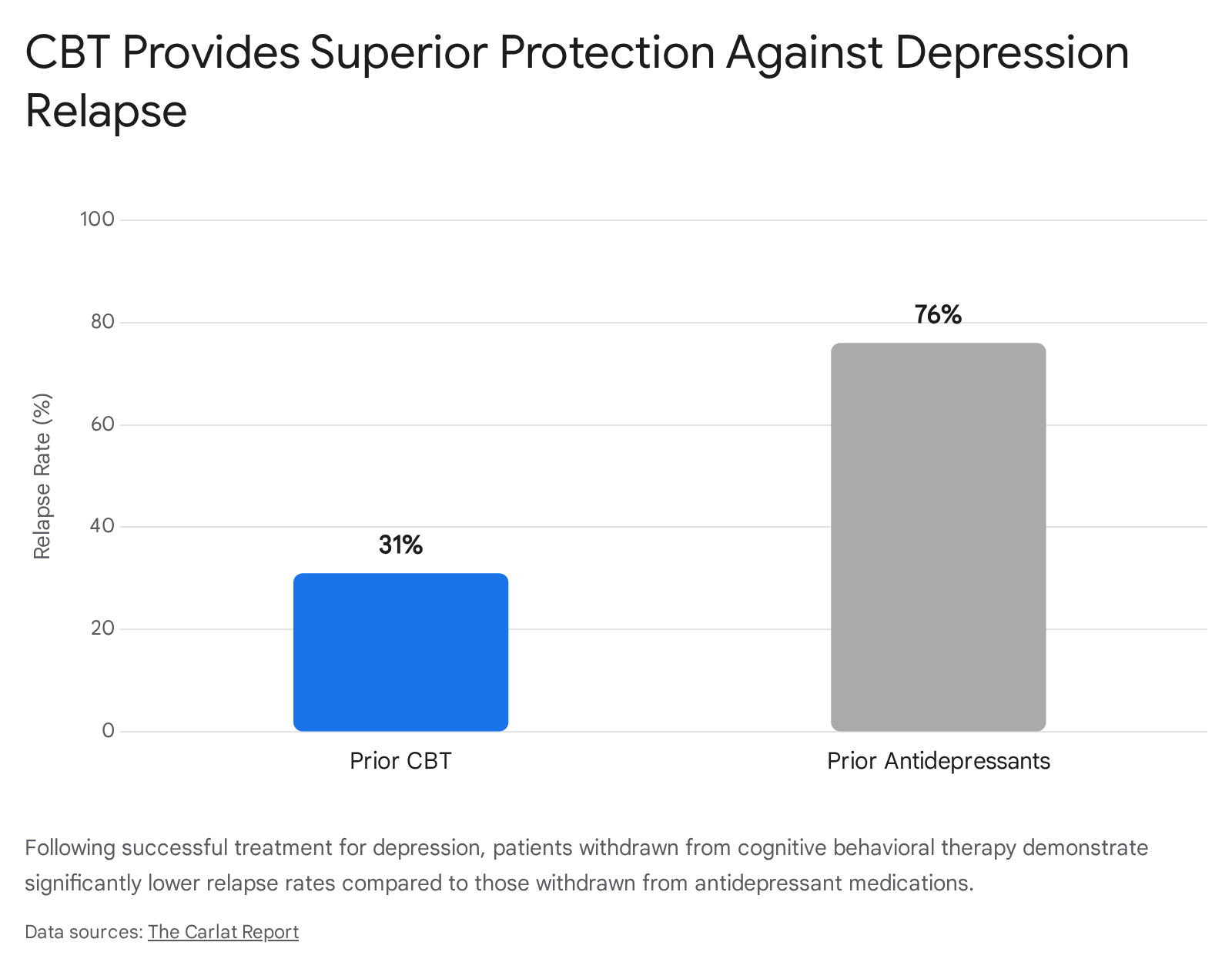
Because CBT fundamentally teaches patients to be their own therapists, the cognitive and behavioral skills remain active long after the clinical sessions conclude 130. Studies show that patients withdrawn from antidepressants relapse at significantly higher rates - often upwards of 76% over a subsequent year - compared to those who conclude a course of CBT, whose relapse rates hover around 31% 37.
In some trials, patients who merely received CBT in the past had lower relapse rates than patients currently maintained on continuous antidepressant treatment 37. The structural changes in thought patterns provide a lasting inoculation against future depressive episodes that chemical interventions alone cannot replicate.
CBT versus Psychodynamic Psychotherapy
When comparing CBT to psychodynamic therapy - which focuses less on present-day symptom management and more on uncovering unconscious patterns, resolving childhood conflicts, and utilizing the therapeutic relationship for deep personality restructuring - the literature becomes highly nuanced.
CBT is generally faster-acting for immediate symptom relief. By breaking the cycle of depressed mood and addressing the immediate negative feelings associated with the disorder, CBT provides rapid stabilization 31. However, long-term studies and meta-analyses suggest that the treatment effects of psychodynamic psychotherapy may actually continue to grow for years after the therapy concludes, particularly for patients with complex, severe personality disorders 40.
| Feature | Cognitive Behavioral Therapy (CBT) | Antidepressants (SSRIs/SNRIs) | Psychodynamic Therapy |
|---|---|---|---|
| Primary Mechanism | Restructuring present-day thoughts and behaviors. Building active coping skills 1931. | Altering neurochemical balances in the brain to elevate mood and reduce physiological anxiety 3032. | Changing deep cognitive structures by exploring unconscious patterns and relational dynamics 314033. |
| Treatment Duration | Short-term and time-limited (typically 6 to 20 structured sessions) 39. | Varies heavily; often long-term or open-ended maintenance 2234. | Often long-term and open-ended (months to years of exploration) 40. |
| Short-Term Efficacy | High. Highly effective for rapid, targeted symptom reduction 1831. | High. Effective for rapid symptom reduction, particularly somatic symptoms 3032. | Moderate to High. Often takes longer to establish deep structural changes and insight 31. |
| Post-Treatment Relapse Risk | Low. Patients retain cognitive coping skills, acting as their own long-term therapist 3730. | High. Symptoms frequently return once the medication is completely discontinued 3730. | Low. Effect sizes often continue to grow and stabilize long after therapy ends 40. |
| Target Conditions | Anxiety, mild-to-moderate depression, phobias, insomnia, eating disorders 1328. | Severe depression, generalized anxiety, chemical imbalances requiring stabilization 3732. | Complex trauma, deep-rooted relational issues, severe personality disorders 4033. |
Patient Predictors: Who is CBT Less Effective For?
While CBT is incredibly versatile, it is not a universally perfect fit for every mind. The success of the therapy relies heavily on the patient's individual traits, their clinical presentation, and their willingness to engage with the model.
Personality Traits and Motivation
Research evaluating personality traits reveals that patients who score highly in Conscientiousness and Agreeableness tend to benefit the most from CBT 35. This is highly logical given the rigid structure of the therapy: a conscientious patient is far more likely to diligently track their automatic thoughts, attend sessions punctually, and complete their weekly homework assignments 3536. A high degree of patient motivation and a willingness to engage in the uncomfortable process of challenging deep-seated personal beliefs is the strongest predictor of a positive clinical outcome 3747. If a patient is unwilling to complete out-of-session homework or refuses to adopt a collaborative approach with their therapist, the therapy will inevitably stall 3747.
Clinical Contraindications
Despite its widespread application, CBT has distinct limitations and may be contraindicated or highly ineffective for certain populations:
- Severe Cognitive Impairment: Because CBT requires active introspection, the ability to hold abstract concepts, and memory retention to bridge lessons from week to week, it is often ineffective for individuals with advanced dementia, severe intellectual disabilities, or significant traumatic brain injuries 3738.
- Acute Crisis or Severe Psychosis: For individuals experiencing active psychotic episodes (such as severe, untreated schizophrenia) or acute mania in bipolar disorder, reality testing is fundamentally impaired. The logical cognitive restructuring of CBT cannot override active psychosis; these patients generally require immediate pharmacological stabilization before any behavioral therapy can be attempted 3337.
- Complex Trauma and Severe Personality Disorders: While CBT can be adapted, standard, highly structured CBT is sometimes viewed as too directive or emotionally invalidating for individuals with complex, childhood trauma or Borderline Personality Disorder (BPD) 3347. These patients usually respond better to Dialectical Behavior Therapy (DBT) - a specialized offshoot of CBT that heavily emphasizes emotional validation and distress tolerance - or longer-term psychodynamic approaches that allow for deeper emotional exploration 4033.
The Global Reach: Culturally Adapted CBT (CaCBT)
Because Cognitive Behavioral Therapy was developed in the West (largely in the United States and the United Kingdom), its foundational principles are steeped in Western cultural values 1213. Standard CBT assumes a high degree of individualism, prioritizes personal autonomy, and favors direct, assertive communication 3940. When exported without modification, these concepts can clash drastically with the cultural, family, and religious values of non-Western populations.
Western Assumptions vs. Global Realities
In many collectivist cultures across Asia, Africa, or the Middle East, challenging the authority of elders, prioritizing personal goals over family obligations, or viewing the self as entirely independent is seen as maladaptive, not healthy 3940. If a Western-trained therapist attempts to use standard CBT to make a patient more "independent" from their family in these regions, the therapy will likely fail, cause profound distress, or result in the patient dropping out of treatment 3940. Furthermore, in cultures where distress is primarily somatized (experienced as physical pain) or attributed to spiritual causes (such as the "evil eye" or God's will), traditional CBT models that focus purely on internal cognitive errors can seem alienating and irrelevant 1340.
Frameworks for Adaptation
To bridge this massive gap, global mental health professionals have developed Culturally Adapted CBT (CaCBT). CaCBT maintains the vital theoretical underpinning of the cognitive model - that thoughts influence feelings and behaviors - while making necessary, culturally sensitive adjustments to the delivery, language, and conceptual framework of the therapy 134041. Using frameworks like the Southampton adaptation framework, therapists engage with local stakeholders to modify the therapy without losing its active ingredients 40.
Examples of effective, real-world cultural adaptation include: * Integrating Religion and Modesty: In the Middle East and North Africa (MENA), adapting the treatment of eating disorders (CBT-E) requires seamlessly integrating Islamic traditions. Therapists modify body-image exposure exercises to respect cultural modesty norms, and carefully manage the religious duty of Ramadan fasting to ensure it does not trigger restrictive or binge-eating cycles, perhaps by exploring Islamic exemptions or finding spiritually meaningful alternatives 39. * Reframing Idioms of Distress: In Uganda, therapists may avoid the Western clinical term "depression" entirely, as it carries no cultural resonance. Instead, they utilize local idioms related to "messages of love and respect" 41. Similarly, for Afghan refugees, specific rationales for meditation and guided imagery are explicitly interwoven with Islamic cultural concepts to increase familiarity and reduce stigma 42. * Broadening Family Involvement: In collectivist societies, the traditional boundary of individual therapy is often widened to include significant others, elders, or parents. The therapist utilizes the family unit to support the patient's cognitive restructuring, reflecting norms of interdependence rather than focusing solely on individual autonomy 3940.
Rigorous meta-analyses confirm that when this robust, respectful methodology is applied, Culturally Adapted CBT is highly effective. CaCBT has demonstrated significant global success in reducing anxiety, somatic symptoms, and emotional dysregulation across ethnoculturally diverse groups, proving that the cognitive model is universally applicable when delivered with profound cultural respect and localized understanding 4253.
Bottom line
Cognitive behavioral therapy is an evidence-based, highly structured treatment that empowers patients to actively alter the negative thoughts and behaviors fueling their emotional distress. While it requires significant active effort, homework, and motivation - and is not a universal cure-all for severe cognitive impairments or active psychosis - its practical approach makes it a premier treatment for depression, anxiety, chronic pain, and insomnia. Most importantly, by teaching patients to become their own therapists and challenging their core schemas, CBT provides durable, long-term protection against relapse that medication alone often cannot match.