Self-optimization technology and health anxiety
The contemporary pursuit of health has increasingly transitioned from generalized wellness to highly quantified, continuous self-optimization. Driven by advanced digital health interventions, wearable activity trackers, and customized biohacking regimens, individuals now possess unprecedented access to their physiological and metabolic data. This paradigm, widely known as the Quantified Self movement, relies on the continuous collection and analysis of personal metrics - ranging from heart rate variability and sleep architecture to glucose levels and step counts - with the explicit goal of enhancing physical health and emotional well-being 112.
While data-driven health management provides tangible metrics that can empower individuals to make informed lifestyle modifications, an expanding body of clinical and sociological research indicates a concurrent rise in technology-induced health anxiety. When the interpretation of continuous biological data shifts from objective observation to an obsessive pursuit of perfection, self-optimization ceases to be a mechanism for wellness and instead becomes a catalyst for psychological distress. This phenomenon demonstrates how the tools designed to alleviate uncertainty regarding human health can inadvertently cultivate hypervigilance, generating distinct clinical manifestations such as orthosomnia, orthorexia nervosa, and profound digital dependency 134.
Foundational Concepts in Wellness and Pathology Models
To understand the threshold where health optimization becomes a psychological burden, it is necessary to examine the theoretical models of wellness and pathology. In mental health and clinical psychology, the wellness model and the pathology model represent two fundamentally different paradigms for evaluating human health 67.
The pathology paradigm is inherently medical; it is defined as the study of disease and is primarily concerned with identifying and correcting states of biological or psychological imbalance 67. Interventions under the pathology model - including pharmacological treatments, surgical procedures, and structured psychiatric therapies - aim to resolve specific, underlying medical dysfunctions that prevent an individual from functioning normally 67. In contrast, the wellness paradigm operates on a holistic continuum, defining health not merely as the absence of disease, but as a positive, proactive state of optimization across the body, mind, and spirit 67. Wellness approaches encourage clients to make continuous positive lifestyle choices to maximize their biological and psychological potential 67.
While both frameworks possess clinical merit, limitations emerge when they intersect without proper boundaries. It is increasingly difficult for healthcare providers to determine whether a patient requires wellness enhancement coaching or treatment for a distinct medical disorder 67. For example, iron deficiency affects approximately 10 million people in the United States, with 5 million suffering from iron deficiency anemia. Symptoms such as fatigue, generalized weakness, dizziness, and brittle nails are highly non-specific 5. Under a wellness paradigm, an individual might attempt to optimize their energy levels through extreme dietary changes, biohacking supplements, or sleep tracking. However, an underlying pathology - such as gastrointestinal bleeding or natural menstrual blood loss (which accounts for a loss of approximately 30 milligrams of iron per month) - requires targeted medical intervention rather than lifestyle optimization 5. When individuals attempt to resolve pathological symptoms exclusively through intensive wellness practices, the failure to achieve symptomatic relief often triggers severe health anxiety and the escalating pursuit of even more extreme optimization protocols.
Macroeconomic Expansion of the Global Wellness Industry
The infrastructure supporting self-optimization is sustained by a rapidly expanding, multi-trillion-dollar global wellness economy. Financial forecasting indicates that the broader wellness market, which had doubled since 2013, experienced a 7.9% growth from 2023 to reach a peak valuation of $6.8 trillion in 2024 67. Analysts project that the industry will expand at an accelerated compound annual growth rate (CAGR) of 7.6%, potentially approaching $9.8 trillion to $10 trillion by 2029 67.
This economic expansion is fueled by converging macroeconomic factors: an aging global population seeking extreme longevity, rampant rates of chronic and metabolic diseases, growing mental health awareness, and a broad cultural pivot toward preventative medicine 67. Wellness expenditures currently represent approximately 6.1% of global GDP and equate to 60% of all global health and medical expenditures (which total roughly $11.2 trillion) 67. The market encompasses 11 distinct sectors, all of which now exceed their pre-2019 values. The most rapid expansion is occurring in wellness real estate (19.5% CAGR) and mental wellness (12.4% CAGR) 67. Conversely, corporate workplace wellness was the only stagnant sector, shrinking by 1.5% between 2023 and 2024 67. Geographically, per capita wellness spending is highest in North America ($6,029) and Europe ($1,876), vastly outpacing regions like Latin America-Caribbean ($607), Asia ($471), and the Middle East-North Africa ($339) 67.
Biohacking Consumption and Institutional Equipment Integration
Within the macroeconomic framework of wellness, the specific sub-sector of biohacking - defined as the application of scientific technology, genetic profiling, and self-experimentation to optimize human biology - was valued at $24.5 billion in 2024. It is forecast to reach $111.3 billion by 2034, driven by a 16.5% CAGR 11. North America dominates this specific market, generating $9.9 billion in 2024 revenue, with the United States accounting for the vast majority 11. The hospital and clinical segment accounts for 36.5% of this market share, indicating a shift toward medicalized wellness spaces offering services like neurostimulation, continuous glucose monitoring (CGM), and real-time biomarker tracking 11.
Simultaneously, institutional wellness infrastructure has expanded to support corporate productivity goals. The global electric height-adjustable standing desk market was valued at $2.8 billion in 2024 and is projected to reach $5.4 billion by 2033 (7.6% CAGR) 8. Driven by corporate wellness initiatives, occupational safety regulations, and the integration of desk usage data with employee productivity metrics, dual-motor standing desks now command 55% of the market 8. Furthermore, corporate wellness tax incentives - estimated at $500 million to $1 billion annually in the United States - have dramatically boosted institutional procurement of premium commercial fitness equipment 910. Manufacturers such as Johnson Health Tech and Nautilus Inc. have heavily relied on these tax credits and government subsidies targeting obesity to bolster B2B sales 910. The commercial climbing gym sector is similarly expanding, projected to grow from $0.80 billion in 2024 to $1.20 billion by 2031 (5.97% CAGR), with major operators like Movement Climbing Yoga & Fitness, Vertical Endeavors, and Hangar 18 leveraging wellness grants and university partnerships to capture the health-conscious market 15.
Subscription Models and Consumer Costs
At the consumer level, the financial burden of maintaining a fully optimized lifestyle is substantial. The industry has increasingly transitioned from discrete product sales to recurring revenue subscription models. A standard high-level biohacking routine can cost between $1,000 and $5,000 per month, factoring in customized diagnostic testing, advanced hardware, and nutritional protocols 11.
| Biohacking Category | Specific Interventions and Devices | Estimated Cost Parameters | Primary Optimization Target |
|---|---|---|---|
| Consumer Wearables | Oura Ring, Whoop 4.0, Garmin Venu 3, RingConn, Biostrap Kairos | $200 - $500 initial hardware + $10 - $30 monthly software subscriptions | Heart rate variability (HRV), sleep architecture, blood oxygen saturation, continuous stress metrics 1213141516. |
| Clinical and Aesthetic Therapies | Intravenous NAD+ Therapy, GLP-1/GLP-2 regimens, Hyperbaric oxygen | $189 - $649+ monthly memberships depending on dosage and frequency | Cellular senescence, mitochondrial function, medical weight loss, resting metabolic rate 22. |
| Environmental and Recovery Tools | Sleep pod cooling systems, HigherDOSE Infrared sauna blankets, Verilux Light Therapy | $500 - $3,000+ per unit | Core temperature regulation, circadian rhythm alignment, muscular recovery optimization 141516. |
| Cognitive Enhancers | EEG headbands (Muse), Audio-Visual Entrainment (Narbis Illume), NeuroVizer | $200 - $350+ hardware | Electroencephalogram (EEG) feedback, brainwave entrainment, focus enhancement, mental clarity 121323. |
| Nutritional Supplements | Customized nootropics, Rootine, AG1, Dihexa peptide, Krill Oil | $50 - $150+ monthly subscriptions | Micronutrient optimization, gut microbiome homeostasis, anti-inflammation, cognitive support 1115162317. |
This financial structure transforms health from an intrinsic biological state into a continuous, monetized service. The economic imperative to engage with these platforms frequently correlates with a perceived loss of autonomy, as users increasingly rely on external, subscription-based data to validate their internal physical conditions 18. When significant capital is invested in health optimization, the psychological pressure to achieve a measurable return on investment intensifies, laying the groundwork for severe tracking anxiety.
Psychological Frameworks of Data-Driven Health Anxiety
The transition from healthy monitoring to clinical anxiety involves complex cognitive and physiological mechanisms. The continuous influx of highly quantified data from fitness trackers and health applications fundamentally alters how individuals perceive their bodies, driven by cognitive biases, altered interoception, and persuasive digital interface designs.
The Illusion of Control in Fitness Tracking
The "illusion of control," a cognitive bias first formally described by psychologist Ellen Langer in 1975, represents the human tendency to overestimate one's capacity to influence outcomes that are demonstrably determined by complex variables or random chance 1920. In the context of the Quantified Self, this illusion is powerfully catalyzed by the sheer volume and high frequency of data provided by wearable technology 2021.
Experimental psychology demonstrates that environments featuring a high probability of action (P(A) - e.g., frequent user input, logging meals, or checking a device) combined with a high probability of outcome occurrence (P(O) - e.g., frequent biometric data updates) reliably generate an illusion of control 2223. Wearable activity trackers (WATs) perfectly replicate these conditions. Users begin to perceive health as a deterministic, linear input-output system, believing that strict adherence to specific behavioral inputs will guarantee precise physiological outputs 12123. This phenomenon is further elucidated by the concept of depressive realism; studies show that depressed individuals often have a highly accurate perception of their lack of control, whereas healthy individuals rely on positive illusions of control to maintain baseline optimism and motivation 1922.
However, the extreme illusion of control cultivated by continuous bio-tracking eventually encounters the unpredictable reality of biological systems. When a user strictly follows their optimized protocol but fails to achieve the predicted metric - for example, experiencing a poor sleep score despite perfect sleep hygiene, or facing an illness despite strict nutritional compliance - the resulting cognitive dissonance leads to severe stress 124. In fitness tracking research, this is compounded by Activity Adequacy Mindsets (AAMs). Research indicates that mindsets about the adequacy of one's physical activity shape actual health outcomes. Individuals receiving artificially deflated step counts from manipulated wearable devices report feeling less healthy and experiencing higher anxiety, despite their objective physical activity remaining identical 25. Consequently, users often respond to unmet goals or negative algorithmic feedback by engaging in excessive, punitive exercise or extreme dieting, turning motivation into behavioral obsession 24.
Informational Manipulation and the Theory of Planned Behavior
The digital platforms that support the wellness industry frequently employ psychological manipulation mechanisms to sustain user engagement and drive product consumption. The Theory of Planned Behavior (TPB) suggests that human behavior is driven by intentions, which are formed by attitudes, subjective norms, and perceived behavioral control 26.
In the realm of fitness and supplement marketing, digital interfaces exploit heuristic trust and cognitive shortcuts rather than promoting careful appraisal of scientific evidence. Simulated social-media environments manipulating authority endorsement, scarcity cues, and conformity cues effectively suppress a consumer's risk perception regarding unregulated supplements, thereby increasing purchase intent 26. When individuals consume wellness media heavily reliant on persuasive cue structures, their baseline risk perception is gradually normalized. They become increasingly susceptible to misleading claims and more likely to invest in aggressive biohacking protocols that may pose genuine public health risks 26.
Interoceptive Hypervigilance and the Domain Loop Model
The psychological burden of continuous tracking is further explained through models of interoceptive hypervigilance and the mind-body feedback loop. Interoception is the nervous system's perception of sensations occurring within the body (e.g., heart rate, gut motility, muscle tension) 3435. In individuals with health anxiety, the brain develops hypervigilance toward standard physiological fluctuations. Normal variations - such as a skipped heartbeat, a minor digestive shift, or momentary fatigue - are amplified and misinterpreted as indicators of severe pathology 343637.
The Domain Loop Model posits that subjective experience is constructed through the continuous interaction of three distinct domains: the physical body (interoceptive), the external environment (exteroceptive), and the cognitive "narrator" that integrates sensory input to assign meaning 35. When an individual relies heavily on technological devices to mediate this loop, standard bodily cues are often preempted by digital data. Biological sensitivities, such as joint hypermobility or intestinal permeability ("leaky gut"), can trigger immune inflammation and oxidative stress, which activates the hypothalamic-pituitary-adrenal (HPA) axis 35. This central stress response system elevates cortisol levels, placing the individual in a persistent "fight or flight" state.
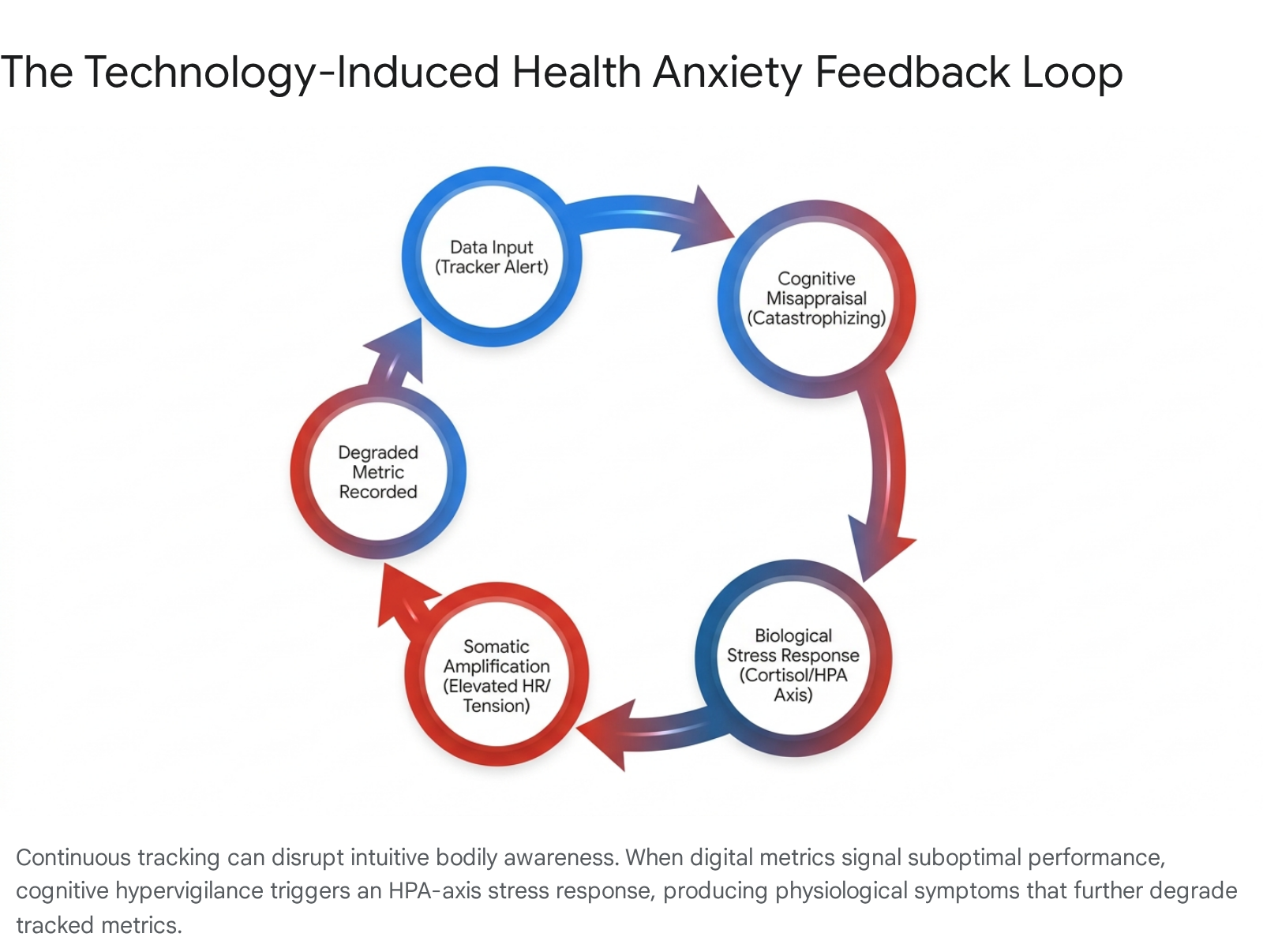
When the narrator domain misinterprets these signals - for instance, assuming a poor recovery metric on a smartwatch means an impending health crisis - the cognitive process of catastrophizing begins 3536. The mind jumps to worst-case scenarios, which in turn triggers a secondary, actual physiological stress response. Heart rate quickens, digestion halts, and muscles tense, creating the exact physical symptoms the user initially feared 3637. This creates a powerful, self-perpetuating positive feedback loop: technology-induced anxiety produces somatic symptoms, the technology records these symptoms as degraded physiological performance, and the degraded data further escalates the user's cognitive distress 34363727.
Clinical psychologists attempt to break this cycle using cognitive behavioral therapy (CBT) and specific interventions such as the 60-second "STOP-SCAN-SHIFT" protocol, which interrupts spiraling catastrophic thoughts in real-time before the HPA axis is fully activated 36.
Clinical Manifestations of Metric Fixation
The integration of intense performance tracking into daily routines has given rise to distinct behavioral disorders characterized by rigidity, social isolation, and pathological obsession. Chief among these phenomena are orthosomnia, related to the quantification of rest, and orthorexia nervosa, related to dietary purity.
Clinical Characteristics of Orthosomnia
Orthosomnia is a newly classified behavioral pattern defined by an obsessive pursuit of optimal sleep, driven explicitly by the data generated from wearable sleep trackers 42840. While not currently recognized as an independent diagnosis in the DSM-5, clinical researchers defined the term in 2017 after observing an influx of patients seeking treatment at sleep clinics for self-diagnosed sleep disorders based entirely on commercial wearable data, rather than subjective feelings of daytime fatigue 3402930.
The etiology of orthosomnia is rooted in a fundamental distrust of one's own interoceptive cues in favor of algorithmic outputs. Patients exhibiting orthosomnia often spend excessive time in bed attempting to maximize their "sleep score," a counterproductive practice that contradicts established sleep hygiene protocols and frequently exacerbates insomnia 40. In a relentless pursuit of a mathematically perfect sleep architecture, users experience heightened pre-sleep performance anxiety, increasing sympathetic nervous system arousal and delaying sleep onset 4029.
Commercial sleep trackers rely on surrogate measures such as actigraphy (movement) and photoplethysmography (heart rate) to estimate sleep stages. These consumer devices have demonstrated poor accuracy in detecting wake periods after sleep onset and cannot reliably discriminate between complex sleep stages compared to the clinical gold standard of overnight polysomnography 34029. Consequently, individuals with orthosomnia endure significant clinical distress over inherently imprecise consumer data.
Diagnostic screening tools, such as the newly developed Anxiety and Preoccupation about Sleep Questionnaire (APSQ) and the Athens Insomnia Scale (AIS), help quantify this condition. Epidemiological algorithms suggest that the prevalence of "full-blown" orthosomnia in the general population sits conservatively at around 3.0%, with higher susceptibility among adolescents and young adults (median age 19) due to their high baseline engagement with mobile technology and nomophobia (the fear of being without a mobile device) 3043.
| Domain | Healthy Sleep Hygiene | Clinical Orthosomnia |
|---|---|---|
| Primary Metric | Subjective feeling of physical restfulness and mental clarity upon waking. | Quantitative sleep score, precise stage percentages, or total duration algorithmically generated. |
| Time in Bed | Leaving the bed if unable to sleep after 20 minutes; associating the bed solely with rest. | Remaining in bed while fully awake for extended periods to accumulate total recorded "time in bed" metrics 440. |
| Pre-Sleep State | Relaxation, natural transition into sleep without conscious cognitive pressure. | High performance anxiety regarding the impending physiological measurement, leading to sympathetic arousal 4029. |
| Response to Data | Utilizing broad trends over weeks to adjust generalized habits (e.g., caffeine timing). | Obsessive daily analysis; daily mood and self-worth dictated entirely by the tracker's output 4029. |
Clinical Characteristics of Orthorexia Nervosa
Parallel to the obsession with sleep metrics is orthorexia nervosa (OrNe), a term coined in 1997 by physician Dr. Steven Bratman to describe a pathological obsession with consuming foods perceived to be healthy, pure, or clean 443132. Unlike anorexia nervosa or bulimia nervosa, which are primarily driven by body shape dissatisfaction and caloric restriction to achieve weight loss, the central motivation in OrNe is dietary purity and strict adherence to self-imposed health rules 32474833. Furthermore, it differs from Avoidant Restrictive Food Intake Disorder (ARFID), which generally stems from sensory aversions or fear of choking 345135.
While orthorexia shares common phenotypic traits with other eating disorders - such as perfectionism, high anxiety, achievement orientation, and obsessive-compulsive tendencies - its clinical presentation is uniquely tied to the modern wellness culture's moralization of food 313536. Individuals with OrNe frequently eliminate entire macronutrient categories or food groups (e.g., all dairy, gluten, grains, processed ingredients, non-organic items) based on unsubstantiated fears of toxicity or systemic disease 3247. Over time, the diet becomes so restrictive that it results in severe medical complications. Patients may present with malnutrition, severe osteopenia (bone density loss), anemia, pancytopenia (low levels of all blood cells), hyponatremia (low sodium), and bradycardia (slow heartbeat) 483351. Paradoxically, the extreme restriction can also lead to intense cravings, resulting in binge eating episodes followed by severe self-punishment and shame 33.
Current psychiatric research relies on measurement tools such as the Eating Habits Questionnaire (EHQ), the Dusseldorf Orthorexia Scale (DOS), and the ORTO-15 to assess the severity of these symptoms 3451. A primary focus of contemporary research is the necessity of distinguishing OrNe from "Healthy Orthorexia" (HeOr), which represents a non-pathological, flexible interest in nutritious eating and health-promoting behaviors 313437.
| Clinical Marker | Healthy Orthorexia (HeOr) | Orthorexia Nervosa (OrNe) |
|---|---|---|
| Cognitive Flexibility | High; minor deviations from dietary preferences or eating "unhealthy" food cause no significant distress. | Extremely low; breaking dietary rules triggers severe anxiety, guilt, panic, and subsequent self-punishment 324833. |
| Social Functioning | Able to participate in social dining, restaurants, and family meals despite specific dietary preferences. | Severe social isolation; frequently refuses to eat in social settings where food sourcing and preparation techniques cannot be strictly controlled 3248. |
| Core Motivation | General vitality, energy, and an appreciation for the natural content of food 3137. | Intense fear of illness, disease, or internal contamination; health equates to moral superiority 324748. |
| Nutritional Outcome | Balanced macronutrient intake resulting in sustained physical health. | Often leads to malnutrition, unintentional weight loss, and severe medical complications due to extreme restriction 4833. |
When controlling for HeOr, studies demonstrate that OrNe is strongly correlated with clinical impairment, elevated eating disorder risk, and health anxiety 3437. Despite the obsession with "healthy" eating, individuals with high OrNe scores often exhibit relatively unhealthier eating patterns due to the extreme elimination of necessary nutrients, proving that the fixation on purity actively overshadows balanced physiological needs 34.
Sociocultural Contexts of Wellness Anxiety
While the biohacking and quantified self movements are global phenomena, the specific manifestations of self-optimization anxiety are heavily influenced by regional socioeconomic structures and cultural paradigms. Sociological data from East Asia - specifically China, Japan, and South Korea - reveals how structural pressures are internalized as mandates for personal optimization.
Involution and Digital Productivity in China
In contemporary China, the concept of self-optimization is deeply intertwined with neijuan (involution), a sociological term describing an environment of zero-sum, hyper-intense competition that yields diminishing returns 383940. Initially observed in the extreme academic pressures placed on students competing for university placements, involution has permeated the urban workforce, characterized by grueling "996" work schedules (working from 9 a.m. to 9 p.m., 6 days a week) 4041. This intense pressure has sparked counter-movements among millennials and Gen Z, such as tangping ("lying flat," choosing to opt out of the hustle culture) and runxue (the philosophy of emigrating to escape the system) 39.
In response to systemic burnout, the Chinese urban middle class has increasingly turned to digital health technologies - such as smartwatches, sleep trackers, and fitness applications - to manage their health. However, rather than providing an escape from pressure, self-care has been co-opted by the logic of involution. Workers utilize health-tech to manage their bodies purely to sustain productivity and survive the relentless workplace competition 42. Health is viewed as a fragile asset requiring strict, data-driven discipline. Studies reveal that passive involution (being forced to compete) has a significant positive predictive effect on clinical anxiety among students and workers 43. The pursuit of wellness becomes yet another domain of performance anxiety, where individuals must demonstrate to themselves and their peers that they possess the physical resilience necessary to navigate structural exhaustion 4243. The government's push for "self-initiated and self-discipline behaviors" under the Health China 2030 strategic plan further internalizes broad public health responsibilities onto the already exhausted individual 42.
Overwork Culture and Institutional Stress Management in Japan
In Japan, the intersection of wellness and anxiety is shaped by the legacy of karoshi (death by overwork) and the government's subsequent regulatory responses. Working more than 60 hours per week significantly increases the risk of karoshi for men, while the threshold for women is approximately 45 hours (due to the compounding burden of domestic labor) 41. In 2023, 883 workers were officially diagnosed with occupational stress-related mental disorders, and workers' compensation cases for mental health remain exceedingly high, with 1,055 cases reported in FY2024 44. Furthermore, depression and anxiety account for 42.0% of the entire disorder segment in the Japanese mental health market, which was valued at $27.5 billion in 2025 44.
To address this crisis, the Japanese government instituted the mandatory annual Stress Check Program in 2015 for all companies with 50 or more employees 4445. While these measures successfully elevated the integration of wellness technologies, corporate fitness subsidies, and Employee Assistance Programs (EAPs) into the workplace, they have also generated secondary anxieties 944. The cultural stigma surrounding formal psychiatric treatment and perceived emotional weakness remains a massive barrier; consequently, employees are pressured to utilize digital self-tracking tools to monitor their own stress levels 4446. The institutional demand for continuous self-disclosure forces individuals to quantify their psychological states for their employers. This dynamic often causes employees to manage their reported data defensively - such as deliberately marking false answers on stress checks to avoid workplace reprisal - rather than seeking genuine, out-of-pocket clinical intervention 4446.
Aesthetic Perfectionism and Psychological Distress in South Korea
South Korea presents a unique manifestation of self-optimization anxiety, driven by extreme aesthetic standards, the pervasive influence of social media, and the expectations of K-culture. The pursuit of "glass skin" (flawless, poreless complexions) and the cultural trend of preparing for highly stylized "body profile" photoshoots dictate rigorous dietary and physical regimens 4748.
This pursuit of flawlessness has exacted a severe psychological toll on the younger demographic. The number of Korean children and adolescents receiving clinical treatment for mental health conditions surged by 76.6% between 2020 and 2024, surpassing 350,337 cases 4950. Among children under 12, Attention Deficit Hyperactivity Disorder (ADHD) is the leading diagnosis, while clinical depression is the most common mental illness among teenagers 49. Sociologists note that physical appearance in South Korea operates as a strict proxy for social status, academic success, and overall self-worth 51. The discrepancy between the heavily filtered, digitally perfected images online and biological reality fosters intense body dissatisfaction, social withdrawal, and high rates of restrictive eating disorders, particularly anorexia nervosa, among adolescents 4748. Furthermore, South Korea consistently exhibits one of the highest suicide rates among developed nations in the OECD, underscoring the lethal consequences of unmitigated societal pressure 51.
Efficacy and Risks of Digital Health Interventions
As the mental health burden of modern life increases globally, the technological sector has responded with Artificial Intelligence (AI) health coaches, conversational agents, and digital therapeutic applications. Leveraging cognitive behavioral therapy (CBT) frameworks, these Digital Health Interventions (DHIs) aim to democratize access to mental health support, bypassing long clinical wait times and the high costs of traditional therapy 6970.
Artificial Intelligence and Hybrid Coaching Models
Recent clinical trials demonstrate that generative AI chatbots and AI-assisted human coaching platforms can effectively reduce symptoms of mild-to-moderate depression and anxiety over short-term periods (e.g., 4 to 8 weeks) 695253. Natural language processing algorithms allow these tools to provide real-time, personalized interventions, tracking user sentiment and reinforcing behavioral skills 52. In corporate environments, platforms like Sibly - which pairs AI assistance with human coaching - achieved a median response time of 132 seconds, resulting in a 79% relative reduction in severe distress reporting and an 18% improvement in self-reported workplace productivity 52. Similarly, the Limbic app, which utilizes clinical AI for guided CBT sessions, demonstrated a 2.4 times higher usage frequency compared to standard control groups, leading to significant reductions in Generalized Anxiety Disorder (GAD-7) and Patient Health Questionnaire (PHQ-9) scores 70.
These systems operate on the principle of continuous feedback loops. By providing immediate, targeted psychological reinforcement, they can theoretically bypass the cognitive biases that fuel health anxiety, actively challenging catastrophic thinking through structured logic trees 277073. Furthermore, research tracking the biological markers of anxiety - such as salivary alpha-amylase (sAA), serum cortisol, lysozyme, and brain-derived neurotrophic factor (BDNF) - suggests that future AI interventions could potentially be paired with real-time biometric sensors to automatically detect and de-escalate panic attacks before the user even registers subjective distress 545556.
Autonomy Reduction and Behavioral Dependency
Despite the promising data on short-term symptom reduction, the widespread deployment of DHIs carries inherent risks regarding long-term digital dependency and the dilution of genuine therapeutic alliances. Health behavior scientists caution that maintaining long-term engagement with fully automated, self-guided DHIs is notoriously difficult; current meta-analyses reveal a pooled estimated dropout rate of 43% across DHI platforms, as users ultimately find the automated responses shallow and transactional 5357.
More critically, reliance on AI algorithms and constant biometric nudges to regulate emotional distress can impede the development of intrinsic psychological resilience 18. The phenomenon of "technostress" - the negative psychological effect of being overwhelmed by continuous technology notifications, information overload, and complex software demands - can actively worsen sleep, induce tension headaches, and spike cortisol levels, negating the very benefits the apps are designed to provide 185859. Continuous exposure to self-quantification data emphasizes algorithmic outcomes over personal experiences, fostering a loss of personal autonomy. Studies indicate that persistent feedback through wearables actually reduces users' belief in their own free will and autonomy, as they become dependent on external metrics to validate their internal emotional states 18.
Psychotherapists argue that while AI can deliver skill-based interventions, it fundamentally cannot replicate the complex human attunement, ethical containment, and shared vulnerability required to navigate deep-seated psychological trauma 69. The persistent outsourcing of emotional regulation to an application may trap users in a perpetual loop of seeking external, digitized reassurance, thereby reinforcing the core mechanics of health anxiety 18695960.
To navigate the "hype cycle" of digital health research - from the peak of inflated expectations to the slope of enlightenment - developers and clinicians must establish clear boundaries 60. Future digital wellness paradigms must prioritize cognitive flexibility and intuitive bodily trust over absolute metric adherence, ensuring that technology serves as a temporary scaffolding for mental health rather than a permanent replacement for human resilience and self-awareness.