Severe hantavirus pulmonary syndrome treatments and critical care
Introduction and Epidemiological Context
Hantaviruses comprise a diverse group of enveloped, negative-sense, single-stranded RNA viruses belonging to the genus Orthohantavirus within the family Hantaviridae and the order Bunyavirales 123. These zoonotic pathogens are primarily maintained in sylvatic rodent reservoirs, causing persistent, asymptomatic infections in their natural host species. Infected rodents shed substantial viral loads continuously through urine, feces, and saliva 4. Human transmission typically occurs via the inhalation of aerosolized viral particles originating from rodent excreta, although exposure through direct mucosal contact or rodent bites has also been thoroughly documented 45.
Globally, hantavirus infections manifest in two distinct and severe acute febrile syndromes, largely delineated by geographic distribution and the specific viral clade involved 136. In Eurasia, Old World hantaviruses - predominantly the Hantaan virus (HTNV), Seoul virus (SEOV), Dobrava-Belgrade virus (DOBV), and Puumala virus (PUUV) - cause Hemorrhagic Fever with Renal Syndrome (HFRS) 126. HFRS is characterized by profound vascular leakage affecting the renal system, culminating in acute kidney injury, hemorrhagic manifestations, and shock, carrying a case fatality rate that generally ranges from 1% to 15% depending on the causative strain and regional healthcare infrastructure 1267.
Conversely, in the Americas, New World hantaviruses cause Hantavirus Pulmonary Syndrome (HPS), a condition frequently referred to interchangeably as Hantavirus Cardiopulmonary Syndrome (HCPS) 128. The predominant etiologic agents for HPS are the Sin Nombre virus (SNV) in North America and the Andes virus (ANDV) in South America 128. Unlike HFRS, HPS primarily targets the pulmonary microvasculature. The infection induces a rapid and massive capillary leak syndrome that floods the alveolar spaces, resulting in non-cardiogenic pulmonary edema, severe hypoxia, and profound cardiopulmonary collapse 69. The case fatality rate for severe HPS is exceptionally high, consistently estimated between 30% and 50%, cementing its status as one of the most lethal viral respiratory diseases in existence 11011.
The urgency surrounding the standardization of critical care protocols and the accelerated development of targeted therapeutics for HPS was significantly amplified by a severe outbreak in early 2026 aboard the cruise ship MV Hondius 111210. Departing from Ushuaia, Argentina, the vessel experienced a confirmed cluster of the Andes virus among passengers and crew. This specific outbreak resulted in at least eight recognized cases - six laboratory-confirmed and two probable - and three fatalities, representing a 38% case fatality ratio within the cluster 81011. The event underscored a unique and highly dangerous characteristic of the Andes virus: it remains the only hantavirus species with a conclusively documented capacity for person-to-person transmission 171012. The international public health response to the Hondius outbreak, which necessitated mandatory quarantines, the activation of high-level isolation units, and aggressive contact tracing across multiple continents, has intensely focused global attention on emergency intensive care algorithms and the rapid progression of specific antiviral countermeasures 12131714.
Pathogenesis and Endothelial Dysfunction
The underlying pathophysiology of Hantavirus Pulmonary Syndrome is fundamentally driven by the virus's interaction with the human microvascular endothelium. The hantavirus genome is tripartite, comprising Small (S), Medium (M), and Large (L) segments. The S segment encodes the viral nucleocapsid (N) protein, the M segment encodes the envelope glycoproteins (Gn and Gc), and the L segment encodes the viral RNA-dependent RNA polymerase (RdRp) 23. The Gn and Gc glycoproteins mediate the initial viral entry into host cells by binding to specific host surface receptors, most prominently the $\beta_3$ integrin, which is highly expressed on the surface of human endothelial cells and platelets 15.
Unlike many cytopathic viruses that cause direct lytic destruction of the cells they infect, hantaviruses do not typically induce gross structural necrosis in the human endothelium. Post-mortem histological examinations of fatal HPS cases consistently reveal remarkably intact cellular architecture without significant tissue destruction or cellular lysis 16. Therefore, the profound vascular leakage and subsequent non-cardiogenic pulmonary edema that characterize HPS are understood to be the result of a hyperactive host immune response rather than direct viral cytopathy 916. The viral infection triggers a massive, dysregulated immune cascade commonly termed a "cytokine storm," marked by the excessive release of pro-inflammatory mediators, including tumor necrosis factor-alpha (TNF-$\alpha$), interferon-gamma (IFN-$\gamma$), and interleukin-6 (IL-6) 1718.
Mechanisms of Interleukin-6 Trans-Signaling
Recent virological and immunological investigations into hantavirus pathogenesis have elucidated the complex role of interleukin-6 (IL-6) in mediating the transition from localized endothelial infection to systemic capillary leak. IL-6 signaling operates via two distinct mechanistic pathways: classical signaling and trans-signaling 1920. In classical signaling, IL-6 binds to the membrane-bound IL-6 receptor (mIL-6R), which is primarily expressed on hepatocytes and specific leukocyte subsets. This receptor-ligand complex then associates with the universally expressed signal-transducing glycoprotein 130 (gp130) to initiate downstream Janus kinase/signal transducer and activator of transcription (JAK-STAT) pathways 1920. Classical signaling is generally homeostatic and plays a critical protective role in resolving acute inflammation.
However, in severe hantavirus infections, an alternative mechanism known as IL-6 trans-signaling becomes pathologically dominant. In this pathway, IL-6 binds to a soluble, truncated form of the IL-6 receptor (sIL-6R) circulating in the plasma. The resulting IL-6/sIL-6R complex can interact with membrane-bound gp130 on virtually any cell type in the body, most notably targeting pulmonary microvascular endothelial cells that do not normally express mIL-6R 1920.
Clinical outcome data indicate that patients with severe hantavirus disease exhibit a markedly elevated ratio of sIL-6R to soluble gp130 (sgp130), a naturally occurring antagonist that typically neutralizes the circulating IL-6/sIL-6R complex 1920. Advanced in vitro models demonstrate that treating hantavirus-infected endothelial cells with sIL-6R rapidly upregulates intercellular adhesion molecule 1 (ICAM-1) and severely disrupts vascular endothelial (VE)-cadherin junctions. This biochemical disruption leads directly to the physical breakdown of the endothelial barrier 20. Consequently, the degree of IL-6 trans-signaling observed in clinical subjects correlates negatively with serum albumin levels (a primary indicator of fluid extravasation) and positively with overall disease severity, the requirement for mechanical ventilation, and mortality 1920.
Clinical Trajectory and Hematological Presentation
The clinical trajectory of Hantavirus Pulmonary Syndrome follows a highly stereotyped temporal pattern. The disease advances through four distinct clinical phases: the prodromal phase, the cardiopulmonary phase, the diuretic phase, and the convalescent phase 1521. Recognition of the specific phase is critical for the application of appropriate critical care interventions, as therapies that may be beneficial in one phase can be disastrous in another.
| Clinical Phase | Typical Duration | Hallmark Symptoms and Pathophysiology | Key Laboratory Indicators |
|---|---|---|---|
| Incubation | 7 to 42 Days | Asymptomatic viral replication following exposure. | No acute markers; retrospective PCR/serology. |
| Prodromal | 3 to 6 Days | High fever, severe myalgias, headache, chills, and profound gastrointestinal distress (nausea, vomiting, diarrhea). | Developing thrombocytopenia; left-shifted myeloid lineage; absence of toxic granulation. |
| Cardiopulmonary | Hours to Days | Rapid onset of dry cough, progressive dyspnea, and hypoxia. Massive capillary leak leading to non-cardiogenic pulmonary edema and cardiogenic shock. | Profound hemoconcentration (rising hematocrit); falling serum albumin; immunoblasts >10%; elevated lactate. |
| Diuretic | Days to Weeks | Spontaneous clearance of extravascular lung water. Resolution of pulmonary edema and stabilization of hemodynamics. | Normalization of hematocrit; gradual recovery of platelet counts; improving PaO2:FiO2 ratios. |
| Convalescent | Weeks to Months | Gradual return to baseline pulmonary function. Prolonged fatigue and exercise intolerance are common. | Seroconversion (IgG presence); resolution of acute phase reactants. |
Following an incubation period that typically ranges from 14 to 21 days - but can span from 7 to 42 days - the patient experiences an abrupt onset of the prodromal phase 1726. Symptoms in this phase are notoriously non-specific and flu-like, universally including high fever, severe myalgias (frequently localized to the lower back and thighs), severe headache, chills, and profound gastrointestinal distress 178. Notably, upper respiratory symptoms such as coryza or sore throat are typically absent, which serves as a vital diagnostic clue distinguishing early HPS from other common viral respiratory infections 4.
The transition from the prodrome to the cardiopulmonary phase is abrupt and often catastrophic, typically developing over a matter of 24 to 48 hours 9. It is marked by the onset of a dry, persistent cough and rapidly progressive dyspnea as capillary leak floods the pulmonary interstitium. Patients swiftly develop hypoxia, extensive non-cardiogenic pulmonary edema, and a severe distributive shock that quickly evolves into refractory cardiogenic shock due to extreme, virus-induced myocardial depression 922. Hemodynamic collapse during this phase is the primary cause of mortality in HPS 2223.
Patients who survive the cardiopulmonary collapse eventually enter the diuretic phase, characterized by the rapid clearance of extravascular lung water and the onset of profound, spontaneous diuresis. Clinical stabilization, weaning from vasoactive support, and extubation typically occur during this window 21. The final convalescent phase requires weeks to months; while pulmonary function generally returns to baseline, survivors frequently report prolonged fatigue, generalized weakness, and persistent myalgias 21.
Critical Care Standards and Infection Control
The medical management of severe HPS is entirely supportive; there is currently no globally approved, specific antiviral therapy 716. Patient survival is heavily dependent on a high index of early clinical suspicion, rapid emergency triage, meticulous fluid management, advanced hemodynamic monitoring, and the timely, protocolized application of extracorporeal life support 1622.
Diagnostic Triage and Precautions
Because the initial symptoms of HPS are indistinguishable from myriad other acute febrile illnesses, early recognition relies on specific epidemiological context - such as recent travel to endemic areas, occupational exposure to sylvatic rodents, or known contact with confirmed cases - combined with highly specific hematological markers 2224. A peripheral blood smear analyzed early in the disease course can provide a rapid, highly sensitive presumptive diagnosis. The classic pentad of hematological findings indicative of advancing HPS includes profound thrombocytopenia (often dropping below 40,000/μL), a marked left shift in the myeloid lineage, the distinct absence of toxic granulation, the presence of atypical lymphocytes (with immunoblasts comprising >10% of the lymphoid lineage), and significant hemoconcentration 2224. Clinically, a rapidly rising hematocrit occurring concurrently with falling serum albumin is highly predictive of the massive capillary leak syndrome that immediately precedes total cardiopulmonary collapse 24.
Stringent infection control protocols must be enforced immediately upon clinical suspicion. While strains like the Sin Nombre virus are not known to transmit from human to human, the Andes virus possesses a well-documented capacity for interpersonal transmission 1712. Research following outbreaks in South America indicates that the risk of secondary infection is acute among close contacts, showing a 17.6% transmission risk to sexual partners and a 1.2% risk to other household contacts 24. Secondary transmission to healthcare workers exposed to respiratory secretions has also been documented 1025.
Consequently, clinical guidelines issued by international health authorities mandate that any patient with suspected HPS - particularly those with a travel history to South America or linkage to maritime clusters - be managed with strict Contact, Droplet, and Airborne Precautions 710. This requires immediate placement in single-patient, negative-pressure airborne infection isolation rooms, and the mandatory use of N95 or higher respirators, comprehensive eye protection, fluid-resistant gowns, and gloves by all healthcare personnel entering the patient environment 71025. Strict surveillance and symptom monitoring of exposed healthcare workers and close contacts must be maintained for a minimum of six weeks post-exposure, encompassing the outer limit of the viral incubation period 7.
Hemodynamic Monitoring Paradigms
The hemodynamic profile of HPS is exceptionally complex and highly dynamic. It initiates as a severe distributive shock, presenting with low systemic vascular resistance and normal or even elevated cardiac output, which rapidly shifts into a profound hypovolemic state driven by massive capillary leak 22. In the most critical stages, patients develop profound myocardial depression, culminating in severe cardiogenic shock 1622. Navigating the extremely narrow therapeutic window between maintaining adequate systemic end-organ perfusion and exacerbating fatal pulmonary edema requires highly sophisticated, continuous hemodynamic monitoring.
Historically, the Pulmonary Artery Catheter (PAC), or Swan-Ganz catheter, served as the gold standard in intensive care for monitoring right-sided heart pressures and estimating left ventricular filling via Pulmonary Artery Occlusion Pressure (PAOP) 2326. However, in pathological states characterized by extreme, acute capillary leak - such as severe HPS - intravascular pressure is a highly unreliable surrogate for actual intravascular volume status or the degree of pulmonary edema.
Modern critical care algorithms for HPS have largely transitioned to Transpulmonary Thermodilution (TPTD) devices, most notably the Pulse Contour Cardiac Output (PiCCO) system 23262728. TPTD provides continuous, beat-to-beat cardiac output analysis through arterial pulse contour analysis, calibrated via intermittent central venous cold saline injections detected by a specialized femoral or axillary arterial thermistor 28. Critically, TPTD calculates precise volumetric indices rather than relying solely on proxy pressure metrics.
| Monitoring Parameter | Traditional Pulmonary Artery Catheter (Swan-Ganz) | Transpulmonary Thermodilution (PiCCO) | Relevance to HPS Clinical Management |
|---|---|---|---|
| Cardiac Output | Intermittent right heart thermodilution. | Continuous pulse contour analysis; calibrated via TPTD. | Continuous data allows for the immediate detection of sudden myocardial depression and the onset of cardiogenic shock. |
| Preload Assessment | Central Venous Pressure (CVP) and Pulmonary Artery Occlusion Pressure (PAOP). | Global End-Diastolic Volume Index (GEDVI) and Intrathoracic Blood Volume Index (ITBVI). | Pressure metrics (PAOP) fail in HPS due to extreme capillary leak. Volumetric indices (GEDVI/ITBVI) reliably assess true intravascular fluid status. |
| Pulmonary Edema | Inferred clinically, radiographically, or via high PAOP suggesting cardiogenic origin. | Extravascular Lung Water Index (EVLWI). | PiCCO directly quantifies lung water. In HPS, EVLWI is markedly elevated regardless of filling pressures, enforcing strict fluid restriction protocols. |
| Capillary Leak | Cannot directly differentiate hydrostatic vs. high-permeability edema. | Pulmonary Vascular Permeability Index (PVPI). | PVPI actively differentiates permeability edema from pure hydrostatic edema. A highly elevated PVPI confirms the specific pathophysiology of HPS. |
| Volume Responsiveness | Limited static indicators. | Stroke Volume Variation (SVV) and Pulse Pressure Variation (PPV). | SVV/PPV accurately predict if a hypotensive patient will improve with fluids, avoiding the iatrogenic exacerbation of pulmonary alveolar flooding. |
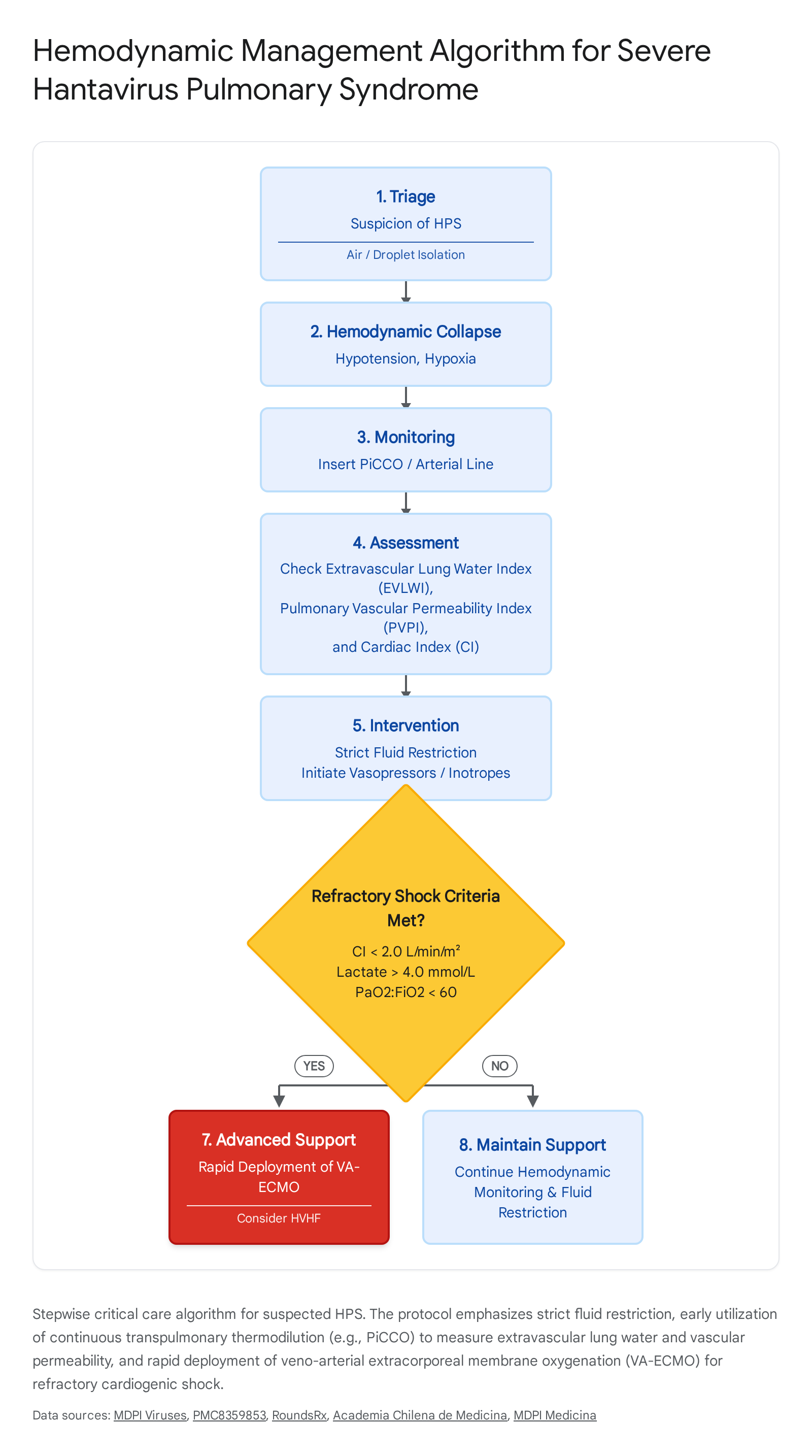
In the management of HPS, the most vital parameters generated by TPTD are the Extravascular Lung Water Index (EVLWI) and the Pulmonary Vascular Permeability Index (PVPI) 2729. In severe HPS, EVLWI is invariably and severely elevated - often reaching up to 14 mL/kg, compared to a normal physiological range of 3 to 7 mL/kg - due to the rapid shifting of intravascular fluid into the alveolar space 232728. Concurrently, the PVPI confirms that this massive edema is fundamentally driven by high vascular permeability rather than hydrostatic pressure overload, definitively characterizing the nature of the shock 232728.
Resuscitation Strategies and Vasoactive Support
The clinical approach to fluid resuscitation in HPS is diametrically opposed to standard critical care protocols for bacterial septic shock 724. While aggressive, early fluid boluses are strictly indicated in standard sepsis, administering high volumes of crystalloids to an HPS patient rapidly and irreversibly exacerbates pulmonary edema due to the severely compromised endothelial barrier 79. Fluid administration in HPS must be exceedingly cautious and restricted.
Hypotension should be managed aggressively and early with the initiation of vasopressors, such as norepinephrine, to support failing systemic vascular resistance. As disease progression leads to myocardial depression, robust inotropic support, commonly utilizing dobutamine or epinephrine, is frequently required to maintain adequate cardiac output 722. Goal-directed therapy algorithms focus entirely on maintaining a mean arterial pressure (MAP) greater than 65 mmHg and sustaining a viable cardiac index while strictly minimizing EVLWI 28.
Extracorporeal Life Support and Extracorporeal Depuration
Despite maximal optimization of mechanical ventilation and aggressive, multi-agent vasoactive support, a significant subset of severe HPS patients will inevitably progress to refractory cardiopulmonary collapse. In these catastrophic scenarios, Veno-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO) stands as the definitive, life-saving intervention 162223. VA-ECMO provides both complete respiratory gas exchange and full hemodynamic support, effectively bypassing the failing pulmonary and cardiovascular systems to maintain systemic perfusion until the viral-induced cytokine storm subsides and the vascular endothelium can regenerate.
The timing of ECMO cannulation is the single most critical determinant of patient survival. Retrospective clinical analyses indicate a remarkable 80% survival rate for HPS patients who undergo preemptive ECMO cannulation prior to total hemodynamic collapse, compared to a meager 54% to 56% survival rate when cannulation is delayed until after full cardiopulmonary arrest has occurred 1624. Established intensive care criteria for initiating VA-ECMO in HPS include a cardiac index persistently remaining below 2.0 L/min/m2 despite maximal combined inotropic and vasopressor support, accompanied by at least one of the following high-mortality clinical predictors: a serum lactate level rising relentlessly above 4.0 mmol/L, a PaO2:FiO2 ratio precipitously falling below 60, or the onset of refractory, life-threatening arrhythmias 2324.
Furthermore, continuous renal replacement therapies, specifically High-Volume Hemofiltration (HVHF), are increasingly deployed as a potent adjunctive therapy prior to or alongside ECMO. HVHF is utilized not only to manage the acute kidney injury commonly seen in severe hantavirus infections but also to actively and mechanically clear circulating pro-inflammatory cytokines and vasoactive mediators from the bloodstream 29. This extracorporeal depuration can theoretically stabilize the hyper-permeable endothelium, potentially avoiding the necessity for full ECMO cannulation in borderline clinical cases 29.
Experimental Therapeutics and Small Molecule Antivirals
Currently, there are no fully approved therapeutic interventions or specific small-molecule antiviral drugs globally recognized for the treatment of HPS 31624. The overwhelming mortality rate, combined with the severe outbreak potential demonstrated by the Andes virus during the Hondius incident, has spurred massive biopharmaceutical investment into experimental therapeutics.
The pipeline for small-molecule antivirals active against negative-sense RNA viruses has historically been sparse, presenting a significant vulnerability in global pandemic preparedness 30. However, recent clinical efforts have pivoted aggressively toward repurposing broad-spectrum, late-stage clinical candidates for hantavirus infection.
Traws Pharma has recently accelerated the clinical advancement of two key small-molecule assets originally developed for other high-threat respiratory viruses, seeking to address the void in HPS treatments 10363738:
- Ratutrelvir: An investigational, ritonavir-independent oral small-molecule inhibitor specifically targeting the viral Main protease (Mpro or 3CL protease). While primarily advancing through Phase II clinical development for the treatment of COVID-19 - where it has demonstrated a highly favorable safety profile showing only 10% adverse events compared to 23.3% for Paxlovid, alongside an absence of clinical viral rebound - its mechanism of comprehensively inhibiting viral replication pathways is currently being evaluated in vitro for cross-applicability to severe HPS 103631.
- Tivoxavir Marboxil: A highly potent inhibitor targeting the cap-dependent endonuclease (CEN) function. Originally developed as a single-dose prophylactic and therapeutic agent for seasonal influenza and highly pathogenic H5N1 avian influenza, this compound physically disrupts the "cap-snatching" mechanism utilized by negative-sense RNA viruses to prime their mRNA transcription, thereby halting viral replication at a fundamental genomic level 103640.
Crucially, because the viral target proteins for these candidates (such as CEN and 3CL protease) lack structural homologues in human biology, the compounds theoretically offer extraordinarily high antiviral specificity coupled with an excellent safety profile 1017. Following the public health emergency declared around the MV Hondius outbreak, Traws Pharma announced urgent plans to rapidly screen these existing non-clinical and clinical-stage chemical libraries to identify the most optimal compounds for standalone or synergistic combination therapy against the Andes and Hantaan viruses 103832.
Other repurposed antivirals have yielded highly mixed and often disappointing results. Ribavirin, a synthetic guanosine analogue, has historically shown moderate clinical efficacy in reducing both morbidity and mortality in HFRS when administered in the early phases of the disease 3. However, multiple comprehensive clinical trials have conclusively failed to demonstrate any survival benefit for intravenous Ribavirin in the treatment of HPS. Consequently, its use is not currently recommended by clinical guidelines outside of strict, monitored research protocols 3824.
Similarly, drugs such as favipiravir and the kinase inhibitor vandetanib have shown some preliminary preclinical promise in cellular assays but critically lack sufficient human efficacy and safety data 3. Theoretical proposals advocating for the use of readily available agents like hydroxychloroquine - posited to act as a zinc ionophore and endosomal pH modulator to prevent viral uncoating - and ivermectin - suggested to act as an inhibitor of importin $\alpha/\beta$ nuclear transport utilized by the viral nucleocapsid protein - have been fiercely debated in the literature. While one isolated Syrian hamster model demonstrated a statistical survival benefit for prophylactic chloroquine administration, major international health authorities have largely dismissed these highly contested, repurposed agents for hantavirus management, emphasizing the critical need for advanced therapies with highly specific, proven antiviral mechanisms 42.
Immunomodulation and Monoclonal Antibodies
Given that the terminal pathogenesis of HPS is primarily driven by an excessive, dysregulated host inflammatory response rather than direct viral cytopathy, modulating the human immune system remains a paramount therapeutic strategy. The administration of systemic glucocorticoids has been widely debated in critical care literature; while frequently administered as a desperate, salvage therapy in scenarios of profound shock, large-scale clinical evidence supporting their routine use to halt or reverse HPS progression remains inconclusive and statistically weak 524.
More precise, targeted interventions aim to systematically dismantle the specific cytokine signaling cascades responsible for extreme vascular permeability. Following the discovery that IL-6 trans-signaling correlates directly with massive capillary leak and overall HPS severity, neutralizing monoclonal antibodies directed against the IL-6 receptor are currently under intense clinical investigation 171920.
Tocilizumab and sarilumab - both of which actively bind to the IL-6 receptor and sterically inhibit both the classical and trans-signaling pathways - are established, approved therapies in other hyperinflammatory states (most notably severe COVID-19 ARDS) and present a highly robust theoretical mechanism for reversing hantavirus-induced endothelial barrier dysfunction 171843. Furthermore, highly specific experimental agents like Olamkicept (an engineered fusion protein comprising sgp130 and the IgG1-Fc domain) selectively inhibit the pathogenic IL-6 trans-signaling pathway while leaving the vital, protective classical IL-6 signaling pathways functionally intact, making it an exceptionally compelling candidate for near-future HPS clinical trials 1719.
Advanced Polyclonal Immunotherapy
Passive immunotherapy, which seeks to provide immediate sterilizing immunity through the direct intravenous administration of high-titer neutralizing antibodies, represents one of the most clinically advanced therapeutic avenues. While convalescent plasma harvested from HPS survivors has historically been utilized in outbreaks, the inherent limitations in scalability, variable antibody titers, and lack of standardization remain prohibitive for global deployment 23.
The most technologically advanced targeted immunotherapy currently in clinical development is SAB-163, an investigational, highly potent pan-hantavirus human polyclonal immunoglobulin 244. SAB-163 is uniquely manufactured using transchromosomic bovines - cattle that have been genetically engineered to harbor large segments of human chromosomes, allowing their immune systems to synthesize fully human, rather than bovine, immunoglobulin G (IgG) in massive quantities 244.
These specialized bovines are hyperimmunized with complex, lipid nanoparticle-formulated DNA plasmids encoding the major envelope glycoproteins (Gn and Gc) of the four most prominent global hantaviruses: SNV, ANDV, HTNV, and PUUV 2. The resulting purified therapeutic product exhibits extraordinary neutralizing potency, consistently demonstrating 50% plaque reduction neutralization test (PRNT50) titers exceeding an unprecedented 200,000 2.
In highly rigorous, lethal Syrian hamster models of the disease, a bioavailable dosage of just 10 mg/kg of SAB-163 completely protected all subjects from lethal ANDV cardiopulmonary disease when administered either 1 day before exposure or as a post-exposure prophylactic up to 5 days after direct viral challenge 245. The pharmaceutical product is highly stable at standard 4°C refrigeration, highly specific with minimal off-target binding, and has successfully cleared Good Laboratory Practice (GLP) safety testing. SAB-163 is currently an Investigational New Drug (IND)-enabled asset actively advancing into Phase 1 human clinical trials, representing a massive leap forward in biodefense capability 244.
| Therapeutic Strategy | Leading Candidate(s) | Mechanism of Action | Current Clinical Status |
|---|---|---|---|
| Small Molecule Antiviral | Ratutrelvir | Ritonavir-independent inhibitor of the Main protease (3CL protease), halting viral replication. | Phase II (COVID-19); undergoing preclinical screening for HPS applicability. |
| Small Molecule Antiviral | Tivoxavir Marboxil | Inhibitor of cap-dependent endonuclease (CEN), disrupting viral mRNA transcription. | Phase I (Influenza); undergoing preclinical screening for HPS. |
| Polyclonal Immunotherapy | SAB-163 | Fully human IgG produced via transchromosomic bovines, providing immediate passive sterilizing immunity against major hantaviruses. | IND-enabled; advancing to Phase 1 clinical trials. |
| IL-6 Pathway Modulators | Tocilizumab, Sarilumab, Olamkicept | Monoclonal antibodies blocking IL-6 receptors, specifically targeting pathogenic IL-6 trans-signaling to halt capillary leak. | Approved for other hyperinflammatory syndromes; theoretical/investigational for HPS. |
| RNA Interference (RNAi) | Short interfering RNAs (siRNAs) | Engineered siRNAs targeting viral S, M, or L genomic segments to induce post-transcriptional silencing. | Preclinical; limited by complex in vivo pulmonary delivery requirements. |
Prophylactic Strategies and Vaccine Platforms
Preventing HPS through broad-based vaccination is an urgent, unresolved public health priority, particularly for deployed military personnel, agricultural workers, and residents of highly endemic regions in the Americas. Currently, absolutely no hantavirus vaccine has been approved by major regulatory bodies in North America or Europe. While an older, inactivated, rodent-brain-derived vaccine (Hantavax) is utilized regionally in Asia specifically for HFRS, its protective efficacy remains highly uncertain, and it offers no cross-protection against New World HPS strains 63347. The inherent difficulty of conducting massive, traditional Phase 3 efficacy trials for rare, highly sporadic diseases further complicates the regulatory approval pathway, heavily emphasizing the critical need for validated immunological surrogate endpoints to enable accelerated approval 44.
To overcome these hurdles, a highly diverse array of next-generation vaccine platforms, all primarily targeting the highly immunogenic Gn and Gc viral glycoproteins, is currently advancing through rigorous preclinical and early clinical stages.
| Vaccine Platform | Leading Developers | Technological Approach | Developmental Challenges & Status |
|---|---|---|---|
| DNA Vaccines | USAMRIID | Plasmid DNA expressing M-segment genes (Gn/Gc) delivered via needle-free electroporation to maximize cellular uptake. | Demonstrated safety in Phase 1/2 trials; challenges remain with multi-dose regimens and long-term durability. |
| mRNA Vaccines | Moderna, VIDO, EnsiliTech | mRNA encapsulated in Lipid Nanoparticles (LNPs) encoding glycoprotein precursors to stimulate robust germinal center responses. | Advanced preclinical; EnsiliTech utilizes "ensilication" (silica stabilization) to bypass severe cold-chain logistical barriers. |
| Protein Subunit | Novavax, VIDO | Highly purified, recombinant display of Gn/Gc spike complexes, combined with advanced saponin-based adjuvants (Matrix-M). | Preclinical; requires potent adjuvants to overcome the inherently poor immunogenicity of monomeric subunit proteins. |
| Recombinant Vectors | Academic Consortia | Attenuated Adenovirus or Vesicular Stomatitis Virus (VSV) backbones genetically engineered to express ANDV/SNV surface proteins. | Preclinical; provides robust T-cell stimulation and serves as a vital BSL-2 surrogate system for high-throughput virological assays. |
Nucleic Acid Vaccine Advancements
The United States Army Medical Research Institute of Infectious Diseases (USAMRIID) has pioneered the longitudinal development of advanced plasmid DNA vaccines expressing the M-segment genes of HTNV, PUUV, and ANDV 264748. Delivered almost exclusively via needle-free electroporation to physically force cellular uptake, these vaccines have proven highly safe in extensive Phase 1 and 2 open-label clinical studies, generating robust and measurable neutralizing antibody responses across multiple cohorts 6.
Simultaneously, utilizing the rapid adaptability of lipid nanoparticle (LNP) delivery systems, multiple global initiatives are aggressively exploring mRNA hantavirus vaccines. Moderna, leveraging its massive mRNA Access Program, has partnered with international academic centers, including Korea University, to develop highly specific mRNA constructs 484950. Other leading academic efforts, such as those at the University of Texas Medical Branch, are developing complex monocistronic linear mRNA platforms encoding the full ANDV glycoprotein precursor. These constructs have successfully demonstrated sterilizing immunity and robust germinal center B-cell responses in highly lethal hamster challenge models 4448.
A uniquely novel approach in the mRNA space is being spearheaded by EnsiliTech, which utilizes a process termed "ensilication" - physically wrapping the highly fragile active mRNA vaccine ingredients in protective, microscopic silica matrices. This groundbreaking physical stabilization allows the mRNA to remain completely viable at ambient temperatures, entirely overcoming the rigorous, expensive cold-chain logistics historically required for standard mRNA distribution, a critical feature for deployment in remote, rural endemic regions 4448.
Protein Subunit and Recombinant Viral Vectors
Protein subunit vaccines aim to safely display the exact architectural structure of the hantavirus Gn/Gc spike complexes directly to the immune system without the presence of any viral genetic material. The Vaccine and Infectious Disease Organization (VIDO) in Canada is actively developing multivalent protein subunit vaccines alongside their viral-vectored platforms 4834. Because the baseline immunogenicity of highly purified, isolated monomeric subunit proteins is notoriously low, these candidates absolutely require advanced chemical adjuvants or nanoparticle display technologies to be effective 3536. Adjuvants such as Matrix-M, a proprietary saponin-based platform heavily utilized by biopharmaceutical developers like Novavax, have been shown to significantly enhance the spatial presentation of subunit antigens, promoting exceptionally robust B-cell activation, follicular dendritic cell retention, and sustained, long-term immune memory 113755.
Finally, recombinant viral vectors, utilizing highly attenuated adenovirus or vesicular stomatitis virus (VSV) backbones engineered to safely express ANDV and SNV glycoproteins on their surface, are also in rapid development. These advanced vectors not only mimic a natural viral infection safely to stimulate powerful, long-lasting cellular T-cell responses but also provide a critically valuable biosafety level 2 (BSL-2) surrogate system. The use of these surrogate vectors allows researchers to perform high-throughput, accurate viral neutralization assays in standard laboratories, completely eliminating the extreme safety risks and intense logistical burdens of working with live, highly pathogenic wild-type hantaviruses in restrictive BSL-3 containment facilities 443538.
Conclusion
Severe Hantavirus Pulmonary Syndrome remains one of the most lethal and rapidly progressive infectious diseases recognized globally, a clinical reality sharply and tragically reinforced by the 2026 MV Hondius outbreak and the distinct, ongoing threat of person-to-person transmission associated with the Andes virus. In the complete absence of approved, targeted antiviral therapies, patient survival remains wholly dependent on aggressive, early critical care interventions and rigid infection control protocols. Hemodynamic management is an incredibly delicate balancing act requiring the implementation of transpulmonary thermodilution to precisely monitor extravascular lung water and vascular permeability, alongside the rapid, protocolized application of VA-ECMO before terminal cardiogenic shock irrevocably sets in.
However, the rapid acceleration of targeted therapeutics - ranging from small-molecule CEN and Mpro inhibitors (Ratutrelvir and Tivoxavir Marboxil) to cutting-edge transchromosomic polyclonal antibodies (SAB-163) and specific IL-6 trans-signaling modulators - offers substantial clinical promise. Moving forward, robust, unencumbered collaboration across international biopharmaceutical networks, military research institutes, and global public health agencies is imperative to bridge the vast gap between advanced preclinical scientific innovations and readily deployable, life-saving clinical countermeasures.