Science and sociology of sleep deprivation in modern society
Sleep deprivation has emerged as one of the most pervasive and multifaceted public health challenges of the modern era, altering cognitive performance, metabolic regulation, and long-term neurobiological health. As post-industrial societies undergo rapid technological, environmental, and occupational transformations, human sleep architecture is experiencing unprecedented disruption. The intersection of clinical neurology, socio-environmental epidemiology, and macroeconomic modeling reveals that insufficient rest is not merely an individual behavioral failure but a systemic, structural deficit. The consequences of this deficit span from the molecular accumulation of neurotoxic proteins in the brain to trillions of dollars in lost global economic output.
Global Epidemiology of Sleep Duration
Epidemiological data collected across diverse geographies indicate a widespread deterioration in both the duration and quality of human sleep. While self-reported metrics often overestimate actual sleep duration, population-level surveys reveal significant deficits relative to the recommended seven to nine hours of nightly rest for adults.
Regional Disparities and the Asian Sleep Deficit
Recent multinational polling underscores a distinct geographic and cultural stratification in sleep habits. According to 2024 survey data analyzing sleep duration across 17 international markets, over half of the residents in the majority of these countries report sleeping seven or more hours on a typical night 1. However, the distribution of rest is highly uneven. Northern and Western European countries demonstrate the highest rates of sufficient sleep, with 67% of adults in Denmark and 65% in Germany reporting seven or more hours of nightly rest 1.
Conversely, populations in Asia and the Middle East report severe sleep constriction. Less than half of the residents in Indonesia (48%), the United Arab Emirates (45%), and Singapore (44%) achieve the recommended seven hours 1. The deficit is particularly acute in advanced East Asian economies. Japan and South Korea consistently record the lowest sleep durations and quality scores globally, with average nightly sleep durations falling below 6.5 hours and 6.25 hours, respectively 23. In Japan, over a fifth of the population reports experiencing only one or two nights of restorative sleep per week, positioning it as one of the most sleep-deprived nations in the developed world 4.
The Southeast Asian region presents a paradoxical relationship with sleep. While populations express a high cultural valuation of rest - with 73% of Indonesians viewing sleep as highly important and enjoyable - actual biological outcomes fail to match this sentiment 5. Scientific monitoring indicates that the average sleep duration in Indonesia is merely 6 hours and 36 minutes 56. This discrepancy highlights a critical disparity where structural and environmental barriers prevent individuals from achieving the rest they actively desire. Similar patterns are observed in the Philippines and Malaysia, where 56% and 42% of the respective populations report experiencing frequent sleep problems 37. In a peer-reviewed study of 11,356 working Malaysian adults, 54.7% were found to sleep less than the recommended seven hours, averaging 6.49 hours per night 3.
| Country | Percentage Sleeping < 6 Hours | Percentage Sleeping 6-7 Hours | Percentage Sleeping 7+ Hours | Regional Context |
|---|---|---|---|---|
| Denmark | 11% | 21% | 67% | Northern Europe |
| Germany | 12% | 22% | 65% | Western Europe |
| United States | 18% | 23% | 49% | North America |
| Singapore | 21% | 33% | 44% | Southeast Asia |
| Indonesia | 24% | 27% | 48% | Southeast Asia |
| Japan | >39% (Estimates vary) | N/A | <30% | East Asia |
Summary of reported typical nightly sleep duration across selected global markets based on 2024 multinational polling data. 137
Longitudinal Trends and Demographic Vulnerabilities
Longitudinal assessments demonstrate that the prevalence of sleep difficulty is accelerating globally. Between 2021 and 2025, the global proportion of individuals who report struggling with sleep (defined as sleeping well "a little, very little, or never") increased from 35% to 38% 8. In 35 out of 39 surveyed countries, more than a quarter of the population reports poor sleep, peaking in regions such as Hong Kong (59%), Chile (56%), and Brazil (52%) 8.
These declines are not distributed equally across demographics. Unemployed individuals exhibit significantly higher rates of sleep disruption, with 47% reporting poor sleep, illustrating the profound impact of psychosocial and financial stress on rest 8. Furthermore, women consistently report fewer nights of quality sleep than men (3.83 nights versus 4.13 nights per week) and face greater difficulties initiating sleep (38% versus 29%) 9. Hormonal transitions serve as a major exacerbating factor; 44% of menopausal and perimenopausal women experience frequent difficulties falling asleep 9. Additionally, 25% of perimenopausal women report symptoms of sleep apnea, an obstructive respiratory condition heavily underdiagnosed in female populations, with prevalence rising to 39% among perimenopausal women in India 4.
Youth populations are equally vulnerable. According to the National Sleep Foundation, more than 87% of high school students in the United States fail to get the recommended hours of sleep, a trend that continues to worsen 10. Similar constraints are observed in China, where preschool children in Shanghai average 9.05 hours of sleep per day, falling nearly an hour short of developmental recommendations 11.
Neurobiological Mechanisms of Sleep and Clearance
The transition from adequate sleep to chronic sleep deprivation triggers a cascade of neurophysiological impairments. Recent advancements in neuroimaging and biomarker analysis have shifted the scientific understanding of sleep from a state of passive rest to an active, non-redundant period of biological maintenance, primarily governed by the brain's unique fluid transport networks.
The Glymphatic System and Cerebrospinal Fluid Transport
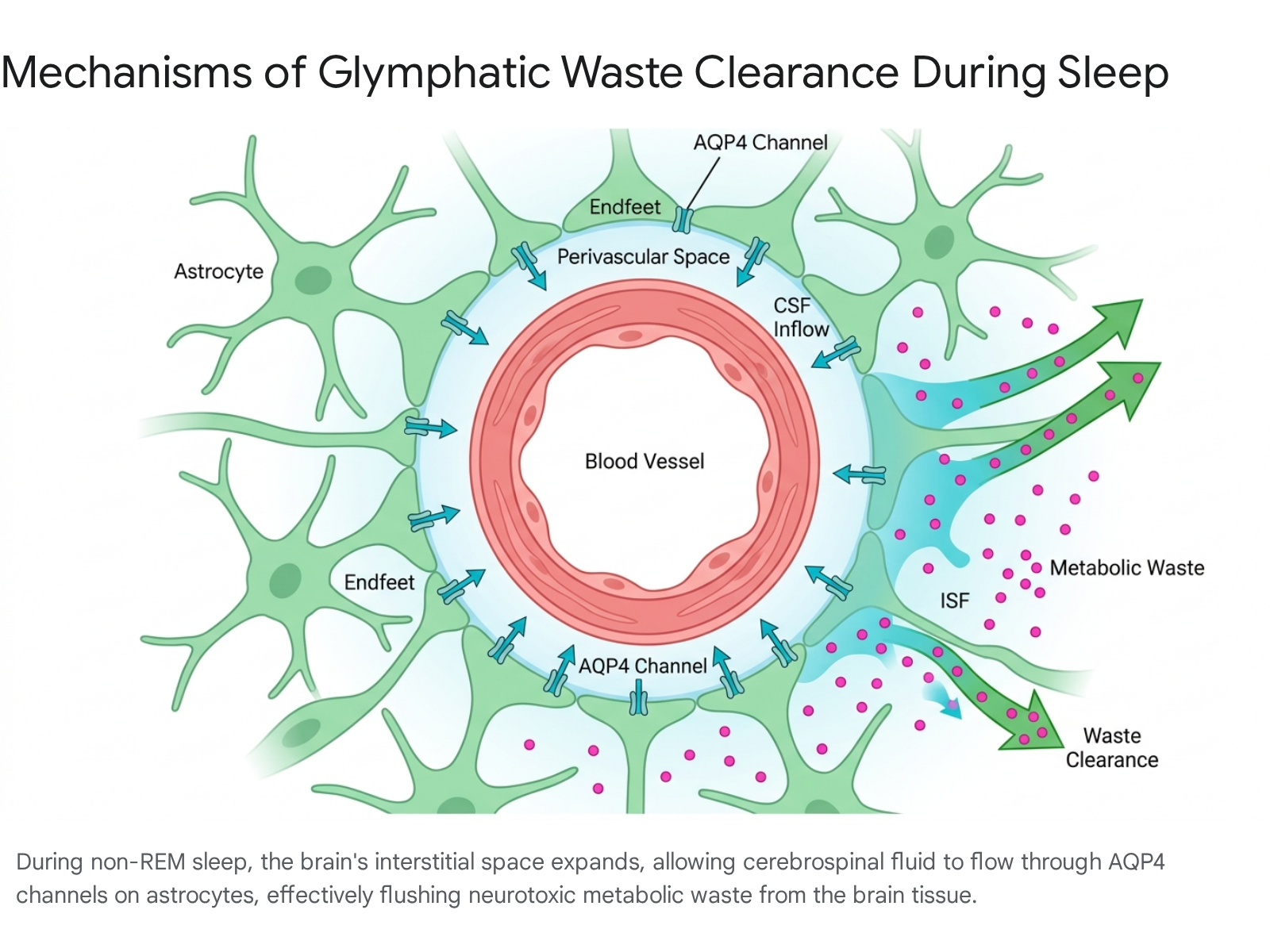
The human brain consumes approximately 20% of the body's metabolic energy, generating a substantial volume of metabolic waste 12. Because the central nervous system lacks a conventional lymphatic drainage network, it relies on a highly specialized paravascular pathway known as the glymphatic (glial-lymphatic) system to manage tissue homeostasis 121314. The glymphatic system facilitates the influx of cerebrospinal fluid (CSF) into the brain parenchyma along periarterial spaces. Once inside the tissue, the CSF mixes with interstitial fluid (ISF), collecting soluble proteins, signaling molecules, and metabolic byproducts 121314. This waste-laden fluid is subsequently propelled toward paravenous and perineural pathways, ultimately draining into the meningeal lymphatics and cervical lymphatic vessels for systemic clearance 1215.
The efficiency of this system relies heavily on aquaporin-4 (AQP4) water channels situated on the endfeet of astrocyte cells, which wrap around the blood vessels 1215. Crucially, glymphatic clearance is state-dependent; it is massively upregulated during deep, non-rapid eye movement (NREM) slow-wave sleep 131617. During natural sleep, a decline in noradrenergic tone (norepinephrine levels) prompts an expansion of the brain's extracellular space by up to 60% 121314. This structural shift drastically reduces tissue resistance, allowing for a surge in convective fluid transport 1314. Wakefulness, conversely, increases parenchymal resistance and suppresses glymphatic clearance by up to 90% 1314. Consequently, sleep deprivation acts as a mechanical bottleneck, preventing the brain from purging neurotoxic metabolic byproducts 1617.
Proteinopathies and Neurodegenerative Disease Pathogenesis
The impairment of glymphatic clearance is increasingly recognized as a core pathophysiological mediator in the initiation and propagation of neurodegenerative cascades 1617. Chronic sleep fragmentation - whether induced by behavioral choices, circadian rhythm disorders, or clinical conditions like chronic insomnia and obstructive sleep apnea (OSA) - creates a self-perpetuating cycle of neuroinflammation and protein accumulation 161718.
In Alzheimer's disease (AD), the failure of glymphatic clearance leads to the interstitial buildup of amyloid-beta (Aβ) plaques and neurofibrillary tau tangles 1318. Research utilizing diffusion tensor image analysis along the perivascular space (DTI-ALPS) - a non-invasive MRI biomarker for assessing glymphatic function - demonstrates that the ALPS index is significantly lower in patients with mild cognitive impairment and AD dementia compared to healthy controls 141920. A reduced ALPS index predicts accelerated amyloid burden, gray matter atrophy, and rapid clinical cognitive decline, suggesting that glymphatic failure frequently precedes overt amyloid pathology 19.
Parkinsonian Syndromes, Traumatic Brain Injury, and Amyotrophic Lateral Sclerosis
The relationship between sleep and brain clearance extends beyond Alzheimer's disease to encompass a spectrum of neurological conditions. In Parkinson's disease (PD), the accumulation of alpha-synuclein aggregates physically obstructs the perivascular spaces, reducing fluid clearance efficiency by roughly 30% 15. This obstruction is mechanistically linked to the matrix metalloproteinase-9 (MMP-9) mediated cleavage of beta-dystroglycan, which disrupts the necessary polarization of AQP4 water channels 15. This depolarization strips the glymphatic system of its fluid-pumping mechanism, creating a self-perpetuating cycle of impaired protein clearance and dopaminergic neurodegeneration 15.
Similar pathophysiological mechanisms are observed in Amyotrophic Lateral Sclerosis (ALS), where glymphatic impairment correlates with the accumulation of misfolded TDP-43 proteins and clinical disability progression 15. In Traumatic Brain Injury (TBI), physical injury often triggers a "noradrenergic storm" that suppresses glymphatic influx, leading to glymphatic-stagnated edema and the retention of toxic solutes 15. Disrupted sleep in these populations further correlates with systemic vascular damage and intermittent hypoxia, degrading the arterial pulsatility required to drive cerebrospinal fluid through the brain 1216. By establishing sleep as an active, modifiable factor in brain health, researchers emphasize that the global decline in sleep quality directly elevates population-level risks for widespread neurological decline 1617.
Macroeconomic Burden of Sleep Deprivation
The physiological damage inflicted by insufficient sleep scales rapidly to the macroeconomic level. When millions of individuals suffer from impaired cognitive function, elevated mortality risks, and heightened morbidity, the aggregate cost to national economies is profound. Economic models measuring the societal burden of sleep deprivation quantify losses through increased healthcare expenditures, diminished workplace productivity, and premature mortality.
Gross Domestic Product Contraction
A landmark cross-country comparative analysis by the RAND Corporation, alongside updated 2025 economic models, reveals that insufficient sleep drains hundreds of billions of dollars from advanced economies annually 2122. Across five major Organization for Economic Co-operation and Development (OECD) nations, the combined annual loss is estimated to exceed $680 billion 2324.
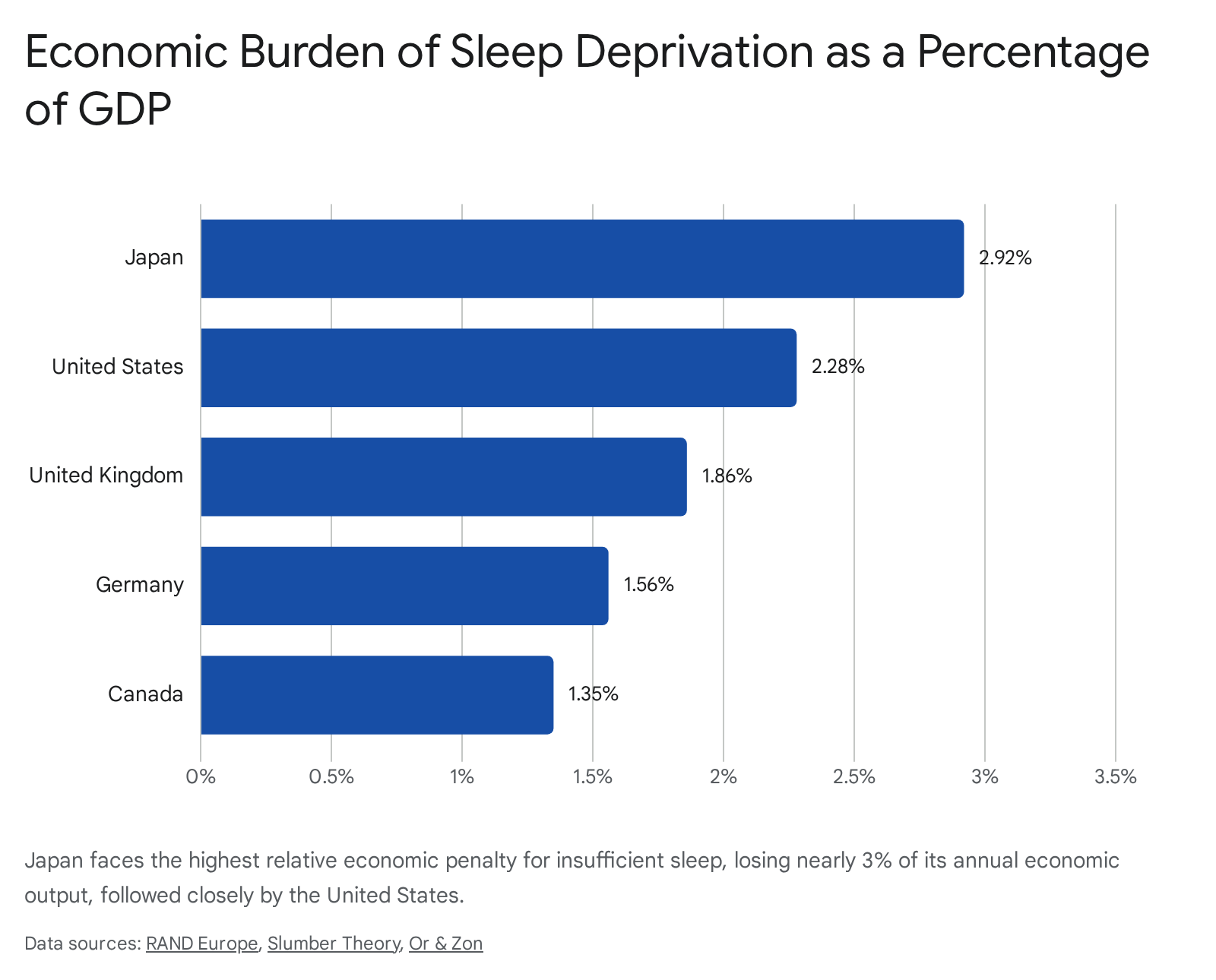
The United States sustains the highest absolute economic losses, forfeiting between $280 billion and $411 billion annually, representing roughly 2.28% of its Gross Domestic Product (GDP) 2225. In relative terms, Japan suffers the most severe macroeconomic impact; sleep deprivation costs the Japanese economy up to $138 billion a year, equating to an unparalleled 2.92% of its GDP 212226. Other major economies face similar penalties: the United Kingdom loses up to $50 billion (1.86% of GDP), Germany loses up to $60 billion (1.56% of GDP), and Canada loses approximately $21.4 billion (1.35% of GDP) 2122.
These macroeconomic figures remain highly conservative, as an estimated 80% to 90% of severe sleep disorders, such as obstructive sleep apnea, remain undiagnosed, generating massive hidden costs through comorbid cardiovascular and metabolic diseases 422. Direct healthcare costs for sleep disorders in the U.S. alone reach $94.9 billion annually, with individuals diagnosed with sleep disorders incurring an additional $7,000 in personal healthcare spending per year 2224.
Macroeconomic modeling in developing and middle-income nations highlights identical vulnerabilities. In Argentina, an Overlapping Generations (OLG) model projected that if the adult population consistently achieved the recommended minimum of seven hours of sleep, it would yield a 1.27% increase in the national GDP - an economic boost equivalent to 3.7 times the nation's total annual budget for science 27.
Absenteeism, Presenteeism, and Occupational Accidents
The mechanisms driving this economic contraction are primarily rooted in lost labor productivity, which manifests in two forms: absenteeism (employees missing work entirely) and presenteeism (employees functioning at reduced capacity while at work). The United States loses the equivalent of 1.23 million working days annually due to insufficient sleep, followed by Japan with 0.6 million lost working days 212628. Workers suffering from chronic insomnia cost employers an average of 14 absent days and 30 unproductive days per year 24.
Workers who sleep fewer than six hours per night report an average productivity loss that is 2.4 percentage points higher than those who achieve seven to nine hours of sleep 212628. This equates to losing an additional six working days over a standard 250-day work year 10. Surveys of global employees corroborate these economic models; 67% of workers in Asia explicitly link a lack of sleep to an impaired ability to focus and perform 29. An emerging metric of this exhaustion is the "snooze day" - a sick day taken specifically due to poor sleep. Within Asia, taking multiple snooze days annually is highly prevalent, reported by 92% of workers in India, 80% in China, 72% in Singapore, and 39% in Japan 29.
Beyond cognitive blunting, severe sleep deprivation translates into critical safety failures. In the U.S. alone, drowsy driving causes an estimated 91,000 crashes, 50,000 injuries, and 800 fatalities annually, generating a direct societal cost of $109 billion 24.
Occupational Structures and Systemic Sleep Loss
The epidemic of sleep deprivation cannot be solved solely through individual behavioral interventions because it is heavily dictated by modern occupational structures and evolving work cultures. When structural design consistently prioritizes continuous output over biological recovery, populations suffer systemic exhaustion.
Extreme Working Cultures and the 996 Schedule
Across various global industries, prolonged working hours have become a culturally enforced norm, fundamentally incompatible with healthy sleep architecture. A prominent example is the "996" work culture pervasive in China's technology and internet sectors, which mandates working from 9 a.m. to 9 p.m., six days a week, totaling a 72-hour workweek 303132. While originally championed as a driver of rapid economic innovation, epidemiological evaluations demonstrate that the 996 schedule extracts a severe physiological toll. The culture sparked the "996.ICU" digital protest movement on GitHub in 2019, metaphorically suggesting that adherence to such hours inevitably leads to the intensive care unit 31.
Extended working hours are an independent risk factor for insomnia and daytime sleepiness 33. A clear dose-response relationship exists: employees working 51 to 60 hours per week are twice as likely to suffer from severe daytime sleepiness compared to those working standard hours, and the risk quadruples for those working over 60 hours 33. The chronic stress and sleep disruption associated with such schedules significantly elevate the risks of burnout, major depression, obesity, and cardiovascular mortality 313234.
Similarly, Japan's occupational culture faces severe challenges with "social jet lag" - the misalignment between an individual's biological circadian rhythm and their socially imposed work schedule 35. This weekly disruption, akin to repeatedly traveling across time zones, induces daytime sleepiness, metabolic disturbances, and mental health decline, directly contributing to an estimated ¥1 trillion annual economic loss in Japan 35. In both regions, the expectation of round-the-clock availability supersedes the physiological requirement for rest 731.
Shift Work and Biological Misalignment
Non-standard work schedules, including rotating and night shift work, force employees to sleep during the day when the body's natural circadian alerting signals are highest. This misalignment results in reduced sleep efficiency, severe circadian disruption, and heightened susceptibility to metabolic syndrome and certain cancers 363738.
To combat Shift Work Sleep Disorder, emerging interventions attempt to artificially re-align biological clocks. Digital frameworks using wearable data have identified optimized patterns, such as "adaptive circadian split sleep," which schedules a main sleep period combined with a strategic late nap to maximize alertness during non-standard hours 3839. Additionally, tailored clinical guidelines now advise shift workers to utilize strategic 15-20 minute naps, employ bright light therapy during night shifts while restricting light exposure before daytime sleep, and carefully manage melatonin supplementation 39.
Remote Employment and the Blurring of Work-Life Boundaries
Concurrently, the post-2020 transition toward remote and hybrid work arrangements has subtly altered global sleep patterns. While working from home theoretically eliminates commute times - which currently average 31 minutes for full-time in-office workers - it frequently erodes the boundaries between professional and personal life 4041.
Studies monitoring sleep via wearable actigraphy technology reveal that hybrid and remote workers tend to shift their functioning to later hours. On days worked from home, individuals generally exhibit delayed bedtimes (averaging 14.7 minutes later) and delayed wake times (42.3 minutes later) compared to in-office days 4042. During the strict COVID-19 lockdowns in 2020, total sleep time generally increased, but sleep architecture was altered, showing less deep sleep and more light sleep 43.
In modern hybrid settings, the absence of a structured schedule and prolonged exposure to screen-based blue light late into the evening frequently disrupts melatonin secretion 42. Furthermore, 59% of remote workers schedule personal appointments during traditional work hours, leading to compensatory work late at night 41. This practice, along with "polyworking" (holding multiple jobs or side hustles, reported by 28% of employees), fragments sleep opportunities, sustains high stress levels, and prevents the nervous system from fully disengaging 41.
Environmental Determinants and Sleep Equity
The ability to achieve restorative sleep is highly stratified by socioeconomic status (SES) and geography. The concept of "sleep equity" recognizes that biological rest is heavily mediated by the Social Determinants of Health, including neighborhood infrastructure, financial stability, and environmental exposures 454445.
Urbanization, Light at Night, and Noise Pollution
Rapid global urbanization has altered the physical environments in which populations sleep. Exposure to light at night (LAN) and anthropogenic noise pollution from traffic, rail, and aviation directly fragments sleep architecture 454647. Sustained environmental noise above 65 decibels correlates strongly with elevated reports of insomnia, daytime dysfunction, headaches, and dizziness 4750.
In the developing world, urbanization frequently compounds sleep deprivation. A major study utilizing objective actigraphy in Chennai, India, found that low-income urban residents spent an average of eight hours in bed but achieved only 5.5 hours of highly fragmented sleep 48. This severe sleep inefficiency - comparable to the disruption caused by clinical insomnia or sleep apnea - was driven by high ambient heat, dense crowding, neighborhood noise, and psychological distress 48. Interestingly, research contrasting rural and urban environments in Mozambique found that while access to electricity delayed sleep onset by an hour, it did not necessarily shorten total sleep time if individuals could adjust their wake times accordingly 4950. This suggests that the rigid schedules of industrial urbanization, rather than the mere presence of artificial light, drive severe sleep truncation 49.
Socioeconomic Stratification and Sleep Deserts
In advanced economies, structural inequalities generate "sleep deserts" - underserved neighborhoods where conditions actively antagonize rest 51. Historically marginalized and "redlined" communities suffer from disproportionate exposure to particulate air pollution, high noise levels, inadequate housing, and pervasive ambient light 3651. For example, urban block groups with a high percentage of Black residents in the U.S. record average nighttime noise levels of 46.3 decibels, compared to 42.3 decibels in predominantly White block groups, contributing to significantly higher rates of suboptimal sleep trajectories 46.
An expansive analysis of the American Cancer Society's Cancer Prevention Study-3 (CPS-3) cohort, which tracked over 180,000 adults, confirmed that neighborhood deprivation is strongly associated with poor circadian health 52. Individuals living in the most economically deprived neighborhoods exhibited a 23% higher likelihood of obtaining less than seven hours of sleep compared to those in affluent areas 52. Individuals from low-SES backgrounds also face intersecting psychosocial barriers, including financial distress, unemployment, and higher rates of multi-morbidity 455354. These populations are subsequently diagnosed with sleep disorders at lower rates but suffer disproportionately from sleep-related metabolic and cardiovascular diseases 364555. Public health interventions demonstrate that addressing these root environmental causes is highly effective; urban investments such as park renovations and housing redevelopments have been shown to buffer against age-related sleep deterioration for residents living in close proximity 51.
Technology, Algorithms, and Behavioral Delay
The intrusion of digital technology into the nocturnal environment has engineered entirely new behavioral paradigms that actively antagonize the onset of sleep. Two prominent phenomena - doomscrolling and revenge bedtime procrastination - illustrate how modern psycho-social stressors hijack the human sleep-wake cycle.
Doomscrolling and the Autonomic Nervous System
"Doomscrolling" refers to the compulsive, extended consumption of negative or distressing digital content, typically on social media or news platforms 5660. Facilitated by platform design elements such as infinite scroll, autoplay, and algorithmically curated personalized feeds, users are stripped of natural psychological stopping points 5662.
Algorithms optimize for engagement by exploiting the brain's inherent negativity bias, utilizing variable rewards to trigger dopamine release while simultaneously serving content that spikes existential anxiety 6257. This sustained exposure to crisis media keeps the user's autonomic nervous system locked in a state of hyperarousal and "threat mode," severely impairing the parasympathetic winding-down process necessary for sleep initiation 62. Studies published in 2024 and 2025 link chronic doomscrolling not only to delayed sleep latency and fragmented sleep architecture but also to cognitive overload, emotional exhaustion, and the depletion of prefrontal cortex resources required for self-regulation 56.
Revenge Bedtime Procrastination
The phenomenon of "Revenge Bedtime Procrastination" (RBP) represents a distinct behavioral response to modern lifestyle pressures. RBP is defined as the deliberate decision to delay sleep to engage in unstructured leisure activities, despite recognizing the negative consequences of sleep deprivation the following day 585960.
Psychological analyses indicate that RBP is driven by a state of "low perceived daytime autonomy" and self-regulation depletion 6067. Individuals whose daytime hours are heavily commandeered by high-stress occupational duties, caregiving, or lengthy commutes reach the end of the day with depleted willpower. Late-night hours become the only available window to reclaim personal agency and engage in leisure 5867. Consequently, high-performing individuals intentionally sacrifice biological rest to restore psychological autonomy 67. Over time, this daily choice transitions into chronic sleep deprivation, worsening baseline stress and trapping the individual in a self-defeating cycle of exhaustion and insomnia 5861.
Anthropological and Historical Perspectives on Sleep
The modern conception that healthy sleep must consist of a single, unbroken eight-hour block is subject to significant historical and anthropological debate. Assessing how our ancestors slept provides crucial context for understanding modern sleep dysfunction.
The Pre-Industrial Biphasic Sleep Debate
Historian Roger Ekirch has prominently argued that prior to the Industrial Revolution and the advent of widespread artificial lighting, the dominant pattern of Western human sleep was segmented, or biphasic 626364. Analyzing centuries of diaries, medical texts, and court records, Ekirch found extensive references to a "first sleep" and a "second sleep," separated by an hour or more of nocturnal wakefulness 6364. During this waking interval, individuals engaged in quiet reflection, socialization, dream analysis, or household chores 6465.
This historical theory was bolstered in the 1990s by sleep scientist Thomas Wehr, who subjected participants to 14 hours of darkness per night to mimic pre-industrial winter conditions. Wehr found that participants naturally transitioned to a bimodal sleep pattern, consisting of two four-hour phases separated by an hour of quiet wakefulness, exactly matching Ekirch's historical archival findings 62. The consolidation of sleep into a single night-time block is therefore theorized to be a modern adaptation to the rigid schedules of industrial capitalism and the pervasive use of electric light, which prolonged waking hours and compressed the time available for rest 736667.
Critiques from Evolutionary Anthropology
However, the biphasic sleep theory remains contested within evolutionary anthropology. Studies observing modern pre-industrial equatorial hunter-gatherer societies, such as the Hadza in Tanzania or the Tsimane in Bolivia, suggest that these groups predominantly sleep in a single, consolidated bout, rarely exhibiting routine nighttime wakefulness 6567. Critics argue that segmented sleep may have been a socio-environmental adaptation specific to the extended winter nights of higher latitudes in Europe, rather than a universal ancestral biological trait 6567.
Despite this debate, historical and clinical consensus acknowledges that modern society's rigid expectation of eight continuous hours, coupled with extreme alarm-driven awakening, generates immense psychological pressure 3762. For many individuals suffering from middle-of-the-night awakenings, the anxiety of "failing" to achieve consolidated sleep exacerbates insomnia, whereas recognizing biphasic rhythms as a potentially natural biological variant can reduce sleep-related distress 6266. Ultimately, whether comparing modern humans to their European ancestors or to equatorial hunter-gatherers, it is unequivocally clear that the chronic deficits, artificial light disruptions, and psychosocial stressors imposed by contemporary globalized society are fundamentally misaligned with optimal human neurobiology.