Efficacy of Magnesium Supplement Forms and Deficiency Prevalence
Cellular Physiology and the Mechanisms of Magnesium Homeostasis
Magnesium is the fourth most abundant mineral in the human body and the second most abundant intracellular cation, surpassed only by potassium. It operates as an indispensable biological catalyst, serving as a fundamental cofactor for over 300 distinct enzymatic reactions 123. The physiological responsibilities of magnesium span virtually every fundamental cellular process, including the synthesis of carbohydrates, lipids, nucleic acids, and proteins 124. At the metabolic level, magnesium is a mandatory component in the regulation of cellular energy cycles. It directly binds to adenosine triphosphate (ATP) to form an Mg-ATP complex, which is required for both glycolysis and oxidative phosphorylation, thereby enabling energy storage and transfer 24.
Furthermore, magnesium plays an indispensable role in maintaining genomic stability by acting as a cofactor for DNA repair enzymes, and it is a structural component of DNA and RNA 34. Systemically, magnesium is essential for the active transport of calcium and potassium ions across cell membranes. This transport mechanism is critical for maintaining ionic gradients, facilitating nerve impulse conduction, ensuring proper muscle contraction, and sustaining normal cardiac rhythm 235. Magnesium also acts as a natural calcium antagonist, regulating vascular tone and preventing excessive intracellular calcium accumulation, which can lead to cellular death and pathological calcification 56.
Despite its critical importance to human biology, clinical assessment of magnesium status remains a significant diagnostic challenge. The adult human body contains approximately 25 grams of magnesium. The vast majority of this reserve is highly compartmentalized: 50% to 60% is stored in bone hydroxyapatite, and roughly 30% resides within the intracellular fluid of soft tissues, predominantly skeletal muscle 247. Less than 1% of the body's total magnesium is present in extracellular fluids, including blood serum 27.
Extracellular fluid concentrations are tightly regulated by homeostatic mechanisms managed primarily by the kidneys and, to a lesser extent, the gastrointestinal tract 278. The kidneys filter and excrete excess magnesium - typically about 120 milligrams (mg) per day in a healthy adult - but will aggressively reduce urinary excretion to conserve the mineral when dietary intake or systemic status is low 24. Because serum magnesium levels are maintained within a narrow physiological reference range - traditionally defined as 0.75 to 0.95 mmol/L (1.82 to 2.33 mg/dL) - through the continuous mobilization of bone and tissue stores, a standard blood test often masks severe intracellular depletion 249.
Clinical consensus increasingly recognizes that subclinical deficiency, often termed Chronic Latent Magnesium Deficiency (CLMD), can persist for years without triggering clinically defined hypomagnesemia (serum levels below 0.75 mmol/L) 910. Advances in non-invasive assessment techniques, such as phosphorus magnetic resonance spectroscopy (31P-MRS) utilized in the Baltimore Longitudinal Study of Aging, have demonstrated that intramuscular magnesium concentrations are significantly more reflective of true systemic status and muscle function than serum magnesium 11. These deeper tissue measurements reveal an inverse relationship with age, demonstrating that intracellular magnesium depletion correlates strongly with age-related functional decline, even when serum levels remain ostensibly within the normal range 111213. Recent epidemiological re-evaluations of data from the U.S. National Health and Nutrition Examination Survey (NHANES) suggest that the standard reference intervals for serum magnesium - originally derived from 1970s data - may be too low. When applying updated intervals based exclusively on metabolically healthy populations, researchers estimate that a substantial portion of the population suffers from CLMD 10.
Global Epidemiology of Magnesium Inadequacy
While severe clinical hypomagnesemia is relatively rare outside of hospital settings or specific pathological conditions, such as advanced chronic kidney disease or severe gastrointestinal malabsorption, inadequate dietary intake of magnesium has emerged as a pervasive global public health crisis 21415.
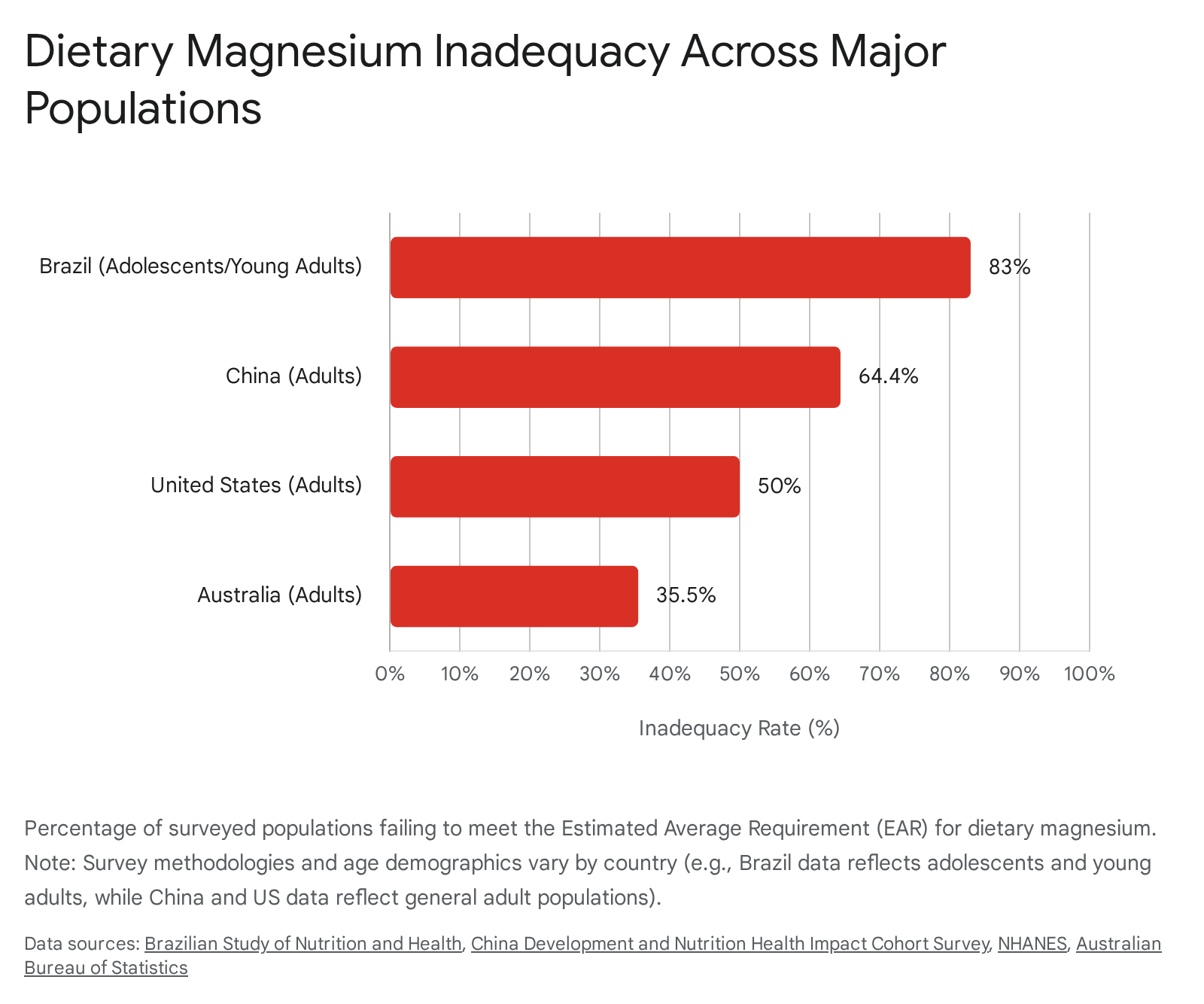
A landmark 2024 modeling analysis published in The Lancet Global Health provided unprecedented insight into global micronutrient deficiencies. The researchers evaluated data across 185 countries, estimating that approximately 2.4 billion people - roughly 31% of the global population - consume inadequate levels of dietary magnesium 14161718. The data revealed distinct demographic patterns. While many micronutrient deficiencies globally tend to disproportionately affect women (such as iron and iodine), the estimates for inadequate magnesium intake are consistently higher for men than for women within the same country and age groups 1718.
The roots of this global deficit are multifactorial, driven by sweeping changes in agriculture, food processing, and lifestyle. Modern intensive farming practices over the past century have led to significant soil mineral depletion. Consequently, crops grown in these depleted soils possess fundamentally lower magnesium concentrations than their historical equivalents 141920. This agricultural deficit is compounded by the global transition toward ultra-processed diets. The refinement of whole foods strips away the most magnesium-rich components. For example, the milling of whole wheat into white flour removes the bran and germ, resulting in a staggering loss of up to 85% of the grain's native magnesium content 19. Finally, lifestyle factors endemic to industrialized societies exert downward pressure on existing magnesium stores. High physiological and psychological stress, excessive caffeine intake, and diets high in refined sugars directly increase urinary magnesium excretion, thereby raising the body's baseline physiological requirement while simultaneously lowering intake 191922.
An examination of specific national health surveys across varied economies underscores the ubiquity and severity of the dietary deficit. The data reveals that geographical location and economic development offer little protection against inadequate magnesium intake.
| Nation | Population Assessed | Prevalence of Inadequate Intake | Key Findings and Demographic Nuances |
|---|---|---|---|
| Brazil | Adolescents and Young Adults (15 - 24.9 years) | >83% | Data from the Brazilian National Health Survey indicates extreme vulnerability in youth. A separate study of apparently healthy university students found 42% possessed subnormal magnesium status in plasma or erythrocytes, indicating subclinical depletion 920. |
| China | General Adults (15 provinces, 2022-2023) | 64.4% | The median daily intake in China has fallen dramatically from 283.7 mg in 1991 to under 239 mg in recent years, representing a stark nutritional decline strongly correlated with rapid industrialization 1624. |
| United States | General Adults | ~50% | NHANES data consistently demonstrates that half of the adult population fails to meet the Estimated Average Requirement. Applying modern, stricter reference intervals suggests up to 67.8% may experience Chronic Latent Magnesium Deficiency 101624. |
| Australia | General Population (>2 years old) | 35.5% (Average) | The National Nutrition and Physical Activity Survey revealed severe spikes in deficiency among adolescents, with 72% of females and 61% of males aged 14 to 18 failing to meet baseline dietary requirements 1925. |
Estimations of magnesium deficiency in the African continent present a unique methodological paradox that highlights the limitations of using raw food supply data without considering biological availability. Studies evaluating primary food supply data from the Food and Agriculture Organization (FAO) suggest that the risk of dietary magnesium deficiency is remarkably low - below 4% - due to the high theoretical magnesium content of staple crops like sorghum, maize, and wheat 21. However, clinical and regional realities severely contradict this theoretical abundance. The bioavailability of magnesium from these African staple crops is heavily compromised by the presence of phytic acid (phytates), which binds to divalent minerals in the gastrointestinal tract and creates insoluble complexes that the body cannot absorb 3821. Furthermore, national surveys in countries such as Nigeria demonstrate a high prevalence of broad micronutrient inadequacies and malnutrition driven by heavy reliance on mono-crop diets with low overall dietary diversity, rendering the theoretical abundance of crop-bound magnesium largely inaccessible 2223.
Clinical Implications of Chronic Depletion
The long-term physiological consequences of CLMD manifest across multiple organ systems. The insidious nature of the deficiency means that symptoms often emerge only after years of cellular depletion, presenting as chronic diseases rather than acute nutritional crises.
Cardiometabolic Pathologies
Epidemiological studies consistently link poor magnesium status to severe cardiovascular and metabolic disruptions. The Atherosclerosis Risk in Communities (ARIC) study, which followed almost 14,000 subjects over 27 years, provided striking evidence of sex-specific cardiovascular risks. Women in the lowest quintile of serum magnesium concentration exhibited a 53% higher risk of coronary heart disease compared to women in the highest quintile 13. Magnesium's role as a natural calcium channel blocker is critical for maintaining healthy vascular tone. Intracellular free magnesium concentrations are significantly lower in hypertensive individuals compared to normotensive controls, contributing to excessive vascular constriction and elevated blood pressure 5.
Metabolically, magnesium is intimately tied to glucose regulation and insulin sensitivity. Both low dietary intake and low serum magnesium levels are established risk factors for the development of type 2 diabetes mellitus 35. The relationship is cyclical and compounding: cellular magnesium deficiency impairs the insulin receptor's tyrosine kinase activity, exacerbating insulin resistance 524. In turn, the hyperglycemia and hyperinsulinemia characteristic of type 2 diabetes trigger excessive urinary magnesium excretion, further draining the body's reserves and accelerating the progression of metabolic syndrome 515.
Sarcopenia and Musculoskeletal Decline
Skeletal muscle represents the largest magnesium reservoir in the human body. As the aging process unfolds, progressive physiological and structural changes in muscles contribute to disability and frailty 413. Magnesium is critical for muscle ATP production, proper contraction mechanics, and anti-inflammatory defense. Clinical studies utilizing dual-energy X-ray absorptiometry and magnetic resonance spectroscopy have demonstrated that low serum and intramuscular magnesium concentrations are strongly associated with low muscle mass and strength 111225. In patients with type 2 diabetes, multivariate logistic regression analyses reveal that lower magnesium levels significantly increase the risk of developing low muscle mass, accelerating the onset of sarcopenia 12.
Furthermore, prolonged magnesium depletion threatens skeletal integrity. Because the body will prioritize serum magnesium homeostasis over bone density, chronic low intake forces the continuous extraction of magnesium from bone hydroxyapatite. This extraction alters the crystalline structure of the bone, making the hydroxyapatite crystals larger and more brittle 13. Consequently, magnesium deficiency is heavily implicated in the pathophysiology of osteoporosis, operating as a distinct risk factor independent of calcium or vitamin D status 51315.
Pharmacokinetics of Magnesium Supplementation
Because reversing systemic deficiency through dietary modification alone is increasingly difficult in industrialized environments, oral magnesium supplementation serves as a primary clinical intervention. However, the efficacy of supplementation depends entirely on the specific chemical form of magnesium administered. Magnesium is a highly reactive alkaline earth metal; it is never ingested in its pure elemental state. Instead, it is bound to a carrier molecule - either an anion to form an inorganic salt, or an organic ligand/amino acid to form a chelate. The chemical nature of this bond dictates the compound's overall mass, elemental yield, aqueous solubility, intestinal absorption kinetics, and ultimate tissue distribution 312633.
Fractional Absorption and Elemental Yield Dynamics
A fundamental clinical concept in magnesium supplementation is the inverse relationship between the physical weight of elemental magnesium in a compound and its overall biological availability. Inorganic forms (such as magnesium oxide) pack exceptionally dense amounts of elemental magnesium into small molecular structures but feature notoriously poor cellular absorption rates. Conversely, organic complexes and amino acid chelates (such as magnesium citrate, glycinate, and malate) contain much lower percentages of elemental magnesium by weight but offer significantly higher and more predictable absorption profiles 31263435.
The mechanism of intestinal magnesium absorption is primarily paracellular (passive diffusion between cells) across the small intestine, supplemented by a saturable, active transcellular pathway 827. When magnesium is ingested, fractional absorption falls progressively as the absolute dose increases. A seminal pharmacokinetic balance study demonstrated that while total net absorption increases with higher intake, the actual percentage of the dose absorbed drops dramatically - from roughly 65% at very low intakes down to just 11% at massive single doses 27. This curvilinear absorption relationship indicates that the intestinal transport mechanisms reach an absorptive maximum quickly 27. Therefore, clinical repletion protocols strongly favor administering several smaller doses of a highly bioavailable organic magnesium compound throughout the day, rather than a single massive dose of an inorganic salt 328.
Gastrointestinal Tolerability and Tolerable Upper Limits
The most ubiquitous and dose-limiting adverse effect of oral magnesium supplementation is osmotic diarrhea, frequently accompanied by abdominal cramping, distension, and nausea 238. This phenomenon occurs when poorly absorbed magnesium salts remain within the intestinal lumen. Because the magnesium ion is highly osmotically active, it draws surrounding water into the colon, overstimulating bowel motility and resulting in rapid gastric emptying 2930. Inorganic forms, notably magnesium oxide, sulfate, and hydroxide, are the primary pharmacological culprits behind these gastrointestinal symptoms 23529.
Due to the risk of significant osmotic diarrhea, international health and regulatory authorities established strict Tolerable Upper Intake Levels (ULs) exclusively for supplemental magnesium. These limits do not apply to dietary magnesium, as the kidneys seamlessly filter excess dietary intake 2831. Historically, the European Food Safety Authority (EFSA) established a conservative UL of 250 mg/day 332, while the U.S. Institute of Medicine (IOM) set a UL of 350 mg/day 2833.
However, recent extensive reviews of clinical data suggest these limits may unnecessarily restrict effective therapeutic dosing. In 2025, the Council for Responsible Nutrition (CRN) conducted an exhaustive review of intervention studies published between 1997 and 2022. The CRN analysis revealed that modern clinical trials administering doses up to 500 mg/day - and in certain protocols, up to 1,200 mg/day - did not consistently produce statistically significant increases in severe diarrhea compared to placebo groups, particularly when utilizing organic chelates or divided dosing schedules 383344. Consequently, the CRN updated its guidelines, raising the safe upper limit for healthy adults to 500 mg/day 3844. The updated consensus posits that transient stool softening associated with higher doses of bioavailable magnesium should be classified as an easily reversible nuisance effect rather than a serious toxicological adverse event, thereby validating higher dosing strategies necessary to combat the high global prevalence of CLMD 3844.
Comparative Efficacy of Specific Magnesium Forms
Clinical outcomes heavily depend on matching the correct magnesium ligand to the patient's specific pathology. Treating magnesium as a monolithic, interchangeable supplement often leads to treatment failure or unacceptable gastrointestinal distress.
Inorganic Salts: Oxide, Sulfate, and Chloride
Inorganic magnesium salts represent the oldest and most widely available class of supplements, typically utilized for their low cost and high elemental density rather than their therapeutic efficacy for systemic repletion.
| Inorganic Form | Elemental Yield | Absorption Profile | Primary Clinical Application |
|---|---|---|---|
| Magnesium Oxide | ~57% - 60% | Extremely poor (~4%). Relies heavily on high stomach acidity to convert to magnesium chloride before absorption. 3134 | Primarily used as an osmotic laxative or antacid. Frequent cause of diarrhea. Highly inefficient for treating systemic deficiency. 3529 |
| Magnesium Sulfate | ~10% | Poor oral absorption. Exerts a massive osmotic pull in the lower intestines. 3135 | Rarely utilized orally for nutritional support. Administered intravenously in clinical settings (eclampsia) or used topically/transdermally as Epsom salts. 535 |
| Magnesium Chloride | ~12% | Moderate absorption, superior to oxide. Less dependent on gastric acid. 3129 | Used in broad-spectrum repletion and topical applications. Demonstrates a moderate risk of gastrointestinal irritation. 2930 |
Organic Salts and Chelates: Systemic and Muscular Optimization
For general systemic repletion, cardiometabolic health, and musculoskeletal optimization, organic acids and amino acid chelates provide the superior balance of high biological availability and gastrointestinal comfort 3529.
Magnesium Citrate: Magnesium bound to citric acid is one of the most thoroughly studied organic forms. It exhibits excellent aqueous solubility, dissolving easily even in achlorhydric (low stomach acid) environments, resulting in bioavailability rates approaching 30% 3134. While it is highly effective at elevating serum and intracellular magnesium levels rapidly, the citric acid ligand still possesses mild osmotic properties. Consequently, higher doses of magnesium citrate can induce stool softening or mild diarrhea, making it a dual-purpose supplement for patients suffering from both mild magnesium deficiency and constipation 352934.
Magnesium Malate: Magnesium bound to malic acid exhibits a distinct pharmacokinetic profile characterized by prolonged serum elevation, generating the highest Area Under the Curve (AUC) in comparative absorption studies 3446. Malic acid is a critical intermediate metabolite in the Krebs cycle (citric acid cycle), directly facilitating cellular ATP generation 35. Because of this synergistic biochemical relationship, magnesium malate is frequently utilized in clinical protocols targeting chronic fatigue syndrome, sports recovery, and fibromyalgia, offering dual-action support for mitochondrial energy production and muscular relaxation 3546. It is exceptionally gentle on the digestive tract, carrying a very low risk of inducing osmotic diarrhea 343529.
Magnesium Glycinate (Bisglycinate): In this formulation, a single magnesium ion is bound to two molecules of the amino acid glycine. This chelate structure protects the magnesium ion as it passes through the acidic stomach environment 35. Furthermore, magnesium glycinate is absorbed highly efficiently via dipeptide transport pathways in the intestinal mucosa, effectively bypassing the competitive saturation limits of standard mineral ion channels used by inorganic salts 3435. Glycine independently functions as an inhibitory neurotransmitter in the central nervous system. Therefore, magnesium glycinate is widely considered the premier clinical choice for patients seeking relief from sleep architecture disruptions, generalized anxiety, and nocturnal muscle cramps 3447. Its extreme structural stability ensures that it reaches the lower intestine intact without dissociating and drawing in water, making it the safest oral option for individuals with irritable bowel syndrome (IBS) or extreme sensitivity to laxatives 3529.
Innovations in Intestinal Delivery: Microencapsulation
To circumvent the fundamental limitations of low bioavailability and gastrointestinal distress associated with high-yield inorganic magnesium, pharmaceutical engineering has developed novel delivery systems, most notably microencapsulation. Clinical cross-over studies evaluating micronized, microencapsulated magnesium oxide (such as the proprietary Magshape ingredient) demonstrate that encasing the raw mineral delays its immediate reaction with stomach acid, allowing for gradual, sustained release throughout the entire length of the lower digestive tract 4835.
In a robust 2024 trial published in Nutrients, participants receiving microencapsulated magnesium demonstrated a sustained, statistically significant increase in blood plasma magnesium levels at one, four, and six hours post-ingestion. Conversely, standard magnesium bisglycinate failed to significantly raise plasma levels within the same testing timeframe, and standard non-encapsulated magnesium oxide caused an immediate plasma spike followed by a rapid, unsustained drop 4835. Furthermore, the microencapsulated formulation drastically reduced patient reports of increased bowel motility and sensations of gastric heaviness. This technological advancement suggests that the physical modification of inexpensive inorganic magnesium can successfully replicate, and in terms of sustained plasma levels, potentially exceed the tolerability and pharmacokinetic profiles of expensive amino acid chelates 4835.
Magnesium L-Threonate: Targeted Neurological Engineering
A critical limitation of all standard magnesium supplements - including highly bioavailable forms like citrate and glycinate - is their inherent inability to significantly alter magnesium concentrations within the central nervous system (CNS). While standard forms effectively correct systemic, cardiovascular, and muscular deficiencies, the highly selective blood-brain barrier severely restricts the passive diffusion of the magnesium ion into the brain's extracellular fluid 5051.
Magnesium L-threonate (patented and marketed as Magtein) represents a pharmacological breakthrough developed by neuroscientists at the Massachusetts Institute of Technology (MIT) specifically designed to solve this blood-brain barrier transport problem 5052. In this unique compound, magnesium is bound to L-threonic acid, an endogenous sugar acid and natural metabolite of ascorbic acid (Vitamin C) normally found in human cerebrospinal fluid 223654. The threonate ligand acts as an active molecular chaperone. Because the brain possesses a massive and constant demand for glucose to fuel neural activity, threonate structurally mimics elements that effectively utilize glucose transporters (GLUT) to bypass standard mineral restrictions, ferrying the magnesium ion directly across the blood-brain barrier and into the central nervous system 5255.
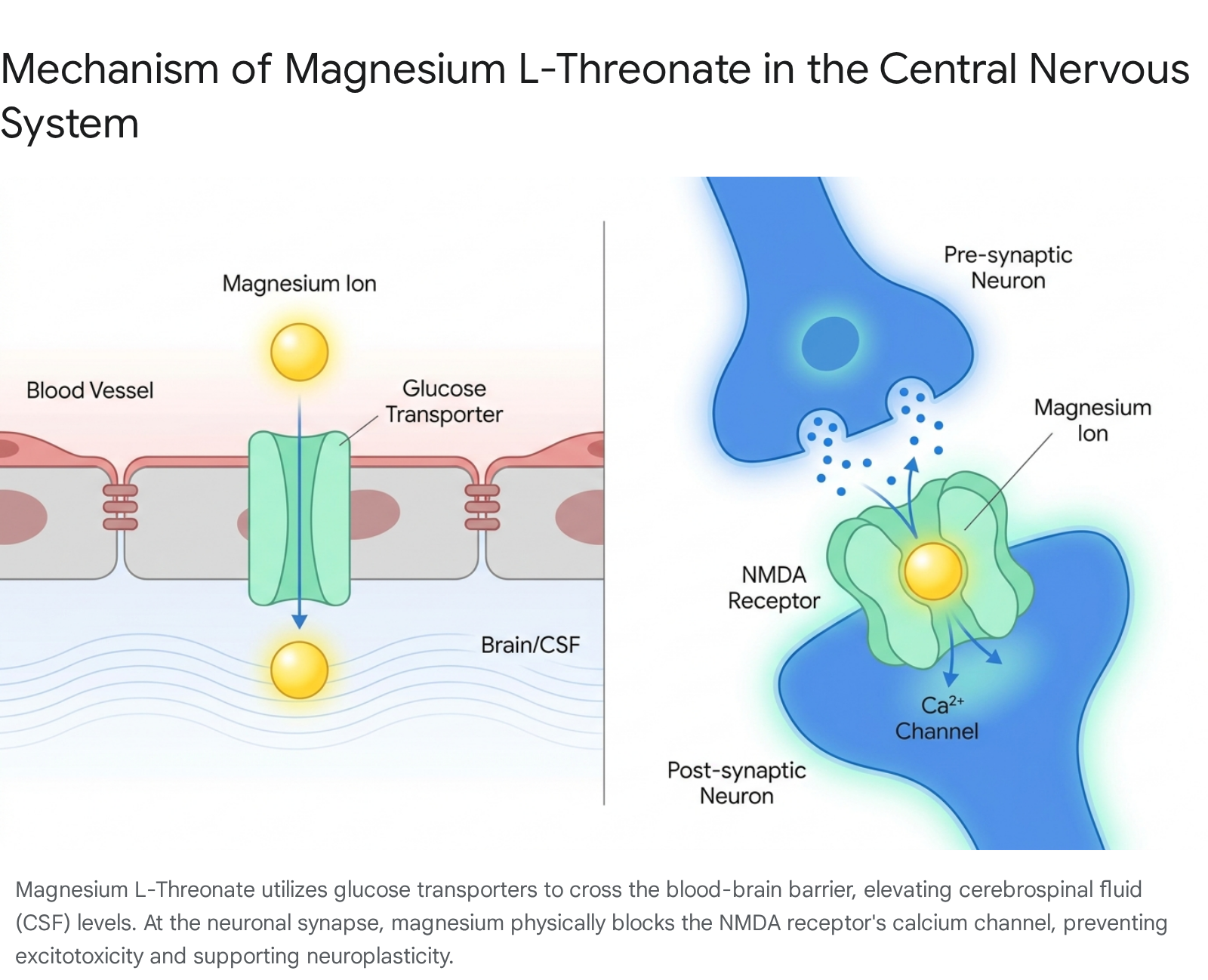
Preclinical animal models indicate that oral administration of magnesium L-threonate can increase cerebrospinal fluid (CSF) magnesium levels by an unprecedented 7% to 15% within a matter of weeks - a feat completely unachievable by oral administration of magnesium sulfate, oxide, or chloride 225237. Once successfully deposited in the brain, this influx of magnesium acts as a vital physiological regulator of N-methyl-D-aspartate (NMDA) receptors at the neuronal synapses. At resting membrane potentials, the magnesium ion sits within the NMDA receptor pore, physically blocking its calcium channel. This voltage-dependent block is crucial; it prevents the uncontrolled influx of calcium ions in response to low-level, background glutamate 3352. By preventing this excessive excitation, magnesium L-threonate directly mitigates excitotoxicity - a primary pathological mechanism underlying neural damage and neurodegeneration 3352. By elevating synaptic magnesium density, L-threonate simultaneously enhances neuroplasticity and heavily stimulates the localized release of Brain-Derived Neurotrophic Factor (BDNF), a neurotrophin foundational to new synapse formation, learning, and memory retention 55.
Rigorous clinical trials in human subjects continue to validate these preclinical neuro-mechanisms. A major 2026 randomized, double-blind, placebo-controlled trial involving 100 healthy adults (aged 18 to 45) suffering from sleep dissatisfaction evaluated the effects of 2,000 mg of magnesium L-threonate daily over six weeks. The researchers documented significant, quantifiable improvements in working memory, episodic memory, and overall executive function (the cognitive domain responsible for planning, adapting, and decision-making) 575859. Most strikingly, utilizing the NIH Toolbox Total Cognition Composite Score, the researchers calculated that six weeks of supplementation reversed functional measures of "cognitive age" by 7.5 years 575860. Additional physiological benefits recorded in the trial included a reduction in resting heart rate, an increase in heart rate variability (a vital marker of autonomic nervous system health and stress resilience), and distinct improvements in sleep architecture, specifically an increase in restorative deep sleep and REM phases at the expense of light sleep 36555859.
Despite these profound neurological capabilities, clinical prescribing of magnesium L-threonate must account for its inherent limitations regarding systemic mineral repletion. The molecular weight of the L-threonic acid ligand is substantial, resulting in a compound where elemental magnesium accounts for only 7.2% to 8.3% of the total mass 285438. Therefore, a standard therapeutic dose of 2,000 mg of magnesium L-threonate yields a mere ~144 mg of elemental magnesium 5438. Consequently, patients presenting with severe systemic, cardiovascular, or muscular magnesium deficiencies - who typically require 300 to 400 mg of elemental magnesium daily for proper repletion - cannot rely solely on L-threonate. Reaching target systemic levels using L-threonate alone would necessitate an impractically large, expensive, and potentially intolerable intake of the compound 2654. In such cases, combination therapy utilizing L-threonate for neurological support and a denser organic chelate (like glycinate) for somatic repletion is clinically optimal.
Pharmacological Interactions and Iatrogenic Depletion
As public awareness of CLMD grows and oral magnesium supplementation increases globally, clinicians and patients must meticulously manage significant, and potentially dangerous, drug-nutrient interactions. Because the magnesium ion is a highly reactive divalent cation (Mg2+), it possesses a strong propensity to form insoluble complexes (chelates) with various pharmaceutical compounds within the gastrointestinal tract. This binding severely inhibits the absorption and systemic efficacy of the targeted medication 6239. Conversely, certain classes of chronic medications aggressively deplete the body's internal magnesium stores, precipitating secondary, iatrogenic hypomagnesemia 4065.
Intestinal Chelation and Absorption Inhibition
The most critical and well-documented negative interactions involve broad-spectrum antibiotics and bone-resorption inhibitors. Concomitant oral administration of magnesium with these drugs must be strictly avoided or carefully temporally staggered.
- Fluoroquinolone and Tetracycline Antibiotics: When oral magnesium encounters antibiotics such as ciprofloxacin, levofloxacin, minocycline, or doxycycline in the gut lumen, the metal cation violently binds to the antibiotic molecule. This chemical reaction creates an inert, insoluble chelation complex that drastically reduces the drug's bioavailability - in some cases by up to 90% 624066. This neutralization can lead to catastrophic clinical treatment failure in the face of severe infectious diseases. Standard clinical guidelines mandate a strict temporal separation: these antibiotics must be taken at least 2 hours before, or 4 to 6 hours after, the ingestion of any oral magnesium supplement, magnesium-based antacid, or laxative 396566.
- Oral Bisphosphonates: Medications utilized as the primary defense against osteoporosis, such as alendronate (Fosamax) and risedronate (Actonel), are highly susceptible to mineral interference. These drugs already possess notoriously low baseline bioavailability (frequently <1% absorption rate even under ideal conditions). If exposed to magnesium (or calcium) in the stomach, absorption drops to zero, entirely neutralizing the bone-protective effects of the therapy 6266. Patients are universally instructed to take oral bisphosphonates first thing in the morning with plain water on an entirely empty stomach, and any magnesium supplementation must be strictly delayed for at least 2 hours following the bisphosphonate dose 623965. (It should be noted that this interaction is isolated to oral administration; intravenous bisphosphonates do not interact with dietary or oral magnesium 65).
- Thyroid Hormones: The absorption of synthetic thyroid hormone replacements, specifically levothyroxine, is similarly impaired by the presence of mineral cations. Organizations such as the UK's National Institute for Health and Care Excellence (NICE) and the British National Formulary (BNF) recommend spacing thyroid hormone replacement and magnesium supplements by a minimum of 4 hours to preserve endocrine stability 39.
- Anticonvulsants (Gabapentin): Frequently prescribed for the management of neuropathic pain and seizure disorders, gabapentin's serum levels can decrease by 20% to 40% when co-administered with magnesium 4065. This pharmacokinetic drop poses a substantial risk for compromising seizure control thresholds or allowing breakthrough nerve pain.
Medications Inducing Iatrogenic Depletion
Beyond direct physical interactions in the gut, long-term pharmacotherapy for common cardiovascular and gastrointestinal pathologies frequently induces chronic latent magnesium deficiency by either accelerating renal wasting or blocking standard intestinal absorption mechanisms.
- Proton Pump Inhibitors (PPIs): Prolonged use of acid-suppressing medications (e.g., omeprazole, pantoprazole, esomeprazole) drastically alters the native pH of the intestinal lumen. This chronic reduction in gastric acidity directly inhibits the active transport mechanisms required to pull magnesium across the intestinal wall 406566. Patients on chronic PPI therapy (extending beyond several months) require routine serum monitoring and often necessitate proactive supplementation. In these cases, highly bioavailable, acid-independent organic forms - such as magnesium citrate or glycinate - must be utilized, as forms like magnesium oxide are rendered entirely useless in low-acid environments 3940.
- Loop and Thiazide Diuretics: Medications such as furosemide and hydrochlorothiazide are designed to forcibly increase urinary volume and sodium excretion to manage fluid retention and hypertension. However, the renal mechanisms governing sodium and water excretion are intimately tied to magnesium handling; the drugs carry massive amounts of magnesium out of the body in the urine simultaneously 406541. Unmonitored, long-term diuretic use is a primary driver of iatrogenic hypomagnesemia. Paradoxically, because magnesium is required to maintain vascular relaxation and stable cardiac rhythms, diuretic-induced magnesium depletion can trigger the very arrhythmias and hypertensive spikes the drugs were originally prescribed to prevent 36641.
| Medication Class | Specific Drugs (Examples) | Interaction Mechanism | Clinical Protocol / Spacing Requirement |
|---|---|---|---|
| Fluoroquinolones | Ciprofloxacin, Levofloxacin | Mg binds to the drug in the GI tract, creating insoluble complexes and reducing absorption by up to 90%. | Space doses strictly: Administer antibiotic 2 hours before or 4-6 hours after Mg. 62406566 |
| Tetracyclines | Doxycycline, Minocycline | Chelation in the gut renders the antibiotic chemically inert. | Space doses: Administer antibiotic 2-3 hours before or 4-6 hours after Mg. 394066 |
| Bisphosphonates (Oral) | Alendronate, Risedronate | Mg completely halts the drug's already poor absorption, neutralizing bone-protective effects. | Administer drug on an empty stomach. Wait ≥ 2 hours before taking Mg. 624066 |
| Thyroid Hormones | Levothyroxine | Mg impairs drug absorption, leading to fluctuating hormone levels. | Separate administration by a minimum of 4 hours. 39 |
| Anticonvulsants | Gabapentin | Decreases drug serum levels by 20-40%. | Stagger doses and monitor clinically for loss of efficacy or breakthrough seizures. 4065 |
| Proton Pump Inhibitors | Omeprazole, Pantoprazole | Reduces GI acidity, blocking the active transport of Mg over long-term use. | Monitor Mg levels. Supplement strictly with highly bioavailable, acid-independent chelates. 406566 |
| Diuretics (Loop/Thiazide) | Furosemide, Hydrochlorothiazide | Induces rapid, massive renal wasting of systemic Mg alongside fluid. | Proactive Mg supplementation and regular electrolyte monitoring required to prevent arrhythmias. 406541 |
Conclusion
The global prevalence of inadequate magnesium intake represents a profound, yet systematically underdiagnosed, public health challenge. With approximately 31% of the global population - spanning both developing and highly industrialized nations - failing to meet baseline dietary requirements, the systemic implications for chronic disease progression are severe 161720. The historical reliance on serum blood testing, which inherently fails to capture severe intracellular depletion, has allowed Chronic Latent Magnesium Deficiency (CLMD) to persist unrecognized, driving the acceleration of cardiometabolic disorders, sarcopenia, osteoporosis, and cognitive decline 10111213.
Addressing this widespread deficit effectively requires a paradigm shift in clinical nutrition, moving away from viewing magnesium as a uniform, monolithic intervention toward a highly targeted, pharmacokinetic-based strategy. Standard inorganic salts, particularly magnesium oxide, continue to dominate commercial markets due to their high elemental density and low cost. However, their exceedingly poor bioavailability and dose-limiting gastrointestinal distress render them highly inefficient, and often counterproductive, for achieving systemic intracellular repletion 313529.
Conversely, organic and amino acid chelates, such as magnesium glycinate and malate, offer superior cellular uptake pathways and exceptional gastrointestinal tolerability, providing the necessary metabolic and muscular support required to combat chronic fatigue and sarcopenia 3546. For neurological pathologies, bioengineered compounds like magnesium L-threonate demonstrate a unique, transporter-mediated capacity to cross the blood-brain barrier. By elevating cerebrospinal fluid levels and regulating NMDA receptor activity, L-threonate provides quantifiable neuroprotective and cognitive benefits - including the reversal of functional cognitive aging - that are fundamentally unattainable with standard peripheral formulations 22515258.
Ultimately, successful magnesium therapy demands a comprehensive understanding of delivery mechanisms, dietary inhibitors, and the critical temporal spacing required to avoid severe, potentially life-threatening drug interactions. As international regulatory bodies update safety frameworks to reflect the benign toxicity profile of advanced organic chelates, proactive, personalized, and form-specific magnesium supplementation stands as an indispensable pillar of modern preventative medicine and chronic disease management.