Psychology of People-Pleasing Origins Costs and Management
Psychological Foundations and Definitions
The concept colloquially recognized as "people-pleasing" does not exist as an independent psychiatric diagnosis within clinical frameworks. Instead, it encompasses a multifaceted behavioral and cognitive pattern defined by an excessive investment in fulfilling the needs, expectations, and emotional states of others, invariably to the detriment of the individual's own autonomy and well-being 12. Psychological literature operationalizes this phenomenon through various overlapping constructs, noting that the primary motivators underlying this conduct are an intense fear of rejection, profound anxiety regarding social acceptance, and an unrelenting need for external approval 1. By minimizing personal preferences and establishing excessively compliant interpersonal dynamics, individuals utilizing these behaviors seek to preempt conflict and artificially sustain environmental harmony 1.
Within cognitive-behavioral paradigms, people-pleasing is extensively studied under the rubric of "sociotropy," a construct introduced by cognitive therapy pioneer Aaron T. Beck 34. Initially formalized through the Sociotropy-Autonomy Scale (SAS), sociotropy is defined as a personality dimension characterized by an over-investment in positive social interchanges and an absolute reliance on interpersonal validation for self-worth 34. Beck's psychometric modeling of the SAS, which was developed utilizing data from 378 psychiatric patients, distilled the construct into three dominant cognitive factors: Concern About Disapproval, Attachment/Concern About Separation, and Pleasing Others 3. Sociotropy stands in direct opposition to autonomy; highly sociotropic individuals are predominantly occupied with the maintenance of relationships, whereas autonomous individuals prioritize independence and individualistic achievement 3.
The cognitive architecture of sociotropy is defined by absolute and dysfunctional beliefs, such as the internalized axiom, "If someone disapproves of me, I am unlovable" 4. Because the sociotropic individual's self-esteem is wholly tethered to relational success, they are rendered uniquely vulnerable to depressive episodes when relationships rupture or fail 34. Research indicates that sociotropic individuals frequently exhibit complementary traits, including lack of assertion and shyness, driven by the fear that assertiveness will invite abandonment 3. In clinical evaluations, sociotropy has also been highly correlated with appearance anxiety and body image dissatisfaction, as the individual's self-perception fluctuates based on the perceived evaluations of their peers 4.
Beyond Beck's framework, subsequent psychometric instruments have sought to measure people-pleasing directly. The Langenfeld Inventory of Personality Priorities (LIPP), developed in 1983, identifies "pleasing" as a primary personality priority, characterized by an overarching desire to gain acceptance by fulfilling others' expectations 2. More recently, the multidimensional People-Pleasing Scale (PPS) was validated across two large German samples, isolating three fundamental dimensions of the behavior: Responsibility, Neglect of Own Needs, and Others' Expectations 5. Further clinical measurements, such as the 24-item CPP scale, categorize the severity of people-pleasing syndrome. Within this metric, scores between 16 and 24 indicate a severe, pathological manifestation of the syndrome, characterized by distorted mindsets, compulsive habits, and fear-based emotional responses 2.
Personality Trait Frameworks and the Big Five
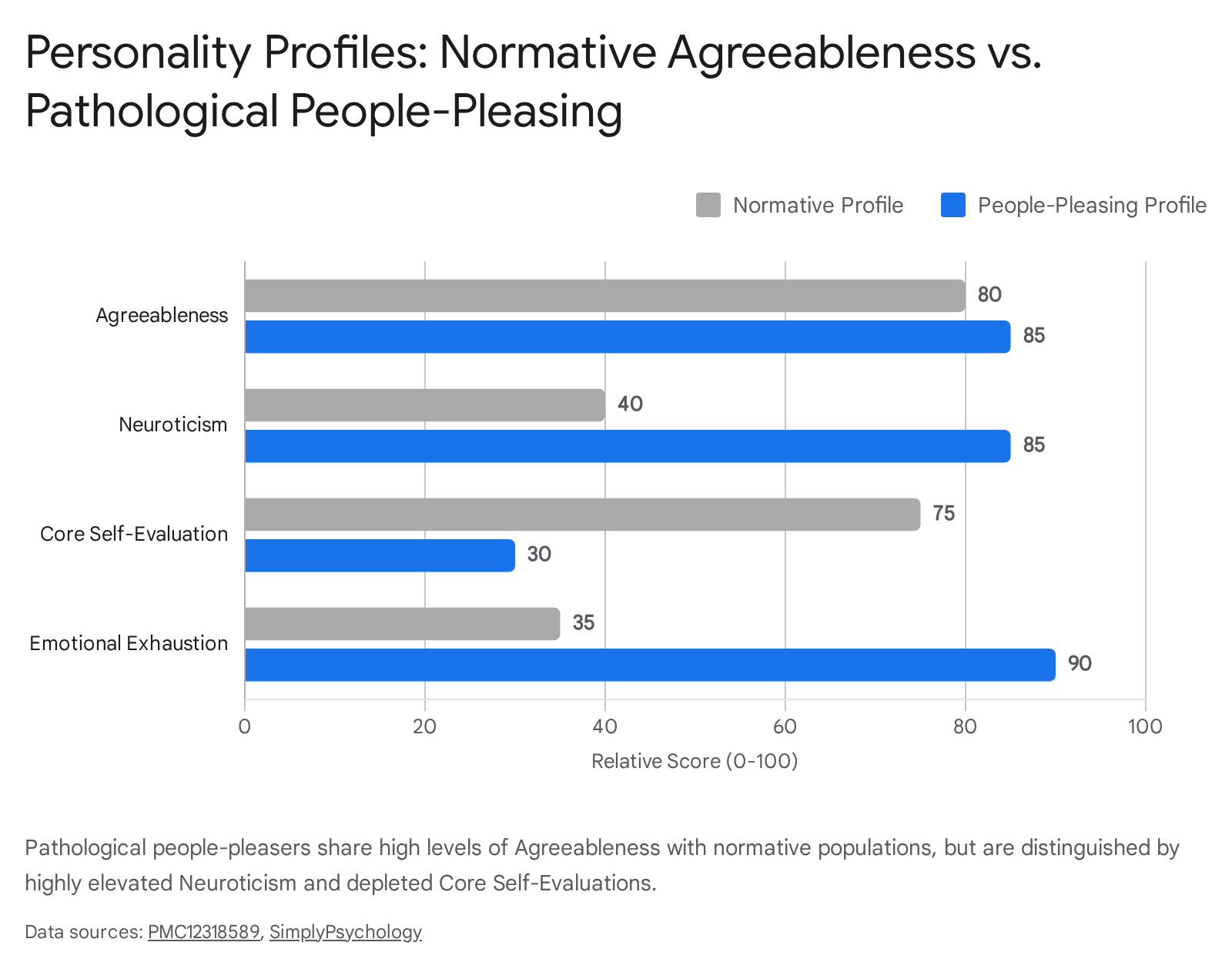
To differentiate pathological people-pleasing from normative pro-social behavior, researchers frequently utilize the Five-Factor Model (the "Big Five") of personality, specifically analyzing the intersection of Agreeableness and Neuroticism 26. Agreeableness serves as a measure of an individual's orientation toward compassion, cooperativeness, and social harmony 67. Individuals demonstrating high baseline agreeableness without complicating factors value egalitarian relationships, easily establish social connections, and possess an optimistic view of human nature, believing others to be fundamentally decent and trustworthy 88. High normative agreeableness acts as a protective psychological factor, aiding in the maintenance of robust support networks and mitigating depressive symptoms 6.
Pathological people-pleasing, however, emerges when extreme levels of agreeableness are combined with highly elevated Neuroticism 27. Neuroticism dictates an individual's emotional instability, propensity for anxiety, and reactivity to negative stimuli 26. When an individual is highly agreeable but concurrently highly neurotic, their cooperative behaviors are not motivated by an optimistic disposition, but rather by self-doubt, hypervigilance, and an intense fear of social isolation 26. This pathological intersection drives the individual to suppress their authentic emotional experiences to placate others, resulting in profound emotional exhaustion and psychological distress 2.
Research linking people-pleasing to core self-evaluations further elucidates this dynamic. Core self-evaluations encompass an individual's baseline self-esteem, self-efficacy, and emotional stability 2. Chronic people-pleasers frequently demonstrate severely diminished core self-evaluations because their sense of worth is perpetually outsourced to external validation 2.
Paradoxically, despite their hyper-focus on relational maintenance, people-pleasers often report intense feelings of loneliness and solitude; because they continuously suppress their authentic identities to mirror the desires of others, their social connections remain shallow and fundamentally unsatisfying 2.
Cognitive, Behavioral, and Emotional Mechanisms
To operationalize the mechanisms of this behavior in clinical contexts, psychologist Harriet Braiker proposed a comprehensive tripartite framework, often termed the "Disease to Please" triad 101112. According to this structural model, compulsive appeasement is not a singular flaw but a self-sustaining cycle driven by overlapping cognitive distortions, compulsive behavioral habits, and deep-seated emotional avoidance 1011.
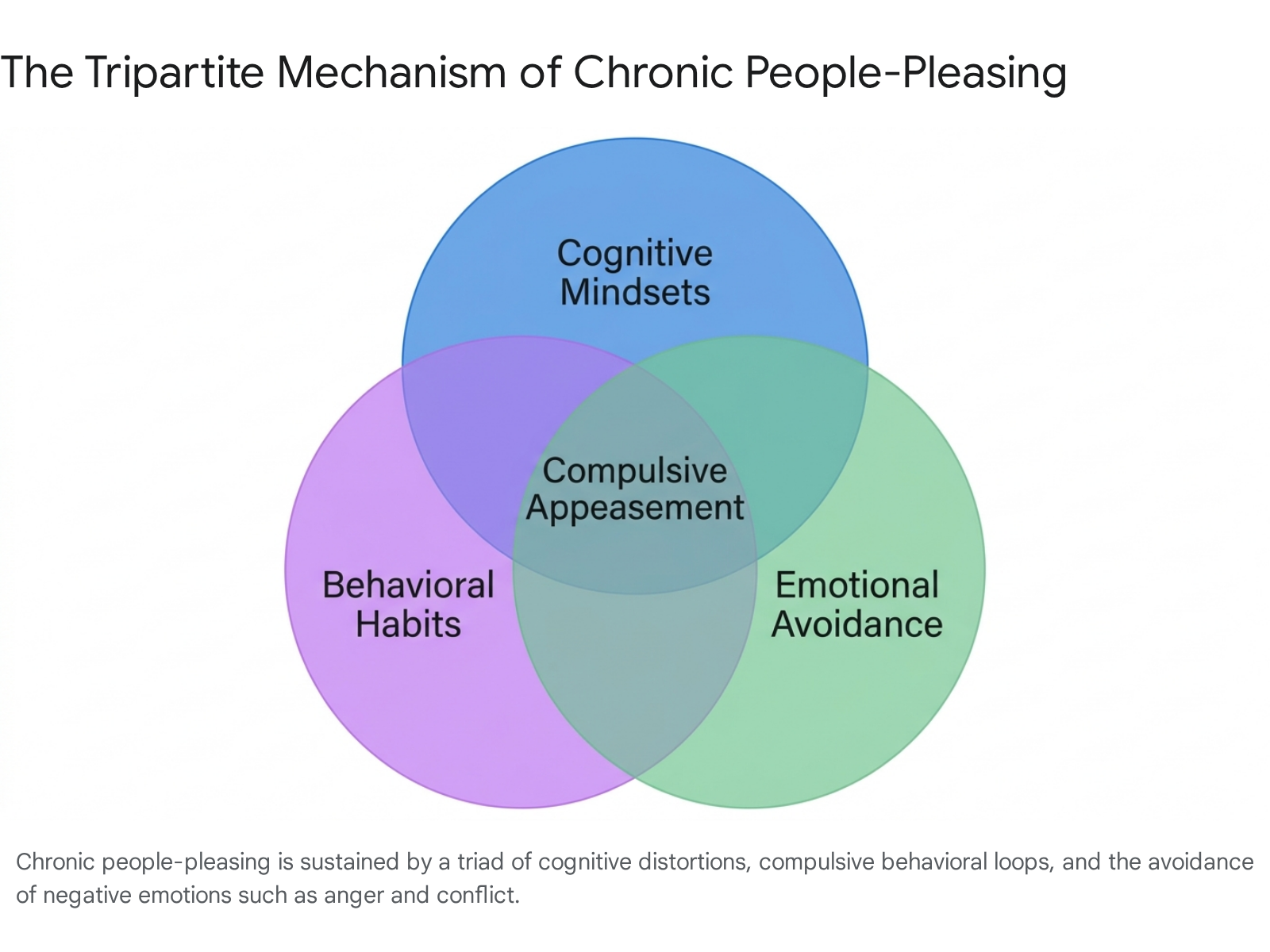
The first dimension of the triad concerns cognitive mindsets 11. People-pleasing is sustained by rigid, logically flawed beliefs and absolute imperatives that the individual applies to their social functioning 1112. These cognitions are frequently categorized into extreme directives, such as the belief that one must always fulfill the expectations of others, or the belief that one must never burden others with personal problems 1213. When the individual inevitably fails to meet these unrealistic cognitive demands, they experience intense self-blame, guilt, and depression, which in turn fuels the perceived need to try harder to please 11.
| Cognitive Distortion Category | Conceptual Example from Psychological Literature | Clinical Consequence |
|---|---|---|
| Absolute Compliance | "I must always do what others want, expect, or need from me." | Generates chronic exhaustion and eliminates the capacity for autonomous decision-making 13. |
| Emotional Suppression | "I must always be upbeat and never show negative feelings." | Results in the presentation of a false self, preventing authentic intimacy and connection 139. |
| Conflict Avoidance | "I must never disappoint anyone or hurt anyone's feelings." | Traps the individual in toxic relationships due to the terror of initiating a rupture 1113. |
| Martyrdom | "I must always put other people first, before my own needs." | Causes profound self-neglect, leading to physical burnout and suppressed internal rage 1113. |
Table 1: Common cognitive distortions sustaining people-pleasing mindsets 111213.
The second dimension involves behavioral habits and the neurochemistry of addiction. Braiker posits that approval-seeking operates similarly to substance addiction due to the mechanics of variable reinforcement 1112. Because external approval is entirely subjective, the people-pleaser does not receive validation every time they sacrifice themselves. This unpredictable, intermittent reward schedule creates a highly compelling behavioral loop; the individual continuously escalates their self-sacrificing behaviors in the desperate pursuit of a validation 'hit' 11. Over time, these actions bypass conscious choice and become deeply ingrained, reflexive habits 1012.
The final dimension is emotional avoidance, specifically regarding the processing of anger 1012. Chronic people-pleasers harbor an intense aversion to confrontation. They engage in preemptive appeasement to prevent anger in others, treating external dissatisfaction as an existential threat 12. Furthermore, this outward fear of anger frequently mirrors an internal inability to regulate personal anger. The individual suppresses their own frustration through the four phases of anger (yellow alert, ignition, escalation, and resolution) to maintain a placid exterior, internalizing the conflict until it manifests as somatic distress 1213.
Distinguishing People-Pleasing from Clinical Disorders
While extreme people-pleasing carries severe psychological costs, it is imperative to distinguish it from formal psychiatric pathology, particularly Dependent Personality Disorder (DPD). The conceptualization of personality traits and disorders has deep historical roots, tracing back to the 5th century BC when Greek and Chinese philosophers hypothesized that temperament derived from bodily humors 10. Modern clinical frameworks, specifically the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), classify DPD under Cluster C, which encompasses anxious and fearful personality pathologies 1011.
A diagnosis of DPD requires the presence of at least five of eight specific criteria, centering on a pervasive, excessive need to be taken care of 1213. Individuals with DPD experience intense separation anxiety, struggle to initiate projects independently, and require inordinate amounts of advice to make mundane daily decisions 1213. While DPD and severe people-pleasing share outward characteristics - such as submissiveness, an inability to express disagreement, and a profound fear of abandonment - their psychological foundations differ substantially 1113.
Dependent Personality Disorder is rooted in an internalized perception of total incompetence; the individual genuinely believes they are incapable of functioning without a caretaker 1012. Submissive behaviors in DPD are strategically, if unconsciously, deployed to elicit care and avoid the terror of self-reliance 1012. From a psychobiological perspective, DPD is characterized by low novelty-seeking and exceptionally high reward-dependence, resulting in uninquiring, isolative behaviors when a caretaker is not present 11.
Conversely, pathological people-pleasers - especially those whose behaviors stem from trauma or high functioning anxiety - are often highly competent, autonomous individuals in contexts separate from interpersonal conflict 114. A people-pleaser may manage complex professional responsibilities and excel independently, yet compulsively subordinate their needs in social relationships to manage the emotional states of others 1420. Rather than eliciting care, the people-pleaser often assumes the role of the caretaker, hyper-accommodating others to neutralize perceived threats 915. The people-pleaser sacrifices their autonomy as a protective strategy, whereas the individual with DPD believes they possess no autonomy to sacrifice.
| Diagnostic Differentiator | Dependent Personality Disorder (DPD) | Pathological People-Pleasing (Fawning) |
|---|---|---|
| Core Self-Perception | Fundamentally incapable of self-care or basic survival without external aid 1012. | Capable, but unworthy of love or safety unless actively serving others 214. |
| Primary Motivation | To elicit caregiving, direction, and constant reassurance from a stronger figure 1013. | To pacify potential threats, prevent conflict, and artificially maintain relational stability 2223. |
| Role in Relationships | The helpless dependent requiring continuous management 13. | The hyper-attuned caretaker, absorbing the emotional burdens of the partner 915. |
| Behavior in Isolation | Severe anxiety, paralysis in decision-making, and profound distress 1112. | Often a sense of relief from social pressure, though accompanied by emptiness or loneliness 224. |
Table 2: Clinical differentiation between Dependent Personality Disorder and pathological people-pleasing 101112131415.
Neurobiological Origins and the Fawn Response
In contemporary clinical trauma theory, severe, compulsory people-pleasing is increasingly analyzed as the "fawn response." Introduced into the psychological lexicon by psychotherapist Pete Walker, fawning is identified as the fourth primary survival strategy, expanding upon the traditional trauma triad of fight, flight, and freeze 142016. While the fight and flight responses involve mobilizing against or fleeing from a threat, and the freeze response involves immobilization to evade detection, the fawn response involves dissolving into the threat 2223. The individual instinctively attempts to pacify a perceived aggressor by abandoning their personal boundaries, mirroring the aggressor's emotional state, and preemptively accommodating their needs 202223.
Polyvagal Theory and Autonomic Regulation
The mechanics underlying the fawn response are illuminated by Polyvagal Theory, developed by Dr. Stephen Porges and expanded by clinicians like Deb Dana 261728. The theory maps the autonomic nervous system into a hierarchy of survival and social engagement 1718. At the top of the hierarchy is the Ventral Vagal state, which supports safe social connection, calm engagement, and groundedness 1719. When an individual is in this state, acts of kindness or accommodation are genuine, prosocial choices 2219.
Below this lies sympathetic activation (the fight-or-flight system), which mobilizes the body using adrenaline and cortisol in response to danger, and the dorsal vagal system, which triggers shutdown, dissociation, and immobilization under extreme, inescapable threat 1719. Autonomic shifts involve distinct physiological timelines; while ventral vagal adjustments happen in milliseconds, sympathetic activation triggers complex chemical cascades that can take 10 to 20 minutes to clear the bloodstream once initiated 17.
Fawning represents a highly sophisticated, blended neurobiological state. It requires the engagement of the prefrontal cortex - the brain region responsible for higher-order thinking, decision-making, and complex social behavior (such as reading micro-expressions and formulating appeasing dialogue) - while the underlying autonomic nervous system is locked in sympathetic threat-activation or dorsal shutdown 2022. The nervous system is effectively running a survival program masked as social grace. The physical markers of appeasement, such as smiling or agreeable vocal tones, are deployed not as invitations for connection, but as desperate tools for de-escalation 1422.
Developmental Neurobiology and the Amygdala-mPFC Circuitry
The fawn response rarely develops spontaneously in adulthood; it is fundamentally a developmental adaptation forged in early childhood, typically within environments characterized by relational trauma, emotional neglect, or volatile caregiving 1420. An infant or young child cannot execute a fight or flight response against a much larger primary caregiver upon whom their survival depends. Consequently, the child adapts by developing hypervigilant attunement to the caregiver's shifting moods, learning that their physical and emotional safety is entirely contingent upon managing the adult through absolute compliance 142023.
Neurodevelopmental research provides specific insight into how this adaptation alters brain architecture. Under standard environmental conditions, the regulatory neural connections between the amygdala (the brain's emotional and threat-detection center) and the medial prefrontal cortex (mPFC) mature gradually from childhood into adolescence 2122. The mature prefrontal cortex provides necessary top-down inhibition of the amygdala, allowing for measured, rational responses to emotional stimuli 2022.
However, early life adversity - such as maternal deprivation or volatile parenting - dramatically accelerates this neural development. Animal models and studies on previously institutionalized youths reveal that repeated elevations of stress hormones, specifically corticosterone (CORT) or cortisol, during critical sensitive periods prompt an early, age-atypical emergence of mature amygdala-mPFC connectivity 2021. In standard development, a regulated caregiver provides "social buffering," blocking the release of excess CORT and preventing the amygdala from undergoing trauma-induced plasticity 20. In the absence of this buffering, the brain executes an ontogenetic adaptation to adversity 21.
This premature neural coupling ensures that the child can rapidly engage sophisticated, prefrontal-mediated social behaviors (fawning and appeasement) the instant the amygdala detects a threat 142122. While highly adaptive for surviving a dangerous childhood environment, this hardwired circuitry becomes profoundly maladaptive in adulthood. The adult's drive to appease an angry colleague or partner feels completely involuntary because it operates via instantaneous, subcortical survival pathways forged decades earlier 1415.
Somatic and Physiological Costs
The sustained, compulsory suppression of authentic emotional needs exacts a devastating toll on physical health. Chronic people-pleasers exist in a state of perpetual nervous system dysregulation, their bodies bearing the physiological burden of unexpressed boundaries 3435.
The Endocrine and Immune Impact
Because people-pleasers continually scan their environments for social threats and suppress their own impulses to maintain the peace, their autonomic nervous systems remain locked in low-grade sympathetic activation 3536. This state of chronic stress leads to the sustained release of cortisol and adrenaline. Over time, hypercortisolemia severely disrupts metabolic and immune function 3536.
Medical researchers consistently highlight the epidemiological correlation between compulsory emotional suppression and chronic illness. Prolonged physiological stress increases systemic inflammation, weakening the immune system and elevating the risk of cardiovascular disease and type 2 diabetes 3637. Furthermore, experts in trauma and physical health, such as Dr. Gabor Maté, emphasize that the societal conditioning of women to prioritize others contributes directly to disproportionately high rates of autoimmune disorders in female populations 3738. The body's immune system, dysregulated by chronic stress, begins to attack its own tissues as a physiological reflection of continuous self-abandonment 3637.
Neuroplastic Pain and Somatization
The suppression of boundaries also inevitably generates internal frustration and rage 1235. When individuals refuse to acknowledge this rage to maintain an agreeable persona, the nervous system must process the emotional energy through alternative channels. Dr. John Sarno's pioneering work on neuroplastic pain identifies that repressed internal rage frequently manifests as physical symptoms - such as severe muscle tension, migraines, digestive issues, and chronic back pain 3435. The brain generates these physical sensations both as a distraction from the unacceptable emotion and as a somatic protest against the violation of the individual's needs 3435. Healing these physical ailments often requires individuals to acknowledge their repressed anger and dismantle their fawning habits 35. Furthermore, oncology researchers like Dr. Kelly Turner and Dr. Nasha Winters have observed that chronic emotional suppression creates oxidative stress that can influence disease progression, noting that processing suppressed emotions is a common variable in unexpected cancer recovery cases 36.
Cross-Cultural Perspectives on Interdependence
A significant methodological challenge within psychological research is accurately differentiating maladaptive, trauma-driven people-pleasing from culturally normative values of interdependence. Western psychology has historically been dominated by an individualistic paradigm, which inherently defines mental health in terms of strict autonomy, self-assertion, and personal independence 392324. Viewed exclusively through this ethnocentric lens, behaviors that prioritize collective harmony over individual desires are frequently, and incorrectly, pathologized as codependency or fawning 1525.
Individualism vs. Collectivism
Cross-cultural psychology operates on a continuum between individualism and collectivism 392644. In highly individualistic societies, such as the United States, United Kingdom, and Australia, self-concept is constructed around personal traits, uniqueness, and competition 394427. Conversely, in collectivist societies - which comprise much of East Asia, Latin America, and sub-Saharan Africa - the self is interdependent 264428. Identity is defined by an individual's relationship to their in-group, and social harmony, loyalty, and communal obligation are considered paramount virtues 392628.
Dutch social psychologist Geert Hofstede's foundational research on "software of the mind" demonstrated that collectivist cultures feel happier exercising socialized power, viewing those who adhere to social norms and foster group cohesion as highly successful 2644. Contemporary research further delineates interdependence into regional variants: conflict avoidance in East Asia, self-assertion for ingroup protection in Arab regions, interpersonal resonance in Latin America, and argumentation for conflict resolution in South Asia 23.
Cultural Constructs of Harmony
Specific indigenous philosophies illustrate robust models of healthy interdependence, which operate via fundamentally different psychological mechanisms than the trauma-based fawn response:
- Amae (Japan): Often translated as the presumed acceptance of one's inappropriate behavior or reliance upon another, amae denotes a deeply secure, symbiotic emotional bond 29. Rather than functioning out of a fear of abandonment, an individual exercising amae trusts that the relationship is sufficiently strong to tolerate their dependency. It is a manifestation of profound relational security, contrasting sharply with the anxious, hypervigilant appeasement characteristic of people-pleasing 29.
- Inhwa / In-shwa (Korea) & He (China): Deeply rooted in Confucian doctrine, these concepts conceptualize interpersonal harmony as a dynamic, continuous process of maintaining universal balance 303132. Conflict is not avoided out of terror, but managed through normative reasoning, self-restraint, and intentional "disintegration avoidance" to preserve the structural integrity of the collective 303233.
- Ubuntu (Southern Africa): Encapsulated by the Nguni proverb "umuntu ngumuntu ngabantu" ("a person is a person through other persons"), Ubuntu is an expansive philosophy of human interconnectedness 345335. It asserts that an individual's humanity is realized and affirmed solely through their relationships with others 3536. Actions supporting the collective are motivated by shared dignity, reciprocal care, and moral duty, operating entirely outside the neurobiological panic of the trauma survival system 5336.
| Psychological Construct | Cultural Context | Primary Driver | Neurobiological State |
|---|---|---|---|
| Fawn Response | Universal (Trauma-based) | Survival, fear of abuse, abandonment terror. | Sympathetic Activation / Dorsal Shutdown (Threat) 2217. |
| Amae | Japan | Trust, relational security, symbiotic comfort. | Ventral Vagal (Safety/Connection) 1729. |
| Inhwa / He | Korea / China | Confucian ethics, structural balance, duty. | Prefrontal Regulation, Ventral Vagal 3233. |
| Ubuntu | Southern Africa | Shared humanity, collective responsibility, empathy. | Ventral Vagal (Safety/Connection) 3536. |
Table 3: Differentiation between trauma-driven appeasement and culturally normative constructs of interdependence 2217293235.
The essential distinction between cultural harmony and pathological fawning lies in agency and neurobiology. Behaviors aligned with Ubuntu or Inhwa are executed from a Ventral Vagal state of physiological safety; the individual experiences profound belonging, prosocial connection, and meaning through their service 173536. Conversely, the fawn response is a desperate survival tactic that leaves the individual feeling empty, depleted, and disconnected from their authentic identity 92223. However, as trauma researchers observe, cultural socialization and trauma can unfortunately reinforce one another; societal expectations demanding female appeasement, for example, can deeply entrench trauma-based fawning by validating it as a moral virtue 1522.
Professional Boundaries and Media Discourse
The tension between boundary-setting and people-pleasing has become highly visible in modern professional environments and digital discourse. As psychological concepts migrate into mainstream social media - a phenomenon termed "therapy speak" - clinical terminology is frequently diluted 5737. Terms like fawning, gaslighting, toxic, and boundaries are increasingly utilized in casual vernacular 57.
While this linguistic shift fosters mental health awareness, clinicians warn that the overuse of therapy speak can impede genuine communication 59. Individuals may misappropriate the concept of "setting a boundary" as an evasion of accountability or a justification for cold, dismissive behavior, ultimately utilizing clinical jargon as a defense mechanism to avoid the vulnerability required for authentic relationship repair 5960. True recovery from people-pleasing requires plain-language honesty rather than performative, textbook-style declarations 60.
Applied Boundary Setting: A Journalistic Case Study
To understand what non-pleasing, objective boundary-setting looks like in practice, researchers can examine the professional standards of journalism. Journalists operate in high-pressure interpersonal environments where sources frequently share traumatic, emotionally charged information 61. A people-pleasing response in this context - becoming overly friendly, offering unmerited reassurance, or blurring personal lines - violates professional ethics and compromises objectivity 6162.
News organizations, such as NBC News, alongside institutions like the Society of Professional Journalists (SPJ), mandate strict boundary enforcement 61. Journalists are trained to be "friendly, but not friends" with sources, expressly avoiding social media overlap (e.g., following sources on Instagram or utilizing overly familiar emojis in communication) and refusing gifts 61. In the digital age, journalists face immense pressure from online mobs and reciprocal social media expectations, risking harassment if they do not appease audience biases 6263. By strictly adhering to predefined ethical frameworks, journalists demonstrate that it is entirely possible to navigate intense emotional demands with empathy and civility, without sacrificing one's professional integrity or succumbing to the compulsion to please 61.
Evidence-Based Clinical Interventions
Dismantling chronic people-pleasing requires comprehensive clinical interventions that address the behavior simultaneously at the cognitive, behavioral, and neurobiological levels. Because fawning and sociotropy involve deeply entrenched neural survival pathways, cognitive insight alone is rarely sufficient to produce lasting change without concurrent somatic regulation 6438.
Cognitive Behavioral and Acceptance Therapies
Cognitive Behavioral Therapy (CBT) operates by identifying and restructuring the distorted mindsets and logical fallacies that fuel appeasement 383940. Clinicians help individuals recognize absolute demands (e.g., "I must avoid conflict at all costs") and replace them with balanced, self-respecting beliefs 3841. A core mechanism of CBT for people-pleasing involves behavioral experiments: the patient is assigned progressively difficult boundary-setting tasks - such as declining a minor request or expressing a dissenting opinion - to empirically test their fears of abandonment and rejection 3841.
Acceptance and Commitment Therapy (ACT) enhances this process by focusing on psychological flexibility. Rather than attempting to eliminate the intense anxiety and guilt that arise when a people-pleaser sets a boundary, ACT teaches the individual to tolerate these uncomfortable sensations while committing to actions that align with their authentic values 383942.
Dialectical Behavior Therapy and Radical Openness
Dialectical Behavior Therapy (DBT), originally developed by Dr. Marsha Linehan, is highly effective for addressing the severe emotional dysregulation that precipitates the fawn response 397043. Utilizing its core modules of Mindfulness, Distress Tolerance, Emotion Regulation, and Interpersonal Effectiveness, DBT equips individuals with the concrete skills required to navigate conflict without automatically defaulting to submission or appeasement 7043.
For chronic people-pleasers, a specialized adaptation known as Radically Open DBT (RO-DBT) is particularly indicated. Traditional DBT primarily addresses emotionally undercontrolled individuals; however, chronic people-pleasers generally exhibit maladaptive overcontrol 44. They obsessively monitor and suppress their spontaneous emotional expressions to maintain a flawless, unthreatening, and agreeable facade 44. RO-DBT targets this precise pathology by actively encouraging openness, vulnerability, and the deliberate dismantling of the fake-agreement mask, ultimately facilitating genuine social signaling and authentic connection 44.
Somatic Experiencing and Autonomic Regulation
Because fawning is ultimately an autonomic survival strategy orchestrated by the amygdala, somatic therapies are essential for resolving the trauma trapped within the nervous system 34644546. Modalities such as Somatic Experiencing (SE), developed by Dr. Peter A. Levine, bypass cognitive narratives to work directly with the body's physiological responses 3445.
| Clinical Modality | Therapeutic Target | Core Mechanisms and Techniques |
|---|---|---|
| Cognitive Behavioral Therapy (CBT) | Conscious thoughts, flawed beliefs, and behavioral habits 3839. | Cognitive restructuring, identification of cognitive distortions, progressive boundary-setting experiments 3841. |
| Radically Open DBT (RO-DBT) | Maladaptive overcontrol and suppressed emotional expression 44. | Identifying unintentional signaling (e.g., fake smiles), vulnerability exercises, dismantling the agreeable mask 44. |
| Somatic Experiencing (SE) | The autonomic nervous system and thwarted trauma responses 3445. | Interoceptive tracking, completing defensive movements, nervous system anchoring, pendulation 4546. |
Table 4: Evidence-based clinical interventions targeting the cognitive, behavioral, and physiological domains of pathological people-pleasing 3839414445.
In SE, clients develop interoceptive awareness - the ability to safely track internal bodily sensations 344647. A critical phase of somatic trauma recovery involves completing "thwarted responses" 45. During childhood trauma, the biological impulses to fight back or run away were suppressed because they were unsafe 45. Somatic therapy allows the nervous system to physically discharge this trapped energy, processing the backlog of repressed fear and anger 4546. By utilizing grounding techniques and specific breathwork protocols (such as diaphragmatic or box breathing), individuals learn to manually shift their autonomic state from sympathetic arousal into ventral vagal safety 4346. As the nervous system slowly learns that the present environment is secure, the biological mandate to fawn extinguishes, allowing the individual to reclaim their psychological autonomy, establish durable boundaries, and engage in relationships rooted in authenticity rather than fear.