Scientific Evidence and Efficacy of Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) occupies a dominant position within global mental health care, widely recognized by major health institutions and clinical guidelines as the gold standard for psychological intervention. This status was not achieved organically through clinical consensus alone, but rather through a decades-long alignment with the principles of evidence-based medicine. Because CBT is inherently structured, time-limited, and goal-oriented, it was uniquely suited for evaluation via randomized controlled trials (RCTs). As a result, cognitive behavioral therapy has accumulated an unparalleled volume of empirical support over the past half-century.
However, contemporary psychiatric research presents a highly nuanced view of the modality. Recent large-scale meta-analyses have prompted a re-evaluation of its absolute efficacy, revealing modest remission rates across several diagnostic categories. These findings have driven the evolution of "third-wave" behavioral therapies, catalyzed neurobiological research into therapeutic mechanisms, and accelerated the development of culturally adapted modalities for diverse populations.
Historical Development and Institutional Endorsement
The ascendancy of cognitive behavioral therapy is inextricably linked to the broader "cognitive revolution" of the mid-20th century and the subsequent global push for evidence-based practice in health care policy.
Origins in Behaviorism and Cognitive Theory
Prior to the 1960s, psychotherapy was largely dominated by psychodynamic and psychoanalytic models, which focused heavily on unconscious conflicts, early childhood experiences, and long-term, open-ended exploration 122. Simultaneously, first-wave behaviorism - championed by figures such as B.F. Skinner, Ivan Pavlov, and John B. Watson - focused strictly on observable behaviors, emphasizing concepts like respondent conditioning, extinction, and habituation 122. While behaviorism offered measurable outcomes, it largely failed to account for internal mental states.
In the 1950s and 1960s, psychologists Albert Ellis and Aaron T. Beck independently recognized the limitations of both pure behaviorism and traditional psychoanalysis. Beck observed that patients suffering from depression exhibited a "cognitive triad" of negative, automatic thoughts regarding themselves, the world, and the future 24. This observation formed the basis of cognitive therapy, which posited that emotional distress is directly mediated by maladaptive information processing and cognitive distortions - such as catastrophic thinking, all-or-nothing paradigms, and mind-reading 3.
The integration of cognitive restructuring with behavioral exposure techniques created classical CBT. This development was bolstered by the broader "cognitive revolution," a movement built on the premise that the mental world can be grounded in physical computation and feedback, and that human behavior is generated by complex, interacting mental programs 4. By targeting both the behavioral symptom and the underlying cognitive distortion, classical CBT provided a comprehensive, problem-focused, and action-oriented intervention strategy 5.
The Shift to Evidence-Based Medicine
As public health systems sought to allocate limited resources effectively, the concept of evidence-based medicine gained immense traction in the 1990s. Health authorities began requiring behavioral treatments to demonstrate superiority over placebos or "treatment as usual" (TAU) in rigorous RCTs 86. Traditional psychodynamic therapies, which were highly individualized and reliant on the unique dynamic between therapist and patient, resisted manualization and were consequently difficult to test in standardized clinical trials 7.
Conversely, CBT was easily manualized. Its session-by-session structure allowed for high treatment fidelity across different practitioners and clinical sites 7. Consequently, CBT amassed a vast, robust evidence base well before other psychotherapeutic modalities, cementing its status as an empirically supported treatment.
Timeline of Major Institutional Endorsements
The rapid accumulation of RCT data led to sweeping endorsements from major clinical guidelines, fundamentally reshaping the global provision of mental health services and public funding.
| Year | Institution or Initiative | Nature of Endorsement and Policy Impact |
|---|---|---|
| 2004 | National Institute for Health and Care Excellence (NICE) | Published guidelines recommending CBT and interpersonal therapy as the primary evidence-based psychological treatments for depression in the UK, effectively excluding non-manualized therapies from first-line status 18. |
| 2008 | Improving Access to Psychological Therapies (IAPT) | The UK National Health Service launched IAPT to scale up psychological care. The program heavily favored CBT, tripling the mental health budget for talking therapies and training a massive workforce of low-intensity CBT practitioners 8. |
| 2008 / 2010 | World Health Organization (WHO) | Launched the Mental Health Gap Action Programme (mhGAP) in 2008 and its Intervention Guide in 2010. The guide recommended CBT as a first-line treatment for depression, anxiety, and substance dependence in low- and middle-income countries, driving global scale-up 812910. |
| 2017 | American Psychological Association (APA) | Published the Clinical Practice Guideline for the Treatment of PTSD, strongly recommending CBT (and trauma-focused variants) as a first-line intervention based on extensive empirical evidence 511. |
Quantitative Efficacy Across Psychiatric Diagnoses
While the relative efficacy of cognitive behavioral therapy compared to waitlist controls and psychological placebos is firmly established, contemporary meta-analytical research has shifted focus toward absolute outcomes. This distinction is critical for health care providers and policymakers seeking to understand the actual likelihood of patient recovery.
Absolute Response and Remission Rates
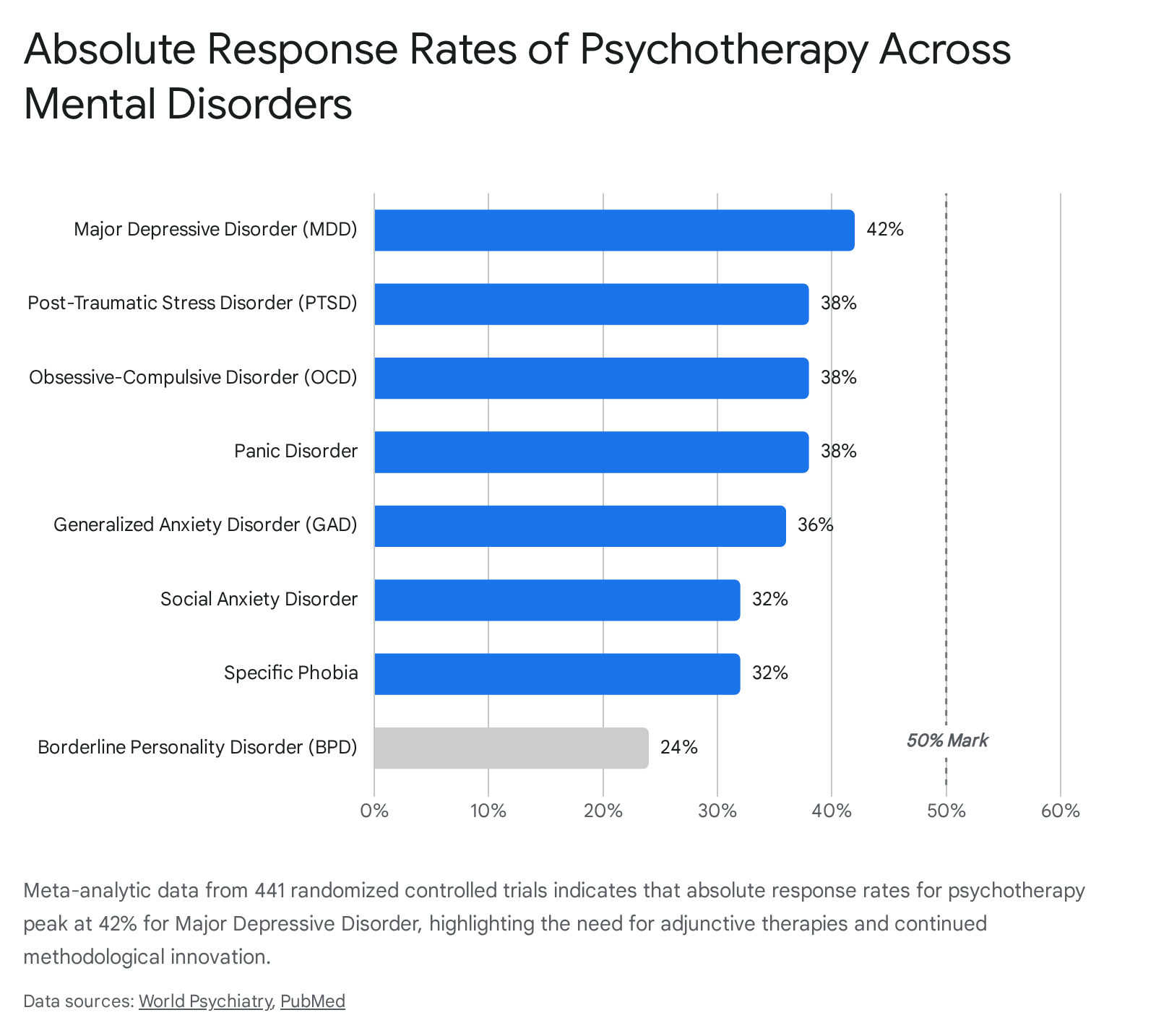
A landmark 2024 living systematic review and meta-analysis led by Pim Cuijpers analyzed data from 441 randomized controlled trials involving 33,881 patients. The study sought to determine the absolute response rates - defined as at least a 50% reduction in symptoms between baseline and post-treatment - across eight major mental disorders 1213. The findings confirmed that psychotherapies (predominantly CBT) are highly effective relative to control groups; however, the absolute response rates remain fundamentally modest.
The Cuijpers data revealed high heterogeneity across trials (I2 ranging from 65% for obsessive-compulsive disorder to 82% for major depressive disorder), indicating that treatment effects vary significantly based on individual patient characteristics and specific trial methodologies 1213.
Beyond response rates, full clinical remission - the complete absence of pathological symptoms - remains a complex hurdle. In the treatment of generalized anxiety disorder (GAD), meta-analyses report post-treatment remission rates of approximately 51.4%, which occasionally increase to 65% at follow-up assessments as patients continue to apply newly acquired cognitive skills 14. In older adults experiencing late-life anxiety, CBT achieves an average remission rate of 54% 15.
For post-traumatic stress disorder (PTSD), trauma-focused variants of CBT (TF-CBT) exhibit robust initial response rates, reaching 85% in select clinical trials, though full remission generally hovers around 40% 16. This suggests that while CBT is highly adept at reducing the severity of distress, residual symptoms often persist, necessitating ongoing symptom management or adjunctive interventions 14.
Efficacy in Pediatric and Adolescent Populations
CBT exhibits particularly strong empirical backing in pediatric psychopathology. A comprehensive Mayo Clinic meta-analysis reviewing 115 studies with 7,719 pediatric patients demonstrated that CBT significantly improves primary anxiety symptoms, remission, and overall response when compared to waitlist or no-treatment controls 1718. Similarly, for pediatric PTSD, an analysis of 70 randomized clinical trials involving 5,528 youth concluded that trauma-focused cognitive behavioral therapies (TF-CBTs) achieved the highest symptom reductions both immediately post-treatment and longitudinally (six or more months post-treatment) when compared to Eye Movement Desensitization and Reprocessing (EMDR) and non-trauma-focused interventions 19.
Despite strong outcomes, qualitative data indicates that working with youth exposed to complex, repeated, and interpersonal trauma presents unique feasibility and acceptability challenges, requiring highly calibrated pacing and robust caregiver involvement to prevent therapeutic ruptures 20.
Applications in Severe Mental Illness and Complex Psychopathology
Historically, CBT was considered most appropriate for mild to moderate anxiety and unipolar depressive disorders. However, its application has expanded significantly to encompass severe mental illness. A 2025 meta-analysis published in JAMA Psychiatry evaluating 375 randomized clinical trials (32,968 adults) found that while CBT was highly effective for PTSD (effect size 1.27) and specific phobias (effect size 1.17), it yielded substantially lower effect sizes for bipolar disorder (0.31) and psychotic disorders (0.43) 21.
Despite these smaller relative effect sizes, cognitive behavioral therapy for psychosis (CBTp) remains a critical adjunctive treatment. For patients who exhibit medication-resistant positive symptoms of schizophrenia, CBTp confers beneficial effects above and beyond those of antipsychotic medication alone. A meta-analytic review of outpatients with medication-resistant psychosis found that CBTp reduced both positive symptoms (Hedges' g = 0.47) and general symptoms (Hedges' g = 0.52), maintaining these gains at follow-up 22. Notably, the dropout rate for these complex patients was only 14%, indicating high treatment acceptability 22. Furthermore, specialized adaptations of TF-CBT are increasingly utilized for patients with comorbid psychosis and PTSD, helping to address traumatic exposures while managing the cognitive distortions inherently linked to hallucinatory experiences 23.
Comparative Analysis with Pharmacotherapy and Alternative Psychotherapies
The clinical reality is that CBT rarely operates in a vacuum; it is frequently evaluated against, or utilized alongside, pharmacotherapy and other psychological modalities.
Cognitive Behavioral Therapy Versus Pharmacotherapy
The current scientific consensus posits that for conditions like Major Depressive Disorder (MDD) and Generalized Anxiety Disorder (GAD), CBT and specific antidepressant medications (such as SSRIs and SNRIs) serve as equally viable first-line treatments.
| Outcome Metric | Cognitive Behavioral Therapy (CBT) | Pharmacotherapy (SSRIs/SNRIs) | Combination Therapy |
|---|---|---|---|
| Short-Term Response | Modestly superior to treatment-as-usual and psychological placebos; roughly equivalent to pharmacotherapy in short-term symptom reduction 2425. | Highly effective in reducing primary symptoms quickly. Response rates are significantly higher than pill placebos (e.g., 62% vs 35% for late-life anxiety) 1517. | Combining CBT with an SSRI consistently yields superior response and remission rates compared to either treatment alone, particularly in moderate-to-severe presentations 3031. |
| Long-Term Relapse Prevention | Demonstrates clear long-term advantages. Patients continue to utilize cognitive restructuring and exposure techniques, resulting in lower relapse rates post-treatment 152526. | Frequently associated with a return of symptoms upon medication discontinuation. Benzodiazepines are specifically contraindicated for PTSD due to high relapse and exacerbation risks 1530. | Maintaining CBT while titrating or adding medication prevents recurrence, acting as a sustained behavioral anchor 430. |
| Adverse Events and Tolerability | Generally features a highly favorable side-effect profile. Dropout rates are historically lower than, or equivalent to, pharmacotherapy arms 1517. | Associated with physiological side effects (e.g., sedation, weight changes, withdrawal syndromes). Dropout rates can be high due to poor tolerability 1718. | Patients must balance the cognitive benefits against the physiological side effects of the medication component 17. |
When traditional CBT monotherapy fails to elicit a sufficient response - such as in chronic PTSD after a standard six-month trial - evidence-based guidelines explicitly recommend maintaining the psychotherapeutic framework while adding an SSRI, rather than terminating CBT to switch exclusively to medication. Research demonstrates that adding antidepressant medication for patients who do not achieve remission with CBT alone generates remission rates ranging from 41% to 89% 30.
Cognitive Behavioral Therapy Versus Psychodynamic Therapy
A major contemporary debate in clinical psychology centers on the comparative efficacy of CBT versus modern, time-limited psychodynamic therapy. While CBT has long claimed empirical superiority, recent high-quality RCTs challenge this assumption.
A 2025 randomized controlled trial involving 100 patients with MDD compared 16 sessions of CBT against short-term psychodynamic psychotherapy (STPP). The results indicated absolute parity: no significant differences were found between the two modalities on primary outcome measures. Both treatments achieved large within-group effect sizes, with approximately 79% of patients across both arms demonstrating reliable clinical improvement 27. Similarly, longitudinal trials evaluating short-term treatments for Social Anxiety Disorder have found that both CBT and psychodynamic therapy exhibit comparable, sustained response rates (ranging from 58% to 72%) at 6-, 12-, and 24-month follow-ups 28.
Defenders of CBT's gold-standard status acknowledge these equivalence findings but emphasize a critical statistical principle: equivalence is not transitive. The fact that a specific psychodynamic protocol achieves equivalence to CBT in a tightly controlled trial for a specific disorder does not automatically elevate all psychodynamic therapies to gold-standard status across all diagnoses 7. CBT remains the clinical benchmark because its specific mechanisms of action are more rigorously mapped, and it has been empirically validated across a vastly wider array of psychopathologies 7.
Neurobiological Mechanisms of Change
Historically, the efficacy of psychotherapy was measured through self-reported psychological inventories. However, advances in neuroimaging and molecular biology have provided empirical evidence that CBT induces quantifiable structural and functional changes in the brain, validating the theory that behavioral and cognitive modifications generate profound neuroplasticity.
Modulation of the Hypothalamic-Pituitary-Adrenal Axis
Chronic stress, severe trauma, and major depressive disorder are highly correlated with hyperactivity in the hypothalamic-pituitary-adrenal (HPA) axis, leading to the sustained release of glucocorticoids such as cortisol. Elevated, chronic cortisol exposure is demonstrably neurotoxic to the hippocampus - a medial temporal lobe structure critical for learning, memory formation, and emotional regulation 2930. This neurotoxicity results in structural damage, including the retraction of apical dendrites in the cornu ammonis (CA3) region, suppressed adult neurogenesis in the dentate gyrus, and measurable macroscopic reductions in total hippocampal volume 3031.
CBT interventions, particularly those involving cognitive restructuring and systematic exposure, directly modulate HPA axis reactivity. By training patients to consciously re-evaluate threat cues and reduce catastrophic thinking, CBT mitigates the physiological stress cascade 1131. This reduction in chronic stress signaling lowers the neurotoxic burden on the hippocampus, facilitating the restoration of brain-derived neurotrophic factor (BDNF). BDNF is an essential neurotrophin that promotes neuronal survival, synaptogenesis, and the integration of newborn neurons into adult brain circuits, ultimately fostering recovery from stress-induced atrophy 293132.
Alterations in Macroscopic Neural Networks
CBT also impacts broad, macroscopic neural networks involved in executive function. A 2024 study conducted by researchers at Stanford Medicine evaluated problem-solving therapy (a specific CBT modality) in adults suffering from comorbid depression and obesity. Utilizing functional magnetic resonance imaging (fMRI), the researchers tracked neural adaptations throughout the treatment course. They discovered significant, adaptive changes in cognitive control circuit activity within just two months of initiating therapy 33.
Crucially, the Stanford researchers found that these early neural changes served as a reliable predictive biomarker. The functional connectivity shifts identified at the two-month mark accurately predicted which patients would demonstrate continued improvement in depressive symptoms at 12- and 24-month follow-ups. This provides concrete evidence that real-world problem-solving and cognitive restructuring literally rewire the brain's executive networks in a lasting manner 33. Furthermore, similar neuroplastic mechanisms are leveraged in the treatment of substance use disorders, where cognitive interventions help restore glutamatergic dynamics and alter the transcriptomic landscape of the nucleus accumbens 32.
Third-Wave Modalities and the Evolution of the Paradigm
The recognition that classical CBT does not guarantee full remission for all patients, and that its focus on actively changing the content of thoughts can sometimes increase distress, led to the proliferation of alternative modalities. Over the last three decades, CBT has evolved into a broad umbrella term encompassing traditional second-wave therapies and newer "third-wave" approaches 734.
Acceptance and Commitment Therapy and Dialectical Behavior Therapy
During the 1980s and 1990s, researchers sought to address complex clinical presentations - such as chronic worry, personality disorders, and deep-seated trauma - by integrating concepts of mindfulness and psychological acceptance into the cognitive behavioral framework 5. This intellectual shift produced therapies such as Acceptance and Commitment Therapy (ACT), pioneered by Dr. Steven C. Hayes, and Dialectical Behavior Therapy (DBT).
While ACT and DBT fall under the broader CBT umbrella and maintain a rigorous commitment to empirical validation, their underlying mechanisms of change differ fundamentally from classical CBT.
| Therapeutic Modality | Core Philosophical Mechanism | Treatment of Maladaptive Thoughts | Primary Clinical Targets |
|---|---|---|---|
| Classical Cognitive Behavioral Therapy (CBT) | Cognitive restructuring; systematic behavioral exposure 2335. | Identifies unhelpful thought patterns (distortions) and actively challenges, reframes, and alters their content to be more accurate 3. | Depression, specific phobias, generalized anxiety disorder, panic disorder, obsessive-compulsive disorder 535. |
| Acceptance and Commitment Therapy (ACT) | Psychological flexibility; cognitive defusion; values-based living 3536. | Does not attempt to change thought content. Teaches clients to change their relationship to thoughts by observing them without judgment or fusion 3. | Chronic worry, substance use disorders, chronic pain, and values-based lifestyle transitions 363738. |
| Dialectical Behavior Therapy (DBT) | Balancing radical acceptance with active change; intensive emotion regulation 339. | Acknowledges and validates the presence of intensely painful thoughts and emotions, while simultaneously building skills to prevent destructive behavioral reactions 3. | Borderline personality disorder (BPD), chronic suicidality, severe self-harm, and severe emotional dysregulation 3946. |
Meta-analytic reviews evaluating third-wave treatments consistently report moderate treatment effects. In head-to-head trials for highly prevalent disorders like depression and anxiety, ACT and classical CBT demonstrate statistically equivalent efficacy 3840. ACT recently surpassed the milestone of 1,000 published randomized controlled trials, establishing it as a highly robust intervention 36. However, for specific conditions like borderline personality disorder, DBT is overwhelmingly recognized as the specialized gold standard, whereas classical CBT remains the undisputed first-line treatment for obsessive-compulsive disorder via its Exposure and Response Prevention (ERP) protocols 5374641.
Digital Delivery and Algorithmic Innovations
In response to acute global clinician shortages, extensive waitlists, and the prohibitive financial cost of traditional therapy, researchers have translated CBT into digital and automated formats. Internet-delivered CBT (ICBT) and digital CBT (DCBT) via smartphone applications have proven remarkably successful.
An individual patient data meta-analysis of 2,866 patients across 29 Swedish trials found that ICBT yielded a reliable response rate of 65.6% and a remission rate of 35.0%, figures that align closely with traditional face-to-face CBT outcomes 42. Furthermore, a recent 2024 trial evaluating a smartphone-delivered DCBT program for adults with generalized anxiety disorder demonstrated a striking 71% remission rate at 10 weeks, compared to just 35% for a psychoeducation control group 43. These high engagement and remission metrics demonstrate that the structured, systematic nature of CBT is highly amenable to algorithmic delivery, representing a critical frontier for public health deployment.
Cultural Adaptations for Non-Western and Minority Populations
A persistent, structural critique of classical CBT is its inherent reliance on dominant Western cultural paradigms. The foundational models of CBT implicitly emphasize individualism, an internal locus of control, and logical empiricism. These frameworks may clash profoundly with the worldviews, coping mechanisms, and familial structures of interdependent, non-Western, or minority populations 444546.
In diverse communities, the rigid application of unadapted CBT is frequently correlated with higher dropout rates, misunderstandings of clinical symptomatology, and therapeutic ruptures caused by cultural microaggressions 4447. To mitigate these disparities, cross-cultural researchers have developed Culturally Adapted CBT (CA-CBT). Meta-analyses indicate that the depth of the adaptation dictates the clinical success of the intervention.
Surface Structure Versus Deep Structure Adaptations
Cultural adaptations are broadly categorized into two tiers:
- Surface Structure Adaptations: These involve superficial, logistical modifications designed to increase basic feasibility and accessibility. Examples include translating clinical materials into native languages, ensuring ethnic and linguistic matching between the therapist and the client, and incorporating culturally relevant metaphors or regional references into the therapy sessions 454648. While surface adaptations increase initial engagement, they do not fundamentally alter the mechanics of the therapy.
- Deep Structure Adaptations: These involve a fundamental restructuring of CBT's core theoretical constructs to accurately reflect the target population's socio-cultural, spiritual, and historical reality. Empirical meta-analyses demonstrate that deep structure adaptations yield significantly larger effect sizes and higher rates of treatment success compared to surface adaptations alone 444549.
Examples of successful deep structure adaptations include: * Asian Populations: Mental distress in Southeast Asian communities frequently presents via somatic (physical) symptoms rather than psychological complaints. Deep structure CBT for these populations explicitly validates these physical manifestations alongside cognitive restructuring, and modifies traditional assertiveness training to respect cultural values that prioritize family harmony and interdependence over individual autonomy 4957. * Latino Populations: Effective interventions have integrated concepts of machismo, gender roles, and family-centric values directly into the cognitive restructuring process, recognizing that systemic family dynamics often take precedence over individual cognitive distortions 48. * Indigenous and Tribal Communities: CA-CBT for Native American and Indigenous populations has successfully expanded the therapeutic framework to encompass the impact of specific historical trauma. Furthermore, these adaptations integrate traditional healing ceremonies, connection to the land, and the active involvement of community elders as vital components of the therapeutic support network 4849.
The Debate Surrounding the Gold Standard Designation
Despite its global dominance, the assertion that CBT is the undisputed "gold standard" is increasingly debated within the academic and clinical psychology communities. Some researchers suggest that CBT's perceived superiority is partially an artifact of methodological bias rather than unique therapeutic power 34.
Critics point to the stagnation of effect sizes over time. A longitudinal review of psychotherapy literature found that aggregate effect sizes for CBT in treating anxiety disorders have stagnated over the past four decades, while a slight, unexpected decline in overall efficacy has been observed in some modern trials for depressive disorders 34. This data contradicts the assumption that CBT is undergoing a process of continuous, linear clinical improvement.
Furthermore, the design of clinical control groups is frequently criticized. When CBT is compared to waitlist controls or "no treatment" arms, it invariably demonstrates massive superiority. However, when CBT is compared to active psychological placebos or alternative bona fide psychotherapies (such as interpersonal or psychodynamic therapy), the differences in effect sizes often shrink to negligible margins 734. Critics argue that the slight advantages sometimes observed for CBT in head-to-head trials are driven by "researcher allegiance effects" - meaning the researchers conducting the trial inherently favor CBT, which unconsciously biases trial design, execution, or therapist enthusiasm 3440. Additionally, trials comparing CBT to "treatment as usual" (TAU) often suffer from high dropout rates in the TAU arm, which can artificially inflate CBT's comparative effect size 21.
Despite these valid methodological critiques, the broader scientific and medical consensus maintains CBT's premier status. This is not because CBT guarantees a cure, but because its theoretical mechanisms are explicitly mapped to cognitive science, its structured format ensures rigorous testability, and it has been empirically validated across a vastly wider array of specific psychopathologies than any competing modality. Ultimately, cognitive behavioral therapy remains the most rigorously vetted, structurally adaptable, and fundamentally scalable psychological intervention available in modern medicine 7.