Scientific research on high-intensity interval training
High-intensity interval training constitutes a physiological exercise modality characterized by brief, intermittent bursts of vigorous activity - typically performed at 85% to 100% of peak oxygen uptake or maximal heart rate - interspersed with periods of active or passive recovery 12. Over the past decade, culminating in updated clinical guidelines published between 2024 and 2026, the volume of empirical data surrounding this modality has transitioned it from a specialized athletic conditioning tool into a frontline therapeutic intervention for cardiovascular disease, metabolic syndrome, oncology rehabilitation, and age-related physiological decline 3456.
The scientific consensus indicates that interval training yields profound physiological adaptations, frequently matching or exceeding those of moderate-intensity continuous training despite requiring a significantly lower volume of total exercise time 7. However, the exact physiological mechanisms, optimal dosing protocols, and long-term mortality benefits remain subjects of intense clinical study. By evaluating the cellular signaling pathways, macroscopic cardiovascular changes, and long-term epidemiological data, a nuanced understanding emerges regarding where high-intensity interval training is most efficacious and where its biological limitations lie.
Cellular and Molecular Adaptations
The foundational appeal of high-intensity interval training lies in its capacity to force rapid, systemic physiological adaptations under conditions of severe metabolic stress. The human body responds to the high mechanical and metabolic demands of near-maximal exertion by upregulating specific gene expressions, altering mitochondrial density, and remodeling vascular architecture.
Mitochondrial Biogenesis and Respiratory Function
Exercise drives adaptations in skeletal muscle mitochondrial respiratory function, but the nature of the exercise stimulus dictates the specific magnitude and type of cellular adaptation. High-intensity interval training specifically targets Type 2A muscle fibers, which are uniquely positioned to offer enhanced anaerobic power for explosive movements while simultaneously improving aerobic capacity for sustained performance 7.
Research comparing high-intensity protocols against moderate-intensity continuous training demonstrates that interval training drives a greater increase in specific markers of mitochondrial content and oxidative capacity 789. In muscle biopsies of the vastus lateralis following six-week training interventions, individuals engaged in high-intensity interval training exhibited citrate synthase activity levels of 189.7 μmol/min/mg protein, compared to 166.3 μmol/min/mg protein in cohorts performing moderate-intensity continuous training 78. Complex I activity - a crucial component of the electron transport chain - also increases following interval training, though statistical significance comparing the two modalities often remains marginal 78.
The protein content of key regulatory signaling molecules reveals stark modality-specific responses. Markers including peroxisome proliferator-activated receptor γ coactivator (PGC)-1α, p53, and plant homeodomain finger-containing protein 20 (PHF20) increase significantly (by 60% to 90%) following sprint interval training, whereas these precise markers remain largely unchanged in volume-matched traditional endurance training 101211.
The macroscopic architecture of the mitochondrial network is also altered by exercise intensity. While moderate-intensity training tends to reorganize sparse, punctate mitochondria into a grid-like structure with robust longitudinal connections, high-intensity interval training drives a predominantly longitudinally oriented network 9. Furthermore, interval training substantially increases the mRNA expression of mitochondrial fusion proteins, specifically MFN1, MFN2, and OPA1, while simultaneously decreasing fission protein expression. This indicates an optimization of the mitochondrial reticulum that facilitates highly efficient energy transfer during periods of severe metabolic demand 789.
Epigenetic Markers and Aging Reversal
Beyond acute metabolic changes, high-intensity interval training exerts measurable effects on epigenetic markers associated with biological aging. It modulates the epigenetic clock by influencing DNA methylation, telomere length, and transcriptomic age.
Clinical observations demonstrate that interval training increases telomere length and elevates telomerase activity by a factor of two to three, improvements that are not universally mirrored in resistance training 12. Twelve-week interventions have been shown to significantly restore DNA methylation in the gene encoding the mitochondrial adaptor p66Shc; methylating this specific protein inhibits its ability to trigger mitochondrial death and systemic oxidative stress 12. In populations with heart failure, interval training is associated with a reduction in cardiac fibrosis, which is linked to the hypermethylation of the ACADVL gene 12.
At the transcriptomic level, rigorous interval protocols have reduced transcriptomic age by 3.59 years and improved transcriptomic age acceleration by 7.04 years in specific adult cohorts 12. The modality also clears neurotoxic proteins, such as β-amyloid and tau, by regulating astrocyte polarization, suggesting potential neuroprotective phenotypes 12. Alternative molecular markers, such as the down-regulation of miR-206 (a marker of cellular apoptosis) and the up-regulation of HSP60 (heat shock protein 60), are more effectively stimulated by high-intensity rather than moderate-intensity training, correlating with improved overall cardiac function 12.
Cardiovascular and Hemodynamic Responses
The circulatory system is highly sensitive to the mechanical and shear stress induced by high-intensity exercise. Sedentary behavior diminishes arterial elasticity and autonomic regulation, leading to elevated pulse wave velocity, which serves as a gold standard metric for assessing arterial stiffness 513. An increase of 1 m/s in pulse wave velocity is independently associated with a 14% to 15% elevated risk of cardiovascular events and all-cause mortality 1314.
Arterial Stiffness and Endothelial Function
Systematic reviews analyzing populations at high risk for cardiovascular disease reveal that high-intensity interval training significantly reduces pulse wave velocity by a weighted mean difference of 0.62 m/s 1314. Subgroup analyses indicate that these vascular benefits are optimized when the protocol is performed two to three times per week with a total session duration capped at 40 minutes 1314.
Endothelial function, objectively measured via flow-mediated dilation, shows marked improvement following interval training. Interventions lasting 12 weeks have demonstrated increases in flow-mediated dilation from 3.45% to 7.39% in clinical cohorts, establishing a statistical superiority over moderate continuous training, which improved from 3.83% to 4.81% in matched demographics 5. The mechanism underlying this enhancement is related to the intense, pulsatile blood flow generated during maximal exertion bouts. This mechanical force aggressively stimulates the vascular endothelium to synthesize and release nitric oxide, thereby promoting acute vasodilation and long-term vascular remodeling 5. Heterogeneity in flow-mediated dilation outcomes is highly dependent on age; studies with populations under 30 years old show substantial variability depending on whether short-sprint interval training or aerobic interval training was prescribed 5.
Blood Pressure and Cardiac Output
Reductions in arterial stiffness cascade into tangible improvements in resting hemodynamics. Meta-analytic data verifies significant reductions in resting systolic blood pressure, ranging between 5.02 and 5.43 mmHg, and diastolic blood pressure, ranging between 2.43 and 2.96 mmHg, following structured interval training 51314.
Central cardiovascular adaptations also manifest as increased maximal stroke volume and enhanced cardiac output 715. High-intensity protocols force the myocardium to adapt to high venous return and elevated contractility demands, expanding the heart's stroke volume capacity more effectively in certain populations than lower intensities of continuous exercise 15. This central adaptation is a primary driver behind the significant improvements in maximal oxygen uptake universally observed following interval interventions 7.
Comparative Efficacy Across Clinical Populations
As interval training methodologies have matured, researchers have systematically applied these protocols to varied demographic and clinical cohorts, isolating precisely how high-intensity stress rehabilitates specific pathophysiological states.
Coronary Artery Disease and Heart Failure
In populations diagnosed with coronary artery disease and heart failure, maximizing peak oxygen uptake (VO2peak) is a critical clinical objective, as VO2peak is an independent predictor of all-cause mortality and long-term prognosis 16. Systematic reviews analyzing randomized controlled trials encompassing over 1,100 patients demonstrate that high-intensity interval training yields superior cardiorespiratory enhancements compared to moderate-intensity training 1617.
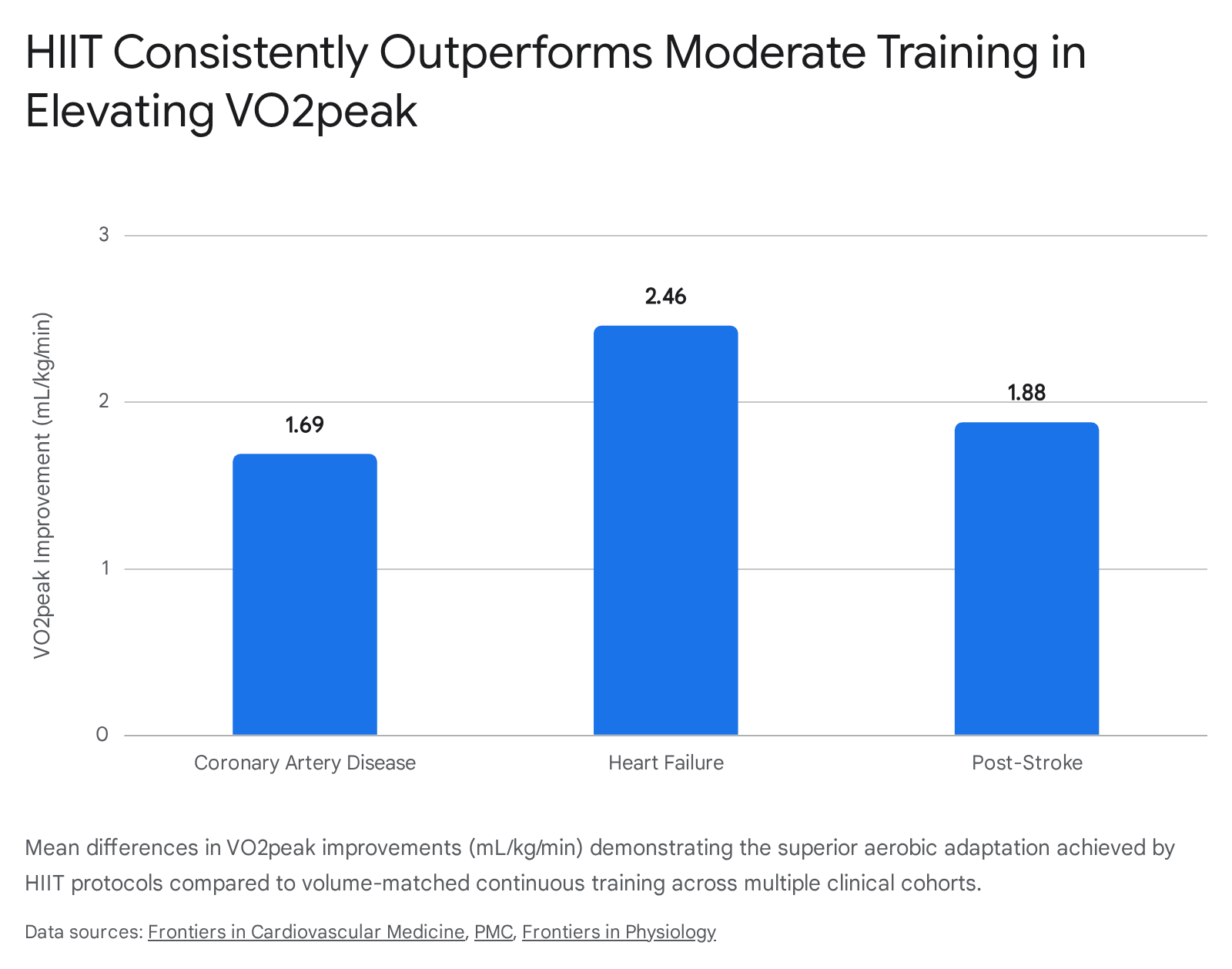
Specifically, interval training has been shown to improve VO2peak in patients with coronary artery disease by an additional 1.69 mL/kg/min compared to moderate continuous training 16. In patients with heart failure, the improvements are even more pronounced, with interval training driving an increase in VO2peak of 2.46 mL/kg/min over continuous baseline protocols 16. Furthermore, cardiac function metrics, such as left ventricular ejection fraction, demonstrate a significant mean difference of 2.69% in favor of interval training 18. Despite the high relative intensity of the exercise, clinical safety profiles reveal that the overall risk of acute cardiovascular events remains low and statistically comparable between interval and continuous training groups, provided the protocols are rigorously screened and supervised 119.
Post-Stroke Rehabilitation
A parallel dynamic is observed in post-stroke rehabilitation, though with crucial limitations regarding neuromuscular translation. Meta-analytic data encompassing 371 stroke patients indicates that high-intensity interval training drives a significantly greater improvement in VO2peak (mean difference of 1.88 mL/kg/min) and oxygen consumption at the first ventilatory threshold (mean difference of 2.20 mL/kg/min) 20.
However, the translation of this enhanced central aerobic capacity into functional mobility performance is constrained. Variables such as the 6-Minute Walk Test, 10-meter gait speed, and the Berg Balance Score showed no meaningful clinical divergence from moderate continuous training 20. This suggests that while interval training effectively rehabilitates the central cardiovascular engine post-stroke, complementary targeted neuromuscular and proprioceptive therapies are required to address peripheral motor deficits.
Oncology Rehabilitation
For cancer survivors, the primary barriers to physical rehabilitation are treatment-induced systemic fatigue and time constraints 21. A comprehensive meta-analysis of randomized controlled trials involving survivors of breast, colorectal, and mixed cancers evaluated the comparative efficacy of interval versus continuous training 2122. Interval training was significantly more effective at improving peak oxygen uptake, yielding a standardized mean difference of 0.53 over moderate-intensity training 2122.
Despite improvements in cardiorespiratory fitness, functional outcomes related to raw mobility - such as the Sit-to-Stand test - showed no statistically significant differences between the modalities 21. Similarly, metrics of overall body composition, including lean body mass, waist circumference, body mass index, and total fat mass, were identically impacted by both training types 2122. A distinct clinical advantage of interval training in oncology populations, however, is adherence. The abbreviated duration of the sessions effectively mitigates "lack of time" as a barrier, with clinical trials noting intervention completion rates of up to 100% in interval groups compared to 91% in continuous training groups, driven largely by higher self-reported enjoyment 21.
Metabolic Syndrome and Polycystic Ovary Syndrome
Polycystic ovary syndrome (PCOS) and metabolic syndrome represent systemic disorders characterized by insulin resistance, elevated visceral adiposity, and impaired skeletal muscle energy metabolism 23. Extensive clinical research, notably led by the late Professor Nigel Stepto at Victoria University, demonstrated that practical, supervised interval training protocols effectively combat these metabolic dysfunctions 2425.
Among women with PCOS, high-intensity exercise has been shown to reduce the odds ratio of metabolic syndrome by 22% 25. Vigorous activity produces superior reductions in the Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) and body mass index, alongside marked improvements in health-related quality of life and reductions in depressive symptoms 2325. Similar metabolic benefits are observed in the reduction of hepatic steatosis; both interval and continuous training elicit comparable, moderate reductions in liver fat content (reductions of 2.85% and 3.14%, respectively) without requiring extensive exercise duration 26. Furthermore, lipid profiles in middle-aged and elderly populations improve significantly, with interval training driving standardized mean differences of 0.41 in high-density lipoprotein cholesterol (HDL-C) and -0.68 in triglyceride reductions 27.
The Intensity Spectrum and Modality Variations
The intense debate surrounding cardiovascular training often frames high-intensity and moderate-intensity modalities in strict opposition. However, systematic comparisons reveal clear areas of superiority, equivalence, and divergence depending on the specific physiological target and metabolic pathway engaged. Data highlights that these modalities trigger fundamentally different cellular signaling pathways, validating the clinical consensus that they are complementary rather than mutually exclusive 7282932.
High-Intensity Interval Training Versus Zone 2 Continuous Training
To fully contextualize the physiological impact of high-intensity training, it must be evaluated alongside moderate-intensity protocols, specifically "Zone 2" training. Zone 2 cardiovascular training occurs just below the first lactate threshold (approximately 60% to 70% of maximal heart rate), a state where the body relies on aerobic metabolism and primarily oxidizes fat for energy 282930.
High-intensity intervals rapidly activate AMPK pathways to improve mitochondrial efficiency and VO2max primarily in Type 2A muscle fibers 732. Conversely, sustained Zone 2 training predominantly activates Type 1 slow-twitch fibers and is recognized as the primary driver of mitochondrial biogenesis - increasing the absolute volume and density of the organelles, rather than just their enzymatic efficiency 3234.
A persistent misconception surrounds the application of these modalities for lipid reduction. While Zone 2 maintains a high contribution of fat to total energy expenditure (40% to 60%), high-intensity exertion rapidly suppresses fat oxidation (dropping to 10% to 20%) in favor of anaerobic glycolysis and carbohydrate utilization 35. Yet, meta-analyses explicitly demonstrate that when total energy expenditure is strictly matched between groups, both interval training and continuous cardiovascular exercise yield virtually identical reductions in total body fat 32303536. Therefore, interval training is not a uniquely powerful fat-burning mechanism inherently, but rather a highly time-efficient method for generating the necessary total caloric expenditure and metabolic disturbance required to drive lipolysis post-exercise 3036.
| Clinical / Physiological Target | High-Intensity Interval Training | Zone 2 / Moderate Continuous Training |
|---|---|---|
| Primary Energy Substrate | Carbohydrates (High AMPK activation, anaerobic glycolysis) 73235 | Lipids (High fat oxidation rate, aerobic metabolism) 3035 |
| Mitochondrial Adaptation | Increased enzymatic efficiency and respiratory flux 3234 | Increased absolute mitochondrial volume and biogenesis 32 |
| Muscle Fiber Recruitment | Dominant activation of Type 2A (fast-twitch oxidative) fibers 7 | Dominant activation of Type 1 (slow-twitch endurance) fibers 7 |
| VO2max / VO2peak | Significantly superior improvements 12022 | Moderate improvements 2022 |
| Total Body Fat Loss | Equivalent (when total energy expenditure is matched) 3236 | Equivalent (when total energy expenditure is matched) 3236 |
| Time Efficiency | Superior (requires up to 5x less training volume) 7 | Inferior (requires extensive duration for adaptation) 7 |
Modality and Protocol Nuances
The application of interval training is not restricted to traditional cycling ergometers or treadmills. Variations in protocol design elicit distinct biological responses. Circuit-based interval training, which integrates resistance exercises such as squats, rows, and presses, has been compared against standard moderate-intensity circuit training. Studies involving middle-aged and older individuals show that both high-intensity and moderate-intensity circuits successfully improve estimated VO2max and diastolic blood pressure, but high-intensity circuits uniquely generate positive, lasting improvements in post-exercise systolic blood pressure 2.
Furthermore, the sequence of modalities matters. Integrating high-intensity bouts prior to circuit weight training elicits higher post-exercise blood lactate concentrations and elevated excess post-exercise oxygen consumption (EPOC) compared to integrating the intervals midway through the circuit, indicating a greater systemic metabolic perturbation 37.
When specifically comparing aerobic-type interval training against resistance-type interval training (using body weight or free weights), distinct metabolic profiles emerge. Aerobic interval training generates significantly higher peak and average oxygen consumption, making it vastly superior for cardiovascular energy expenditure 31. Conversely, resistance-type intervals result in substantially higher blood lactate concentrations immediately post-exercise, indicating a much greater reliance on the anaerobic glycolysis energy system 31. Neither variation drastically alters serum testosterone, cortisol, or heart rate variability differently than the other, but they require differing neuromuscular adaptations 31.
Epidemiological Outcomes and Longevity
While clinical trials establish the acute physiological benefits of exercise intensity, longitudinal epidemiological studies are required to ascertain if these transient adaptations translate into extended longevity and delayed morbidity.
The Generation 100 Study
The impact of exercise intensity on aging and mortality was comprehensively evaluated in the landmark Generation 100 study conducted by the Norwegian University of Science and Technology. Initiated in 2012, this trial tracked 1,567 adults aged 70 to 77 years over a five-year period 3233. Participants were randomized into a high-intensity interval training group (executing the "Norwegian protocol" of four 4-minute intervals at 90% peak heart rate), a moderate-intensity continuous group, or a control group following general physical activity guidelines 3435.
Over the 5-year observation period, the absolute mortality rates were 3% for the interval training group, 5.9% for the moderate-intensity group, and 4.7% for the control cohort 3243. Because of significant cross-over between intervention groups - up to 20% of the control group autonomously engaged in high-intensity training - and a generally high baseline fitness among the volunteers, the differences in mortality did not reach strict statistical significance 3435. However, the data revealed a compelling clinical trend toward superior survival outcomes in the high-intensity cohort 3243.
Crucially, the interval training group achieved significantly greater preservation of cardiorespiratory fitness across the one, three, and five-year intervals. Generally, adults in their 70s experience an expected 20% decline in physical capacity over a decade 3236. The interval-trained participants largely arrested this age-related cardiovascular decline, demonstrating objectively superior physical and mental quality of life metrics upon the study's conclusion 3243.
Broader Epidemiological Associations
These supervised trial findings align with broader observational epidemiology. Data derived from the Australian Longitudinal Study on Women's Health tracked the incidence of all-cause, cardiovascular, and cancer mortality 37. Women who consistently met physical activity recommendations throughout mid-life exhibited half the incidence rate of all-cause mortality compared to those who consistently failed to meet the recommendations 37.
Further pooled individual participant data meta-analyses comprising 3.36 million participants indicate an L-shaped dose-response association between exercise intensity and mortality 38. Compared to a reference group with no leisure time activity, the minimal and optimal doses of vigorous-intensity exercise for all-cause mortality reduction were 60 minutes per week (hazard ratio 0.86) and 200 minutes per week (hazard ratio 0.69), respectively 38.
Safety, Feasibility, and Clinical Guidelines
The transition of high-intensity protocols from athletic conditioning into general clinical practice requires rigorous safety validations and standardized prescribing guidelines. A persistent criticism of interval training involves the hypothesized risk of acute cardiovascular events and musculoskeletal injuries stemming from near-maximal exertion.
Adverse Events and Injury Prevalence
Systematic reviews of clinical trials have extensively audited these risks. Among populations with established cardiovascular disease, the incidence of adverse cardiac events during supervised interval training is exceptionally low. Data aggregates reveal an adverse event rate of approximately 3%, which is statistically indistinguishable from the adverse event rate observed during traditional moderate-intensity cardiac rehabilitation 11939.
Similarly, analyses of musculoskeletal injury prevalence reveal that interval training does not carry a disproportionately higher risk of joint or soft tissue injury compared to continuous training protocols, provided the modality is tailored to the individual's biomechanical capacity 1940. High relative intensities can be safely achieved through low-impact mechanisms such as cycle ergometry or aquatic training, completely removing the severe mechanical sheer forces associated with high-impact sprinting while preserving the metabolic stimulus 4142.
American College of Sports Medicine Guidelines
The integration of interval training into broader lifestyle medicine is codified in the guidelines published by the American College of Sports Medicine (ACSM). The 2025 and 2026 framework updates emphasize a well-rounded approach targeting all key components of physical health 43. The baseline recommendation dictates 150 to 300 minutes of moderate-intensity or 75 to 150 minutes of vigorous-intensity aerobic activity weekly 4344.
Notably, long-term epidemiological analyses tracking over 100,000 adults spanning three decades confirm that meeting these baseline guidelines lowers the risk of all-cause mortality by approximately 21% 45. However, performing two to four times the recommended minimum dose - specifically up to 300 minutes of vigorous activity per week - further suppresses mortality risk, reducing it by up to 31% 45. Exceeding 300 minutes of vigorous activity weekly does not appear to confer additional mortality benefits, establishing a clear threshold for optimal cardiovascular dosing 45.
For clinical populations initiating an exercise program, safety dictates a highly conservative entry. Guidelines recommend introducing interval training at a frequency of one to two sessions per week on non-consecutive days 46. These intense sessions should not entirely replace moderate-intensity baseline work; rather, they serve as a potent metabolic adjunct. Furthermore, the 2026 ACSM guidelines on resistance training underscore that while high intensity accelerates specific adaptations, the overarching determinant of functional longevity is consistency. Training all major muscle groups twice weekly yields profound benefits, and complex periodization is generally deemed unnecessary for the average aging adult 4.
Conclusion
The scientific evidence overwhelmingly validates the clinical utility and physiological potency of high-intensity interval training. It successfully justifies its reputation by providing a highly time-efficient mechanism for drastically improving maximal oxygen uptake, reducing arterial stiffness, and initiating positive mitochondrial and epigenetic adaptations. Through rigorous randomized controlled trials across oncology, cardiology, gerontology, and metabolic medicine, interval training has proven to be an exceptionally safe and scalable intervention when properly supervised.
However, recognizing its profound strengths also requires acknowledging its strict biological limitations. High-intensity training is not inherently superior for absolute fat loss when total energy expenditure is accounted for, nor does it effectively replace the specific mitochondrial volume adaptations achieved through extensive, moderate-intensity "Zone 2" training. Furthermore, while it effectively rehabilitates central cardiovascular function in compromised populations, it does not unilaterally resolve peripheral mobility and neuromuscular deficits. Ultimately, the optimal application of high-intensity interval training is not as an isolated, standalone panacea, but as a precise, high-impact clinical tool integrated within a broader, consistent framework of steady-state aerobic conditioning and progressive resistance training.