The rubber hand illusion in body ownership and self-perception
Bodily self-consciousness - the intimate, pre-reflective experience that one's body belongs to oneself and is situated in a specific spatial location - has historically been conceptualized as a fixed, hardwired biological phenomenon. However, empirical investigations over the past two decades have fundamentally challenged this assumption, demonstrating that the sense of body ownership is a highly malleable construct. The brain actively and continuously generates the boundaries of the bodily self through the dynamic integration of multisensory signals. The foundational experimental paradigm for investigating this phenomenon is the rubber hand illusion, first documented by Botvinick and Cohen in 1998 123.
By systematically manipulating visual, tactile, and proprioceptive inputs, researchers have utilized the rubber hand illusion to map the neurobiological and computational foundations of the bodily self. The illusion has yielded profound insights into multisensory integration, predictive coding, the distinction between body ownership and motor agency, and the pathophysiology of various neuropsychiatric and neurological disorders. This report provides an exhaustive analysis of the rubber hand illusion, its methodological parameters, its neural correlates, the theoretical debates surrounding phenomenological control, and its broader clinical implications.
Theoretical Frameworks of Bodily Self-Consciousness
To understand the mechanics of the rubber hand illusion, it is necessary to differentiate between various components of bodily self-consciousness. The neurocognitive literature generally distinguishes between the "body schema," an unconscious, dynamic sensorimotor representation of the body used for guiding action, and the "body image," a conscious, conceptual, and perceptual representation of the body's appearance and spatial boundaries 45.
The Tripartite Model of Embodiment
The subjective experience of embodiment during bodily illusions can be structurally decomposed into three distinct sub-components. The first is body ownership, which is the pre-reflective feeling that a specific body part, or the body as a whole, belongs to oneself 36. The second component is self-location, defined as the spatial experience of where the conscious "I" is situated, which is typically localized within the physical borders of the biological body 78. The third component is the sense of agency, encompassing the feeling of motor control and the capacity to initiate and execute voluntary physical actions 910.
The classic passive rubber hand illusion primarily manipulates body ownership and self-location by recalibrating the proprioceptive localization of the limb. Subsequent modifications of the paradigm involving active movement manipulate the sense of agency, demonstrating that ownership and agency are computationally and anatomically distinct processes 911.
Predictive Coding and Bayesian Causal Inference
Contemporary computational neuroscience frames the rubber hand illusion within the frameworks of predictive coding and Bayesian causal inference 1213. According to these models, the brain functions as an inference machine, constantly generating predictions regarding the sensory consequences of the body's interaction with the external environment. When conflicting sensory information arises - such as feeling a tactile stimulus on a hidden hand while observing a paintbrush stroke a visibly artificial rubber hand - the brain seeks to minimize prediction errors 13.
If the temporal and spatial congruency between the visual and tactile inputs is highly correlated, the brain's Bayesian optimal solution is to infer a single common cause for both sensory events. Consequently, the visual information, which typically dominates human spatial perception, overrides the inherently noisier proprioceptive information. The brain updates its internal structural model, concluding that the rubber hand must be the physical hand. This resolution of the multisensory conflict triggers the subjective illusion of ownership 1214.
Methodological Foundations and Experimental Setup
The Standard Induction Paradigm
The classical induction of the rubber hand illusion requires a strictly controlled physical architecture to manipulate visual and somatosensory data streams.
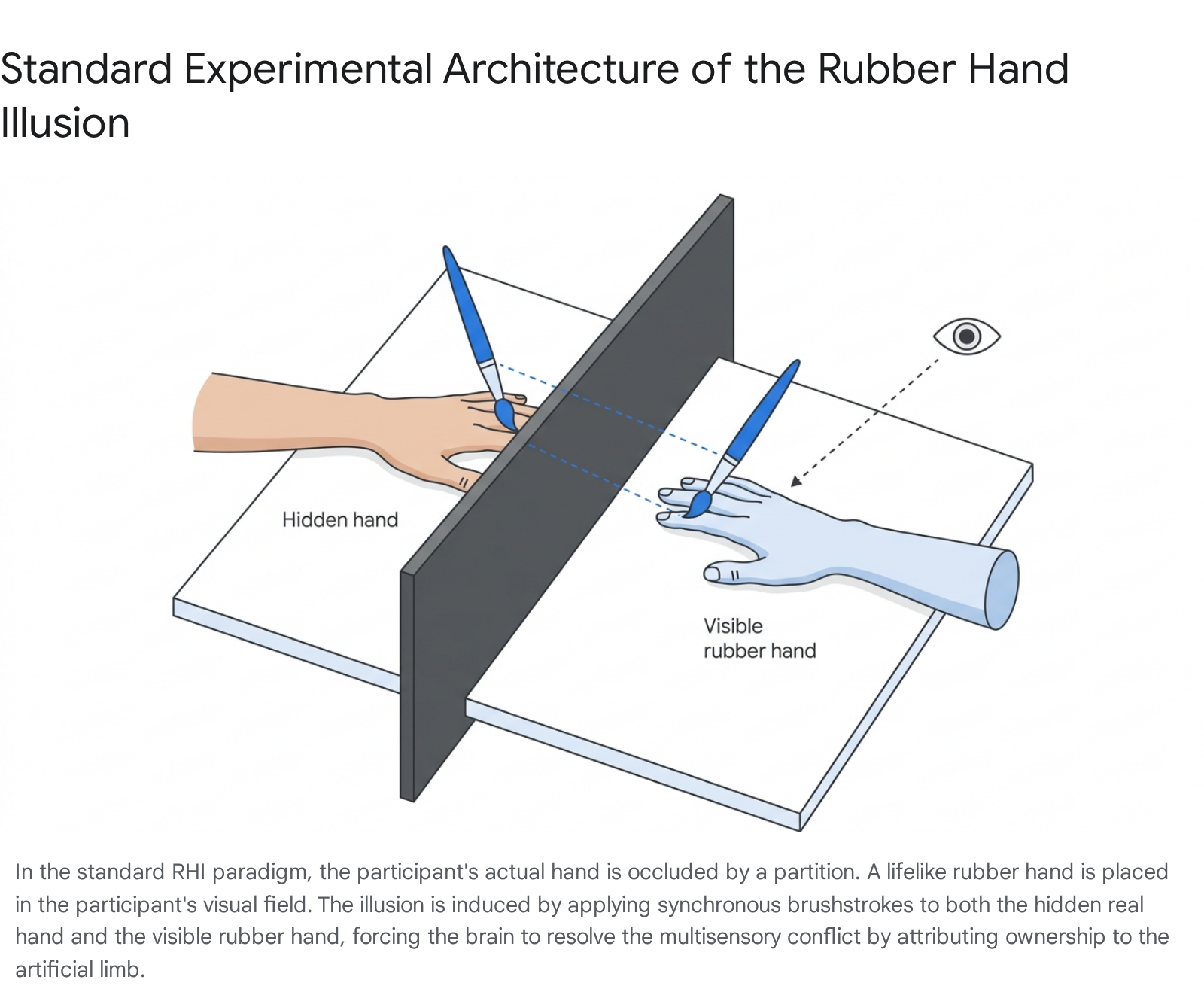
The participant is seated at a table with their target hand, most commonly the left hand, placed completely out of view behind a standing vertical partition or inside a specialized enclosed box 141516. A lifelike rubber or cosmetic prosthetic hand is positioned in front of the participant, typically aligned with their corresponding shoulder and placed approximately 15 to 30 centimeters away from the hidden biological hand 1617. A cloth or cape is frequently utilized to cover the proximal end of the rubber arm and the participant's shoulder to obscure the anatomical disconnect and enhance the visual plausibility of the artificial limb 1517.
An experimenter utilizes two small paintbrushes to apply tactile stimulation to the fingers or the dorsum of both the real hand and the rubber hand. In the synchronous condition, which serves as the experimental intervention, the brushstrokes are delivered simultaneously and in the exact same spatial pattern on both hands. Within an induction phase typically lasting between 10 seconds and two minutes, the vast majority of naive participants begin to experience the illusion 111518. Conversely, in the asynchronous condition, which serves as the standard control, a temporal delay - often ranging from 500 to 1000 milliseconds - is deliberately introduced between the touch observed on the rubber hand and the touch felt on the real hand 1419. This temporal mismatch disrupts the necessary conditions for multisensory integration, effectively preventing the subjective feeling of ownership from occurring in most subjects 36.
Quantitative and Qualitative Measurements
Researchers utilize a robust combination of subjective, behavioral, and physiological metrics to quantify the strength and presence of the rubber hand illusion across diverse populations.
| Measurement Type | Primary Metric | Methodological Description | Theoretical Implication |
|---|---|---|---|
| Subjective Evaluation | Self-Report Questionnaires | Participants rate agreement on a Likert scale for statements regarding feeling the touch on the rubber hand and ownership of the artificial limb 1420. | Quantifies the conscious, phenomenological experience of embodiment and ownership. |
| Behavioral Evaluation | Proprioceptive Drift | Participants blindly estimate the spatial location of their hidden index finger before and after induction. A shift toward the rubber hand is recorded in centimeters 1415. | Demonstrates the unconscious recalibration of the body schema and spatial self-location. |
| Autonomic Response | Skin Conductance Response (SCR) | A physical threat (e.g., a knife or hammer) is directed at the rubber hand. The resulting spike in electrodermal activity is measured 618. | Provides objective physiological evidence that the brain's threat-detection systems perceive the artificial limb as part of the biological body. |
| Thermoregulatory Response | Skin Temperature Modulation | Continuous temperature monitoring of the hidden real hand during the illusion reveals a limb-specific cooling effect 2122. | Suggests a top-down physiological "disowning" of the biological limb as ownership transfers to the rubber counterpart. |
| Motor System Response | Motor Cortical Excitability | Transcranial magnetic stimulation (TMS) is applied to the motor cortex. A drop in the strength of electrical pulses reaching the real hand is observed 2324. | Indicates that as the brain transfers ownership, it winds down its readiness to use the disembodied real hand. |
While proprioceptive drift and subjective ownership usually co-occur during standard inductions, advanced robotic and temporal tracking studies have demonstrated that they can be experimentally dissociated. Research involving highly frequent measurements of finger position using automated robotic arms demonstrated that proprioceptive drift can occur under visual-proprioceptive conditions alone, meaning participants looking at the rubber hand without any stroking may exhibit drift without feeling ownership 14. Furthermore, highly suggestible individuals may report strong subjective ownership without a corresponding increase in proprioceptive drift, implying that the behavioral and subjective dimensions of the illusion rely on partially distinct neurocomputational mechanisms 3.
Principles of Multisensory Integration
The rubber hand illusion operates strictly within the computational rules governing multisensory integration in peripersonal space. The brain's willingness to integrate disparate sensory streams into a unified percept depends on several foundational constraints regarding space, time, and probability 25.
Spatial, Temporal, and Auditory Constraints
For the illusion to successfully manifest, the visual and tactile stimuli must adhere to strict temporal synchrony. Empirical research indicates that as the temporal asynchrony between the seen touch and the felt touch exceeds a critical processing window of approximately 200 to 300 milliseconds, the probability of the illusion occurring drops precipitously 26.
Spatial congruency is equally vital to the integration process. The rubber hand must be placed in a position that the brain accepts as anatomically plausible. If the artificial limb is rotated 180 degrees so that it faces the participant, placed outside of near-personal space, or positioned at an impossible anatomical angle, the top-down body schema vetoes the bottom-up sensory integration, and the illusion fails entirely 3619. Furthermore, while vision and touch are the primary modalities, auditory inputs heavily influence the formation of the body representation. Experimental variants delivering synchronous auditory cues (e.g., the sound of the brushstrokes) significantly enhance the strength of the illusion, while asynchronous auditory cues diminish both subjective ownership and proprioceptive drift 27.
The Impact of Sensory Uncertainty
Bayesian integration theory posits that the central nervous system weights incoming sensory inputs based on their perceived reliability. If visual information becomes uncertain or noisy, the brain alters its weighting algorithms to rely more heavily on other available modalities. Data from augmented reality paradigms demonstrate that as visual noise increases, the brain relies more heavily on synchronous visuotactile timing, thereby increasing the overall probability of experiencing the illusion 12.
| Visual Noise Level (Sensory Uncertainty) | Resulting Illusion Prevalence |
|---|---|
| 0% Visual Noise (Baseline Clarity) | 93% Prevalence |
| 30% Visual Noise (Moderate Uncertainty) | 96% Prevalence |
| 50% Visual Noise (High Uncertainty) | 95% Prevalence |
This data supports Bayesian models of sensory integration. Under conditions of high visual uncertainty, it is computationally easier for the brain to mistake the artificial hand for the biological hand, as it assigns greater weight to the highly reliable temporal correlation of the tactile inputs 12. Classical descriptive models of the illusion fail to account for this phenomenon, making Bayesian probability the dominant paradigm for explaining bodily self-consciousness 12.
Neural Correlates of Bodily Self-Consciousness
Neuroimaging techniques, particularly functional Magnetic Resonance Imaging (fMRI) and electroencephalography (EEG), have successfully mapped the neuroanatomical networks responsible for processing the rubber hand illusion. The sense of body ownership does not reside in a single localized brain region but emerges from a distributed frontoparietal and occipitotemporal network working in concert 36.
The Frontoparietal Multisensory Network
The core neuroanatomical axis of multisensory integration for body ownership lies in the reciprocal connections between the posterior parietal cortex and the ventral premotor cortex 31828.
The Intraparietal Sulcus (IPS) acts as a primary hub for transforming unimodal sensory inputs - vision, touch, and proprioception - into a cohesive, body-centered reference frame. Neurons in this region possess highly specialized bimodal and trimodal receptive fields that map the peripersonal space immediately surrounding the limbs 725. Activity in the IPS correlates strongly with the spatial remapping processes associated with proprioceptive drift 3.
The Premotor Cortex (PMC) is responsible for evaluating the spatiotemporal congruence of the signals relayed from the parietal lobe. The subjective feeling of body ownership - the conscious phenomenological realization that the artificial limb is part of the self - is most directly and consistently correlated with Blood-Oxygen-Level-Dependent (BOLD) activation in the ventral premotor cortex 329. When multisensory conflicts are successfully resolved in favor of the rubber hand, the premotor cortex integrates this external object into the neural representation of the body schema 3.
The Temporoparietal Junction and Extrastriate Body Area
Beyond the frontoparietal network, other higher-order regions play critical roles in self-other differentiation and the processing of the body in space. The Temporoparietal Junction (TPJ), encompassing the supramarginal gyrus and angular gyrus, is deeply involved in updating the structural model of the body, distinguishing the self from others, and maintaining global self-location 33030. Electrical stimulation or dysfunction of the TPJ is known to induce severe out-of-body experiences 31. During complex bodily illusions, the TPJ acts as an error-detection center, processing the mismatch between expected and actual sensory inputs to construct a coherent world-centered reference frame 330.
Additionally, the Extrastriate Body Area (EBA), located in the occipitotemporal cortex, responds selectively to visual representations of the human body. During third-person full-body illusions, the EBA shows significant modulation, indicating its essential role in the visual receptivity to external body forms and the processing of allocentric body parts 31.
Disentangling Ownership and Agency: The Moving Paradigm
The classic rubber hand illusion relies on passive tactile stimulation. However, the "moving rubber hand illusion" introduces voluntary or passive movement into the experimental design. In this paradigm, the participant's hidden hand is mechanically linked to a visible artificial hand. When the participant moves their biological finger, the artificial finger moves in exact synchrony 1128.
This setup allows researchers to neuroanatomically disentangle the correlates of ownership (the feeling that the hand belongs to the self) from agency (the feeling of controlling the hand). fMRI studies of the moving paradigm reveal a clear functional segregation: perceived hand ownership is associated with activity in the premotor, posterior parietal, and cerebellar regions, identical to the classic passive illusion. In contrast, the sense of agency over the movements is distinctly linked to activity in the dorsal premotor cortex and the superior temporal cortex 9. This dissociation proves that the human brain computes somatic identity and motor volition through overlapping but anatomically distinct networks.
Variations and Extensions of the Bodily Illusion Paradigm
The foundational principles of the rubber hand illusion have been creatively adapted by neuroscientists to manipulate the ownership of different body parts and even the entire physical self, revealing the extraordinary plasticity of the brain's representation of the body.
The Invisible Hand Illusion
Perhaps the most striking theoretical variation is the "invisible hand illusion," pioneered by Guterstam and Ehrsson in 2013 183233. In this paradigm, the experimenter applies synchronous brushstrokes to the participant's hidden real hand and to a discrete volume of entirely empty space in front of the participant 1828.
Remarkably, despite the visual system explicitly confirming that no physical hand exists in that space, participants experience the profound sensation of possessing an invisible hand 1833. This illusion generates the same physiological stress responses, including skin conductance spikes when a knife is thrust into the empty space, and activates the identical premotor-intraparietal circuit as the classic rubber hand illusion 1832. The invisible hand illusion proves that the brain does not strictly require an anatomical, human-like object to generate a sense of limb ownership; the precise spatiotemporal correlation of visuotactile and proprioceptive signals alone is computationally sufficient to redefine the spatial boundaries of the bodily self 3233.
Full-Body and Body-Swap Illusions
Researchers have successfully scaled the mechanisms of the local illusion to encompass the entire body using Virtual Reality (VR) and Head-Mounted Displays (HMDs). In the Full-Body Illusion or Body-Swap Illusion, participants view a virtual avatar or a live video feed of another person's body from either a first-person or third-person perspective 163435. When the experimenter applies synchronous tactile stimulation, such as stroking the back or torso, to both the participant's real body and the virtual body, participants experience a massive shift in self-location and report ownership over the avatar 7836.
These full-body paradigms have shown that self-identification and self-location can be decoupled from the physical body, a process mediated by gamma and alpha band oscillations in the right TPJ and medial prefrontal cortex 7. Manipulating visuo-vestibular cues within these virtual environments, such as altering the visual perception of gravity, further demonstrates that the brain relies on vestibular inputs to lock the conscious self into a specific spatial coordinate 8.
The Enfacement Illusion
The principles of multisensory integration also apply to facial representation, heavily linking physical body ownership to psychological self-identity. In the Enfacement Illusion, a participant looks into a mirror or at a monitor showing another person's face. An experimenter synchronously strokes the participant's cheek and the corresponding cheek of the face on the screen 1338.
Following synchronous stimulation, participants experience a quantifiable blurring of self-other boundaries. When asked to recognize their own face in a morphing continuum between themselves and the stranger, participants who underwent the illusion are significantly more likely to accept the stranger's features as their own 13. Neural imaging shows that the enfacement illusion modulates activity in the intraparietal sulcus, the TPJ, and the inferior occipital gyrus, including the Occipital Face Area and Fusiform Face Area 29373839. This indicates that multisensory integration can alter high-level visual representations of personal identity, creating a mirror-mask effect where the subject's self-concept becomes remarkably fluid 38.
The Phenomenological Control and Suggestibility Controversy
Despite the widespread acceptance of the multisensory integration model across the neuroscience community, the rubber hand illusion has recently been the subject of intense methodological and theoretical debate regarding the role of psychological suggestibility and experimental demand characteristics.
The Demand Characteristics Hypothesis
In 2020, Peter Lush and colleagues published a series of highly scrutinized studies challenging the foundational validity of the rubber hand illusion and its standard control conditions. Lush argued that the illusion is not a purely perceptual phenomenon, but is primarily driven by "phenomenological control" - the imaginative capacity of a subject to alter their subjective experience to meet implicit task expectations, a trait heavily related to hypnotic suggestibility 224041.
Utilizing large sample sizes, Lush found substantial correlations between trait suggestibility, measured by the Sussex-Waterloo Scale of Hypnotizability (SWASH), and reported experiences of the illusion. Furthermore, Lush demonstrated that when naive participants merely read detailed descriptions of the synchronous and asynchronous conditions without actually experiencing them, they accurately predicted that the synchronous condition would produce the illusion 224042. Lush concluded that the standard asynchronous control condition is fundamentally flawed because it does not control for demand characteristics; participants simply report what they expect the experimenter wants to happen 404142.
The Multisensory Integration Defense
In a major 2022 rebuttal published in Nature Communications, Henrik Ehrsson and an international consortium of leading embodiment researchers sharply criticized Lush's conclusions and defended the perceptual basis of the illusion 222643. Through exhaustive reanalysis of Lush's own datasets, Ehrsson and colleagues demonstrated that the rubber hand illusion cannot be reduced to a hypnotic suggestion effect.
Ehrsson's counterarguments established several critical data points that reaffirmed the classical model. First, the data showed resilience across suggestibility spectrums. Even participants with the lowest possible scores on hypnotic suggestibility - the bottom quartile of the SWASH scale - still exhibited a robust and statistically significant difference in illusion ratings and proprioceptive drift between the synchronous and asynchronous conditions 2643. The multisensory effect dominates the perceptual experience regardless of trait suggestibility.
Second, the reanalysis highlighted the nonspecificity of hypnotizability. While trait suggestibility accounted for a minor variance of approximately 9% in subjective ratings, it accounted for similar variance in the asynchronous control condition and in completely unrelated control statements regarding impossible visual hallucinations. This indicates that suggestibility has a broad, non-specific influence on questionnaire-answering behavior generally, rather than uniquely driving the neurophysiological mechanisms of the illusion 26.
Finally, explicit verbal suggestions predicting that the asynchronous condition would produce the stronger illusion completely failed to override the fundamental multisensory rules; participants invariably experienced the illusion only in the synchronous condition 26. The scientific consensus maintains that while high-level expectations can slightly modulate questionnaire responses, the core mechanism of the rubber hand illusion remains firmly rooted in bottom-up multisensory integration restricted by precise temporal rules that defy pure top-down cognitive expectancy 26.
Clinical and Psychopathological Perspectives
The malleability of bodily self-consciousness demonstrated by experimental illusions provides a powerful diagnostic and theoretical lens for understanding various psychiatric and neurological conditions characterized by a disturbed sense of self.
Schizophrenia and Aberrant Self-Other Differentiation
Schizophrenia is frequently characterized by profound disturbances in self-awareness, leading to symptoms such as thought insertion, auditory hallucinations, and somatic delusions. Research using the rubber hand illusion has revealed that individuals with schizophrenia exhibit a significantly more flexible and easily perturbed sense of body ownership compared to healthy controls 2130.
During experimental protocols, patients with schizophrenia often experience the illusion faster, more intensely, and crucially, they frequently report experiencing the illusion even during asynchronous stimulation 21. This indicates a systemic breakdown in the precise temporal processing windows required for accurate multisensory integration. These abnormal embodiment responses correlate strongly with positive symptoms, such as delusions and hallucinations, measured by the Scale for the Assessment of Positive Symptoms (SAPS), as well as with positive and negative schizotypy 21. Neuroimaging via the enfacement paradigm reveals that this breakdown is functionally linked to structural abnormalities and reduced activation in the right temporoparietal junction, impairing the patient's ability to maintain rigid self-other boundaries and contributing directly to the lack of clinical insight often seen in the disorder 103044.
Somatic Delusions and Body Integrity Identity Disorder
Neurological damage, particularly right hemisphere strokes affecting the parietal and insular networks, can induce severe somatic delusions. Conditions such as somatoparaphrenia - the delusional belief that one's biological limb belongs to someone else - and asomatognosia - the explicit denial of the existence of a limb - are closely related to the mechanisms of experimental illusions 2. These conditions demonstrate what occurs when damage to multisensory integration hubs prevents the brain from updating the body schema with immediate sensory feedback, causing a permanent disconnect between the physical body and the central representation 24.
A highly specific and related psychiatric condition is Body Integrity Identity Disorder (BIID), also historically termed apotemnophilia, in which individuals experience an intense, distressing desire to amputate a perfectly healthy limb. BIID patients report a feeling of "overcompleteness," claiming that the targeted limb feels alien and does not belong to their true body shape 45. Neurological models suggest that BIID arises from an analogous congenital or functional failure in the multisensory integration networks of the premotor and parietal cortices. The physical sensory inputs from the limb fail to map onto the brain's innate, hardwired body map, leading to a profound, enduring mismatch between the mental representation and the physical body shape 445.
Body Image Disturbances in Eating Disorders
Eating disorders, such as Anorexia Nervosa, are characterized by rigid, distorted internal body representations maintained by hyper-precise high-level priors. Patients hold an unshakable belief regarding their bodily dimensions despite severe physical evidence to the contrary. Studies utilizing full-body and enfacement illusions have shown that exposing patients to congruent visuotactile stimulation over average-sized or differently shaped virtual avatars can induce strong prediction errors in the brain 1336.
These prediction errors force the central nervous system to momentarily update its rigid priors, temporarily alleviating body image disturbances 13. The enfacement illusion further demonstrates that patients with eating disorders suffer from wider disruptions in self-representation that extend beyond body fat estimation to encompass facial identity and overall self-other boundaries, suggesting a generalized deficit in multisensory body representation 13.
Neurorehabilitation and Prosthesis Embodiment
Understanding the perceptual principles of the rubber hand illusion is actively transforming the field of neurorehabilitation. For individuals with amputations, the successful daily use of a prosthesis depends heavily on "embodiment" - the extent to which the brain accepts the artificial limb as part of the body rather than an external, cumbersome tool 46.
Researchers have adapted illusion protocols to train patients during the critical preprosthetic phase. By using surface electromyography (EMG) to control a virtual prosthesis while simultaneously receiving synchronous vibrotactile feedback on the residual stump or shoulder, amputees can be trained to cognitively embody the device before being fitted with a physical limb 46. This visuotactile and visuomotor integration not only minimizes prosthetic rejection rates but also reduces phantom limb pain by reorganizing the maladaptive cortical maps in the somatosensory and motor cortices 2446. Similar Extended Reality (XR) paradigms are increasingly utilized in stroke rehabilitation to rebuild accurate body schemas and facilitate sensorimotor recovery in hemiplegic patients 547.
The Modulatory Role of Interoception
While the rubber hand illusion relies almost exclusively on the manipulation of exteroceptive signals, such as vision and touch, the overarching stability of the bodily self is anchored by interoception - the brain's perception and integration of internal bodily states, including heartbeat, respiration, and visceral sensations 4849.
Research assessing Interoceptive Accuracy (IAc), frequently measured by heartbeat counting tasks, reveals a stark inverse relationship between internal physiological sensitivity and external perceptual malleability. Individuals with high interoceptive accuracy possess a highly stable, internally anchored body representation. Consequently, they are significantly less susceptible to the rubber hand illusion, the enfacement illusion, and full-body manipulations 49. Their brains inherently assign higher precision weighting to internal physiological signals over conflicting external visuotactile inputs, effectively restricting the boundaries of their peripersonal space 49. Conversely, individuals with low interoceptive accuracy rely heavily on external visual cues to define their bodily boundaries, resulting in significantly greater susceptibility to body transfer illusions 4849. This dynamic underscores that normal bodily self-consciousness requires a continuous, delicate equilibrium between interoceptive stability and exteroceptive adaptability.
Conclusion
The rubber hand illusion has fundamentally shifted the paradigm of cognitive neuroscience away from the assumption that the bodily self is an immutable biological given. Instead, bodily self-consciousness is proven to be an active, ongoing computational process - a highly sophisticated Bayesian inference wherein the brain constantly weights and integrates visual, tactile, and proprioceptive data to determine the spatial and identity boundaries of the self.
Through the manipulation of temporal and spatial sensory congruency, the rubber hand paradigm and its advanced technological variants - from invisible hands to full virtual avatars - have mapped a complex frontoparietal and occipitotemporal network responsible for distinguishing the self from the external world and motor agency from body ownership. While debates regarding the influence of top-down suggestibility have refined experimental controls and heightened methodological rigor, the core phenomenon remains a robust artifact of fundamental multisensory integration. As clinical applications expand, leveraging the mechanics of these illusions holds profound therapeutic potential for rectifying the distorted body schemas present in schizophrenia, eating disorders, stroke, and amputee rehabilitation, ultimately providing clinical pathways to recalibrate the very experience of human selfhood.