Science of virtual reality and one-session phobia treatment
Specific phobias are psychiatric conditions characterized by an intense, enduring fear of an identifiable object or situation that leads to profound anxiety symptoms, severe distress, and persistent avoidance behaviors. Diagnostic frameworks, such as the DSM-5, stipulate that these reactions must be out of proportion to the actual threat and persist for six months or longer to warrant a clinical diagnosis 1. Epidemiological data indicates that specific phobias affect between 5% and 10% of children and young people, while lifetime prevalence rates in adults range from 7.7% to 12.5% 2345. The economic and societal burden of these disorders is immense. In the United States alone, anxiety disorders and specific phobias account for an estimated $122 billion in lost productivity and $135 billion in direct healthcare costs annually 67.
Traditional psychological interventions based on cognitive-behavioral therapy (CBT) remain the dominant model for treating specific phobias. Standard in vivo exposure therapy relies on systematic desensitization, where a patient is gradually exposed to the phobic stimulus in real-world environments 3789. While clinically effective, multi-session in vivo CBT is constrained by severe logistical limitations. Treatment is time-consuming, expensive, and subject to high attrition rates 37. Research suggests that only 19% to 33% of patients treated for anxiety disorders receive in vivo exposure due to structural challenges, space requirements, and practitioner reservations 10. Furthermore, the anticipatory anxiety associated with confronting physical stimuli leads to high treatment refusal rates among patients 89. In response to these barriers, clinical research has rapidly advanced alternative exposure modalities. One-Session Treatment (OST) and Virtual Reality Exposure Therapy (VRET) have emerged as highly efficacious, resource-efficient alternatives that leverage the neurobiology of fear extinction to accelerate recovery.
Neurobiology of Fear Extinction and Memory Reconsolidation
The clinical efficacy of both OST and VRET is fundamentally governed by the neurobiological mechanisms of fear conditioning, memory retrieval, and extinction learning. A consensus within the neuroscience literature establishes that successful exposure therapy does not erase the original fear memory. Instead, exposure facilitates the formation of a new, competing inhibitory memory trace that suppresses the expression of the initial excitatory fear response 111213.
Amygdala Circuitry and Memory Destabilization
The architecture of fear acquisition and extinction involves complex interactions between the amygdala, the hippocampus, and the medial prefrontal cortex. The basolateral nucleus of the amygdala is critical for processing threat stimuli and storing fear memories. Experimental studies demonstrate that the pharmacological inhibition of Thy1-expressing neurons within the basolateral amygdala, or the disruption of noradrenergic projections from the locus coeruleus, successfully blocks fear memory reconsolidation 14. Additionally, distinct clusters of intercalated neurons govern the physiological fear state. Dorsal intercalated clusters respond during states of fear, whereas ventral clusters are activated during extinction learning, projecting inhibitory signals to the medial central amygdala 14.
The hippocampus, which is responsible for episodic memory and contextual processing, dictates the environmental retrieval of these memories. Memory destabilization reduces neuronal activity in the CA1 and CA3 regions. Interventions that block projections from the dorsal hippocampus to the prelimbic regions of the medial prefrontal cortex prior to memory retrieval prevent reconsolidation altogether 14. Clinical researchers have identified a specific "reconsolidation window" that typically lasts between 0.5 and 6 hours following the retrieval of a fear memory. During this brief period, the memory trace becomes malleable. Administration of amnesic agents, such as propranolol, during this window can disrupt the reconsolidation of the original fear memory 1114. However, if exposure to the stimulus is prolonged, the biological processes shift from memory disruption to the formation of a distinct extinction memory 11.
The Inhibitory Learning Model
Modern exposure protocols are increasingly designed around the Inhibitory Learning Model. Historically, exposure therapy relied on the principle of habituation, operating under the assumption that a patient's anxiety must naturally decline during a session to achieve fear reduction 1215. The Inhibitory Learning Model challenges this paradigm, positing that the original stimulus-threat association remains intact indefinitely. Because excitatory fear memories are highly durable and new inhibitory memories are relatively fragile, successful therapy depends on creating robust secondary learning experiences 1213.
Under the Inhibitory Learning Model, clinical efficacy is maximized by introducing "desirable difficulties" during exposure sessions 15. Therapists actively design scenarios that violate the patient's catastrophic expectations, focusing on building tolerance to anxiety rather than merely waiting for habituation 1215. The objective is to provide the patient with definitive proof that the feared outcome is highly improbable and that the physiological symptoms of panic are survivable 15. Both VRET and OST utilize these principles by massing intense, varied exposures to ensure the new inhibitory response is strong enough to compete with the legacy fear memory.
Clinical Architecture of One-Session Treatment
One-Session Treatment is a highly condensed, intensive variant of cognitive-behavioral therapy developed by Lars-Göran Öst. Rather than distributing exposure exercises across weeks or months, OST consolidates the therapeutic protocol into a single session maximized to three hours 1316.
Procedural Foundations of Massed Exposure
The OST protocol integrates graduated exposure, participant modeling, cognitive challenges, and behavioral reinforcement. The process begins with a functional assessment to establish the patient's fear hierarchy 31617. During the active exposure phase, the clinician utilizes participant modeling, demonstrating safe interaction with the phobic stimulus before inviting the patient to engage 1. The therapist facilitates joint approaches, gradually fading their own involvement until the patient can interact with the stimulus independently and their catastrophic beliefs are empirically disconfirmed 116. Controlled clinical studies examining OST for specific phobias have historically demonstrated a positive response rate of 76% or higher 16.
The ASPECT Trial Methodology and Outcomes
The most comprehensive validation of OST was conducted through the Alleviating Specific Phobias Experienced by Children Trial (ASPECT). Designed as a pragmatic, multi-center, non-inferiority randomized controlled trial, ASPECT evaluated the clinical effectiveness of OST against standard multi-session CBT 2318. The trial recruited 268 children and young people aged 7 to 16 years across 26 Child and Adolescent Mental Health Services sites and related agencies 21819. Participants were randomized equally to receive either OST (n = 134) or multi-session CBT (n = 134) 1820.
Clinical non-inferiority was primarily assessed using the Behavioural Avoidance Task at a six-month follow-up. The Behavioural Avoidance Task measures approach behavior on a standardized 0 to 10 scale, recording the number of steps a patient successfully completes toward the feared stimulus 220.
| Trial Population | Treatment Arm | Mean Behavioural Avoidance Task Score (6 Months) | Adjusted Mean Difference (CBT vs. OST) | 95% Confidence Interval |
|---|---|---|---|---|
| Intention-to-Treat (ITT) | CBT (n = 76) | 7.1 | -0.123 | -0.449 to 0.202 |
| Intention-to-Treat (ITT) | OST (n = 73) | 7.4 | -0.123 | -0.449 to 0.202 |
| Per-Protocol (PP) | CBT (n = 57) | 7.4 | -0.204 | -0.579 to 0.171 |
| Per-Protocol (PP) | OST (n = 56) | 7.6 | -0.204 | -0.579 to 0.171 |
The predefined standardized non-inferiority limit was set at 0.4. Because the upper bounds of the 95% confidence intervals for both the intention-to-treat and per-protocol populations were wholly below this 0.4 margin, the trial provided definitive statistical evidence that OST is clinically non-inferior to multi-session CBT 2318.
Secondary outcome measures, including the Anxiety Disorder Interview Schedule clinical severity rating, corroborated the primary findings. At the six-month follow-up, 73% of the intention-to-treat population in both arms still met the diagnostic criteria for a specific phobia, indicating that while functional approach behaviors improved significantly, complete diagnostic remission requires ongoing consolidation 3. No reliable statistical evidence of subgroup interactions based on phobia type or treatment preference was detected 3.
Economic Viability of One-Session Treatment
While achieving clinical equivalence with multi-session CBT, OST presents a markedly different health economic profile. The traditional multi-session model requires extensive clinical hours, contributing to long waiting lists and high institutional costs within public health systems 317. The ASPECT trial incorporated a nested health economic evaluation to quantify these differences.
Cost-Effectiveness and Quality-Adjusted Life Years
The economic analysis utilized the EQ-5D-Y and CHU-9D psychometric instruments to calculate Quality Adjusted Life Years alongside comprehensive service utilization questionnaires documenting healthcare, community service, and educational resource consumption 11821.
After adjusting for baseline imbalances and performing non-parametric bootstrapping, the data revealed that patients randomized to OST incurred lower overall health and social care costs. On average, the OST cohort incurred £302.96 less in incremental costs (95% CI -£598.86 to -£28.61) compared to the CBT cohort 231921. Concurrently, the OST group maintained similar, or marginally superior, utility improvements, gaining an incremental 0.002 Quality Adjusted Life Years (95% CI -0.004 to 0.008) 21921.
When plotted on a Cost-Effectiveness Acceptability Curve across standard willingness-to-pay thresholds, the probability of OST being the more cost-effective intervention exceeded 97% 221. At a willingness-to-pay threshold of £20,000 per Quality Adjusted Life Year, there was a 98% probability that OST was the optimal economic choice 3. Consequently, OST represents a highly scalable, cost-saving intervention that mitigates the strain on over-capacity mental health infrastructure.
Virtual Reality Exposure Therapy
Virtual Reality Exposure Therapy digitizes the mechanisms of the Inhibitory Learning Model by immersing patients in controlled, computer-generated simulations. By eliminating the necessity of sourcing real-world phobic stimuli, VRET circumvents the primary logistical limitations of in vivo exposure 78222324.
Efficacy Metrics and Meta-Analytical Data
The clinical efficacy of VRET has been validated across a broad spectrum of anxiety-related conditions. A comprehensive meta-analysis of 26 randomized controlled trials encompassing 1,649 clinically diagnosed participants evaluated VRET's impact on both self-reported symptomatic distress and objective behavioral mechanisms 25.
| Clinical Domain | Standardized Effect Size (Hedges' g) | 95% Confidence Interval | Statistical Significance |
|---|---|---|---|
| Phobia Symptom Reduction | -0.98 | -1.37 to -0.60 | P < 0.001 |
| General Anxiety Symptoms | -0.61 | -0.90 to -0.33 | P < 0.001 |
| Post-Traumatic Stress Symptoms | -0.51 | -0.72 to -0.30 | P < 0.001 |
| Approach Behavior | +0.62 | +0.11 to +1.12 | P = 0.02 |
The meta-analysis demonstrates that VRET yields large, significant reductions in specific phobia symptoms and moderate to large reductions in general anxiety and trauma symptomology 25. Crucially, VRET also drives a significant increase in approach behavior (Hedges' g = +0.62), validating its capacity to facilitate functional fear extinction 25. Moderator analyses within these trials indicated that shorter intervention durations - specifically sessions lasting under 60 minutes - were associated with the largest treatment effects on anxiety and phobia, likely due to optimized attention spans and the avoidance of cybersickness 25.
Comparison to In Vivo Exposure
Head-to-head comparative studies generally confirm that VRET is similarly efficacious to standard in vivo exposure 262728. Meta-analyses comparing the two modalities report negligible differences for specific phobias and agoraphobia 27. For Social Anxiety Disorder, VRET demonstrates significant, enduring efficacy, yielding a large effect size post-intervention (Hedges' g = -0.86) that persists reliably at three-month (Hedges' g = -1.03), six-month (Hedges' g = -1.14), and twelve-month (Hedges' g = -0.74) follow-ups 29.
However, the literature exhibits some heterogeneity regarding long-term non-inferiority. While short-term outcomes are heavily comparable, select meta-analyses suggest that VRET's efficacy may become marginally inferior to in vivo exposure for certain complex social phobias during extended follow-up periods 2930. Conversely, other analyses suggest a slight trend favoring VRET due to the precise environmental control it affords therapists 2728.
Augmented and Mixed Reality Exposure Interventions
While VRET isolates the patient within a fully simulated environment, Augmented Reality Exposure Therapy (ARET) and Mixed Reality Exposure and Response Prevention (MERP) overlay digital stimuli onto the patient's actual physical surroundings 31323333.
Clinical Outcomes in Mixed Reality
ARET has demonstrated reliable efficacy primarily in the treatment of small animal phobias, such as arachnophobia and entomophobia. By allowing the patient to perceive their real-world environment while interacting with a digital threat, ARET maintains a high degree of situational realism without requiring head-mounted total isolation 263133. Comparative studies show ARET is as effective as both VRET and in vivo exposure for specific small animal phobias, with no significant differences in behavioral avoidance task performance post-treatment 526.
The application of mixed reality has also been trialed for complex anxiety disorders, including contamination-related Obsessive-Compulsive Disorder. A randomized clinical trial evaluated a six-session MERP protocol against a self-guided exposure protocol. Participants in the MERP cohort demonstrated a mean reduction of 3.15 points on the Yale-Brown Obsessive Compulsive Scale, representing a medium to large effect (Cohen d = 0.584 to 0.931) 32. However, the trial highlighted a critical limitation of current mixed reality hardware: participants reported a relatively weak sense of digital presence, resulting in heterogeneous subjective appraisals of the therapy 32. Until hardware immersion improves, fully occlusive VRET remains the dominant digital modality.
Patient Acceptance and Treatment Attrition Dynamics
The logistical and psychological burdens placed on the patient diverge sharply across exposure modalities. Anticipatory anxiety prevents a significant portion of phobic individuals from initiating or completing in vivo exposure, whereas digital modalities often present a lower psychological barrier to entry 789.
Modality Preferences and Logistics
Survey data comparing patient perceptions of VRET and in vivo exposure indicate a strong preference for digital interventions. In a comparative cohort, 90.2% of participants reported a willingness to receive VRET, compared to 82% for in vivo exposure 6. Patients consistently reported higher perceived effectiveness, greater comfort, and increased enthusiasm for VRET 6.
While both modalities share an average clinical dropout rate of approximately 16%, the etiology of treatment attrition differs fundamentally 3436.
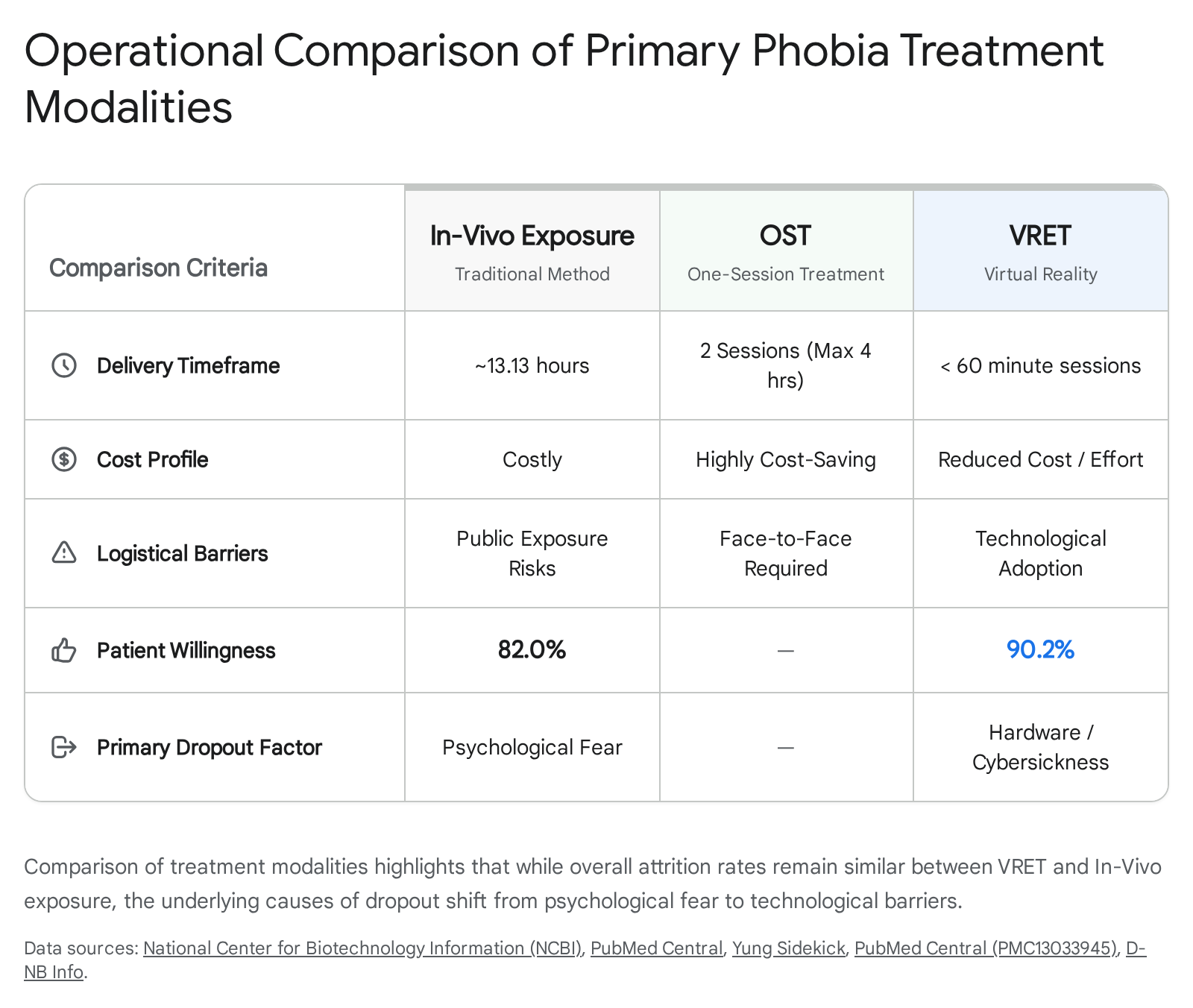
When patients withdraw from in vivo exposure, the primary driver is the intense psychological distress of confronting the physical stimulus, compounded by feelings of shame or embarrassment when exposure occurs in public settings 634. Conversely, attrition in VRET protocols is overwhelmingly driven by technological barriers, including failed immersion, vision complications, and the onset of cybersickness 34.
Cybersickness and Hardware Limitations in Virtual Reality
Despite resolving the logistical challenges of physical stimulus acquisition, VRET introduces hardware-dependent adverse events. Cybersickness remains the primary physiological barrier to prolonged virtual exposure, presenting as a constellation of symptoms mimicking motion sickness 363536.
Pathophysiology of Simulator Sickness
Cybersickness is typically assessed using the Simulator Sickness Questionnaire, which measures symptom severity across three domains: nausea, oculomotor discomfort, and disorientation 3637. Meta-analytical data indicates that specific low-level visual factors directly govern symptom intensity. The presence of visual oscillation, visually simulated off-vertical axis rotation, and multidimensional visual motion stimuli consistently exacerbate cybersickness 35. Conversely, engineering interventions such as peripheral field-of-view restriction and the inclusion of static, independent visual reference frames significantly attenuate symptom severity 35.
The degree of physical movement required by the user within the simulation also influences tolerability. In an observational study comparing two psychiatric VR simulations - an opioid overdose response scenario requiring high physical movement and a suicide risk assessment scenario requiring low movement - the high-movement simulation generated significantly higher mean nausea scores (4.59 out of 48) compared to the low-movement scenario (3.10 out of 48) 38. Notably, the required physical movement primarily impacted nausea, while oculomotor symptoms remained statistically similar across both simulations 38.
Anthropometric Hardware Discrepancies
Beyond software design, physical hardware limitations directly precipitate adverse events. Interpupillary distance mismatch - occurring when the optical lenses of the headset cannot accurately align with the user's anatomical eye spacing - is a primary driver of oculomotor strain and disorientation 37.
Legacy VR headsets often featured narrow or stepped interpupillary distance adjustment ranges, which systematically failed to accommodate the facial anthropometry of large population segments, particularly females of Asian, Caucasian, and African descent 37. Studies comparing hardware iterations demonstrate that upgrading from headsets with limited optical tracking (e.g., Meta Quest 2) to models featuring continuous eye-tracking and dynamic interpupillary adjustment (e.g., Meta Quest Pro) results in significant, measurable reductions in the total Simulator Sickness Questionnaire scores 37. Consequently, clinical implementation of VRET necessitates rigorous hardware evaluation to prevent anatomical mismatch from triggering treatment attrition.
Artificial Intelligence and Adaptive Therapeutic Environments
The efficacy of traditional VRET relies heavily on the therapist's manual control of the simulation. The integration of Artificial Intelligence transforms these static environments into responsive, closed-loop systems capable of dynamic exposure titration.
Closed-Loop Biometric Integration
Advanced AI-supported VRET frameworks utilize convolutional neural networks and machine learning algorithms to continuously analyze a patient's physiological state during exposure 4142. Wearable biosensors capture multimodal data streams, including Electroencephalography, Heart Rate Variability, and Electrodermal Activity 4139.
By processing this biofeedback in real-time, the AI infers the patient's emotional tolerance and dynamically adjusts the parameters of the virtual environment 414041. If the biosignals indicate an imminent panic response, the algorithm automatically reduces the intensity, realism, or proximity of the phobic stimuli to prevent re-traumatization and emotional overload 414041. As physiological resilience improves, the system incrementally increases exposure difficulty. This automated adaptation ensures that the patient remains within the optimal physiological window for inhibitory learning, thereby maximizing the efficacy of the session without requiring constant manual adjustment by the therapist 22413940.
Commercial Clinical Platforms
The transition from experimental laboratory setups to scalable clinical implementation is currently being driven by several commercially available AI-integrated software platforms.
| Platform Name | Target Architecture and Primary Clinical Functionality | Target Demographics and Conditions |
|---|---|---|
| oVRcome | Integrates VRET with generative AI to deliver self-guided or clinician-managed exposure programs via consumer smartphones or standalone headsets 424748. | Consumers, schools, and clinics targeting specific phobias and social anxiety 4247. |
| PsyTechVR | Provides advanced clinician-facing dashboards, modular session design, and integration with Eye Movement Desensitization and Reprocessing (EMDR) protocols 47. | Complex clinical presentations, including PTSD, OCD, and severe anxiety 47. |
| XRHealth | Combines immersive spatial data analytics with AI Creator Spaces, allowing therapists to procedurally generate highly customized treatment environments 43. | Clinical facilities treating trauma, phobias, addiction, and stress 43. |
| Rephobia | A therapist-led platform built strictly on CBT frameworks that tracks physiological responses to guide the patient through graded exposure in real time 50. | Clinical settings requiring evidence-based, data-driven specific phobia treatment 50. |
These platforms demonstrate the commercial viability of AI-driven VRET, shifting the modality from niche technological experimentation into standardized, reimbursable clinical practice.
Cross-Cultural Efficacy and Global Trial Infrastructure
The overwhelming majority of exposure therapy protocols were developed and validated within Western, high-income clinical settings 2544. The global burden of anxiety disorders necessitates adaptations that account for non-Western psychological constructs and regional infrastructural limitations.
Cultural Processing in Therapy
Because traditional CBT relies heavily on direct confrontation and specific cognitive reframing techniques, applying rigid, manualized treatments to diverse ethnic populations can lead to a cultural mismatch that dilutes treatment efficacy 44. To address this, researchers have developed culturally adapted protocols.
In a randomized pilot trial evaluating One-Session Treatment for phobic Asian Americans, researchers compared standard OST against a Culturally Adapted One-Session Treatment (OST-CA) 454647. The adapted protocol incorporated specific cultural modifications, such as emphasizing emotional control frameworks and leveraging a vertical, authoritative therapist-client relationship 4547. Follow-up data at six months indicated that while both treatments effectively reduced phobic symptoms, low-acculturation Asian Americans benefited significantly more from the culturally adapted protocol, demonstrating superior reductions in catastrophic thinking and general fear 4547. Similar localization efforts in China advocate for transitioning away from simple behavioral desensitization toward integrated "five-acceptance" psychotherapy strategies that align closely with native cultural paradigms .
Infrastructure and Refugee Interventions
Digital exposure modalities offer distinct advantages in regions lacking specialized psychiatric infrastructure or where profound cultural stigma surrounds mental health treatment. In the Middle East, VRET interventions have been successfully deployed for Syrian refugee women suffering from chronic, war-related post-traumatic stress disorder 48. A mixed-methods pilot study utilized a 13-session VRET program featuring culturally relevant auditory triggers, localized Arabic dialects, and 360-degree simulations of war-related environments 48. The intervention yielded a highly significant reduction in PTSD symptoms, with the mean PTSD Checklist (PCL-5) score dropping by 30.75 points (d = 2.89) 48. Qualitative data indicated that the enclosed nature of the VR headset shielded patients from community observation, effectively bypassing the severe social stigma that typically precludes treatment engagement in refugee populations 48.
Despite these localized successes, scaling clinical research across low- and middle-income countries faces systemic hurdles. The Middle East, Mediterranean, and Africa (MEMA) region currently hosts only 6% of worldwide registered clinical trials 49. This underrepresentation is driven by a lack of international standard regulatory frameworks, inadequate digital infrastructure, and a workforce lacking sufficient training in standardized clinical research methodology 495051. However, ongoing collaborative initiatives in countries like South Africa, Brazil, and Indonesia are increasingly prioritizing the development of native clinical trial infrastructure 49525354. By scaling regional trial capacity, these networks aim to validate and optimize brief exposure interventions for culturally diverse, medication-naive populations on a global scale.
Conclusion
The science of phobia treatment is undergoing a profound methodological shift, transitioning from protracted, in vivo habituation exercises to highly optimized, neurobiologically precise interventions. Driven by the Inhibitory Learning Model, therapeutic efficacy relies on the rapid, intense violation of catastrophic expectations to build resilient extinction memories. One-Session Treatment achieves this through intense, massed clinical collaboration, proving both clinically non-inferior and economically superior to standard multi-session CBT, presenting a highly scalable solution for strained public health systems. Concurrently, Virtual Reality Exposure Therapy digitizes this exposure process. By immersing patients in controlled environments, VRET eliminates the logistical barriers of physical stimulus acquisition and mitigates the anticipatory anxiety that drives treatment refusal. While challenges such as hardware-induced cybersickness remain, the integration of AI-driven biometric feedback loops and culturally adapted protocols ensures that these advanced modalities are positioned to democratize access to sophisticated, personalized mental healthcare globally.