Trends in ADHD overdiagnosis and underdiagnosis
The Core Diagnostic Debate
The epidemiological landscape of attention-deficit/hyperactivity disorder (ADHD) has undergone a profound transformation over the past three decades. What was once considered a relatively rare, childhood-onset behavioral disorder predominantly affecting school-aged males is now recognized as a complex, highly heritable neurodevelopmental condition that frequently persists across the entire human lifespan. As global prevalence rates and clinical diagnoses have surged - particularly among adults and specific demographic subgroups - a central and deeply contested research question has emerged: Is ADHD fundamentally overdiagnosed due to the pathologization of normal human variation, or is it systematically underdiagnosed due to historical clinical blind spots?
The empirical evidence from comprehensive global health data, psychiatric literature, and epidemiological cohort studies reveals a paradoxical reality: both phenomena are occurring simultaneously, driven by entirely different mechanisms within the healthcare ecosystem. There is robust, undeniable evidence of diagnostic inflation and overtreatment at the margins, heavily influenced by systemic educational pressures, the rapid commercialization of telehealth, and the algorithmic amplification of psychiatric symptoms on social media. Conversely, the concept of "clinical catch-up" explains the massive diagnostic surges seen in adult women and marginalized racial groups. For these populations, the rise in diagnosis represents the delayed recognition of deeply impairing executive dysfunction that traditional, male-centric diagnostic models historically failed to capture.
Key Opinion Leaders and Divergent Paradigms
The tension between overdiagnosis and underdiagnosis is best exemplified by the divergent philosophical and clinical paradigms of leading psychiatric authorities. The historical debate frequently centers on the threshold for pathology - specifically, where the line between neurotypical variation and clinical impairment should be drawn.
Dr. Allen Frances, a prominent psychiatrist who chaired the task force responsible for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), has become a leading critic of what he terms "diagnostic inflation" 113. Frances argues that incremental relaxations in the stringency of psychiatric definitions have inadvertently contributed to "false epidemics" of ADHD, autism, and childhood bipolar disorder 1. From this perspective, the broadening of diagnostic criteria combined with the subjective nature of symptom evaluation has cast the diagnostic net too wide 13. Critics aligned with this view assert that the DSM-5 criteria are overly ambiguous; all eighteen diagnostic criteria for ADHD utilize the descriptor "often" (e.g., "often easily distracted") without providing an objective, quantifiable baseline for what constitutes a pathological frequency 1. This ambiguity, Frances argues, allows normal developmental immaturity, environmental stress, and the standard rigors of human experience to be erroneously medicalized, creating a massive cohort of the "worried well" 32.
In stark contrast, Dr. Russell Barkley, a leading clinical psychologist and preeminent researcher in executive functioning, maintains that the expansion of ADHD diagnoses is a necessary correction to decades of restrictive and arbitrary clinical thresholds 34. Barkley fiercely contests the narrative that ADHD is a flexible social construct, pointing to overwhelming neurobiological and genetic evidence. Modern research supports Barkley's paradigm, demonstrating that ADHD is a highly heritable condition, with twin studies establishing a mean heritability of approximately 74% 58. Furthermore, genome-wide association studies (GWAS) have identified specific genomic regions associated with the disorder, and neuroimaging studies consistently reveal delayed cortical maturation and alterations in striatal dopamine transporter density among individuals with ADHD 386.
Barkley and aligned researchers argue that arbitrary diagnostic cut-offs historically denied crucial accommodations and pharmacological support to significantly impaired individuals 3. They highlight the severe real-world consequences of untreated ADHD, which include a reduction in life expectancy by 7 to 9 years, significantly higher rates of substance abuse, increased risks of vehicular accidents, profound academic and occupational failure, and pervasive interpersonal dysfunction 7812. From the neurobiological paradigm, failing to diagnose and treat ADHD constitutes a far greater public health hazard than the risk of localized overdiagnosis 39.
This ideological clash occasionally manifests in severe academic and institutional conflict. For example, in the mid-1990s, when researchers like Dr. Gretchen LeFever identified exceptionally high rates of ADHD drug treatment in southeastern Virginia (where 17% of white boys were being medicated), efforts to implement regional public health interventions were met with aggressive opposition 10. LeFever's work, which suggested a widespread failure to distinguish between true disorder and developmentally normal variation, was attacked by key opinion leaders tied to pharmaceutical interests, ultimately leading to the termination of the regional health coalition 10. This historical context underscores how deeply entrenched financial, academic, and philosophical interests complicate the objective measurement of ADHD prevalence.
Evolution of Diagnostic Criteria
A critical mechanism driving the change in ADHD prevalence is the evolution of the diagnostic criteria themselves. Successive iterations of the American Psychiatric Association's diagnostic manuals have demonstrably influenced the rate at which individuals qualify for a diagnosis. A systematic meta-analysis evaluating diagnostic stringency from 1980 to 2013 documented statistically significant inflation between the DSM-III and DSM-III-R editions, resulting in an 18% increase in ADHD diagnoses 11. Further, albeit non-statistically significant, inflation occurred between the DSM-III-R and DSM-IV (33%), and between the DSM-IV and DSM-5 (17%) 11.
The publication of the DSM-5 in 2013 introduced several key modifications explicitly designed to accommodate the lifespan trajectory of the disorder. Most notably, it raised the required age of onset for symptoms from before age 7 to before age 12, acknowledging that many individuals - particularly those with the predominantly inattentive presentation - do not face impairing environmental demands until later in their educational careers 15. Additionally, the DSM-5 lowered the symptom threshold for older adolescents and adults (aged 17 and older) from six to five symptoms in either the inattentive or hyperactive-impulsive domains 1116.
While the United States primarily utilizes the DSM-5, the World Health Organization's International Classification of Diseases (ICD) governs much of the diagnostic data in Europe and globally. The recent transition from the ICD-10 to the ICD-11 represents a significant harmonization with the DSM-5, fundamentally altering international prevalence comparisons.
| Diagnostic Framework Feature | DSM-5 Standard (APA) | ICD-11 Standard (WHO) | Epidemiological Impact |
|---|---|---|---|
| Symptom Threshold | Requires a fixed, strict count: 6 symptoms for children, 5 for adults in either domain 116. | Utilizes a more descriptive, evaluative model; less prescriptive about exact symptom cut-offs 1612. | The descriptive nature of the ICD-11 allows for milder presentations, aligning more closely with the broader DSM-5 net 1612. |
| Impairment Setting Requirements | Impairment must be strictly evident in two or more distinct settings (e.g., home and school) 16. | Refers to evidence of impairment in multiple settings without rigid, numerical constraints 16. | Strict DSM-5 setting rules can arbitrarily exclude highly masked adults who function well at work but suffer at home 1314. |
| Subtypes and Presentations | Uses fixed symptom thresholds to rigidly categorize into inattentive, hyperactive, or combined presentations 16. | Relies on clinical judgment to determine which descriptive subtype is present and diagnosable 16. | Convergence between DSM and ICD frameworks is currently driving historical European prevalence rates up to mirror US rates 1215. |
Under the older ICD-10 framework, "Hyperkinetic Disorder" required symptoms of both inattention and hyperactivity to be present simultaneously, and excluded the diagnosis if comorbid conditions like anxiety or depression were present 1215. This resulted in European prevalence rates appearing artificially low (often between 1% and 3%) compared to the United States 1521. The ICD-11's alignment with the broader DSM-5 definitions of ADHD - allowing for predominantly inattentive presentations and acknowledging psychiatric comorbidities - has triggered a statistical surge in diagnoses outside of North America 1612. This global alignment suggests that rising international rates are not an epidemic, but rather a standardization of how the medical community defines and measures executive dysfunction.
Empirical Evidence for Overdiagnosis
While key opinion leaders debate the theoretical boundaries of pathology, empirical population data isolates specific contexts where ADHD is undeniably overdiagnosed. This systemic overdiagnosis is rarely the result of malicious clinical intent; rather, it is the byproduct of structural educational environments, the unconstrained commercialization of telehealth, and the democratization of psychiatric information on social media.
The Relative Age Effect in Educational Settings
The most robust, statistically validated evidence for the systemic overdiagnosis of ADHD resides in the "relative age effect" (RAE). Educational systems universally group children into grade cohorts based on an arbitrary annual cut-off date. Consequently, within any given classroom, there is up to a 12-month age difference between the oldest and youngest students 161718. At ages five to seven, a 12-month developmental gap represents a massive variance in neurological maturity, impulse control, and sustained attention.
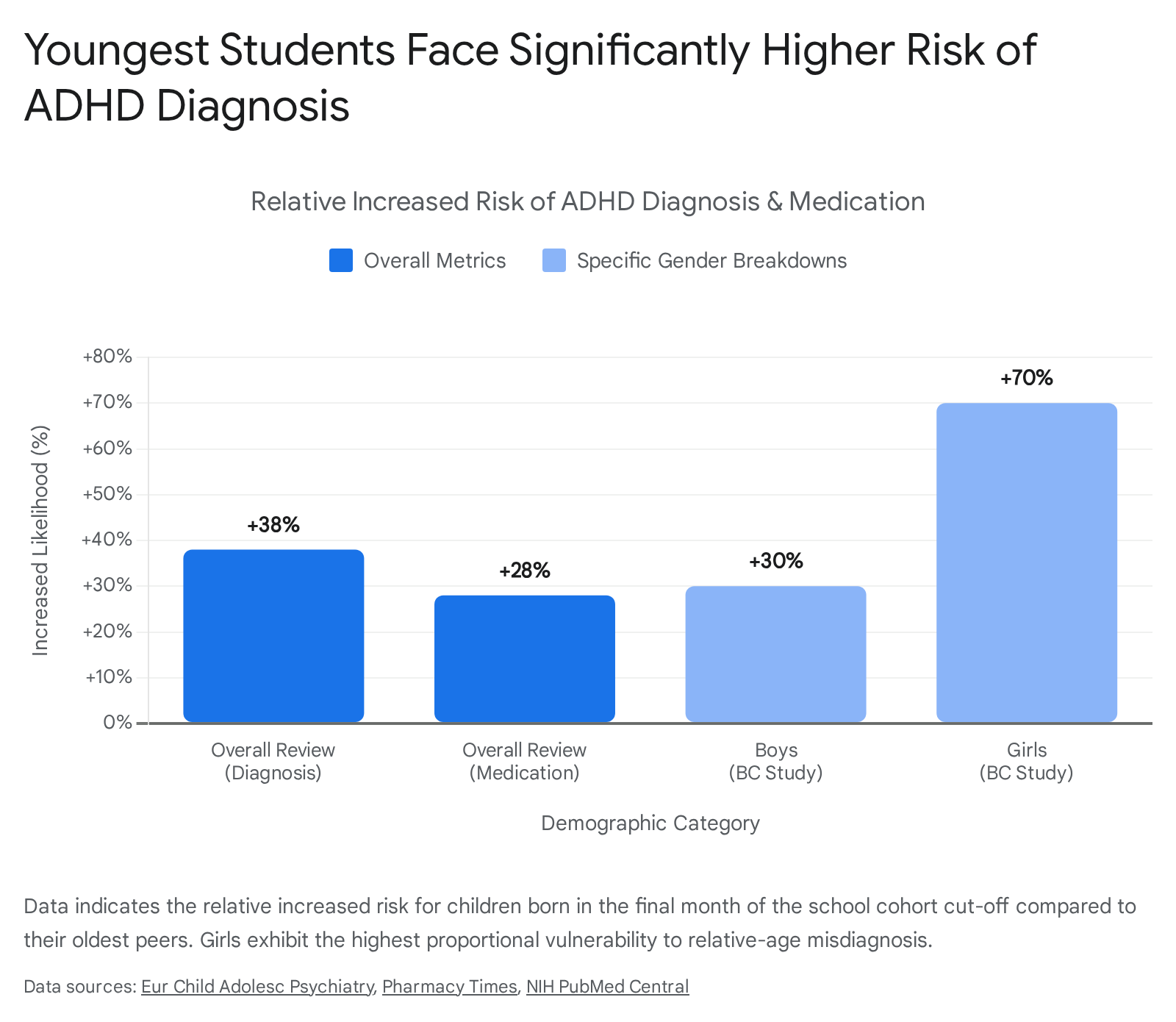
Research consistently demonstrates that adults - specifically teachers evaluating classroom behavior - frequently fail to account for chronological age, instead benchmarking the youngest students against their older, more mature peers 1719. This results in adults misattributing the standard signs of relative immaturity as clinical symptoms of ADHD 1719. A comprehensive 2024 systematic review and meta-analysis of 32 studies confirmed this phenomenon on a global scale. The analysis revealed that the youngest children in a school cohort are approximately 38% more likely to receive an ADHD diagnosis (relative risk of 1.38) and 28% more likely to be prescribed stimulant medications than the oldest children in the exact same grade 1619.
Extensive cohort studies map exactly when this diagnostic divergence occurs. A nationwide study analyzing data from 355,421 children born in Finland found that prior to school entry (ages 5 to 6), the probability of an ADHD diagnosis remained below 0.5% for all children, and crucially, there was absolutely no relative age effect 1820. In fact, children born toward the end of the year were slightly less likely to receive a diagnosis before school age 20. However, immediately following school entry, the RAE emerged abruptly. At age 7 for boys and age 8 for girls, the probability of diagnosis spiked dramatically for the youngest cohort members 20.
Further supporting this, a massive cohort study in British Columbia analyzing nearly one million children aged 6 to 12 found that boys born in December (the cut-off month) were 30% more likely to receive an ADHD diagnosis than boys born in January 21. For girls, the disparity was even more severe; December-born girls were 70% more likely to be diagnosed than their January-born counterparts 21. Similarly, the youngest boys were 41% more likely, and the youngest girls 77% more likely, to be given a prescription for ADHD medications such as methylphenidate or dextroamphetamine 21. Importantly, studies analyzing diagnostic informants reveal that teacher ratings of ADHD symptoms show a massive relative age effect, whereas parent ratings do not, indicating that the educational environment and peer-comparative benchmarking are the primary engines of this specific overdiagnosis 162223. The relative age effect provides undeniable proof that systemic grade-level assessments are artificially converting chronological immaturity into pathological diagnoses.
Social Media Influence and Prevalence Inflation
A modern and rapidly escalating driver of potential overdiagnosis is the proliferation of mental health content on short-form social media platforms. The concept of "prevalence inflation" describes a sociological phenomenon wherein individuals - immersed in an environment saturated with psychiatric terminology - begin to process normal psychological fluctuations, everyday stress, and temporary cognitive lapses as perilous signs of intrinsic pathology 2.
The platform TikTok, in particular, has become a massive vector for this phenomenon. As of late 2022, videos utilizing the hashtag #ADHD had amassed over 11.4 billion views, making it one of the most popular health-related topics on the network 2425. While social media can reduce stigma, foster community, and improve baseline health literacy, the algorithmic incentivization of highly relatable, short-form content fundamentally distorts complex medical concepts 2526.
Academic analyses of ADHD content on TikTok reveal alarming rates of misinformation. A 2025 study in the journal PLOS One tasked clinical psychologists with evaluating the top 100 most-viewed #ADHD videos, which collectively held nearly half a billion views 2426. The clinicians determined that 51.3% of the medical claims made in these videos were entirely inaccurate and failed to align with the DSM-5 2426. More concerningly, 68.5% of the inaccurate claims actively pathologized the "normal human experience" 2426. Content creators frequently present ubiquitous, transdiagnostic traits - such as occasional forgetfulness, temporary task avoidance, general fatigue, or normal mind-wandering - as definitive, isolated proof of a neurodevelopmental disorder 262734.
The psychological impact of this consumption on young adults is highly measurable. A study of 843 undergraduate students found that as participants spent more time consuming ADHD-related TikTok content, they became increasingly likely to overestimate both the severity of their own symptoms and the general prevalence of ADHD in the wider population 2426. A related Harvard master's thesis evaluating young adults undergoing neuropsychological testing found a significant positive correlation between time spent on TikTok and current self-reported hyperactivity symptoms 2528. Individuals spending more than an hour daily on the platform were significantly more likely to report that TikTok directly influenced their decision to seek a professional diagnosis 28.
This dynamic creates a feedback loop that directly impacts clinical practice. Patients increasingly arrive at psychiatric evaluations with rigidly preconceived self-diagnoses anchored in oversimplified social media narratives 252734. When patients view occasional lapses in concentration as pathology, they demand clinical intervention, placing immense pressure on diagnosticians and inflating the ranks of the "worried well" entering the mental health system 22429.
Telehealth Expansion and Commercialized Prescribing
The structural risk of overdiagnosis introduced by social media was severely compounded by the COVID-19 pandemic, which radically altered the regulatory environment governing psychiatric care. In March 2020, to ensure continuity of care during global lockdowns, the U.S. Drug Enforcement Administration (DEA) and the Department of Health and Human Services temporarily lifted the in-person medical evaluation requirement mandated by the Ryan Haight Online Pharmacy Consumer Protection Act 373031. This waiver allowed practitioners to prescribe Schedule II controlled substances - including highly regulated ADHD stimulants like Adderall and Vyvanse - entirely via telehealth platforms 3730.
This regulatory easing catalyzed the explosive growth of venture-backed, direct-to-consumer mental health startups utilizing subscription models, such as Cerebral and Done 37. Survey data indicates that in the post-2020 landscape, 57% of adults seeking ADHD care utilized telehealth services 37. While telehealth undeniably improved access for rural and underserved populations 32, the commercial imperatives of these platforms led to highly questionable diagnostic practices.
Reports indicate that some platforms utilized evaluations lasting merely 30 minutes, frequently conducted by nurse practitioners rather than specialized psychiatrists, before immediately issuing stimulant prescriptions 3731. In one user survey, 97% of patients diagnosed with ADHD on a specific platform reported receiving a new prescription within a week 37. The prioritization of patient acquisition and subscription retention over rigorous differential diagnosis led to severe legal and regulatory consequences.
In late 2024, the embattled telehealth provider Cerebral signed a non-prosecution agreement with the U.S. Department of Justice, agreeing to pay a $3.6 million fine for business practices that actively encouraged the unauthorized distribution of controlled substances 33. Federal prosecutors revealed that between 2021 and 2022, Cerebral implemented internal metrics specifically designed to drive prescription volume. The company tracked an "Initial Visit Rx Rate" and sought to increase it to 95%, explicitly implementing bonus structures to financially incentivize practitioners who prescribed stimulants to newly enrolled patients 33. Furthermore, the company tracked an "ADHD Stimulant Rx Metric" and instituted internal plans to push this metric to 100%, going so far as to audit providers and threaten disciplinary measures against those who did not prescribe stimulants at high enough rates 33.
This commercialization of diagnosis represents a profound systemic failure. When corporate entities financially incentivize the diagnosis of a psychiatric condition to drive the sale of controlled substances, it artificially and aggressively inflates prevalence data. The telehealth boom proves that a measurable portion of the recent surge in adult ADHD diagnoses was driven not by biological reality, but by profit-driven overtreatment.
Evidence for Underdiagnosis and Masking
While overdiagnosis occurs visibly at the commercial and educational margins, it obscures a parallel, statistically larger crisis: the chronic, historic underdiagnosis of millions of individuals. For nearly a century, the clinical definition of ADHD was anchored entirely to externalizing, hyperactive, and disruptive behaviors predominantly observed in white, school-aged boys 34354436. Because these boys disrupted classrooms and family dynamics, they were rapidly funneled into clinical evaluation 37. Consequently, diagnostic criteria, assessment scales, and pharmacological trials were built almost entirely around male behavioral baselines 3637. This narrow clinical lens created a massive backlog of underdiagnosed populations - primarily adult women, older adults, and marginalized ethnic minorities - whose symptoms manifest as internalizing distress rather than external disruption.
The Female Presentation and Compensatory Strategies
The underdiagnosis of women and girls is one of the most critical blind spots in modern psychiatry. In childhood, boys are diagnosed at a ratio of approximately 2:1 or even 3:1 compared to girls 383940. However, this ratio steadily narrows into adulthood. Between 2007 and 2016, adult ADHD diagnoses in women surged by an astonishing 344%, compared to a 264% increase for men 41. This spike does not represent a sudden outbreak of female ADHD; rather, it represents a generational "clinical catch-up" as adult women finally seek treatment for lifelong, unacknowledged neurodevelopmental impairment 4151.
The primary reason girls evade early diagnosis is that their symptom presentation frequently diverges from the traditional hyperactive model. Women and girls are significantly more likely to present with the predominantly inattentive subtype of ADHD 1337. Rather than physically acting out, inattentive girls exhibit internal restlessness, daydreaming, mental fatigue, and severe disorganization 37. Because these traits do not disrupt the classroom environment, teachers rarely flag these children for evaluation, leaving them to struggle silently 37.
Furthermore, girls face immense societal pressure to conform to gender norms that expect them to be organized, nurturing, and emotionally stable 52. To survive in neurotypical environments, women with ADHD frequently develop highly sophisticated "masking" or compensatory strategies 525342. Masking involves the conscious or unconscious suppression of ADHD symptoms through the expenditure of massive amounts of cognitive energy 1442.
| Strategy Type | Description of Compensatory Behavior | Clinical Consequence of Masking |
|---|---|---|
| Organizational Overcompensation | Developing elaborate, obsessive-like systems, excessive note-taking, and rigid external support structures to counteract working memory deficits 5253. | Clinicians observe the rigid systems and misdiagnose the underlying executive dysfunction as Generalized Anxiety Disorder or Obsessive-Compulsive tendencies 53. |
| Social Adaptation | Suppressing physical restlessness; constantly monitoring and mirroring neurotypical behaviors to avoid social rejection 1452. | Women present a "polished exterior" during clinical interviews, leading practitioners to dismiss their internal distress and delay diagnostic consideration 1453. |
| Energy Budgeting | Expending intense cognitive effort to maintain focus and professionalism at work, resulting in total executive collapse and emotional exhaustion at home 1452. | Leads to severe chronic burnout, identity confusion, and a five-fold increased risk for postpartum depression and severe emotional dysregulation 1443. |
While these masking strategies allow women to function temporarily, they extract a devastating psychological toll. The constant effort required to maintain the mask frequently leads to emotional exhaustion, chronic burnout, and severe emotional dysregulation 1444. Consequently, when women finally seek psychiatric help, clinicians often focus entirely on the secondary consequences of the masking - diagnosing them with anxiety, major depression, or borderline personality disorder - while remaining completely blind to the underlying ADHD driving the distress 36375343.
Additionally, the female experience of ADHD is profoundly impacted by the endocrine system. The efficacy of neurotransmitters like dopamine is heavily modulated by female sex hormones 845. Fluctuating estrogen and progesterone levels across the menstrual cycle, pregnancy, and perimenopause drastically influence the severity of inattention, impulsivity, and emotional dysregulation 81443. Compensatory strategies that work perfectly during a high-estrogen phase may collapse entirely during a low-estrogen phase, creating a chaotic clinical picture that standard diagnostic tools - which do not track hormonal cycles - fail to accurately capture 1445.
Adult ADHD and the Persistence of Symptoms
For decades, the medical consensus erroneously held that ADHD was strictly a pediatric condition that children simply "outgrew" upon reaching puberty 79. Modern longitudinal data has entirely dismantled this myth, demonstrating that impairing symptoms persist into adulthood in approximately 60% to 86% of childhood cases 73841. Despite this, the legacy of the pediatric model persists; it is currently estimated that up to 85% of adults living with ADHD globally remain undiagnosed and untreated 38.
Diagnosing adults presents highly specific challenges. The DSM criteria were originally calibrated using field trials of school children aged 8 to 12, focusing on overt behaviors like "runs about or climbs in situations where it is inappropriate" 4446. These criteria fail to capture the adult experience of the disorder, where hyperactivity frequently internalizes into a persistent feeling of inner restlessness, chronic procrastination, and severe executive dysfunction in occupational settings 744.
Furthermore, diagnosing adults requires them to accurately self-report their current internal experiences while simultaneously recalling childhood behaviors that occurred decades earlier, a task inherently difficult for individuals with working memory deficits 44. The lack of objective, gold-standard diagnostic guidelines for adults forces clinicians to rely heavily on subjective rating scales, which are vulnerable to bias, masking, and poor patient recall 36. A 2026 review of 292 randomized controlled trials for adult ADHD highlighted a concerning lack of diagnostic rigor in the field, finding that nearly 50% of the trials diagnosed adult ADHD without conducting a formal assessment of broader psychopathology to rule out mimicking conditions like trauma, depression, or attachment disorders 44.
The cost of leaving adults undiagnosed is staggering. In the United States, the total societal excess cost attributed to adult ADHD is estimated to be $122.8 billion per year 4147. This economic burden is primarily driven by $66.8 billion in increased unemployment, $28.8 billion in lost workplace productivity, and $14.3 billion in additional healthcare services 47. Adults with untreated ADHD experience higher job turnover, lower educational attainment, and earn, on average, $13,000 to $19,000 less annually than their neurotypical peers 738.
Racial and Ethnic Disparities in Diagnosis
Marginalized racial and ethnic groups have historically faced profound, systemic underdiagnosis and undertreatment within the psychiatric system. Longitudinal studies have repeatedly shown that despite exhibiting ADHD symptoms at rates equal to or higher than white populations, Black, Hispanic, and Asian children are frequently left out of the diagnostic pipeline 3548. A landmark 2013 population study revealed that by the eighth grade, African American children were 69% less likely, and Latino children 50% less likely, to receive an ADHD diagnosis compared to their white counterparts 35. A follow-up study tracking children before kindergarten entry found the disparity started almost immediately, with African American children 70% less likely to be diagnosed at an early age 35.
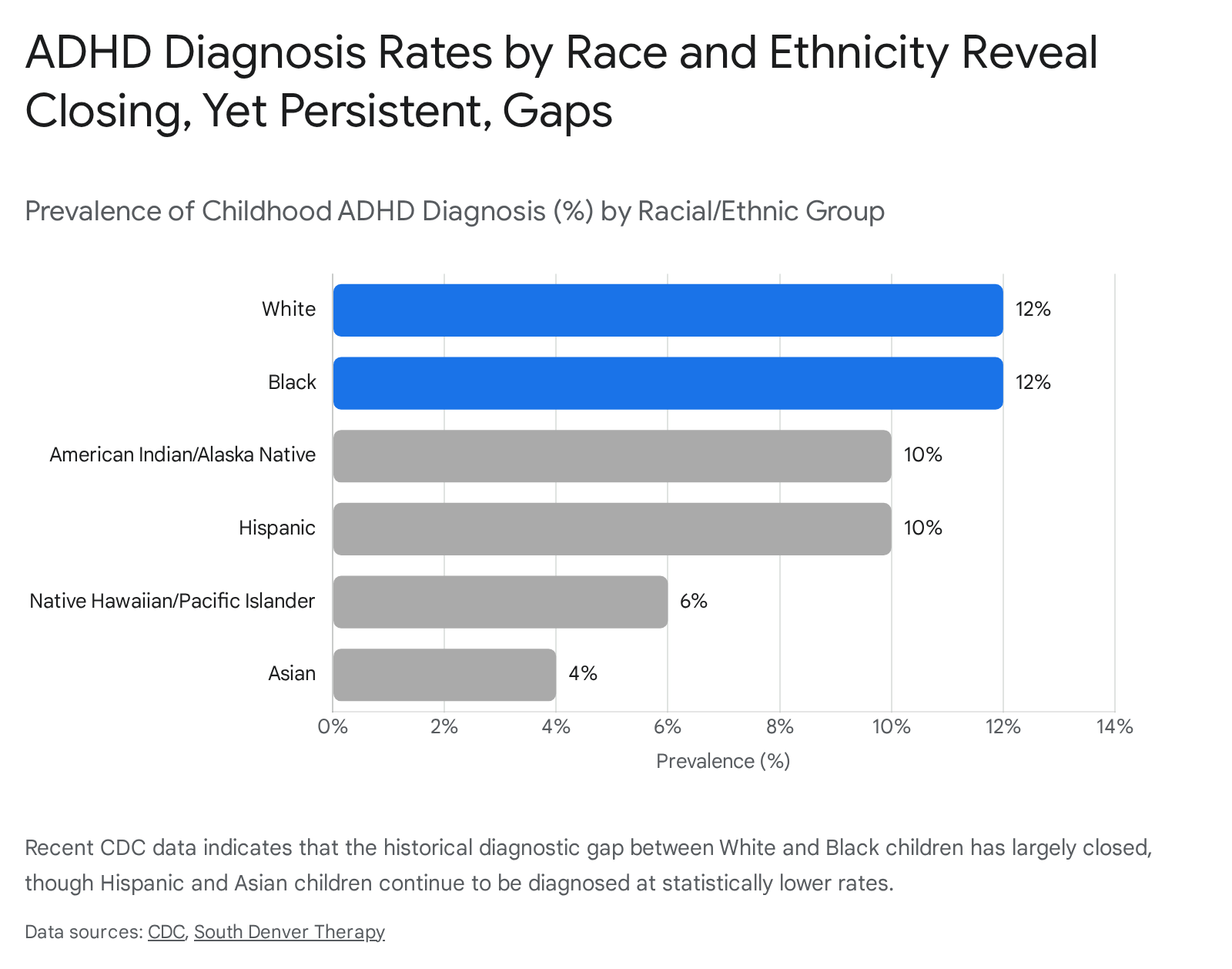
Recent data indicates that raw diagnostic rates are finally beginning to equalize, representing a positive clinical catch-up. Data from the Centers for Disease Control and Prevention (CDC) utilizing 2022 parent surveys indicates that the gap between Black and White children has effectively closed, with both non-Hispanic groups now reporting a lifetime diagnosis rate of approximately 12% 495063. However, significant diagnostic disparities persist for other groups; Hispanic children are diagnosed at a rate of 10%, Native Hawaiian/Pacific Islander children at 6%, and Asian children at merely 4% 4963.
While the raw diagnostic gap is closing, devastating disparities in treatment persist. The CDC and psychiatric researchers note that even when properly diagnosed, children of color are substantially less likely to receive pharmacological intervention, behavioral therapy, or high-quality continued care 354850. Historical data shows that while 65% of diagnosed White children received medication, only 36% of Black children and 30% of Latino children received similar pharmacological support 35.
These disparities are not the result of biological differences in disease prevalence, but rather complex, systemic socioeconomic and cultural barriers. Implicit bias within a predominantly white psychiatric workforce frequently leads clinicians and educators to misinterpret the exact same ADHD symptoms differently based on race 51. While disruptive behavior in a white child is often viewed through a medical lens, the exact same behavior in a Black or Hispanic child is frequently interpreted as defiance, insubordination, or a disciplinary issue, funneling the child toward punitive school suspension rather than clinical intervention 5051. Furthermore, cultural mistrust of the medical establishment, lingering stigmas regarding mental health in minority communities, lack of adequate health insurance, and linguistic barriers consistently depress treatment engagement across non-white populations 5152.
Epidemiological Data and Global Prevalence Trends
To definitively answer the overdiagnosis versus underdiagnosis question, it is essential to contextualize the absolute prevalence rates both nationally and globally. The data suggests that the biological incidence of the disorder is relatively uniform worldwide, but cultural awareness, access to healthcare, and specific diagnostic practices heavily dictate the reported epidemiological rates.
United States Prevalence and Treatment Gaps
In the United States, reported ADHD prevalence is currently higher than the global baseline. According to data sourced from the CDC's National Center for Health Statistics Rapid Surveys System in late 2023, approximately 15.5 million U.S. adults - or 6.0% of the adult population - have a current, self-reported ADHD diagnosis 13304153. Emphasizing the reality of clinical catch-up, over half (55.9%) of these individuals received their diagnosis in adulthood 41.
Among U.S. children, the numbers are notably higher. A 2024 analysis of CDC data reports that approximately 11.4% of U.S. children aged 3 - 17 (roughly 7.1 million children) have received an ADHD diagnosis at some point in their lives 134954. This represents an increase of approximately one million newly diagnosed children between 2016 and 2022 68. Within this pediatric population, boys are diagnosed at a rate of 15% compared to 8% for girls, and the prevalence is highest among adolescents aged 12 - 17 (14.3%) compared to younger children aged 5 - 11 (8.6%) 495556.
Despite this high overall prevalence, a massive "treatment gap" persists, undercutting the narrative that the U.S. population is entirely over-medicated. The CDC reports that in 2022, nearly 2 million U.S. children with ADHD (approximately 30% of the diagnosed pediatric cohort) did not receive any ADHD-specific treatment - neither medication nor behavioral therapy 4963. Only about 32% of diagnosed children received the clinically recommended combination of both medication and behavioral treatment 4963. Among adults, the treatment gap is even wider; 36.5% of adults with ADHD received no treatment in the past year, and among those attempting to utilize stimulant pharmacotherapy, 71.5% reported severe difficulties filling their prescriptions due to ongoing national medication shortages 3063. Furthermore, ADHD is rarely an isolated condition; approximately 78% of children with ADHD have at least one co-occurring condition, with 40% experiencing comorbid anxiety, complicating treatment pathways significantly 63.
International Diagnostic Rates
Internationally, the estimated prevalence of ADHD rests at a slightly lower, though highly stable, baseline. A landmark 2024 meta-analysis published in The Lancet Psychiatry estimated the global prevalence of persistent adult ADHD at 6.76%, affecting an estimated 366.3 million adults worldwide 1241. In childhood populations, comprehensive meta-analyses point to an overall global pooled estimate of approximately 7.2% 1257.
Historically, European nations reported childhood ADHD rates at a fraction of U.S. rates, often hovering between 1% and 3% 21. This discrepancy was not biological, but bureaucratic; European nations heavily utilized the stricter ICD-10 criteria, which demanded the presence of both severe inattention and severe hyperactivity simultaneously 1215. However, recent epidemiological shifts show European and international nations converging with the U.S. as diagnostic awareness increases and diagnostic systems align.
Recent data indicates that the prevalence of childhood ADHD in France now ranges from 3.5% to 5.6% 40. Germany reports a prevalence of 4.1% for children and 3% for adults 40. In the United Kingdom, the National Health Service's Adult Psychiatric Morbidity Survey observed the proportion of adults screening positive for ADHD rise from 8.2% in 2007 to 13.9% in 2023/24, alongside a twenty-fold increase in formal adult diagnoses over the last two decades 1268. In contrast, rates in South America remain high (Colombia reports childhood prevalence up to 11-20%), while certain nations in the Middle East and Eastern Europe report rates below 1%, heavily reflecting localized stigma, lack of clinical infrastructure, and varying thresholds for pathology 3940.
Interestingly, a comprehensive analysis of global incidence and Disability-Adjusted Life Years (DALYs) trends from 1990 to 2021 indicates a marginal decline in the absolute new incidence of ADHD globally (an average annual decline of 0.6%) 3473. This global data suggests that the biological presence of ADHD is relatively stable, and the periodic surges in specific nations largely reflect sociodemographic changes, increased healthcare access, and evolving clinical definitions rather than an exploding biological epidemic 3473.
Genetic Heritability and Distinguishing Sluggish Cognitive Tempo
The foundation of the argument against ADHD as a purely sociological overdiagnosis lies in its profound biological and genetic roots. Modern psychiatric genetics has established that ADHD is one of the most highly heritable psychiatric disorders. A comprehensive review of 37 twin studies confirms a mean heritability of 74%, indicating that genetic factors account for the vast majority of the variance in the trait 8. A recent genome-wide association meta-analysis (GWAS) involving over 20,000 individuals identified 12 specific genomic regions associated with the disorder, calculating that polygenes account for about one-third of ADHD's total heritability 58.
Furthermore, neuroimaging studies consistently demonstrate structural and functional differences in the ADHD brain. For example, studies investigating striatal dopamine transporter density found that it is, on average, 14% higher in individuals with ADHD compared to neurotypical controls, directly impacting the brain's reward and executive function pathways 8.
As the biological understanding of the disorder matures, researchers are also working to refine the diagnostic boundaries to prevent the overdiagnosis of related, but distinct, conditions. Dr. Russell Barkley and others have pioneered research into "Sluggish Cognitive Tempo" (SCT), a distinct dimension of executive dysfunction characterized by daydreaming, mental fogginess, and slow information processing 4. Historically, individuals with SCT were lumped into the "Predominantly Inattentive" subtype of ADHD. However, modern research suggests SCT is a distinct clinical entity; while ADHD is fundamentally a "productivity disorder" related to motor inhibition and task execution, SCT is an "accuracy disorder" more closely linked to information processing speed and anxiety 4. Refining these boundaries ensures that individuals receive highly targeted care, reducing the risk of misapplying ADHD stimulants to patients whose primary dysfunction stems from SCT or generalized anxiety.
Conclusion
The vast body of clinical, epidemiological, and sociological research definitively answers the question of whether ADHD is overdiagnosed or underdiagnosed: it is undeniably both.
At the systemic margins, diagnostic inflation is a measurable reality. Educational environments arbitrarily pathologize the chronological immaturity of the youngest students in a cohort, driving a validated relative age effect 1617. Social media platforms algorithms amplify transdiagnostic traits, convincing the "worried well" to seek medical validation for normal human stressors 226. Concurrently, commercial telehealth entities have historically exploited regulatory leniency to drive prescription volume, fundamentally prioritizing profit over rigorous psychiatric evaluation 3733. In these specific vectors, ADHD is overdiagnosed.
However, this peripheral inflation obscures the profound, ongoing crisis of historical underdiagnosis. For decades, the psychiatric establishment effectively ignored the internalizing presentations of adult women, leading to a generation of females relying on exhausting masking strategies to survive, only to be misdiagnosed with anxiety or personality disorders when those masks inevitably failed 143752. Furthermore, millions of adults continue to suffer immense economic and personal costs due to a lack of developmentally appropriate diagnostic criteria 3647. Simultaneously, despite recent statistical improvements, marginalized racial and ethnic communities continue to face severe disparities in accessing quality treatment, frequently having their clinical symptoms misinterpreted as disciplinary issues due to systemic bias 3550.
Ultimately, ADHD is a highly valid, heavily genetic, and profoundly impairing neurodevelopmental disorder 812. The chaotic prevalence data of the 21st century does not reflect a biological epidemic, but rather a healthcare system struggling to calibrate its measurement tools. The path forward requires a transition from purely subjective, male-centric behavioral rating scales toward objective, developmentally, and culturally nuanced diagnostic frameworks that can accurately identify the silent sufferers while screening out the environmentally stressed.