Psychophysiological measurement and theory of emotion
1. Introduction
The study of psychophysiology has historically sought to map the body's peripheral physiological responses to subjective emotional experiences. For over a century, the field was dominated by classical frameworks, tracing back to the James-Lange theory, which posited that physiological arousal precedes and inherently defines emotional experience. Subsequently, basic emotion theories argued for the existence of universal, biologically hardwired "fingerprints" for discrete emotions such as anger, fear, sadness, and disgust 1. Under these classical models, researchers pursued the identification of invariant neural circuits and highly specific autonomic nervous system profiles corresponding to these predefined emotional categories, assuming that a specific emotion would universally elicit a specific pattern of heart rate, skin conductance, and respiration 123.
However, contemporary neuroscience and psychophysiological research from 2023 onward have precipitated a massive paradigm shift. Exhaustive historical background debates over basic emotion theories are increasingly deprioritized in favor of modern, data-driven frameworks. The search for invariant physiological fingerprints has largely been superseded by models emphasizing predictive coding, allostasis, and the dynamic, context-dependent construction of emotion 345. Concurrently, the landscape of physiological measurement has been transformed by the proliferation of consumer-grade wearables, which have begun matching - and in some specific nocturnal contexts, exceeding - the practical validity of clinical-grade tools, thereby enabling the continuous ambulatory assessment of autonomic indicators 6798. Furthermore, the globalization of psychological research has illuminated profound cultural variations in how emotions are regulated, physiologically expressed, and socially constructed, challenging the notion of universal biological emotional responses 91011.
This comprehensive research report delineates the modern psychophysiology of emotion. It provides an exhaustive analysis of the foundational tenets of the Theory of Constructed Emotion, evaluates the underlying mechanisms of autonomic indicators, critically reviews the recent 2026 scientific consensus surrounding the Polyvagal Theory, analyzes recent developments in wearable biometric technology versus clinical-grade instrumentation, and synthesizes robust cross-cultural findings regarding the physiological manifestation of emotion.
2. Neurobiological and Theoretical Paradigms: The Shift to Constructed Emotion
2.1 The Departure from Autonomic Fingerprints and Typological Thinking
Classical basic emotion theory operates on an inductive assumption rooted in typological thinking: because humans experience emotions as distinct categories, there must exist distinct, innate neural and physiological essences underpinning them 112. This framework implies that an instance of fear should universally elicit a highly specific, repeatable pattern of autonomic arousal. However, extensive meta-analyses of peripheral psychophysiology and neuroimaging have consistently failed to isolate these purported biological essences. Recent investigations have definitively demonstrated that there is no one-to-one mapping between an emotion category and a specific autonomic nervous system response pattern 212.
Instead of an invariant fingerprint, autonomic changes during emotion represent a population of highly variable, context-sensitive instances tailored to the specific action demands of a given situation 212. This shift mirrors the biological transition from typological thinking to population thinking. Variation among instances of a single emotion category (e.g., the physiological difference between freezing in fear versus fleeing in fear) is no longer viewed as statistical noise or experimental error, but rather as a structured, meaningful feature of the nature of emotion itself 212. Heart rate may increase, decrease, or remain stable during occurrences of anger depending entirely on what the individual's brain predicts the body must do next to cope with the environment 12.
2.2 The Theory of Constructed Emotion (TCE)
Developed prominently over the last decade and rigorously expanded in recent 2024 and 2025 literature, the Theory of Constructed Emotion (TCE) reconceptualizes emotions not as innate, hardwired reactions to external stimuli, but as dynamic, active constructions created by the brain 41516. According to the TCE, the brain continuously integrates internal bodily signals (interoception) with external sensory information (exteroception) and learned conceptual knowledge (derived from culture, language, and past experiences) to create a situated emotional experience 4515.
The fundamental psychological ingredients of emotion are not distinct neurological circuits located in subcortical regions, but rather "core affect" - a basic, continuous representation of the body's internal state defined by dimensions of valence (pleasure versus displeasure) and arousal (activation versus deactivation) 51517. The brain utilizes emotion concepts, which are heavily influenced by linguistic and social norms, to categorize these continuous affective fluctuations 1513. A word or concept serves as an abstract feature of equivalence for an ad hoc emotion category, helping an individual learn that vastly different physiological signal patterns can serve the same functional goal in a given context 12. Therefore, emotions do not passively happen to an individual; they are actively constructed psychological events resulting from the brain's attempt to make meaning of interoceptive and exteroceptive sensations 51614.
Recent advances in artificial intelligence further validate this framework. In 2026, researchers successfully developed a computational model based on the TCE using multilayered multimodal latent Dirichlet allocation (mMLDA). By feeding the model unlabeled physiological data (interoception proxies like heart rate) alongside visual and auditory data (exteroception), the AI successfully categorized emotion concepts that matched human participants' self-reported emotional evaluations with 75% agreement, significantly above chance 4. This demonstrates that the formation of emotions can be computationally modeled as an integration of physiological states and environmental context without relying on pre-programmed, hardwired emotional reflexes 4.
2.3 Allostasis, Predictive Coding, and Interoceptive Inference
At the precise neurobiological core of the Theory of Constructed Emotion is the principle of allostasis: the brain's proactive regulation of the body's metabolic and physiological resources 151315. Unlike homeostasis, which is fundamentally reactive, allostasis is predictive. The brain functions as a sophisticated inference engine, continuously generating internal models and predictions about the body's upcoming energy needs based on past experiences and the current environmental context 151415. Efficiency requires the brain to anticipate the body's needs and prepare to satisfy them before a physiological deficit arises 15.
To execute allostatic regulation, primary allostatic control neurons - located in cortical regions such as the anterior cingulate cortex, the insula, and the ventromedial prefrontal cortex - issue visceromotor predictions to the autonomic nervous system, the endocrine system, and the immune system 1216. Simultaneously, the brain monitors interoceptive signals, which are sensory representations of the body's internal milieu originating from organs, the cardiovascular system, and the gastrointestinal tract 151713.
When there is a discrepancy between the brain's predicted bodily state and the actual interoceptive sensory feedback, a "prediction error" occurs 1714. The brain then updates its internal model to minimize these errors, creating a dynamic feedback loop of active inference 1415. In this framework, an emotion is simply the psychological manifestation of the brain successfully categorizing these visceromotor predictions and interoceptive prediction errors to execute a specific, goal-oriented action 117.
2.4 Reevaluating Neural Architecture: The Default Mode Network and Executive Function
The shift toward constructionist and predictive models has also prompted a reevaluation of the neural architecture underlying emotion regulation. Classical dual-process models often posited that emotion regulation required high-level executive cortical processes (e.g., the dorsolateral prefrontal cortex) to actively provide "top-down" modulation of "bottom-up" subcortical emotional reactivity in the amygdala 17. However, recent meta-analyses of functional Magnetic Resonance Imaging (fMRI) studies challenge the necessity of these executive systems for all forms of emotion regulation.
A comprehensive 2021 meta-analysis of emotional acceptance - a key emotion regulation strategy - demonstrated that high-level executive cortical processes are not a distinctive feature of acceptance 1718. Instead, the specific neural substrate of emotional acceptance involves functional deactivations in the posterior cingulate cortex (PCC) and the precuneus, regions heavily associated with the Default Mode Network (DMN) 1718. The TCE aligns with these findings, noting that the DMN is highly active when individuals simulate or conceptualize emotions, supporting its function in cascading predictions that minimize errors between expected and actual bodily states without relying strictly on forced executive control 17. Furthermore, 2025 deep learning models utilizing electroencephalography (EEG) data have demonstrated that integrating complex spatial and temporal EEG dynamics from these distributed neural networks can classify emotional states with over 90% accuracy, relying on multimodal physiological signal fusion rather than isolated subcortical activation 16.
3. Autonomic Indicators and Underlying Physiological Mechanisms
The physiological manifestations of constructed emotions are executed via the autonomic nervous system (ANS). The ANS regulates the body's internal state through two primary branches: the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS), operating continuously and dynamically to adapt to allostatic predictions 242519.
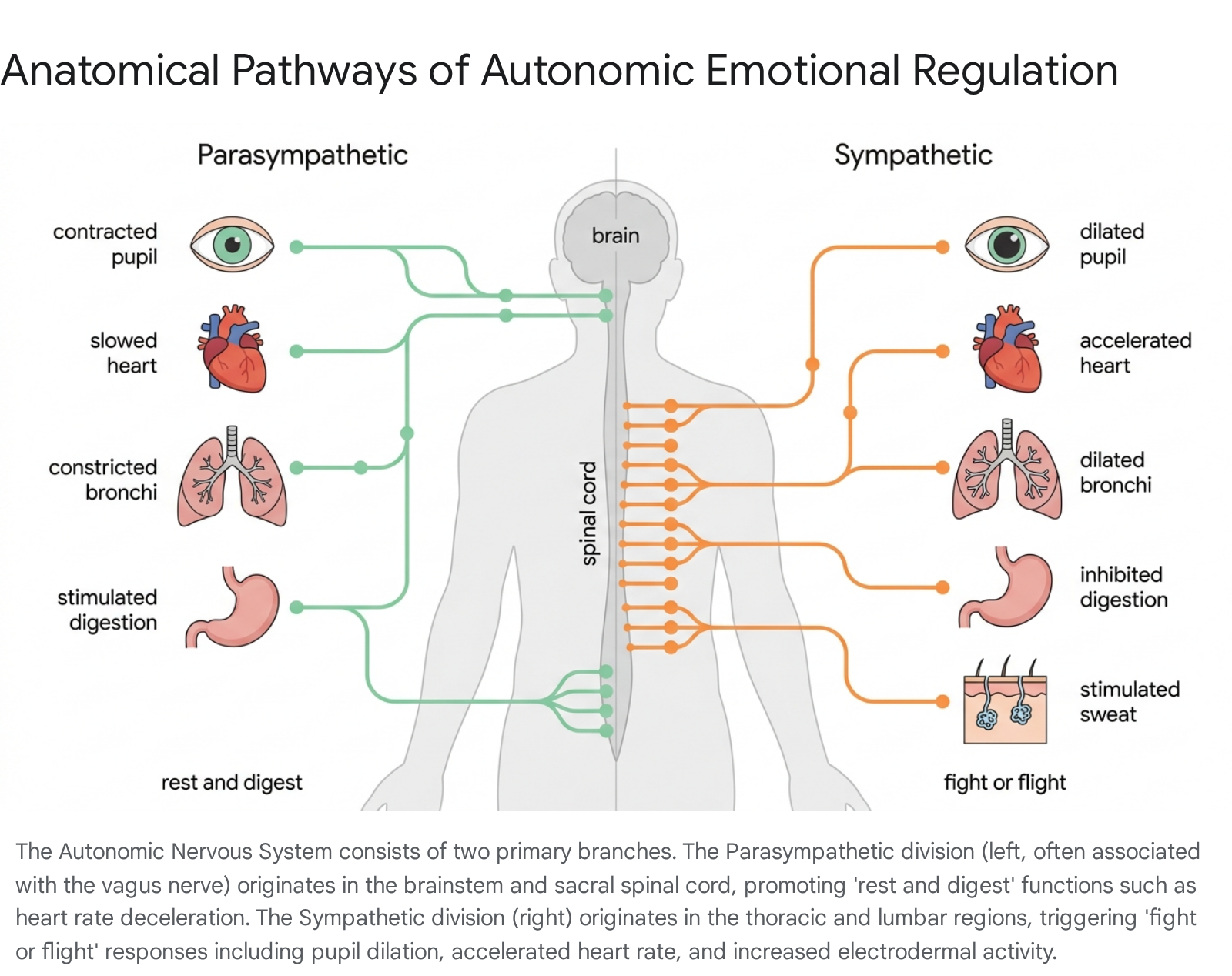
3.1 Sympathetic and Parasympathetic Activation Dynamics
The SNS is primarily responsible for mobilizing the body for action - frequently characterized as the "fight-or-flight" response 2427. Activation of the SNS results in the release of epinephrine and norepinephrine into the bloodstream, leading to immediate physiological changes: the heart beats faster and more forcefully to deliver oxygen to muscles, the bronchi in the lungs widen, pupils dilate to increase visual acuity, and digestion is inhibited to conserve energy 2728. While essential for acute survival and high-arousal task performance, chronic activation of the SNS is associated with perseverative negative thinking, fragmented attention, and long-term systemic wear 2420.
Conversely, the PNS governs the "rest-and-digest" response, facilitating physiological recovery, cellular maintenance, and energy conservation. Mediated largely by cranial nerves, most notably the vagus nerve, PNS activation slows the heart rate, diminishes the force of cardiac contraction, stimulates digestive and immune processes, and promotes cognitive flexibility and active social engagement 2427. Individuals with higher baseline parasympathetic activity generally exhibit greater creative potential, emotional intelligence, and resilience against acute stress 2421.
Historically, psychophysiological models assumed that the SNS and PNS operated on a strict continuum of reciprocal inhibition - that as sympathetic activity increased, parasympathetic activity invariably decreased 2122. However, modern autonomic space models emphasize that these systems possess independent anatomical origins and can operate orthogonally 22. Depending on the specific environmental stressor and individual differences, the two branches can exhibit reciprocal coupling, co-activation (both high, often seen during complex emotional states or stress recovery), or co-inhibition (both low) 22. For example, research indicates that women, younger adults, and individuals with higher baseline vagal tone show greater reciprocal coupling and coordinated physiological responding during social stress than older adults or those with lower baseline vagal activity 22.
3.2 Mapping Autonomic Indicators to Emotional Processing
To rigorously quantify autonomic activity in experimental and ambulatory settings, psychophysiologists utilize specific biometric indicators. The accurate interpretation of these signals requires a precise understanding of their physiological origins and the specific autonomic branch they reflect.
| Autonomic Indicator | Abbreviation | Primary ANS Branch | Underlying Physiological Mechanism | Relevance to Emotional State |
|---|---|---|---|---|
| Heart Rate | HR | SNS & PNS (Mixed) | The number of ventricular contractions per minute. Regulated simultaneously by sympathetic acceleratory pathways and parasympathetic (vagal) braking. | Serves as a general indicator of arousal; systematically increases during fear, anger, or active physical mobilization, and decelerates during relaxation, restorative processes, or when orienting to novel stimuli 272324. |
| Heart Rate Variability | HRV | Predominantly PNS | The precise temporal variation between consecutive heartbeats (interbeat intervals). High-frequency (HF) components of HRV are closely linked to parasympathetic efferent activity on the heart's sinoatrial node. | Reflects the capacity for physiological self-regulation, adaptability, and cognitive flexibility. Low HRV is strongly associated with rigid emotional responses, poor negative emotion differentiation, and chronic stress 24212425. |
| Respiratory Sinus Arrhythmia | RSA | PNS | A specific, breathing-linked component of HRV where heart rate naturally accelerates during inspiration (due to vagal withdrawal) and decelerates during expiration (due to vagal resumption). | Serves as a primary, non-invasive index of cardiac vagal tone. High RSA correlates with effective emotion regulation, social engagement capacity, and efficient physiological recovery from acute stressors 212225. |
| Pre-Ejection Period | PEP | SNS | The time interval between the electrical onset of ventricular depolarization (the Q wave on an electrocardiogram) and the opening of the aortic valve. | Acts as a pure measure of sympathetic inotropic (contractile) influence on the heart. A shortened PEP clearly indicates higher sympathetic arousal and active task engagement 212226. |
| Electrodermal Activity (Skin Conductance) | EDA / SCL / SCR | SNS | Measures minute changes in the electrical conductance of the skin caused by moisture from eccrine sweat glands. These glands are uniquely and exclusively innervated by the sympathetic nervous system. | Considered a highly sensitive index of purely sympathetic arousal. Comprises tonic activity (baseline Skin Conductance Level, SCL) indicating general alertness, and phasic activity (rapid Skin Conductance Responses, SCR) triggered by acute emotional, cognitive, or startle stimuli 362728. |
4. The Polyvagal Theory Debate: Clinical Utility vs. Scientific Consensus (2023 - 2026)
Developed by Dr. Stephen Porges in the 1990s, the Polyvagal Theory (PVT) has achieved immense popularity within clinical psychology, somatic trauma therapy, and education. The theory posits an evolutionary hierarchy of autonomic responses mediated by distinct branches of the vagus nerve. According to PVT, a newer, myelinated "ventral vagus" evolved specifically in mammals to support a "Social Engagement System," fostering co-regulation, communication, and feelings of safety 3929. In contrast, an older, unmyelinated "dorsal vagus" is posited as an evolutionary reptilian remnant responsible for life-threatening "shutdown," freezing, and extreme psychological dissociation 3930.
While PVT has undeniably revolutionized trauma-informed care by providing a biologically grounded, compassionate framework that destigmatizes autonomic survival responses - reframing them as adaptive physiological strategies rather than moral failings or psychological weaknesses - its specific neuroanatomical and mechanistic claims have faced severe, organized pushback from the mainstream autonomic neuroscience community 392930.
4.1 The 2026 Mainstream Critique
In 2026, a landmark paper co-authored by 39 leading psychophysiologists and autonomic scholars, led by Paul Grossman, concluded that the foundational physiological and evolutionary tenets of Polyvagal Theory are scientifically "untenable" 3930. The critics assert that the anatomical distinctions Porges describes are grossly oversimplified and that the evolutionary timeline of vagal development contradicts established comparative biology 293042. Specifically, the critique targets the assertion that the dorsal vagus is responsible for emotional freezing and the claim that the ventral vagus is an exclusively mammalian adaptation.
Porges has actively defended the theory, arguing that the critiques systematically misrepresent his original claims and focus disproportionately on evolutionary phylogeny while ignoring the functional reality of mammalian adaptations 394231. He notes that the dorsal vagal complex does indeed induce bradycardia and modulate anxiety-like behavior, and argues that the 2026 critique relies heavily on editorial bias without adhering to a formal scientific consensus process, such as a Delphi panel or systematic meta-analytic adjudication 3942.
Despite this intense mechanistic dispute, clinicians and scientists alike emphasize that the efficacy of polyvagal-informed therapeutic interventions - such as prolonged exhalation breathing, rhythm, chanting, and social co-regulation - remains robustly supported by an enormous body of independent physiological research 3929. These bottom-up interventions effectively enhance parasympathetic tone and reduce sympathetic hyperarousal, even if the specific "polyvagal" evolutionary narrative used to explain them is technically inaccurate 3929.
4.2 Comparative Analysis: Clinical Claims vs. Scientific Consensus
| Domain | Polyvagal Theory (PVT) Clinical Claim | 2023-2026 Scientific Consensus / Critique (Grossman et al., 39 Scholars) |
|---|---|---|
| Evolutionary Origin of Sociality | The myelinated "ventral vagus" (Nucleus Ambiguus) is a uniquely mammalian adaptation that was repurposed exclusively to support the "Social Engagement System" and higher-order social behaviors 3042. | Extensive scientific observation provides ample evidence of highly complex social behaviors in non-mammalian vertebrates (fish, reptiles, birds); there is no evidence that the ventral vagus is uniquely responsible for sociality 3042. |
| Dorsal Vagus Function and Trauma | The "dorsal vagus" is an evolutionarily primitive, reptilian structure that drives massive heart rate drops (bradycardia), freezing, and emotional "shutdown" or dissociation during extreme, inescapable threat 30. | The dorsal vagus predominantly innervates sub-diaphragmatic organs (the gut) with minimal cardiac impact in humans. Dissociation and freezing rarely feature massive heart rate drops and are centrally mediated by complex brain networks, not simply isolated ANS components 30. |
| Measurement via RSA / RHRV | Respiratory Sinus Arrhythmia (RSA) or Respiratory Heart-Rate Variability (RHRV) serves as a direct, unconfounded measure of brainstem ventral-vagal tone and social engagement capacity 3031. | RSA/RHRV is considered an imperfect index. It reflects a complex coordination of respiratory and cardiac phases and does not serve as a pure, direct measure of absolute brainstem ventral-vagal influence 3031. |
| Intervention Validity and Efficacy | Interventions targeting the "ventral vagal state" (e.g., breathwork, vocal prosody, Safe and Sound Protocol) effectively reduce sympathetic hyperarousal and trauma symptoms by engaging the mammalian smart vagus 3929. | Agreed on efficacy, but not mechanism. Practices like deep breathing, humming, and social co-regulation undeniably enhance parasympathetic tone and reduce arousal. However, this efficacy is independent of the contested PVT phylogenetic models 3929. |
5. Advancements in Measurement: Consumer Wearables vs. Clinical-Grade Tools (2023 - 2026)
A major historical hurdle in psychophysiology has been the limitation of ecological validity. Laboratory settings, which mandate the use of stationary electrocardiography (ECG) and wired electrodermal activity (EDA) sensors, inherently alter the psychological state being measured, potentially masking true emotional responses 2628. To address this, 2023 - 2026 research has intensely focused on validating ambulatory wearable technology (smartwatches, smart rings, and armbands) against clinical-grade criterion devices in real-world settings 6798.
5.1 Photoplethysmography (PPG) vs. Electrocardiography (ECG)
While hospital-grade ECG measures the direct electrical activity of the heart via electrodes placed on the chest, most consumer wearables utilize photoplethysmography (PPG) - a technology that shines light into the skin to detect subtle volumetric changes in microvascular blood flow 63245.
Recent validation studies demonstrate that while PPG-based consumer wearables capture resting heart rate (HR) with exceptional accuracy, they struggle significantly with Heart Rate Variability (HRV) during active or ambulatory periods 746. HRV calculations (specifically metrics like the root mean square of successive differences, RMSSD) rely on the precise, millisecond-level detection of every single interbeat interval 732. PPG signals are highly susceptible to movement artifacts; even minor hand motions, postural changes, or performing a mental arithmetic task involving speech can decrease the signal-to-noise ratio, resulting in dropped peaks and heavily biased HRV metrics 732. Therefore, researchers conclude that wearable HRV data is only highly reliable when recorded during stationary periods, notably during nocturnal sleep or seated rest 32.
5.2 Device-Specific Accuracy and The "Research-Grade" Paradox
A rigorous 2025 independent peer-reviewed study analyzing major consumer wearables found vast discrepancies in measurement accuracy. For nocturnal resting HR and HRV, the Oura Ring (both Generation 3 and Generation 4) demonstrated the highest concordance with clinical ECG references 84748. In the study, the Oura Ring achieved a Lin's Concordance score of 0.99 for HRV, significantly outperforming devices from Garmin, Polar, and WHOOP 848. The Oura Ring's superior performance is attributed to its form factor - the finger boasts a stronger capillary density than the wrist - and its 18-path multi-wavelength PPG system, which samples heart rate at a high frequency of 250 Hz, allowing it to rival medical-grade accuracy during sleep and making it highly viable for longitudinal clinical research 8473350.
Conversely, recent studies have revealed a paradox regarding devices explicitly marketed and priced as "research-grade." The Empatica E4 and its successor, the EmbracePlus - long considered the gold standard for wrist-worn academic research - have been shown to occasionally underperform high-end consumer wearables in specific contexts. Validation research indicates that in ambulatory settings involving movement, the accuracy of HRV and EDA indices derived from the Empatica significantly diminishes, sometimes showing valid data rates as low as 8.7% for PPG and 41% for EDA in daily life, compared to 93% for stationary laboratory ECG 746. This suggests that the "research-grade" label does not automatically guarantee superior data quality outside of strictly controlled environments 7.
5.3 Innovations in Ambulatory Electrodermal Activity (EDA)
Validating ambulatory Electrodermal Activity (EDA) has been particularly challenging. Medical-grade EDA relies on wired Ag/AgCl electrodes placed on the palmar surface of the hands or distal phalanges (fingertips), where eccrine sweat gland density is highest, capturing robust skin conductance responses (SCR) 2834. Wireless consumer devices, however, typically measure EDA at the wrist or via a ring format.
A 2025 maritime simulation study comparing wired fingertip EDA to wireless wrist EDA found that while wired sensors produced signal amplitudes ten times higher due to superior anatomical placement, the wireless sensors effectively mirrored the temporal trends 28. Both sensors accurately captured the timing and patterns of phasic SCRs during sudden stress-inducing events, such as bridge alarms 28. The wireless system was vastly favored for its ergonomics, as the complex wired system was noted to induce "measuring anxiety" in participants, inadvertently altering their physiological baseline simply due to the encumbrance of the technology 28.
Furthermore, a massive 2025 systematic review and meta-analysis of 87 peer-reviewed studies involving over 2,000 subjects revealed a paradigm-shifting finding regarding nocturnal EDA. Contrary to daytime measurement conventions, wrist-based EDA during sleep exhibits superior amplitude compared to palm measurements on 84-91% of nights 9. The wrist location shows 34% fewer motion artifacts and 68% lower electrode drift variability during sleep, leading to highly accurate (83.7%) machine-learning classifications for sleep apnea screening and advanced sleep stage discrimination 9.
Concurrently, hardware innovations are expanding daytime EDA capabilities. In 2025, researchers at the Javey Lab demonstrated the efficacy of newly developed breathable, water-permeable electrodes that prevent sweat from pooling at the skin surface . This breakthrough solves a historical limitation where heavy sweating during physical exertion saturated the skin and short-circuited EDA sensors. Consequently, modern EDA can now reliably distinguish between continuous signals caused by physical exertion (hydration loss) and those driven by acute mental stress, opening the door to comprehensive, everyday physiological monitoring 53.
6. Cross-Cultural Psychophysiology: Global Perspectives on Emotional Reactivity
A critical, underlying assumption in the classical view of emotion was the strict universality of emotional responses 5455. However, modern frameworks like the Theory of Constructed Emotion explicitly anticipate physiological variance. Because cultural context fundamentally shapes the conceptual knowledge that the brain utilizes to categorize interoceptive signals and predict metabolic needs, the resulting emotional architecture must vary across distinct populations 51517. Research published between 2023 and 2025 provides robust, geographically diverse evidence that cultural background significantly moderates both the psychological experience and the objective autonomic physiological response to emotion.
6.1 Cultural Variances in Emotion Regulation Strategies
Emotion regulation - the inherent motivation and the specific strategies utilized by individuals to influence which emotions they experience and how those emotions are expressed - demonstrates distinct geographical divides. A massive two-part study conducted during the COVID-19 pandemic (2020 - 2021) compared residents of Western countries (including the United States, the United Kingdom, and Germany) with residents of East Asian countries (including Japan, South Korea, and China) 35.
The findings revealed that individuals in East Asian cultures exhibited significantly lower motivation to decrease unpleasant emotions compared to their Western counterparts. Rooted in differing cultural syndromes, East Asian participants generally viewed negative affect as a more acceptable, transient, and inevitable component of a balanced life. Consequently, they utilized active emotion regulation strategies less frequently than Western populations, who demonstrated a higher drive to actively suppress or cognitively reappraise negative states to maximize subjective well-being 3557.
Similarly, pronounced cultural differences emerge in the physiological generation and experience of positive emotions. Recent cross-cultural research on "positivity resonance" - defined as a co-experienced, kind-hearted positive emotion thought to universally strengthen interpersonal bonds - revealed unexpected variances 10. In comparative studies spanning over 5,700 participants, East Asian individuals reported significantly lower levels of positivity resonance with strong social ties compared to European Americans 10. Statistical modeling indicated that this variance was heavily mediated by differences in perceived "relational mobility." This suggests that societies prioritizing high personal autonomy and fluid, choice-driven relationships (such as the United States) culturally necessitate a higher frequency of physiological and expressive positive affect to actively build and maintain social networks, whereas societies with more fixed, dutiful social structures do not require the same degree of affective resonance 10.
6.2 Psychophysiological Responses to Social Stimuli and Exclusion
The physiological impact of cultural framing is perhaps most evident in studies evaluating social interaction and ostracism. Utilizing the "Cyberball" paradigm - a digital ball-tossing game explicitly designed to induce feelings of social exclusion - researchers continuously measured the autonomic and muscular responses of European Americans and Chinese Americans to sudden social loss 11.
While previous meta-analyses largely comprised Western subjects and assumed an automatic, universally distressing "social pain" response to exclusion (often correlating social pain with physical pain neural circuitry in the dorsal anterior cingulate cortex), real-time psychophysiological monitoring revealed profoundly divergent profiles 11. During exposure to stimuli associated with social loss, East Asian participants exhibited distinct signs of physiological withdrawal, characterized by a decreased heart rate and an increase in respiratory sinus arrhythmia (RSA) - indicating a parasympathetically driven disengagement from the environment 11.
Conversely, European Americans demonstrated an active sympathetic distress profile, marked by elevated heart rate variance and distinct facial electromyography (fEMG) activation at the corrugator muscle, which is heavily associated with intense frowning and active distress 11. This fundamental difference indicates that the loss of social affordances triggers completely different allostatic predictions - and therefore different autonomic responses - based on cultural conditioning.
6.3 Cross-Cultural Perception of Physiological Intensity
Cultural variance extends beyond the generation of emotions to the perception of physiological cues in others. Cross-cultural perceptual studies modeling facial movements indicate that individuals from East Asian and Western European cultures expect facial musculature to dynamically represent intensity differently depending on the specific emotion being conveyed 9.
While both cultural groups share similar physiological expectations for high-intensity threat emotions (such as anger, disgust, and fear), they differ significantly on the specific facial-muscular movements they expect for low-threat emotions (such as happiness and sadness) 9. Furthermore, certain facial movements serve different communicative roles entirely; for example, the simultaneous Lip Corner Puller and Cheek Raiser (Action Units 12 and 6) functions primarily as a core emotion classifier for Western European receivers, but acts only as an intensity amplifier for East Asian receivers 9. These findings underscore that the interpretation of physiological affective cues is heavily modulated by cultural "dialects," complicating the notion of universally recognized emotional expressions.
7. Conclusion
The science of psychophysiology is currently undergoing a profound conceptual and methodological evolution. The theoretical shift away from classical basic emotions toward the Theory of Constructed Emotion asserts that autonomic responses - such as acute shifts in heart rate variability or spikes in electrodermal activity - are not rigid biological fingerprints. Instead, they are dynamic, context-dependent visceromotor predictions generated by the brain in the continuous service of allostatic regulation 341515.
This nuanced, predictive understanding of the human body requires equally sophisticated measurement capabilities. As evidenced by robust 2023 - 2026 validation data, while significant challenges remain regarding motion artifacts in ambulatory settings, high-end consumer wearables utilizing multi-path PPG sensors and refined algorithms are democratizing access to highly reliable psychophysiological data, particularly during stationary and nocturnal periods 798. However, both clinical researchers and practicing clinicians must remain critically informed regarding the limitations of these tools and the theories they support. Theoretical frameworks that are widely adopted in clinical practice, such as the Polyvagal Theory, offer undeniable therapeutic utility for trauma intervention, yet their specific neuroanatomical and evolutionary claims are increasingly rejected by mainstream psychophysiologists 3929.
Ultimately, as psychophysiological monitoring continues to scale globally through digital health platforms and wearable technology, researchers and developers must account for the extensive cross-cultural variability in emotional regulation, affective expression, and autonomic reactivity 91135. Physiological arousal is inextricably linked to learned cultural concepts, confirming that the body's response to emotion is as diverse, adaptable, and constructed as the human experience itself.