Stress Inoculation and Psychological Resilience
Foundations of Stress Inoculation
Stress is a universal biological and psychological reality, defined as a generalized set of physiological and psychological responses observed when an organism is placed under challenging circumstances 1. Historically, the scientific understanding of stress was dominated by the concept of the "general adaptation syndrome," first articulated by Hans Selye, which framed stress primarily as a process that causes biological wear and tear 1. While chronic and traumatic exposure to stress frequently overwhelms the coping abilities of an individual, leading to stress-related mental disorders, controlled exposure to mild stress can yield the opposite effect. Drawing directly from the medical paradigm of vaccination, the concept of "stress inoculation" suggests that exposure to minor, manageable stressors fosters psychological preparedness and promotes long-term resilience against more severe adversity 12.
The foundational logic of stress inoculation mirrors immunology. Just as Edward Jenner's inoculation of humans with the cowpox virus stimulated the production of physical antibodies to confer immunity against the more deadly smallpox virus, the controlled introduction of psychosocial stressors stimulates the development of "psychological antibodies" 2345. This process enhances an individual's repertoire of coping mechanisms, facilitating a state of dynamic adaptation rather than pathological breakdown. The objective is not the eradication of stress, which is an inevitable aspect of the human environment, but the calibration of the organism's response systems to maintain homeostasis under pressure 15.
Contemporary research delineates stress into three distinct functional categories based on the organism's adaptive capacity. Eustress represents beneficial stress that occurs within a manageable, hermetic zone, inducing a mild response that enhances the buffering capacity of homeostasis 6. Distress refers to high-level, unmanageable stress that impairs systemic functioning and leads to psychopathology 6. Finally, sustress denotes inadequate stress, which paradoxically shrinks the buffering capacity of homeostasis by allowing coping mechanisms to atrophy through disuse 6. Stress inoculation operates by deliberately introducing eustress to expand the individual's functional capacity.
Clinical Framework of Stress Inoculation Training
Stress Inoculation Training (SIT) was developed in the 1970s and 1980s by Dr. Donald Meichenbaum as a preventative and therapeutic cognitive-behavioral intervention designed to prepare individuals for stress-inducing scenarios 378. SIT is not a rigid, session-by-session protocol, but rather a flexible, evidence-based cognitive-behavioral therapy (CBT) framework tailored to the individual's or group's unique psychosocial landscape, typically spanning eight to fifteen sessions 79.
SIT operates on the constructivist understanding of human beings as homo narrans, or storytellers 910. Meichenbaum proposed that the divergence between individuals who demonstrate resilience after trauma and those who develop post-traumatic stress disorder (PTSD) lies largely in the autobiographical narratives they construct 91011. Individuals who develop PTSD often generate fragmented, sensory-driven memories and engage in excessively negative appraisals of environmental threats 911. SIT intervenes by helping individuals "reauthor" their personal accounts, retrieving and integrating positive survival skills to construct a coherent, redemptive narrative 911.
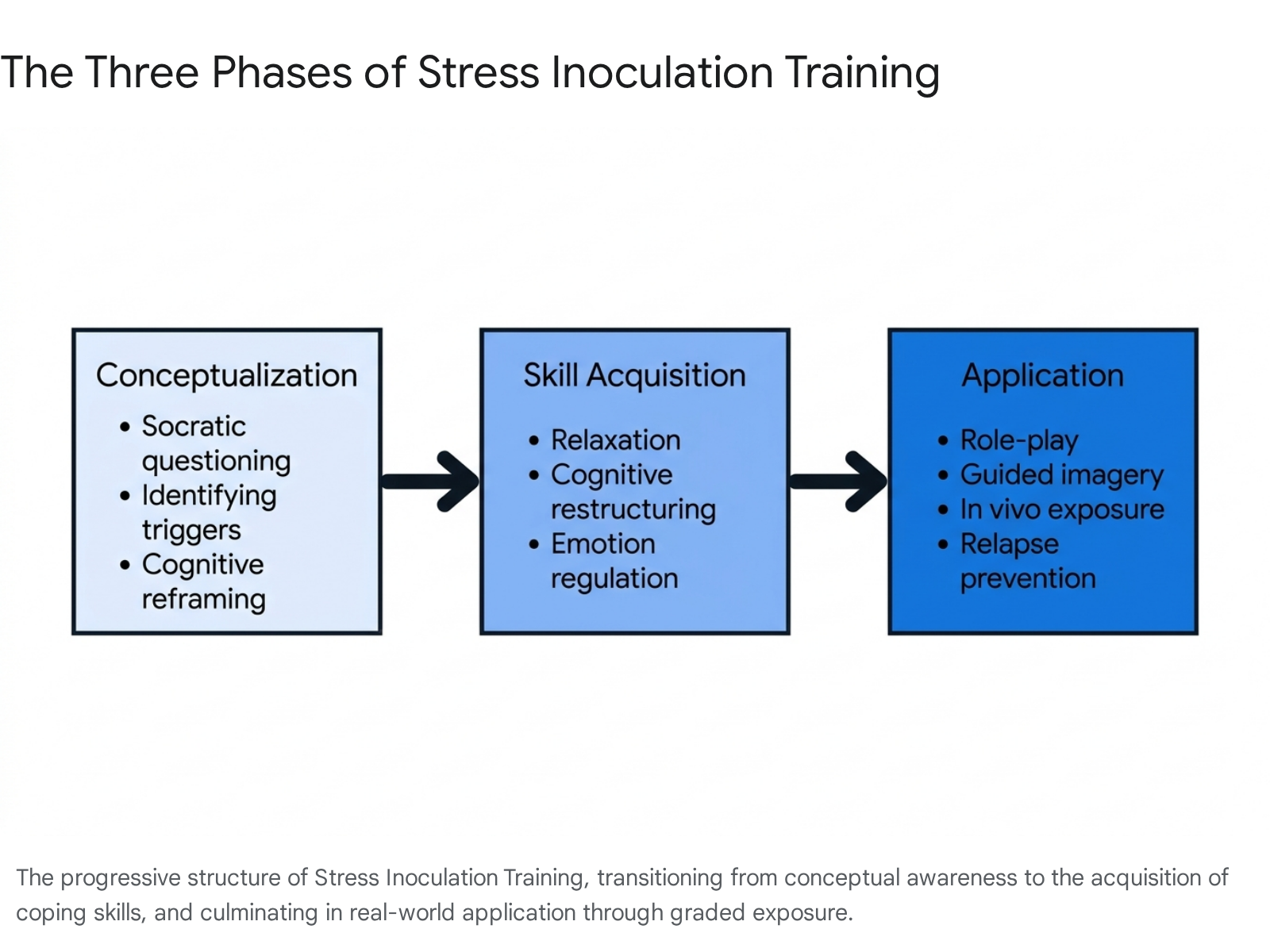
The clinical implementation of SIT is systematically structured into three distinct, overlapping phases designed to build efficacy gradually 378911.
Conceptualization Phase
The initial phase establishes a collaborative therapeutic alliance and utilizes Socratic questioning to help the individual identify their specific stress triggers and habitual response patterns 79. Patients learn to recognize the cognitive, physical, and behavioral warning signs of escalating stress. A core objective of this phase is cognitive reframing: shifting the individual's perception of stressors from overwhelming threats to manageable challenges or problems to be solved 378. The psychoeducation process also includes a discussion of the neurobiological correlates of resilience, establishing a foundation of understanding regarding how the brain processes fear and anxiety 9.
Skill Acquisition and Rehearsal Phase
Once the individual's stress profile is conceptualized, the focus transitions to building a concrete repertoire of coping skills. Because stress manifestations are heterogeneous, the skills acquired are multimodal, tailored to the patient's specific deficits 911. Therapists introduce applied relaxation techniques, such as progressive muscle relaxation and controlled breathing, to manage physical arousal 37. Cognitive restructuring techniques are employed to challenge hostile, catastrophic, or irrational self-talk 3711. Crucially, this phase leverages self-efficacy theory, encouraging patients to use self-rewarding internal dialogues to reinforce their agency over their physiological and emotional responses 37.
Application and Follow-Through Phase
The final phase operationalizes the acquired skills through graded exposure to stressors. This represents the literal "inoculation" mechanism of the therapy. Therapists employ behavioral rehearsal, guided imagery, and role-playing to simulate high-pressure scenarios 8911. These in-session rehearsal applications are eventually supplemented by in vivo (real-world) exposure to progressively more difficult situations 789. By practicing coping mechanisms in a controlled environment, the individual builds physiological and psychological tolerance. This phase also incorporates relapse prevention, assisting the individual in anticipating future high-risk scenarios and formulating contingency plans to prevent the recurrence of maladaptive responses 911.
| Training Phase | Primary Objective | Key Clinical Interventions |
|---|---|---|
| Conceptualization | Establish therapeutic alliance and understand stress patterns. | Socratic questioning, psychoeducation, identification of triggers, cognitive reframing of threats into challenges. |
| Skill Acquisition | Develop a multimodal repertoire of coping mechanisms. | Progressive muscle relaxation, cognitive restructuring, problem-solving training, emotion regulation, positive self-statements. |
| Application | Operationalize skills through controlled exposure to stressors. | Guided imagery, behavioral rehearsal, role-playing, in vivo graded exposure, relapse prevention planning. |
Neurobiological Mechanisms of Resilience
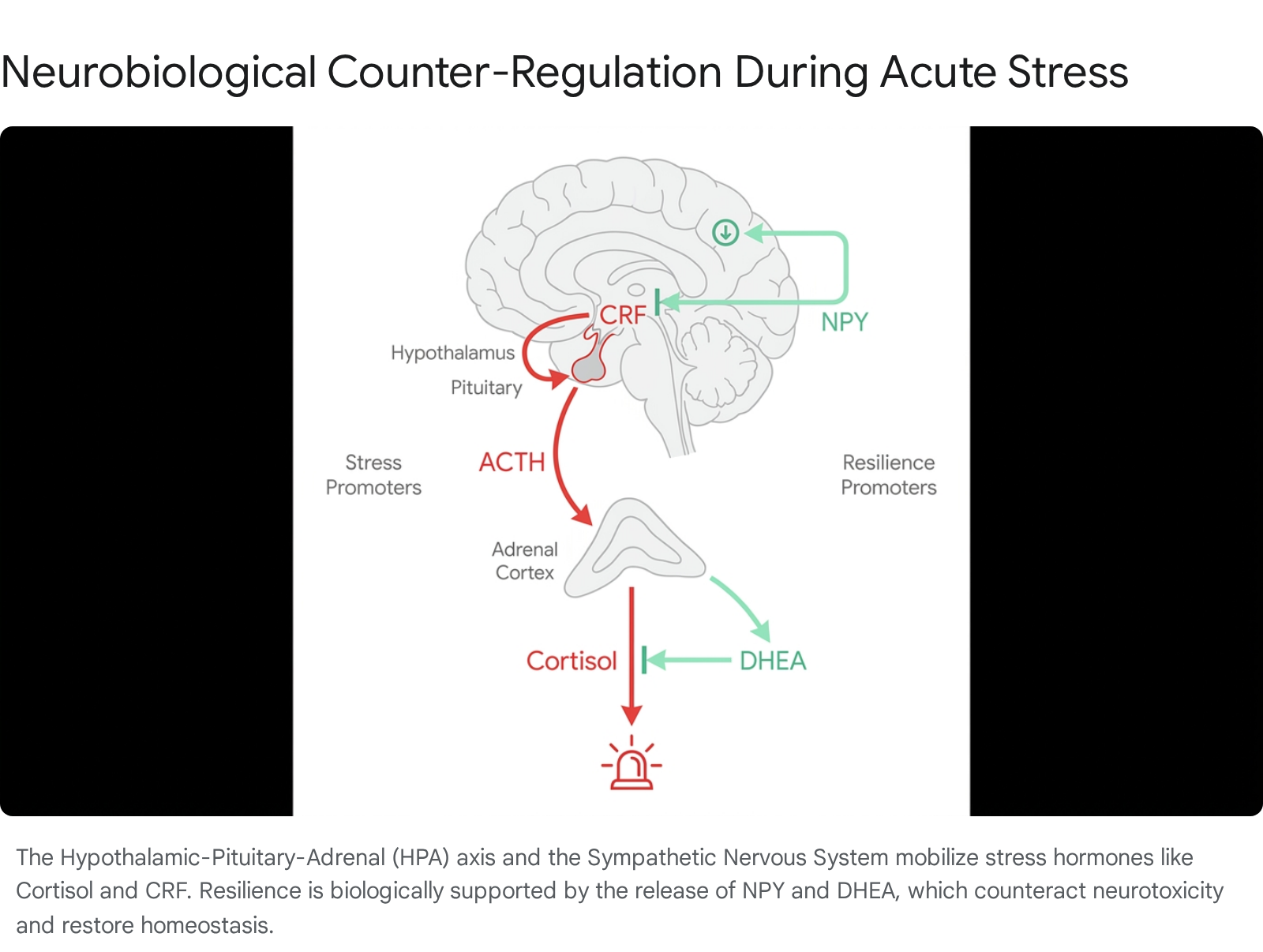
Psychological resilience is heavily underpinned by distinct neurobiological and endocrine mechanisms. When an organism faces adversity, the autonomic nervous system (ANS) and the hypothalamic-pituitary-adrenal (HPA) axis are mobilized 12. The hypothalamus secretes corticotropin-releasing factor (CRF), stimulating the pituitary gland to release adrenocorticotropic hormone (ACTH), which in turn triggers the adrenal cortex to synthesize glucocorticoids, primarily cortisol, to mobilize energy 1213. While cortisol is essential for immediate survival, prolonged elevation is neurotoxic and impairs higher-order cognitive function. Successful stress inoculation is characterized by the presence of specific biomarkers that actively downregulate and counterbalance this stress response 13.
Regulatory Role of Dehydroepiandrosterone
Dehydroepiandrosterone (DHEA) and its sulfate metabolite (DHEAS) are anabolic steroid hormones synthesized primarily in the adrenal cortex 1415. DHEA functions as a critical neurosteroid that exerts neuroprotective, anxiolytic, and antidepressant effects throughout the central nervous system 15. Crucially, DHEA acts as a biological antagonist to cortisol. During acute stress, DHEA levels increase in tandem with cortisol, but a higher DHEA-to-cortisol ratio is strongly correlated with relative stress resilience 1316.
Clinical evaluations of military combat veterans undergoing survival training demonstrate that high DHEA-to-cortisol ratios are associated with reduced dissociation and superior task performance under severe duress 17. Meta-analytic data encompassing 14 studies confirm that DHEA acts as a reliable biomarker of acute stress, peaking immediately after a stressful event and aiding in the rapid restoration of homeostasis, thereby mitigating the negative mood and cognitive impairments typically induced by excess cortisol 161819.
Function of Neuropeptide Y
Neuropeptide Y (NPY) is a 36-amino-acid peptide abundantly distributed throughout the central and peripheral nervous systems, with the highest concentrations found in the hypothalamus 20. NPY plays a direct role in regulating anxiety, fear, and the systemic stress response by counteracting the effects of corticotropin-releasing factor (CRF). While CRF initiates the panic and fear cascades, NPY dampens amygdala excitability and prevents the over-activation of the sympathetic nervous system, specifically by potentiating peripheral vasoconstriction mediated by norepinephrine 13.
Clinical studies reveal that serum NPY levels are significantly lower in patients suffering from depression and anxiety disorders compared to healthy, resilient controls 20. Furthermore, genetic variants of the NPY gene (such as specific alleles of the NPY SNP rs16147) have been linked to variations in treatment response and innate resilience, demonstrating that NPY availability is a fundamental biological determinant of how an individual processes adversity 20.
Brain Architecture and Neuroplasticity
Beyond acute hormonal regulation, repeated exposure to manageable stress structurally alters brain architecture through neuroplasticity. The structural integration of early-life stress involves mechanisms such as neurogenesis, synaptogenesis, and synaptic pruning 21. Functional neuroimaging demonstrates that resilient individuals exhibit greater structural connectivity between the prefrontal cortex (PFC) and the amygdala, allowing for superior top-down cognitive control over emotional reactivity 121.
Current research conceptualizes the impact of stress through integrated models, including the Match/Mismatch Hypothesis, which posits that early stress programs the organism for adult stress, and the Cumulative Stress Hypothesis, which tracks allostatic load over time 21. Processes such as adult hippocampal neurogenesis (AHN) are stimulated by manageable stress, actively reversing the neuronal atrophy typically caused by chronic trauma 21. Recent clinical trials focusing on cognitive bias modification demonstrate that training individuals to routinely recall positive, self-relevant memories directly lowers daytime cortisol levels, proving that structured cognitive resilience strategies exert measurable neuroendocrine effects 22.
Habituation Versus Sensitization Pathways
The efficacy of stress inoculation relies heavily on the characteristics of the stress exposure. The neurobiological response to repeated stress bifurcates into two opposing learning pathways: habituation and sensitization 222324.
Habituation is defined as a form of non-associative learning characterized by a decrease in physiological and psychological responsiveness to a repeated, identical (homotypic) stimulus 22232425. When an individual is exposed to a manageable stressor, the initial activation of the HPA axis redistributes metabolic resources. If the individual successfully copes with this challenge, subsequent exposures to similar stressors elicit a markedly attenuated cortisol response 42223. Animal models confirm this trajectory; infant squirrel monkeys subjected to brief, intermittent periods of maternal separation exhibit a reduced hormonal stress response, enhanced exploratory behavior, and larger prefrontal cortex volumes later in life compared to non-inoculated controls 141226. Approximately 60% to 70% of healthy human individuals experience this habituation process when repeatedly exposed to acute stress tests 23.
Conversely, sensitization occurs when the initial stressor is overwhelming, chronic, unpredictable, or uncontrollable. In these scenarios, the biological system does not habituate; instead, neuronal activity in response to the stimulus increases 242728. The threshold for tolerating future stress is lowered, resulting in an exaggerated, hyper-reactive physiological response even to minor subsequent stressors 242729.
Conditions for Stress Sensitization
The stress sensitization model provides a critical boundary condition for resilience training. Exposure to severe early childhood adversity - such as emotional maltreatment, physical abuse, or profound neglect - rarely acts as an inoculant. Instead, it systematically sensitizes the individual, significantly increasing the risk for major depression, post-traumatic stress disorder, and severe anxiety disorders later in life 2728303132.
A landmark longitudinal randomized controlled trial involving children abandoned to Romanian institutions provided stark experimental evidence of this phenomenon. The study revealed that severe early neglect sensitized children to the effects of later stressful life events, resulting in broadband externalizing problems in adolescence 2733. Notably, this sensitization effect was absent in children who were randomly assigned to high-quality foster care early in life, demonstrating that positive caregiving can interrupt the biological sensitization process 2733.
Similarly, population studies among military personnel reveal that individuals with a history of frequent emotional or physical childhood maltreatment exhibit a statistically stronger risk for past 30-day major depressive episodes when faced with adult stressors compared to peers without such histories 3132. Sensitization is characterized by a lack of adaptive capacity, where early exhaustion of stress coping mechanisms degrades systemic performance 2229.
Allostatic Load and Systemic Degradation
A popular cultural aphorism posits that "what doesn't kill you makes you stronger." However, rigorous psychobiological research systematically refutes the universality of this claim 34353736. While moderate adversity can inoculate an individual and promote post-traumatic growth, chronic, severe, or unmitigated trauma fundamentally breaks down systemic biological functioning 3937. When distress is prolonged, it exacts a severe metabolic toll, quantified as "allostatic load."
Allostasis refers to the body's active process of maintaining stability through physiological change in response to dynamic stressors 3839. While allostasis is highly adaptive in the short term, the continuous, prolonged activation of the HPA and sympathetic-adrenal-medullary (SAM) axes results in allostatic load - the cumulative biological wear and tear on the body and brain 384340.
The Energetic Model of Allostatic Load
Recent scientific advancements propose the Energetic Model of Allostatic Load (EMAL) to explain how chronic stress transduces into physical disease. Living organisms possess a finite capacity to consume and metabolize energy 41. Chronic stress forces the brain and body into a state of severe hypermetabolism to sustain the allostatic response. This massive energetic diversion away from routine biological maintenance, cellular repair, and growth leads to accelerated biological aging, rapid telomere shortening, and epigenetic degradation 41.
Clinically, allostatic load is calculated using a composite index of biomarkers spanning the cardiovascular, metabolic, and immune systems. These typically include systolic and diastolic blood pressure, hemoglobin A1c, waist-to-hip ratio, HDL cholesterol, body mass index, and C-reactive protein 394046. In comprehensive cohort studies, such as the All of Us Research Program, individuals scoring above the 75th percentile (an AL score ≥ 6 on a 12-point scale) are classified as having "High AL" 4243.
High allostatic load serves as a powerful preclinical indicator of premature mortality 3846. Data indicates an inverse correlation between allostatic load and endothelial function (measured via flow-mediated dilation), linking chronic stress directly to vascular dysfunction 39. Furthermore, research among cancer survivors demonstrates that a mere 1-point increase in allostatic load prior to cancer diagnosis corresponds to a 10% to 16% heightened risk of major adverse cardiac events (MACE), including heart failure and ischemic stroke, within two years 44.
Social determinants of health heavily influence allostatic load. Neighborhood environments with low educational, health, and economic opportunity are significantly associated with higher allostatic load counts, reflecting the physiological burden of structural deprivation 40. Similarly, marked racial disparities exist, with Black participants frequently demonstrating higher secondary mediator scores and elevated allostatic load compared to White participants, driven by the cumulative impact of social stressors 43. Consequently, the assertion that surviving severe trauma automatically engenders strength is a biological fallacy; without intervention, severe trauma leaves a legacy of hidden systemic degradation.
Cross-Stressor Adaptation Hypothesis
One of the most effective, non-pharmacological interventions for building systemic resilience and lowering allostatic load is regular physical exercise. The mechanism behind this benefit is delineated by the "cross-stressor adaptation hypothesis" 45464748.
The hypothesis posits that because physical activity is itself a controlled physiological stressor, regular participation trains and habituates the body's stress response systems 474849. As cardiovascular and neuroendocrine efficiency improves in response to physical exertion, these physiological adaptations transfer - or "cross over" - to buffer the individual against non-physical, psychosocial and emotional stressors 474849. When an emotionally taxing event occurs, the pre-adapted HPA axis responds with reduced vigor and recovers to emotional equilibrium more rapidly 47.
Laboratory studies utilizing the Trier Social Stress Test (TSST) provide empirical support for this mechanism. Individuals with higher cardiorespiratory fitness exhibit attenuated cortisol secretion, reduced heart rate reactivity, and smaller increases in state anxiety when subjected to acute psychosocial stress compared to sedentary controls 234650. The benefits extend to structural changes; aerobic activity elevates brain-derived neurotrophic factor (BDNF) by up to 31%, enhancing mood and cognitive capacity, while modulating monoamine systems to increase synaptic serotonin availability 51. Furthermore, team-based exercise environments teach adaptive behavioral coping strategies - such as problem-focused engagement and emotional regulation - amplifying the physiological benefits through integrated social support structures 51.
| Mechanism of Adaptation | Physiological Response | Psychological Benefit |
|---|---|---|
| Cardiovascular Habituation | Lower resting heart rate; faster heart rate recovery post-stress. | Reduced perception of panic and somatic anxiety symptoms. |
| HPA Axis Regulation | Attenuated cortisol secretion during non-physical stressors. | Decreased emotional reactivity; faster return to equilibrium. |
| Neurotrophic Modulation | Increased peripheral Brain-Derived Neurotrophic Factor (BDNF). | Enhanced mood, improved cognitive flexibility, and stress resilience. |
| Social / Behavioral Engagement | Increased social support and cooperative goal pursuit. | Reduction in isolation-induced depression; fulfillment of belongingness needs. |
Applications in High Adversity Occupations
Populations routinely exposed to potentially traumatic events (PTEs), such as military personnel, emergency medical technicians, and law enforcement officers, require highly specialized stress inoculation. These roles are classified as High Adversity Occupations (HAOs) 5253. The demands of these occupations place daily psychological and physiological stress on personnel, increasing their risk for cardiovascular disease, metabolic syndrome, and post-traumatic stress disorder 5254.
Under extreme, unmitigated stress, the human central nervous system exhibits predictable, catastrophic performance degradation. Research indicates that once a human heart rate exceeds 145 beats per minute (BPM) due to acute stress arousal, fine motor skills rapidly disintegrate 60. When the heart rate surpasses 175 BPM, cognitive processing fails entirely, accompanied by auditory exclusion and a loss of up to 70% of peripheral vision due to amygdala hijacking 60.
To counteract this physiological override, military and law enforcement units utilize rigorous SIT methodologies. The objective is to build a psychological immunity to the effects of adrenaline by forcing personnel to execute complex cognitive and physical tasks while their sympathetic nervous systems are deliberately driven to extreme arousal 60. For example, the Singapore Army Commandos employ intense physical and psychological screening prior to specialized counter-insurgency training, ensuring candidates have the baseline musculoskeletal and cardiovascular integrity required to survive stress inoculation protocols 61.
Modern advancements in this field include Virtual Reality-Stress Inoculation Training (VR-SIT), which exposes medical military personnel to highly immersive, chaotic combat scenarios 55. By repeatedly facing these virtual stressors and employing controlled relaxation and cognitive restructuring techniques, personnel build neurological pathways that allow the prefrontal cortex to remain active even when flooded with adrenaline, effectively converting the maladaptive "freeze" response into actionable, goal-directed behavior 6055. However, if rest intervals are insufficient, intense physical inoculation can result in adverse outcomes, necessitating strict evacuation and safety oversight protocols 61.
Cross-Cultural Perspectives and Institutional Models
Because resilience is determined by a complex interplay of biology, psychology, and environment, Stress Inoculation Training and resilience-building frameworks cannot be uniformly applied without considering cultural context. A significant limitation in historical resilience research is the reliance on samples from Western, Educated, Industrialized, Rich, and Democratic (WEIRD) societies 56. Western models of resilience traditionally emphasize individual self-efficacy, autonomy, and corporate occupational performance 5657.
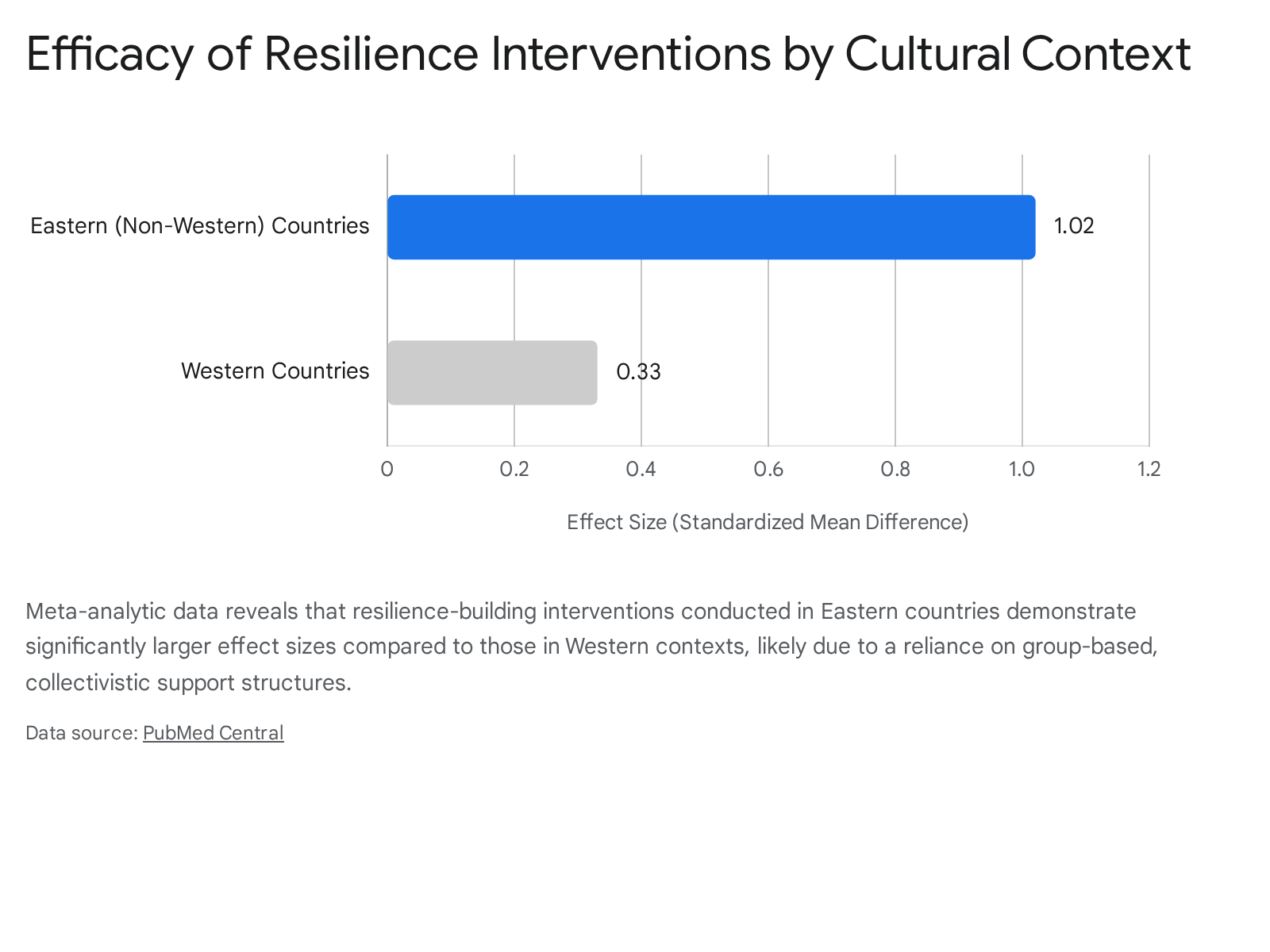
However, systematic reviews comparing resilience interventions reveal distinct cultural variances in how stress inoculation is applied. Research analyzing interventions across Eastern and non-Western countries (e.g., China, India, Iran, Thailand) indicates that resilience programs in these regions lean heavily toward group-based settings and frequently target family caregivers or general community populations rather than isolated corporate employees 56.
Meta-analytic data evaluating 43 studies involving over 6,200 participants demonstrated that interventions in Eastern countries yield significantly larger effect sizes for improving overall resilience compared to their Western counterparts 56.
The emphasis on collectivistic coping, extended social regulation, and community support in non-Western models appears to provide a more robust buffer for psychological immunity 5665. Self-regulation develops most effectively on top of robust social regulation; environments that foster secure attachment and peer support reduce cortisol reactivity and accelerate cognitive recovery 65.
Systemic Models of Institutional Resilience
Recognizing that individual psychological resilience cannot entirely overcome severe structural deprivation or systemic occupational burnout, researchers in the Global South, particularly in South Africa, are pioneering transdisciplinary, socio-ecological models of resilience 5859. The Integrated Student Well-being and Resilience (ISWR) Model, tailored to South African health professions education, addresses the syndemic of academic overload, historical inequality, and financial vulnerability 5859.
Grounded in Bronfenbrenner's Socio-Ecological Systems Theory, these institutional models argue explicitly against the "resilience fallacy" - the deleterious idea that individuals should merely toughen up in the face of systemic institutional failure 58. Instead, true resilience training at the institutional level requires a multi-tiered public health approach. This involves proactive, system-level interventions, such as workload audits, early alert systems, and coordinated crisis protocols to redistribute academic pressure and stabilize the campus climate before distress escalates 58. By shifting the focus from reactive, individual counseling to proactive, systemic architecture, these frameworks coordinate institutional governance with the complex psychosocial needs of the population, ensuring that resilience is cultivated as a shared environmental resource rather than solely an individual burden 5860.