Scientific evidence and myths of testosterone and behavior
Introduction
In both clinical endocrinology and the broader cultural zeitgeist, testosterone occupies a highly polarized and frequently misunderstood position. For decades, it has been caricatured as a biological imperative for aggression, a molecular blueprint for antisocial behavior, and the foundational essence of male violence. More recently, the commercial medical sector has rebranded it as a clinical panacea for the physiological, cognitive, and sexual declines associated with aging, driving a massive surge in off-label prescribing. However, contemporary neuroendocrinology, behavioral economics, and evolutionary anthropology present a paradigm that fundamentally contradicts both of these simplified narratives.
Far from being a blunt instrument of indiscriminate hostility or a ubiquitous anti-aging tonic, testosterone is a highly contextual, facilitatory hormone. Its primary behavioral directive is not aggression, but the acquisition, maintenance, and signaling of social status 123. Depending entirely upon the environmental demands and the social context of the organism, this status-seeking drive can manifest as dominance, reactive aggression, or - counterintuitively - extreme prosociality, fairness, and generosity 123.
This exhaustive report provides an evidence-based deconstruction of how testosterone modulates human behavior. By isolating physiological realities from pervasive cultural mythologies, the analysis explores the neurobiological mechanisms dictating hormonal feedback loops, the sexually dimorphic responses in the human prefrontal cortex, and the evolutionary framework of "competitive altruism." Furthermore, it rigorously evaluates the contemporary surge in testosterone replacement therapy (TRT) among healthy men, utilizing the most recent independent meta-analyses and clinical trial data from 2023 to 2025 to delineate the clinical efficacy of exogenous androgens from the powerful placebo of cultural expectations.
Part I: Neurobiological Mechanisms and the Architecture of Action
To comprehend how testosterone influences behavior, one must first examine the foundational neuroanatomy and the complex, bidirectional feedback loops that regulate hormonal secretion, transport, and interpretation within the brain. Behavior is not merely the downstream result of hormonal release; rather, behavior and environmental stimuli actively drive endocrine function.
The Hypothalamic-Pituitary-Gonadal (HPG) Axis and the KNDy Network
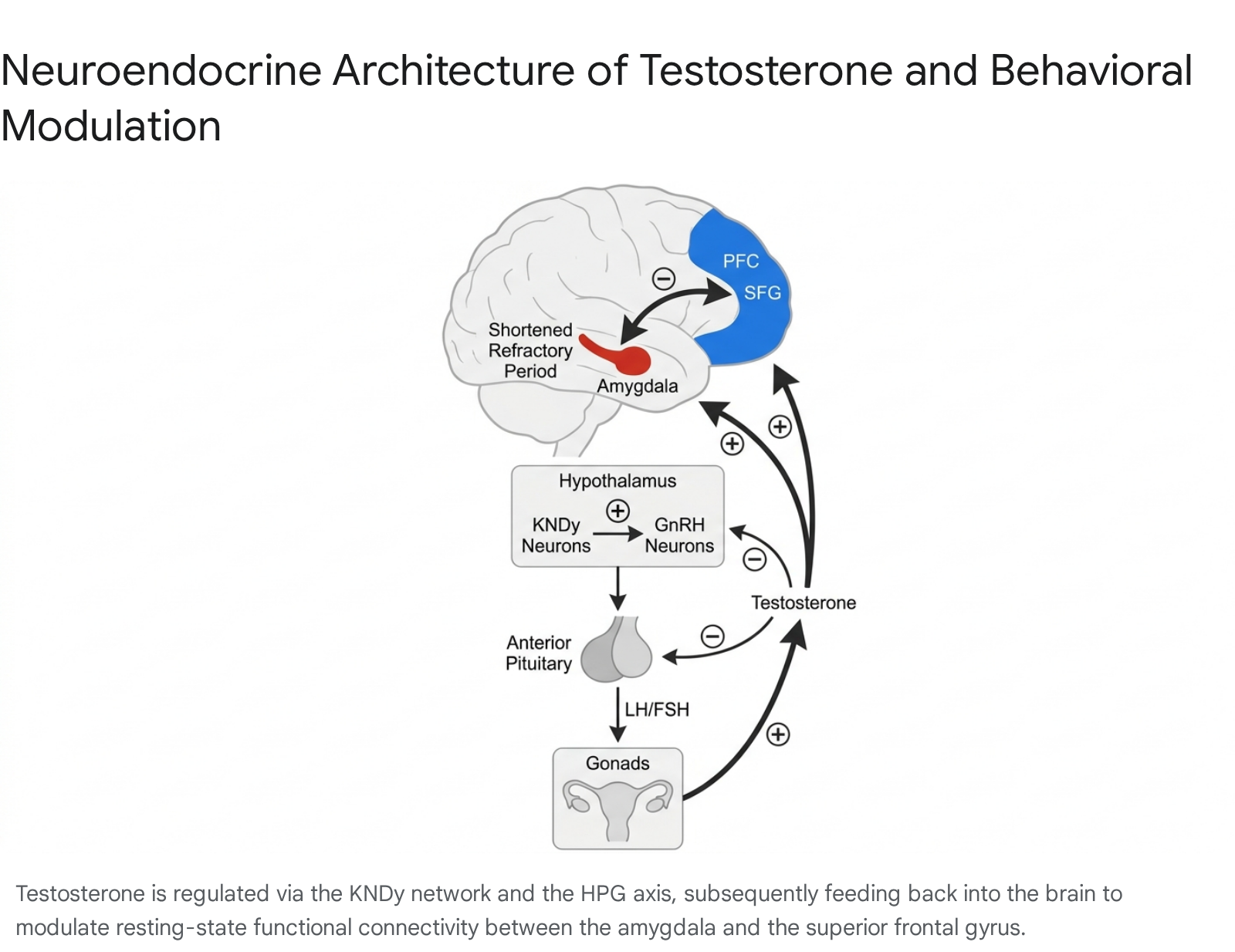
Testosterone synthesis is governed by the Hypothalamic-Pituitary-Gonadal (HPG) axis, a highly calibrated physiological feedback loop. The process initiates in the forebrain, where neurons projecting to the median eminence secrete gonadotropin-releasing hormone (GnRH) in a pulsatile manner 45. This pulsatile secretion stimulates the anterior pituitary gland to release the gonadotropin hormones - luteinizing hormone (LH) and follicle-stimulating hormone (FSH) - which subsequently travel through the systemic circulation to drive the synthesis of testosterone and estradiol in the gonads 4610.
Crucially, the regulation of this system requires continuous monitoring of circulating sex steroids, yet GnRH neurons themselves lack the requisite alpha-estrogen and androgen receptors to perform this direct feedback monitoring 7. Instead, neuroendocrinologists have identified that GnRH neurons rely on an upstream regulatory system known as the kisspeptin-neurokinin B-dynorphin (KNDy) neuronal network, located primarily in the infundibular nucleus of the hypothalamus 7.
The KNDy network serves as the master integrator for the reproductive axis. It synthesizes diverse environmental, metabolic, and social signals, acting as the primary mediator for both negative and positive sex-steroid feedback control 7. Kisspeptin acts as the most potent known secretagogue for GnRH, directly stimulating its release, while dynorphin exerts an inhibitory effect 57. This intricate network explains the biological mechanism through which social challenges, environmental stressors, and even the mere perception of a social threat can rapidly modulate testosterone availability. The presence of a rival, the threat of status loss, or the opportunity for a mate triggers upstream neurological processing that alters KNDy signaling, thereby establishing a rapid, bidirectional relationship between social behavior and systemic endocrinology 8910.
Amygdala Modulation and Prefrontal Cortex Connectivity
At the cellular level, circulating testosterone crosses the blood-brain barrier and exerts its behavioral influence primarily through androgen receptors densely distributed in the limbic system, with a particular concentration in the amygdala. The amygdala is the brain's central processing hub for threat detection, social evaluation, fear, and affective memory 1112.
The precise mechanism by which testosterone alters amygdala function illustrates the hormone's non-deterministic nature. Testosterone does not spontaneously generate action potentials within the amygdala; it does not spontaneously create a signal of fear or aggression 13. Instead, it alters the neurophysiological threshold for excitation. Following an action potential, a neuron enters a refractory period during which it is temporarily silent and cannot fire again. High levels of testosterone shorten this refractory period for neurons within the amygdala, allowing them to fire more rapidly and repeatedly when stimulated by an external trigger 13.
However, this effect is strictly facilitatory and permissive. If the neural circuitry is already excited by an external stimulus - such as a provocation, a perceived threat, or a competitive challenge - testosterone amplifies the response, increasing the volume of the neural signal 121318. If there is no external stimulus, the hormone causes no change in the amygdala's electrical activity. Thus, testosterone does not invent aggressive or dominant behaviors; it merely increases the organism's sensitivity to the environmental triggers of those behaviors 13.
The ultimate behavioral outcome of this amplified amygdala activation is heavily gated by the prefrontal cortex (PFC), specifically regions such as the superior frontal gyrus (SFG) and the dorsolateral prefrontal cortex (DLPFC) 1119. The PFC provides top-down executive control, regulating impulsivity, evaluating long-term consequences, and contextualizing the raw affective signals originating from the amygdala.
Recent neuroimaging studies utilizing resting-state functional connectivity (rsFC) mapping have revealed that endogenous testosterone functionally reorganizes the coupling between the amygdala and the PFC, but it does so across a highly sexually dimorphic and developmentally dynamic spectrum 111415. In adult men, higher endogenous testosterone tends to be associated with increased functional coupling between the amygdala and frontal cortical regions 1112. This tighter integration potentially facilitates rapid, goal-directed behavioral responses to social challenges, effectively channeling limbic arousal into strategic competitive action.
However, longitudinal neurodevelopmental studies tracking this circuitry from adolescence into adulthood demonstrate profound shifts. During early adolescence (ages 14 to 17), testosterone exhibits a positive effect on PFC engagement during emotion regulation tasks; yet, as cortical thinning progresses in these frontoparietal regions, this relationship inverts. By age 20, higher testosterone in males correlates negatively with prefrontal-amygdala connectivity during emotion control tasks, indicating a neurodevelopmental maturation process where the adult brain requires different hormonal thresholds for cognitive control 14. Furthermore, activation in the right precentral gyrus - a region implicated in the cognitive and motor aspects of inhibitory behavior - increases alongside rising testosterone levels during high-difficulty working memory tasks, demonstrating testosterone's role in executive network modulation 14.
Conversely, in women, the neurobiological response is inverted. Higher endogenous testosterone levels in healthy adult women are consistently associated with decreased resting-state functional connectivity between the right amygdala and the SFG 1119. This decoupling suggests that in females, elevated testosterone may reduce cortical cognitive down-regulation of affective processing. Behaviorally, this decoupling correlates with lower scores in agreeableness and openness, pointing to a mechanism where the hormone facilitates sex-specific patterns of assertiveness and emotional regulation 1112. The presence of such sexually dimorphic resting-state networks highlights that testosterone's influence cannot be universally generalized; its effects are intrinsically tied to the structural and organizational framework of the individual's brain 15.
Part II: Deconstructing the "Roid Rage" Myth and Physiological Variance
The pervasive cultural mythology surrounding testosterone is heavily anchored in the concept of "roid rage" - the entrenched belief that testosterone is the fundamental biological cause of violent, unprovoked aggression. This misconception arises from a profound scientific illiteracy regarding the difference between normal physiological endocrine fluctuations and the administration of massive, supraphysiological doses of synthetic androgens.
The Permissive Effect and the 20-to-200 Percent Rule
To understand testosterone's role in aggression, one must examine its permissive effect. Within the normal physiological range of a healthy human male, individual differences in basal testosterone levels do not predict who will be aggressive 123. Measuring the testosterone levels of individuals within a group offers zero predictive validity regarding which individuals will initiate a conflict or demonstrate baseline hostility 1316.
The relationship between the hormone and aggressive behavior is entirely non-linear. As detailed by prominent neuroendocrinologists, testosterone is required for the full expression of certain competitive or aggressive behaviors, but it does not independently generate them 313. This is classically demonstrated through castration studies across mammalian species. If an organism is castrated, dropping its circulating testosterone to near-zero, aggressive behavior predictably declines. However, if the organism had extensive prior experience being aggressive, the decline is less pronounced, indicating that established neural pathways maintain the behavior independently of the hormone 1213.
Crucially, if testosterone is artificially reinstated in the castrated subject, the behavioral baseline is restored. The critical neurobiological revelation is that whether the hormone is restored to a mere 20 percent of its original level, exactly 100 percent of its normal level, or 200 percent of its normal baseline, the resulting behavioral output remains entirely unchanged 13. The limbic system simply cannot differentiate between minor, moderate, and highly elevated levels of testosterone provided they remain within this vast physiological plateau 13. Because the brain is insensitive to fluctuations within this 20-to-200 percent range, claiming that an individual is more aggressive simply because their endogenous testosterone is slightly higher than their peer's is a biological fallacy 213.
This reality is further illustrated by the unique endocrinology of the spotted hyena. In this highly unusual mammalian species, social structure is entirely matriarchal. Female spotted hyenas are physically larger, vastly more aggressive, and socially dominant over males, and they possess significantly higher circulating testosterone levels than their male counterparts 13. However, the female's aggression is heavily dictated by complex socialization and early organizational brain development, rather than the acute, activational effects of circulating androgens in adulthood 1318. This underscores the principle that hormones amplify pre-existing social structures rather than independently forging them.
Therefore, the frequently observed correlation wherein high-status or highly aggressive human individuals possess higher testosterone levels is primarily driven by reverse causality. It is the execution of dominant, competitive, or aggressive behavior - and specifically, the act of winning a competition - that drives the secretion of testosterone, establishing a reinforcing physiological feedback loop, rather than the hormone spontaneously generating the behavior 21316.
The Pathology of Anabolic-Androgenic Steroids (AAS)
If physiological variance does not cause aggression, whence comes the concept of "roid rage"? The phenomenon is an empirically documented reality, but it is exclusively linked to the psychiatric sequelae of Anabolic-Androgenic Steroids (AAS) abuse 172418.
AAS abusers - ranging from professional athletes to recreational bodybuilders - routinely inject synthetic testosterone derivatives at dosages that are 10 to 100 times higher than the male body's natural physiological production 1819. A standard abuse regimen frequently entails 600 to 1,000 milligrams of testosterone per week, combined with other synthetic anabolic agents 18.
At these massive, supraphysiological concentrations, the permissive biological boundaries of the hormone are breached, overriding the brain's natural regulatory feedback inhibition and leading to profound psychiatric complications. Systematic reviews and randomized controlled trials evaluating exogenous administration at these extreme levels document distinct, dose-dependent increases in self-reported irritability, hostility, and unprovoked violence 171920. High-dose AAS administration alters the structural integrity and receptor density of the brain, precipitating severe mood destabilization.
Furthermore, the psychiatric effects of AAS abuse are deeply cyclical. During the administration phase, abusers frequently experience euphoria, increased energy, and episodes of mania or hypomania, alongside heightened aggression 1920. However, these supraphysiological exogenous doses severely suppress the HPG axis, halting the body's endogenous production of testosterone. Consequently, during the withdrawal or discontinuation phase, the user is left in a state of profound, drug-induced hypogonadism, which frequently precipitates severe clinical depression, anxiety, and suicidal ideation 241920.
The scientific consensus is unequivocal: while "roid rage" is a verified psychiatric consequence of extreme chemical abuse, attributing this violent pathology to the endogenous, daily hormonal fluctuations of a healthy human is categorically false 31818.
Part III: Status-Seeking, Generosity, and "Competitive Altruism"
Having dismantled the myth of testosterone as a dedicated aggression molecule, contemporary research has redefined it as a status-seeking hormone 1228. Testosterone modulates the brain's reward circuitry to increase the motivation to attain, defend, and elevate social rank within whatever hierarchy the individual inhabits.
The Challenge Hypothesis and Dual-Hormone Dynamics
The evolutionary and behavioral framework for this neuroendocrine response is known as the "Challenge Hypothesis." Originally formulated by Wingfield and colleagues to explain seasonal hormonal patterns in avian species, the hypothesis proposes a three-tiered model of testosterone circulation: Level A represents the non-breeding baseline, Level B represents elevations induced by environmental cues (such as day length), and Level C represents the physiological maximum reached solely through direct social stimulation 892122.
The Challenge Hypothesis states that testosterone dynamically increases from Level B to Level C specifically to facilitate male-male competition, territory formation, and mate guarding during periods of social instability 2122. Elevated testosterone represents a biological trade-off, strongly favoring mating effort and competition at the expense of paternal care and maintenance behaviors 2122. In humans, this translates to rapid, transient spikes in testosterone in anticipation of, and in response to, competitive challenges, negotiations, and direct threats to social rank 823. Exogenous testosterone administration has been shown to significantly boost motivation to compete specifically in men who hold an unstable, low social status, driving them to improve their rank when the opportunity arises 2823.
However, testosterone's ability to drive dominance is heavily moderated by the presence of cortisol, the primary glucocorticoid stress hormone, a relationship codified in the "Dual-Hormone Hypothesis." The Dual-Hormone Hypothesis posits that testosterone only effectively promotes dominant, status-seeking behavior when cortisol levels are low 322434. The biological imperative is clear: when cortisol is high - signaling severe physiological distress, chronic tension, or fear - it actively inhibits the HPG axis, suppressing testosterone synthesis and blunting androgenic receptors in the brain to conserve energy for survival 63234.
Consequently, high testosterone combined with high cortisol does not lead to calculated dominance; instead, it results in unstable, anxiety-driven, or poorly regulated erratic behavior 3234. In competitive scenarios, men given exogenous testosterone who have low basal cortisol actively seek status by competing against high-status opponents. Conversely, men given testosterone who possess high basal cortisol exhibit status-loss avoidance, preferring to compete against weaker opponents to protect their rank 34. A calm, low-stress neuroendocrine environment is therefore an absolute prerequisite for testosterone to effectively manifest its confident, approach-oriented, and strategic behavioral effects.
Prosociality and the Economics of Fairness
If status is the ultimate biological goal, the method of achieving it depends entirely upon the social context. In many complex human societies, unprovoked aggression is highly maladaptive; it routinely results in ostracization, physical retaliation, or imprisonment, equating to a severe loss of status 1. Instead, human beings often acquire and maintain rank through prestige - which is defined as freely conferred deference resulting from the public display of valuable skills, fairness, and generosity, as opposed to dominance, which relies on the threat of force 2536.
Because of this sociological reality, testosterone frequently acts as the most explicitly prosocial hormone in the human endocrine system, provided that prosocial behavior is the mechanism rewarded by society 13.
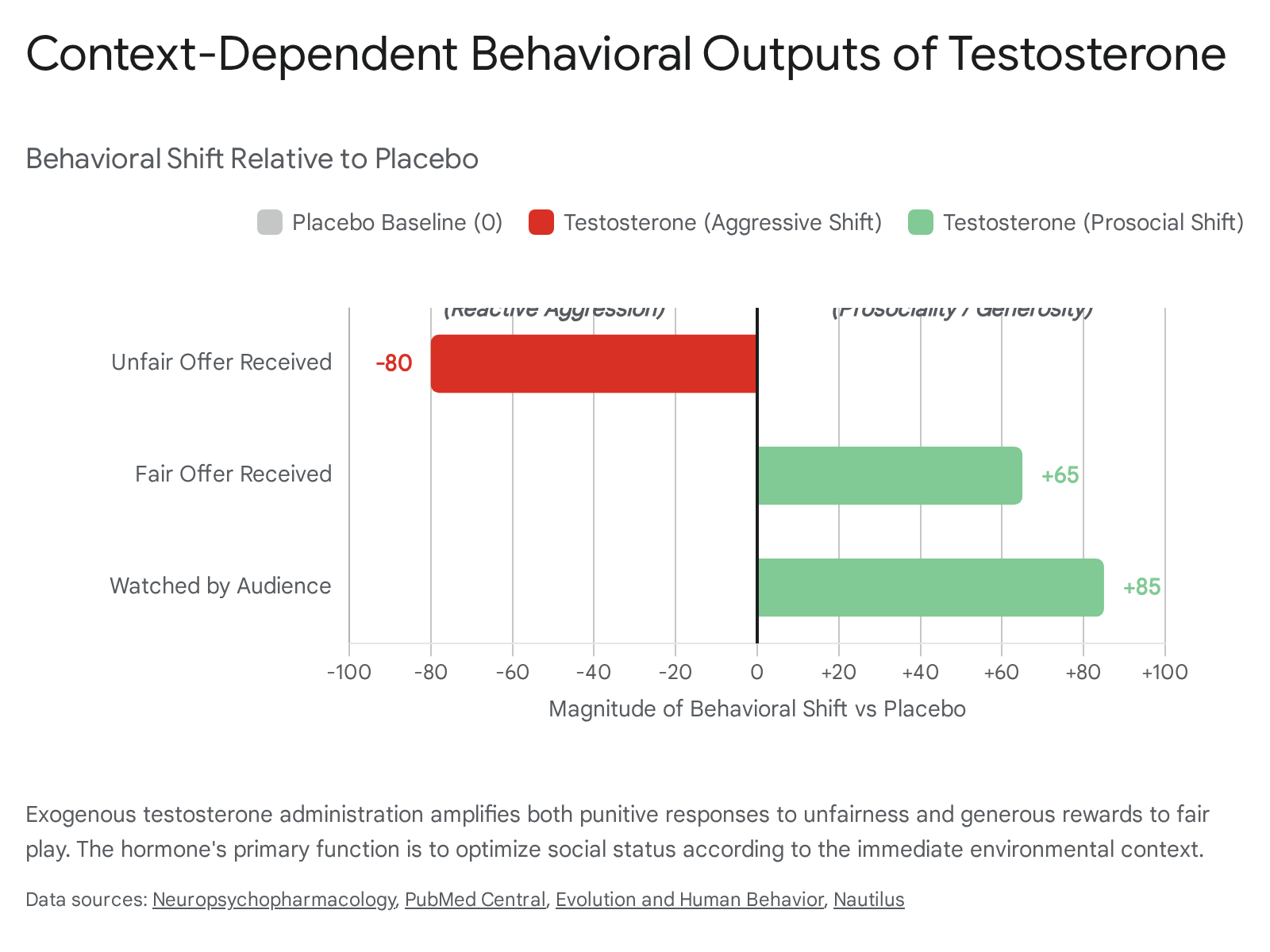
This paradigm has been rigorously tested in neuroeconomic laboratory settings utilizing the Ultimatum Game and the Dictator Game. In the Ultimatum Game, a "proposer" offers a division of a sum of money to a "responder." If the responder accepts, both keep the money; if the responder rejects the offer as unfair, both receive nothing. In double-blind, randomized trials, men injected with exogenous testosterone demonstrated two distinct behaviors compared to those on a placebo: they were more likely to severely punish proposers who made extremely unfair offers (reactive aggression to defend status), but crucially, when they were the proposers receiving large endowments, they offered significantly higher, fairer amounts to the responders (generosity to acquire status) 1226. Testosterone amplifies the punitive response to provocation, but equally amplifies generosity in the absence of provocation to secure a positive reputation 126.
The Dictator Game isolates altruism further, as the responder has no power to reject the offer. In a 2024 study assessing endogenous salivary hormones and Bayesian data modeling, researchers found that higher basal testosterone levels in general-population men correlated with significantly greater generosity and altruistic allocations 327.
Computational drift-diffusion modeling reveals the underlying cognitive architecture of these decisions. Testosterone does not deteriorate reinforcement learning or logical reasoning; rather, it increases the motivational weight of a social reward 2840. When male participants engage in tasks where they know they are being observed by an audience (the "audience effect"), testosterone administration eliminates deceptive or strategic prosociality. Instead, it boosts an honest, deeply ingrained drive to contribute, ensuring the individual is perceived as a benevolent, high-value asset to the group, which directly translates to elevated social rank 2284029.
Ethnographic Evidence of Competitive Altruism
This laboratory evidence is robustly supported by extensive cross-cultural ethnographic data from nonindustrial and small-scale societies. Across these populations, high-status men consistently achieve greater reproductive success, lower offspring mortality, and enhanced political influence 30314432.
For example, among the Tsimane people, an indigenous forager-horticulturalist society in the Bolivian Amazon, researchers have conducted multivariate longitudinal analyses of male status. While dyadic physical fights are infrequent among the Tsimane, men who achieve high status and influence within the community demonstrate significantly higher fertility and lower offspring mortality within their marriages, owing to the superior support of community allies and access to resources 3144. Conversely, high status also affords these men a higher rate of extra-marital affairs, underscoring that status pursuit optimizes both parenting and mating effort simultaneously 3144.
Achieving this status, however, relies primarily on the anthropological mechanism of "competitive altruism." This theory posits that group members actively compete with one another to demonstrate the greatest capacity to benefit the community, as followers award the highest social status to those who provide the most public goods 36303246.
A striking historical manifestation of this is the "potlatch" ceremonies practiced by the indigenous communities of the Pacific Northwest Coast, such as the Coast Salish and Nootka 253644. In these societies, tribal chiefs and leaders competed aggressively not through physical violence, but through conspicuous generosity, intentionally distributing or destroying vast collections of their personal material wealth 3646. The individual who demonstrated the most extreme, self-sacrificial benevolence accrued the most prestige, which directly translated to political power and coalitionary support necessary for organizing complex collective actions like inter-village ceremonies or military defense 3646. Similar patterns of status allocation based on the provisioning of skills or resources are documented among the Nuer of Sudan and the Toba of South India 44.
In these environments, individuals with a neurobiological predisposition for high testosterone are driven to excel in these group-beneficial tasks - such as hunting large game, resolving disputes, or distributing wealth - because the resulting prestige is the most reliable vector for reproductive fitness 363031. Thus, the evolutionary architecture of testosterone heavily favors diplomacy, resource sharing, and public altruism whenever those strategies represent the optimal path to ascend the social hierarchy.
Part IV: Behavioral Effects in Women and the Power of Expectancy
While the majority of endocrinological research has historically focused on men, modern studies integrating female participants have unveiled critical nuances regarding testosterone's function, particularly concerning sexually dimorphic behavioral responses and the profound psychological impact of cultural expectations.
In a landmark neuroeconomic study conducted by Eisenegger, Naef, and colleagues, female participants were engaged in the Ultimatum Game under a double-blind, placebo-controlled protocol. They were administered either a sublingual dose of testosterone or a placebo, and subsequently asked to guess which substance they had received 3334.
The results systematically dismantled the biological determinism of aggression. The women who actually received testosterone made significantly fairer, more generous, and more prosocial offers than those who received the placebo, perfectly aligning with the status-seeking hypothesis wherein fair play ensures successful social transactions 1634. However, the data revealed a stunning counter-narrative based on belief: the women who merely believed they had received testosterone - regardless of whether they had ingested the active hormone or the placebo - behaved far more aggressively, selfishly, and unfairly 333449.
This demonstrates a powerful psychosocial phenomenon. The cultural mythology insisting that testosterone causes aggressive, egocentric behavior is so deeply entrenched in the societal consciousness that the mere expectancy of the hormone overrides baseline behavioral tendencies 3334. People use the mythology of testosterone as a subconscious permission structure to act poorly, projecting biological justification onto socially conditioned selfishness. It highlights that human behavior is far less tightly controlled by sheer biology than in other animal models, heavily mediated by cognitive prejudices 3334.
Furthermore, the behavioral effects of endogenous testosterone in women are not universally prosocial and exhibit distinct sexually dimorphic patterns. In the aforementioned 2024 Dictator Game study utilizing Bayesian analysis, while higher basal testosterone promoted altruistic behavior in men, both testosterone and cortisol were negatively correlated with generosity in women 32750. Female participants with higher endogenous testosterone offered significantly less to their counterparts 350.
This dimorphism is likely tied to complex, recurrent biological feedback loops unique to the female endocrine system, which heavily alter stress reactivity. In women, estrogen generally suppresses cortisol; however, during the luteal phase of the estrus cycle when estrogen drops, cortisol reactivity spikes 32. The interplay between estrogen, progesterone, and cortisol creates a recurrent loop that heightens female stress sensitivity 32. If a woman with naturally high endogenous testosterone is placed in a high-stress, high-cortisol environment, the protective, status-seeking prosociality of testosterone is severely blunted, leading to decreased oxytocin sensitivity and increased defensiveness 3234. Understanding these sex-linked hormonal cyclities is crucial for decoding relational dynamics and behavioral dysregulation, proving that hormone-behavior interactions are fundamentally systemic, operating within an intricate web of competing neurochemicals rather than as isolated variables.
Part V: The Clinical Realities of Testosterone Replacement Therapy (TRT)
The massive disparity between testosterone's scientific reality and its cultural perception has manifested most acutely in the modern medical marketplace. Driven by aggressive marketing campaigns promising restored youth, cognitive sharpness, endless energy, and heightened libido, prescriptions for Testosterone Replacement Therapy (TRT) have skyrocketed globally, evolving from a niche endocrine treatment to a mainstream wellness trend 35525354.
In the United States, prevalence rates for TRT increased dramatically between 2018 and 2022. While usage rose across all demographics, the sharpest percentage increases occurred in young men. Rates climbed by 86% in men aged 25 to 34, and by an astonishing 120% in those under 24 (a statistic notably encompassing shifts toward gender-affirming care) 35. An estimated 40% of men under the age of 40 now express active interest in testosterone supplementation, largely seeking to "optimize" their lifestyle and combat perceived fatigue or mood disorders 35. The product landscape is currently dominated by topical gels, accounting for over 60% of the market share, though innovations in subcutaneous implantable pellets and nasal sprays are gaining traction to avoid the liver strain associated with older oral formulations 35535455.
However, independent, peer-reviewed meta-analyses published between 2023 and 2025 paint a starkly different picture regarding the efficacy and safety of TRT, particularly for eugonadal men (those with normal baseline testosterone levels) seeking off-label wellness benefits 3637383960.
Efficacy: Clinical Hypogonadism vs. Eugonadal Enhancement
TRT remains an essential, FDA-approved medical treatment for clinical hypogonadism - a pathological deficiency typically resulting from testicular failure or severe pituitary dysfunction 535540. In truly hypogonadal men, TRT yields measurable, highly beneficial physiological results: it effectively increases lean body mass, stabilizes bone mineral density, and modestly improves sexual function and depressive symptoms, particularly in men suffering from treatment-resistant depression (TRD) 41426443.
Conversely, the commercial "wellness" industry largely targets men experiencing natural age-related late-onset hypogonadism (LOH) or men with standard physiological ranges seeking lifestyle optimization 544044. For this demographic, the clinical data is highly unsupportive of the marketing hype. Pushing testosterone levels above a standard threshold of approximately 12 nanomoles per liter (roughly 350 ng/dL) in an otherwise healthy man produces rapidly diminishing returns 40.
A massive 2024 Cochrane Database systematic review, encompassing 43 randomized controlled trials and over 11,400 participants, rigorously assessed the effects of TRT on sexual dysfunction in men without severe, primary hypogonadism. The findings were definitive: in the short term, TRT has little to no clinically significant effect on erectile function compared to a placebo, and is vastly inferior to standard phosphodiesterase-5 (PDE5) inhibitors 363845. Furthermore, it resulted in negligible improvements to general sexual quality of life, scoring a mean difference of only -2.31 on the Aging Males' Symptoms (AMS) scale, falling well short of the minimal clinically important difference of 10 3645.
Behaviorally, the results are similarly muted. In two independently conducted double-blind, placebo-controlled trials published in 2025, researchers tested whether a single exogenous dose of testosterone boosted competitive drive, self-confidence, or financial risk-taking in healthy eugonadal men engaging in economic tasks 68. The results demonstrated zero significant behavioral changes, confirming that a brief hormonal boost does not magically transform an individual's economic or competitive profile 68.
| Clinical Endpoint | Meta-Analysis Consensus (2023-2025) for Healthy/LOH Men | Scientific Certainty & Representative Sources |
|---|---|---|
| Erectile Function | Little to no improvement compared to placebo; inferior to targeted PDE5 inhibitors. Minor WMD increases noted in select sub-cohorts. | High Certainty 3638454647 |
| Cognitive Confidence & Risk-Taking | No significant effect on willingness to compete, assertiveness, or risk-taking in standardized economic tasks. | High Certainty 68 |
| Sexual Quality of Life | Minimal clinical difference (MD: -2.31 on the 85-point AMS scale, failing to meet the MCID threshold of 10). | Moderate Certainty 3645 |
| Depression & Mood | Minor improvements in fatigue and mood noted, but significant anti-depressant effects primarily restricted to men with pre-existing clinical TRD. | Mixed/Moderate 6443 |
| Musculoskeletal Profile | Successfully increases total/free serum testosterone and slightly elevates BMI and lean mass, but fails to improve functional handgrip strength or reduce fracture risk over placebo. | High Certainty 42 |
The Cardiovascular Safety Profile: The TRAVERSE Trial Paradigm
The safety profile of TRT has been historically contentious, marked by severe FDA black-box warnings regarding increased risks of myocardial infarction and stroke 355260. The clinical landscape shifted dramatically in 2023 with the completion of the TRAVERSE trial, a highly powered, multi-year randomized clinical trial designed explicitly to test cardiovascular outcomes in men receiving transdermal TRT versus a placebo 6071.
The TRAVERSE trial demonstrated that restoring testosterone to normal physiological levels did not increase the incidence of major adverse cardiovascular events (MACE), prompting the FDA to officially remove the MACE black-box warning from all testosterone products in 2025 3560. This was corroborated by a 2024 NIHR (National Institute for Health and Care Research) individual participant data meta-analysis of 35 trials, which found no statistically significant difference in mortality or cardiovascular events between TRT and placebo groups in the short-to-medium term 37.
However, this newfound perception of relative cardiovascular safety is highly nuanced and demands strict clinical oversight. While the FDA removed the MACE warning, it simultaneously mandated a new warning regarding persistent elevations in ambulatory blood pressure associated with the therapy 35. Furthermore, the granular TRAVERSE data indicated slight but statistically significant increases in the risks for nonfatal arrhythmias (such as atrial fibrillation) and acute kidney injury 4071. Additionally, while TRT does not appear to trigger the de novo generation of prostate cancer, it definitively elevates Prostate-Specific Antigen (PSA) levels and prostate volume, requiring rigorous long-term urological and oncological surveillance 42464771.
Perhaps most critically for the younger demographic driving the recent market expansion, exogenous TRT severely disrupts the delicate HPG axis. The continuous influx of external androgens suppresses the brain's natural production of GnRH, LH, and FSH via negative feedback. Prolonged administration effectively shuts down endogenous testicular function, drastically reducing spermatogenesis and leading to severe, and occasionally irreversible, infertility and testicular atrophy 534071. For men wishing to preserve fertility, clinicians are increasingly forced to prescribe adjunctive therapies, such as clomiphene citrate or gonadotropin analogues, to artificially maintain testicular function alongside TRT 5340.
Conclusion
The behavioral neuroendocrinology of testosterone reveals an exquisitely complex, context-dependent regulatory system that bears virtually no resemblance to its cultural caricature. Testosterone is not the biological progenitor of aggression. It does not blindly incite violence, it does not invent hostility out of a vacuum, nor does it override rational cognitive control in healthy individuals.
Instead, testosterone acts as a profound amplifier of pre-existing social structures; it is a dedicated status-seeking hormone. It facilitates whatever behaviors are necessary to acquire, maintain, and signal social rank within a specific environmental framework. When placed in cooperative, prestige-based environments, testosterone drives remarkable prosociality, fairness, and "competitive altruism," pushing individuals to demonstrate their indispensable value to the group. The neural mechanism driving this - gated by cortisol, modulated by the KNDy network, and regulated by highly sexually dimorphic prefrontal cortex connectivity - highlights a fundamental biological truth: human behavior dictates hormonal surges just as strongly as hormones influence behavior.
The stubborn persistence of the "roid rage" and aggressive "alpha male" myths relies heavily on the profound misattribution of supraphysiological anabolic steroid abuse to natural human physiology. This is further compounded by the potent psychological placebo effect, wherein individuals act aggressively and selfishly simply because they falsely believe their biology mandates it.
As the wellness industry aggressively markets testosterone replacement therapy to increasingly younger, healthy men under the guise of lifestyle optimization, modern 2023-2025 clinical meta-analyses provide a necessary and sobering scientific anchor. Exogenous testosterone offers vital, life-improving therapeutic relief for men suffering from severe clinical hypogonadism. However, as an off-label enhancement tool for eugonadal men, it fails to significantly elevate sexual function, competitive drive, or overall quality of life above placebo levels, while carrying persistent risks of infertility, elevated blood pressure, and cardiovascular strain. In both behavioral biology and clinical medicine, more testosterone does not inherently create a more dominant or vital human; it merely amplifies the socio-behavioral infrastructure that is already present.